
Abstract
Background
Hybrid iterative reconstruction can reduce image noise and produce better image quality compared with filtered back-projection (FBP), but few reports describe optimization of the iteration level.
Objective
We optimized the iteration level of iDose4 and evaluated image quality for pediatric cardiac CT angiography.
Materials and methods
Children (n = 160) with congenital heart disease were enrolled and divided into full-dose (n = 84) and half-dose (n = 76) groups. Four series were reconstructed using FBP, and iDose4 levels 2, 4 and 6; we evaluated subjective quality of the series using a 5-grade scale and compared the series using a Kruskal-Wallis H test. For FBP and iDose4-optimal images, we compared contrast-to-noise ratios (CNR) and size-specific dose estimates (SSDE) using a Student’s t-test. We also compared diagnostic-accuracy of each group using a Kruskal-Wallis H test.
Results
Mean scores for iDose4 level 4 were the best in both dose groups (all P < 0.05). CNR was improved in both groups with iDose4 level 4 as compared with FBP. Mean decrease in SSDE was 53% in the half-dose group. Diagnostic accuracy for the four datasets were in the range 92.6–96.2% (no statistical difference).
Conclusion
iDose4 level 4 was optimal for both the full- and half-dose groups. Protocols with iDose4 level 4 allowed 53% reduction in SSDE without significantly affecting image quality and diagnostic accuracy.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
An optimal protocol of pediatric cardiac CT angiography examination should be performed in accordance with ALARA (as low as reasonably achievable) dose principles [1, 2] while maintaining diagnostic accuracy. Recently, rapid developments in CT technology have allowed reduced radiation exposure for children, including body-size-adaptive CT protocols, low tube voltage, low tube current and automated tube current modulation [3, 4]. However most of these strategies are limited by increased noise and reduced image quality with too-low radiation. Thus CT scanner manufacturers suggested several new image reconstruction methods based on iterative reconstruction techniques [2], including iDose4 and iterative model reconstruction (Philips Healthcare, Cleveland, OH) [5–7], adaptive statistical iterative reconstruction and model-based iterative reconstruction (GE Healthcare, Waukesha, WI) [5, 8], iterative reconstruction in image space and sinogram affirmed iterative reconstruction (Siemens Healthcare, Erlangen, Germany) [9], and adaptive iterative dose reduction (Toshiba Medical Systems, Otawara, Japan) [10]. Recently, pediatric CT studies have shown that compared with CT scans reconstructed with filtered back-projection, low-dose CT scans reconstructed with iterative reconstruction techniques maintain image quality with less noise [1, 6, 8, 10–16]. Few reports describe the technical and clinical feasibility of iterative reconstruction for children with congenital heart disease [9, 11, 17–19] or the optimal iDose4 for a low-dose protocol. Additionally, optimal iteration levels might be different depending on radiation dose for CT images. Thus we studied pediatric CT angiography with two radiation doses and assessed subjective and objective image quality with an advanced fourth-generation iterative reconstruction technique (iDose4, Philips Healthcare, Cleveland, OH).
Materials and methods
Patients
This prospective study was approved by our research ethics committees. The potential risks of contrast medium injection and radiation exposure were explained to the study children’s parents by a cardiac radiologist. Informed consent was obtained from parents of all children included in the study (n = 160; 114 boys). We included children younger than 1 year who had congenital heart disease previously assessed by echocardiography. All children were examined with cardiac CT angiography between February 2011 and February 2014. CT angiography scanning was used for preoperative assessment of cardiovascular anatomy or for evaluation of postoperative results. Exclusion criteria were allergies to iodine contrast medium, tachycardia (>180 beats per minute [bpm], exceeding the scanner limit for electrocardiograph gating), hyperthyroidism and impaired renal function (serum creatinine >1.4 mg/dl).
CT scanning technique and data acquisition
All CT angiography scans were performed using a 256-slice CT system (Philips Brilliance iCT; Philips Healthcare, Cleveland, OH) equipped with a filtered back-projection and hybrid iterative reconstruction (iDose4) reconstruction and post-processing package (Brilliance Workspace; Philips Healthcare, Cleveland, OH). All cases were performed by prospectively gated axial cardiac CT (Step & Shoot Cardiac; Philips Healthcare, Cleveland, OH), and all electrocardiograph electrodes were placed at standard positions. Short-term sedation of uncooperative children was achieved with chloral hydrate solution (0.1 mg/kg, per os; Brilliant Pharma, Chendu, Sichuan, China). No additional drugs were given to modify heart rate.
The following acquisition parameters were used: collimation, 96–128 × 0.625 mm; gantry rotation time, 270 ms; slice thickness, 0.8 mm; reconstruction interval, 0.4 mm. All raw data were obtained at 40–50% of the R-R interval; and three datasets were reconstructed at 40%, 45% and 50% of the R-R interval, and the best phase was chosen to be the evaluation objective. For evaluation of image quality and potential radiation dose reduction with hybrid iterative reconstruction techniques (iDose4) for pediatric cardiac CT angiography, we designed two image-acquisition protocols (full- and half-dose). Children were randomized to one group according to their registered time (i.e. 1st-full dose, 2nd-half dose, etc.). Children with parents who refused low-dose cardiac CT angiography were assigned to the full-dose group.
Based on findings from Paul et al. [20], we used a weight-based protocol (Table 1) as our full-dose protocol. For the half-dose group, we fixed tube voltages and adjusted tube currents (mAs) to the corresponding group. If CT angiography scans with either protocol failed, we planned to perform another full-dose protocol of CT angiography or MRI scan as a remedial measure within a week.
Iodinated contrast medium (Ultravist 300; Bayer Schering Pharma, Berlin, Germany) was injected with a dual-syringe power injector (2.5 ml/kg, intravenously) followed by 5 ml saline. Flow rates were calculated as (weight [kg] × 2.5)/(post threshold delay + scan time +3) ml/s [21]. Bolus tracking was used in a region of interest within the descending aorta at the level of the carina, with an attenuation threshold of region of interest >100 Hounsfield units (HU) to trigger scanning after a 7-s delay. The coverage of the CT angiography scan was from the thoracic inlet to the lower end of the liver, and the scan course was accomplished in one or two passes based on patient size.
Image post-processing and quality analysis
To optimize iDose4 in pediatric CT angiography, we reconstructed all raw datasets of the best phase into four image sets, with the filtered back-projection and the hybrid iterative reconstruction (iDose4) at iteration levels 2, 4 and 6. Images were reconstructed using a XCB (standard) kernel with a thickness of 0.8 mm; the reconstruction interval was 0.4 mm. All images were transferred to an external workstation (Cardiac Viewer, Extended Brilliance Workspace 4.0; Philips Healthcare, Cleveland, OH) for interpretation. Multi-planar reformatting, curved planar reformatting, maximum-intensity projection and volume rendering were used to display cardiac abnormalities depending on target structure.
Subjective image-quality evaluation
Subjective image quality was independently evaluated with a five-point score by two experienced cardiovascular radiologists (L.Y. and H.L, 8 and 10 years of experience). The radiologists evaluated all images with mediastinum and lung window settings, and both radiologists were allowed to change the window width and level to their preference.
Overall subjective image quality was assessed by looking at cardiac and vascular structures (cardiac chambers, thoracic aorta, pulmonary arteries, pulmonary veins, coronary arteries) on 2-D axial images and other reformatted images (multi-planar reformatting, curved planar reformatting, maximum-intensity projection and volume rendering). Both radiologists were blinded to scanning parameters and patient characteristics (weight, age, gender). The scale used to assess subjective image quality was based on the one used by Huang et al. [21]. The grades were as follows; grades 3 or greater were considered sufficient for diagnostic purposes.
-
Grade 5: Excellent anatomical clarity and image quality
-
Grade 4: Good anatomical clarity; all structures clearly interpretable
-
Grade 3: Fair anatomical clarity; the anatomical relationships required clinically could be defined with confidence
-
Grade 2: Poor image quality or anatomical detail; incomplete demonstration of anatomical structures
-
Grade 1: No useful information obtained
Objective image-quality evaluation
To evaluate image quality objectively, the following data were measured: (1) attenuation and image noise, determined as the mean CT value and the mean standard deviation (SD) in the three regions of interest: ascending aorta (AA), main pulmonary artery (MPA), and myocardial walls (MW); (2) contrast-to-noise ratios (CNR), defined as the difference between CT value in the two regions of interest (ascending aorta and main pulmonary artery) and CT value in the myocardial walls divided by the standard deviation of the ascending aorta. The related formulae were CNRAA=(CT value AA – CT value MW) /SDAA, CNRMPA=(CT value MPA – CT value MW) /SDMPA. Regions of interest were adjusted to the area of interest (range from 15 mm2 to 137 mm2).
Assessment of radiation doses
CT dose index volume (CTDIvol) of CT scans was noted from the CT console after each scan. The size-specific dose estimates were calculated with methods recommended by the American Association of Physicists in Medicine (AAPM) report 204 [22]. First, we measured with on-screen calipers in centimeters the maximum lateral diameters (DLAT) of the chest on a standard axial image through the left inferior pulmonary vein. Second, we converted CTDIvol 32 cm and CTDIvol 16 cm to size-specific dose estimates values using the conversion factors listed in Tables 1 and 2 of the AAPM report [22].
Statistical analysis
Statistical analysis was performed with SPSS 20.0 software (IBM, Armonk, NY). We evaluated inter-observer agreement in subjective image-quality grading using kappa statistics, with 0.81 ≤ kappa ≤ 1.0 being excellent consistency, 0.61 ≤ kappa ≤ 0.80 good consistency, 0.41 ≤ kappa ≤ 0.60 moderate consistency, 0.21 ≤ kappa ≤ 0.40 fair consistency, and kappa < 0.20 poor consistency. The differences in age, heart rate and weight were compared between the two dose groups using a Student’s t-test. Subjective image-quality scores of the four image sets (filtered back-projection and three iDose4 levels) for groups were compared using a Kruskal-Wallis H test; if there were statistically significant differences, multiple comparisons were performed with a Bonferroni test to explore the optimal iDose4 iteration level. Mean CT values, noise, CTDIvol, contrast-to-noise ratios and size-specific dose estimates were compared using a Student’s t-test between filtered back-projection images and the iDose4-optimal iteration level images in each dose group. Diagnostic accuracy of CT angiography images was calculated based on the surgical or heart catheterization findings. Diagnostic accuracy differences among the four image sets were compared with Kruskal-Wallis H test. If statistically significant differences were found, multiple comparisons were studied with a Bonferroni test (P-value <0.05 was considered statistically significant).
Results
Patients
No serious adverse events were recorded and all children had successful cardiac CT angiography scanning. In four cases, parents refused to allow low-dose cardiac CT angiography, which meant that four children originally in the half-dose group underwent full-dose CT angiography, resulting in 84 children in the full-dose group and 76 in the half-dose group. Tables 1 and 2 depict patient data. There were significant differences in age (P < 0.05) but no significant differences in weight or heart rate between the two dose groups.
Radiation dose
Significant differences were noted in CTDIvol and size-specific dose estimates between the two dose groups (Table 2; all P < 0.05). Table 3 depicts data for cardiac deformities confirmed in both dose groups. Diagnostic accuracy for cardiac deformities for the four image sets were 92.6%, 94.6%, 95.1% and 96.2% (not significantly different).
Subjective evaluation results
There was a good consistency of overall subjective image quality between independent observers (half-dose group, kappa = 0.74; full-dose group, kappa = 0.73). Diagnostic-quality images (score ≥3) were achieved in all cases (100%, 160/160) using iDose4 levels 4 or 6. Only 1 case (0.6%, 1/160) with transposition of the great arteries did not result in diagnostic-quality images using either filtered back-projection or iDose4 level 2, (this child was scanned with a half-dose protocol). Statistically significant differences were found in subjective scores among the four algorithms for each dose group (Table 4). Data show that the best subjective image quality was reconstructed with iDose4 level 4 for both groups (Figs. 1 and 2).

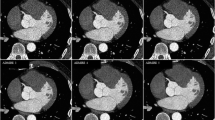
Subjective image quality in the full-dose group. Effects of iDose4 on visibility of left anterior descending coronary artery (arrow in a) in a 10-month-old girl (full-dose group). a–d Different image construction algorithms: (a) filtered back projection, (b) iDose4 level 2, (c) iDose4 level 4, (d) Dose4 level 6. Image reconstructed with iDose4 level 6 (d) displays over-smoothing, or plastic-appearing edges. iDose4 level 4 (c) was considered optimal by both reviewers

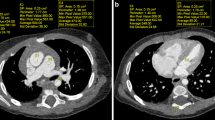
Subjective image quality in the half-dose group. Ventricular septal defect (arrow in a) in a 7-month-old girl child (half-dose group). a–d Different image construction algorithms: (a) filtered back-projection, (b) iDose4 level 2, (c) iDose4 level 4, (d) Dose4 level 6. Image reconstructed with iDose4 level 6 (d) displays over-smoothing, or plastic-appearing edges. iDose4 level 4 (c) was considered optimal by both reviewers
Objective evaluation results
Attenuation
No statistically significant differences in mean CT values were found between filtered back-projection and iDose4 level 4 for the same evaluated anatomical region (ascending aorta, main pulmonary artery and myocardial walls) for each group. iDose4 level 4 caused minimal changes in CT numbers in the same regions of interest in the same dose group (Table 5).
Image noise
Mean noise reduction with iDose4 level 4 was 28% in the ascending aorta (range, 11–38%), 27% in the main pulmonary artery (range, 7–42%) and 24% in the myocardial walls (range, 8–33%) in the half-dose group; 27% in the ascending aorta (range, 13–46%), 21% in the main pulmonary artery (range, 8–38%) and 26% in the myocardial walls (range, 8–45%) in the full-dose group, compared to filtered back-projection. Data in Table 5 show that iDose4 level 4 reduced image noise compared to filtered back-projection for both groups.
Contrast-to-noise ratio
Significant differences in contrast-to-noise ratios were observed between filtered back-projection and iDose4 level 4 for the same evaluated anatomical region (ascending aorta or main pulmonary artery) in each dose group (all P < 0.05) (Table 5). Mean contrast-to-noise ratios increased with iDose4 level 4, including 40% in the ascending aorta (range, 11–62%) and 38% in the main pulmonary artery (range, 13–86%) in the half-dose group; 38% in the ascending aorta (range, 4–72%) and 27% in the main pulmonary artery (range, 4–64%) in the full-dose group, compared with filtered back-projection.
Discussion
The traditional filtered back-projection technique provides poor image quality when CT scanning with low-radiation protocols because of the limits of its mathematical model. More recent hybrid iterative reconstruction technologies, such as iDose4, allow for radiation reduction while maintaining overall diagnostic quality. However, limited studies about optimization of hybrid iterative reconstruction for pediatric CT scanning exist in the literature [6, 17, 23]. Karmazyn’s [6] group compared filtered back-projection and five hybrid iterative reconstruction levels (levels 2–6 of iDose4) for pediatric body CT and found that hybrid iterative reconstruction levels 3 or 4 were optimal for most studies. Mieville et al.’s [17] work suggests that cases performed with filtered back-projection and several hybrid iterative reconstruction levels cause structure conspicuity decreases exceeding 50% of the hybrid iterative reconstruction levels. Their data indicate that ~20–40% hybrid iterative reconstruction level (e.g., levels 1–3 in iDose4) provides the best images [17]. Brady and colleagues [23] also reported that this technique (adaptive statistical iterative reconstruction, GE Healthcare, Waukesha, WI) decreased noise variance and increased graininess with increasing hybrid iterative reconstruction level. Based on the results of phantom and clinical observations, they concluded that 40% hybrid iterative reconstruction level (e.g., iDose4 level 3) provided the best results [23]. However, all of these studies were performed with a full- or single-dose protocol, so whether the optimal iteration is the same with full- or half-dose radiation was unclear until now.
In our study, we compared filtered back-projection and three levels of iDose4 (levels 2, 4, 6) in two groups (full- and half-dose radiation) to find the optimal iteration for each group (Figs. 1 and 2). iDose4 levels 1, 3, 5 and 7 are available, but limited experience with these suggests that differences in any two consecutive levels were minimal. We found that iDose4 level 4 was optimal for both dose groups, indicating that the level of hybrid iterative reconstruction is most important for subjective evaluation results. Data from prior studies suggest that many images reconstructed with iDose4 level 6 appeared unusually smooth, which resulted in degradation of image quality, and both radiologists in this study noted that most of images for both dose groups reconstructed with iDose4 level 6 displayed a plastic appearance (Figs. 1 and 2).
Recently, pure iteration methods, such as model-based iterative reconstruction and iterative model reconstruction, have been developed, and these can be more easily compared than those acquired with a hybrid iterative reconstruction technique [14, 16, 19, 24]. However clinical application of model-based iterative reconstruction and iterative model reconstruction is limited by a longer reconstruction time compared with hybrid iterative reconstruction or filtered back-projection [19] methods, and, as reported by Mieville and colleagues [5], structure conspicuity in these techniques is decreased by more than 50% as compared to hybrid iterative reconstruction. So, whether similar results are obtained with pure iteration images requires more studies with large sample sizes. For this pediatric CT angiography study of hybrid iterative reconstruction, neither radiologist noticed artifacts or alterations in image appearance for any regions with iDose4 level 4.
A reliable iterative reconstruction method should not change the attenuation (HU). Our results demonstrate that there were no statistically significant differences in attenuation between filtered back-projection and iDose4 level 4 images for the full- or the half-dose group, which indicates that iDose4 level 4 does not influence the attenuation. A similar result was found by Zheng et al. [11].
There were no statistically significant differences for diagnostic accuracy among the four image sets (full- and half-dose filtered back-projection and optimal hybrid iterative reconstruction level images). This may be because there were limited effects of half-doses of radiation or that the half-dose protocol might be still higher than needed, indicating that further radiation reduction is possible. Our data show that the hybrid iterative reconstruction technique (iDose4) allowed a reduction of size-specific dose estimates by half without a loss of diagnostic information. Mieville’s group [17] evaluated the benefits of adaptive statistical iterative reconstruction on diagnostic image quality in pediatric cardiac CT examinations and indicated that a 36% radiation reduction is possible for a 2- to 3-year-old child when using 40% adaptive statistical iterative reconstruction. Tricarico and colleagues [9] assessed image quality of simulated half-dose pediatric cardiovascular CT angiography, and they reconstructed all raw data with filtered back-projection and iterative reconstruction. They reported that iterative reconstruction improved image noise, contrast-to-noise ratios, and subjective image quality compared with filtered back-projection for low-radiation-dose pediatric CT angiography and might allow for further radiation reductions without compromising diagnostic image quality. Zheng and co-workers [11] decreased radiation by 53.8% for 62 pediatric cardiovascular CT angiography exams and reported that a combination of prospectively electrocardiograph-triggered high-pitch spiral acquisition, low tube current, and iterative reconstruction technologies offered diagnostic images for pediatric cardiovascular CT angiography with effective dose <0.1 mSv. Compared with prior studies, we documented similar or higher dose reductions with hybrid iterative reconstruction in children with congenital heart disease. Effective dose or size-specific dose estimate values from our study might be greater than those of published reports because we used a large scanning range (from the thoracic inlet to the lower end of the liver) and large phase tolerance around the 45% phase (40–50%).
Our study has several limitations. First, the study only evaluates one vendor’s reconstruction technique, and optimization parameters might not be easily translated to other vendor technology. Second, during the subjective image assessment, although we removed all study information from CT angiography images, the typical smoothing effect of hybrid iterative reconstruction on CT angiography images limited a true blinding — radiologists can differentiate these from traditional filtered back-projection images and this might introduce some bias. Finally, the sample size was moderately small, with only 76 children enrolled in the half-dose group. Although our data indicate that hybrid iterative reconstruction in pediatric CT angiography examinations reduced radiation without affecting image quality, more studies with larger sample sizes are required to confirm our findings before routine application in the field. We plan to conduct more studies with larger sample sizes to evaluate the stability of the half-dose protocol. If our findings are confirmed, we plan to implement the half-dose protocol with iDose4 level 4 as a routine protocol for all pediatric CT angiography exams.
Conclusion
iDose4 level 4 was optimal for most patients in both dose groups, indicating that iDose4 might significantly reduce radiation used for pediatric cardiovascular CT angiography studies. A low-dose protocol with iDose4 level 4 and prospective electrocardiograph-triggered acquisition permitted a 53% reduction in size-specific dose estimates, without significantly affecting image quality and diagnostic confidence. This work might be helpful for promoting hybrid iterative reconstruction for pediatric cardiovascular CT angiography and thereby decreasing radiation exposure.
References
Ho C, Oberle R, Wu I et al (2014) Comparison of image quality in pediatric head computed tomography reconstructed using blended iterative reconstruction versus filtered back projection. Clin Imaging 38:231–235
Khawaja RD, Singh S, Otrakji A et al (2015) Dose reduction in pediatric abdominal CT: use of iterative reconstruction techniques across different CT platforms. Pediatr Radiol 45:1046–1055
Herzog C, Mulvihill DM, Nguyen SA et al (2008) Pediatric cardiovascular CT angiography: radiation dose reduction using automatic anatomic tube current modulation. AJR Am J Roentgenol 190:1232–1240
Tsai IC, Lee T, Chen MC et al (2007) Visualization of neonatal coronary arteries on multidetector row CT: ECG-gated versus non-ECG-gated technique. Pediatr Radiol 37:818–825
Mieville FA, Gudinchet F, Brunelle F et al (2013) Iterative reconstruction methods in two different MDCT scanners: physical metrics and 4-alternative forced-choice detectability experiments — a phantom approach. Phys Med 29:99–110
Karmazyn B, Liang Y, Ai H et al (2014) Optimization of hybrid iterative reconstruction level in pediatric body CT. AJR Am J Roentgenol 202:426–431
Klink T, Obmann V, Heverhagen J et al (2014) Reducing CT radiation dose with iterative reconstruction algorithms: the influence of scan and reconstruction parameters on image quality and CTDIvol. Eur J Radiol 83:1645–1654
Sun J, Peng Y, Duan X et al (2014) Image quality in children with low-radiation chest CT using adaptive statistical iterative reconstruction and model-based iterative reconstruction. PLoS One 9, e96045
Tricarico F, Hlavacek AM, Schoepf UJ et al (2013) Cardiovascular CT angiography in neonates and children: image quality and potential for radiation dose reduction with iterative image reconstruction techniques. Eur Radiol 23:1306–1315
Buchmann RF, Bruce Greenberg S (2014) Optimizing image quality for pediatric torso computed tomography: the use of advanced iterative reconstruction and wide-detector scanning techniques. J Comput Assist Tomogr 38:786–789
Zheng M, Zhao H, Xu J et al (2013) Image quality of ultra-low-dose dual-source CT angiography using high-pitch spiral acquisition and iterative reconstruction in young children with congenital heart disease. J Cardiovasc Comput Tomogr 7:376–382
Brady SL, Moore BM, Yee BS et al (2014) Pediatric CT: implementation of ASIR for substantial radiation dose reduction while maintaining pre-ASIR image noise. Radiology 270:223–231
Kim JH, Kim MJ, Kim HY et al (2014) Radiation dose reduction and image quality in pediatric abdominal CT with kVp and mAs modulation and an iterative reconstruction technique. Clin Imaging 38:710–714
Koc G, Courtier JL, Phelps A et al (2014) Computed tomography depiction of small pediatric vessels with model-based iterative reconstruction. Pediatr Radiol 44:787–794
McKnight CD, Watcharotone K, Ibrahim M et al (2014) Adaptive statistical iterative reconstruction: reducing dose while preserving image quality in the pediatric head CT examination. Pediatr Radiol 44:997–1003
Smith EA, Dillman JR, Goodsitt MM et al (2014) Model-based iterative reconstruction: effect on patient radiation dose and image quality in pediatric body CT. Radiology 270:526–534
Mieville FA, Gudinchet F, Rizzo E et al (2011) Paediatric cardiac CT examinations: impact of the iterative reconstruction method ASIR on image quality — preliminary findings. Pediatr Radiol 41:1154–1164
Han BK, Grant KL, Garberich R et al (2012) Assessment of an iterative reconstruction algorithm (SAFIRE) on image quality in pediatric cardiac CT datasets. J Cardiovasc Comput Tomogr 6:200–204
Son SS, Choo KS, Jeon UB et al (2015) Image quality of CT angiography with model-based iterative reconstruction in young children with congenital heart disease: comparison with filtered back projection and adaptive statistical iterative reconstruction. Int J Cardiovasc Imaging 31:31–38
Paul JF, Rohnean A, Elfassy E et al (2011) Radiation dose for thoracic and coronary step-and-shoot CT using a 128-slice dual-source machine in infants and small children with congenital heart disease. Pediatr Radiol 41:244–249
Huang M-p, Liang C-h, Zhao Z-j et al (2011) Evaluation of image quality and radiation dose at prospective ECG-triggered axial 256-slice multi-detector CT in infants with congenital heart disease. Pediatr Radiol 41:858–866
Boone JM, Strauss KJ, Code DD et al (2011) Size-specific dose estimates (SSDE) in pediatric and adult body CT examinations. AAPM Report No. 204. http://www.aapm.org/pubs/reports/RPT_204.pdf. Accessed 13 July 2016
Brady SL, Yee BS, Kaufman RA (2012) Characterization of adaptive statistical iterative reconstruction algorithm for dose reduction in CT: a pediatric oncology perspective. Med Phys 39:5520–5531
Vardhanabhuti V, Loader RJ, Mitchell GR et al (2013) Image quality assessment of standard- and low-dose chest CT using filtered back projection, adaptive statistical iterative reconstruction, and novel model-based iterative reconstruction algorithms. AJR Am J Roentgenol 200:545–552
Acknowledgments
This work was supported by the National Natural Scientific Foundation of China (No. U1301258 and No. U1401255) and the Guangdong Province Science and Technology Planning Project of China (No. 2014A020212228).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Rights and permissions
About this article

Cite this article
Yang, L., Zhuang, J., Huang, M. et al. Optimization of hybrid iterative reconstruction level and evaluation of image quality and radiation dose for pediatric cardiac computed tomography angiography. Pediatr Radiol 47, 31–38 (2017). https://doi.org/10.1007/s00247-016-3698-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-016-3698-4