
Abstract
Background
Radiographic bone age determination is part of the routine evaluation of suspected growth disorders. Simplicity and low cost are its major advantages, but although the effective dose of ionizing radiation is low, it should be taken into consideration given its cumulative effect.
Objectives
To assess the chronological ultrasonographic emergence of the ossification centers of the hand and wrist.
Materials and methods
Cross-sectional study of healthy patients ages 1 to 24 months (n = 498) from Buenos Aires, Argentina. All patients underwent ultrasonographic evaluation of the left hand and wrist to identify the different bone nuclei; a subgroup of infants had their nuclei measured (n = 228).
Results
Girls showed an earlier emergence of the evaluated nuclei and a trend to a greater size than age-matched boys. Size-for-age relation showed linear increase. Carpal bones (capitate and hamate) were the first to appear, as early as from the first 3 months of life, an age gap not thoroughly present on the radiographic atlas developed by Greulich and Pyle. The distal epiphysis of the radius and the second metacarpophalangeal joint (index finger) followed in order of emergence. The proximal epiphysis of the first metacarpal bone (thumb) was the last to emerge and was infrequently found on boys at age 24 months. Overall, these findings are in accordance with the radiographic atlas. An ultrasonography atlas of the left hand and wrist was outlined for girls and boys.
Conclusion
Conventional ultrasonography allows proper identification of the ossification centers of the hand and wrist and may become an innocuous follow-up tool for patients with growth disorders.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Bone age estimation is part of the routine evaluation of children with suspected growth disorders [1]. It is determined by comparing different bone structures evaluated through radiographic exposure with an age- and sex-adjusted radiographic atlas.
The initial project by T. Wingate Todd [2] was completely developed by Greulich and Pyle [3] and is considered the gold standard for bone-age determination. It is widely used given its worldwide acceptance, simplicity, low cost and effective dose. The cumulative effect of ionizing radiation on patients with high life expectancy should not be underestimated. Other methods, such as the one developed by Tanner and Whitehouse, may be more accurate by including a larger number of variables but it is time-consuming [4–6].
Mineralization of ossification centers starts around the fifth month of gestational age [7]. Cartilaginous ossification centers (non-mineralized) are ultrasonographically hypoechoic while bone (mineralized) tissue is echogenic and has an acoustic shadow. There have been attempts to determine skeletal age with conventional US techniques [8–10] and with specifically designed ultrasonographic devices [4, 11] that have not met adequate correlation parameters with the Greulich and Pyle method in all studies in order to replace standard radiographic procedures [12].
We aimed to determine the chronologic emergence of the different ossification centers of the hand and wrist on a healthy population from birth to 2 years old, with conventional US, a non-invasive, non-ionizing method.
Materials and methods
We conducted a multicenter, cross-sectional prospective study of healthy children from Buenos Aires, Argentina. Patients ages 1 to 24 months with an appointment for a US study not related to growth or developmental disorders were recruited after parental consent.
Based on the radiographic emergence of the ossification centers of the hand and wrist [3], patients ages 1, 2, 3, 4, 6, 9, 12, 15, 18 and 24 months were included in the study. Ultrasonographic evaluation of the left hand and wrist was performed with a commercial US machine (Voluson 730 Pro; GE Healthcare Technologies, Milwaukee, WI, USA) equipped with a high-frequency linear transducer (7.5-20 MHz) by either of two participating pediatric imaging specialists (M.D. and C.C.).
According to expected normal bone development and ossification [3], the absence or presence of the ossification centers of the hand and wrist was registered in all patients: capitate and/or hamate bones; distal epiphysis of the radius; distal epiphysis of the second metacarpal bone and proximal epiphysis of the first phalange of the index finger, and proximal epiphysis of the thumb metacarpal bone (Fig. 1). A subgroup of patients had these ossification centers measured at the same sitting. US was performed through the dorsal face of the hand lying on the examination couch or on the parent’s hand or lap. According to the expected growth direction, carpal findings were measured with the transducer positioned transversally, while metacarpal and phalangeal bones were measured longitudinally (Fig. 1).

Radiographic schematic representation (I) and ultrasonographic appearance (II) of the left hand and wrist of an infant up to age 24 months. (I) Dotted lines represent the direction of the linear transducer at the different evaluation points: (a) capitate and hamate; (b) distal epiphysis of the radius; (c) metacarpophalangeal joint of the index finger and (d) proximal epiphysis of the thumb metacarpal bone. (II) Ultrasonographic view of the absence (left) and presence (right) of the mentioned ossification nuclei (white arrows)
The institutional review board approved the study
Statistical analysis
Continuous variables were expressed as group media and 95% confidence interval (95% CI). Odds ratio with its respective 95% CI was calculated to compare the relative odds of the emergence of the different nuclei between sexes in age-matched groups. Non-parametric tests were used to compare continuous variables between groups. Fisher exact test and sign and binomial test were used to compare categorical variables. A two-sided P-value < 0.05 was considered statistically significant. A correlation coefficient (R2) was calculated to assess the degree of linear association between variables. Data analysis was performed with a software package (SPSS for Windows,Version 15.0; SPSS Inc., Chicago, USA).
Results
During the study period, 498 white (Hispanic and Caucasian) patients without growth or developmental disorders ages 1 to 24 months (specifically 1, 2, 3, 4, 6, 9, 12, 15, 18 and 24 months) were evaluated; 252 were girls (50.6%). A subgroup of 228 patients had their ossifications centers measured; 117 were girls (51.3%) (Table 1). On average, less than 10 min were necessary to perform the complete evaluation.
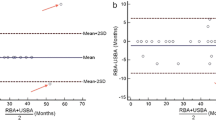
The different ossification centers’ measures displayed on a length-for-age scatter plot with their respective trend lines, showed linear increase with modest R2 correlation (Fig. 2). Non-significant results of the Kolmogorov-Smirnov test for normality showed that the size of the ossification centers, when divided into groups of the same age and sex, trended toward a normal distribution.

Length-for-age measurements of the evaluated nuclei of the hand and wrist on girls and boys. Linear trend lines show modest R2 fitness, with lower values on smaller samples and narrower size ranges. Capitate (a), hamate (b), distal epiphysis of the radius (c) and proximal epiphysis of the first metacarpal (thumb) ossification nuclei (d). The index finger metacarpophalangeal joint of boys (e) and girls (f) shows a higher expected slope of growth of the distal epiphysis of the index finger metacarpal compared to the proximal epiphysis of index finger proximal phalanx
The population was mainly of western European heritage (primarily 3rd-4th generation from Spain, Italy, Great Britain) and to a lesser extent Latin-American neighboring countries. It has been proposed that the population resembles the Italian population regarding bone maturation speed and maturation is faster than that of North America and Great Britain [13].
Children were grouped according to sex and age. The presence and absence of the evaluated ossification centers was analyzed with sign test to determine whether the odds of the nuclei were likely to be present, absent or either present or absent. The result of this analysis combined with the ultrasonographic aspect of the nuclei at the above determined ages constituted an age-adjusted US atlas of the hand and wrist of girls and boys (Figs. 3 and 4).

Ultrasound images of the hand and wrist of girls ages 1 to 24 months show the chronological emergence and appearance of the ossification centers. (+) Significantly present, (−) significantly absent and (±) either present or absent, according to sign-test results

Ultrasound images of the hand and wrist of boys ages 1 to 24 months show the chronological emergence and appearance of the ossification centers. (+) Significantly present, (−) significantly absent and (±) either present or absent, according to sign test results
Carpal ossification centers: capitate and hamate
The first nuclei in the carpal region to ossify were capitate and hamate, most frequently simultaneously, but occasionally the former preceded the latter (odds ratio 1.5 [95%CI 0.80, 2.80] and 1.84 [95%CI 0.84, 4.0] for boys and girls; P = 0.27 and 0.18, respectively). Initially they appeared as punctuate echogenic images and later evolved to rounded lineal images, a sounder feature for the capitate. The capitate was likely to be present in girls from the first month while hamate was almost uniformly present by the second month. On the other hand, the capitate was frequently present on boys by the third month and the hamate by the fourth month. In comparison, the capitate was more frequently absent in boys than in girls until the third month of life (odds ratio 7.62 [95%CI 2.13, 27.2] and 5.63 [95%CI 1.33, 23.8]; P = 0.001 and 0.02 in the first and second months, respectively) and the hamate until the second month (odds ratio 5.14 [95%CI 1.52, 17.4]; P = 0.01). When present, age-matched mean sizes were not significantly different (P = ns) (Fig. 2).
Distal radial epiphysis
The rounded shape of the distal epiphysis of the radius began being visible at the age of 4 months but was more frequently negative until the age of 6 months in girls and 9 months in boys. By the age of 12 months, it was more frequently absent in boys than in girls (odds ratio 5.95 [95%CI 1.80, 19.70]; P < 0.01). Girls showed a greater size of the ossification nucleus at 18 months (5.75 mm [95%CI 4.52, 6.98] vs. 4.54 mm [95%CI 3.17, 5.91]; P = 0.096) (Fig. 2).
Metacarpophalangeal joint of the index finger
The ossification nuclei that make up the metacarpophalangeal joint appeared frequently simultaneously, but sometimes the distal epiphysis of the index finger metacarpal was visible before the proximal epiphysis of the first phalange of the second finger (odds ratio 1.23 [95%CI 0.76, 2.0; P = 0.46] and 1.09 [95%CI 0.69, 1.72; P = 0.81] for boys and girls, respectively). They started being evident by the sixth month but they were more frequently absent until 9 months in girls and 12 months in boys. By the ages of 15 and 18 months, they were more frequently absent in boys than in girls (odds ratio at 15 and 18 months for distal epiphysis 39.4 [95%CI 4.44, 349] and 20.2 [95%CI 1.1, 370], respectively; for proximal epiphysis 82.1 [95%CI 4.41, 1,528] and 31.7 [95%CI 1.75, 573]; P < 0.05 for all). At the age of 24 months, mean sizes were significantly larger among girls than in boys (distal epiphysis: 2.42 mm [95%CI 1.98, 2.85] vs. 1.63 mm [95%CI 1.21, 2.06]; and proximal epiphysis: 1.28 mm [95%CI 1.13, 1.43] vs. 0.88 mm [95%CI 0.75, 1.01] and boys, respectively; P < 0.01 for both).
In concordance with radiographic developmental anatomy, the slope of growth of the proximal epiphysis of the first phalange of the index finger was less pronounced than that of the distal epiphysis of the index finger metacarpal bone (Figs. 1 and 2).
Proximal epiphysis of the proximal epiphysis of the thumb metacarpal
The last ossification center to be visualized ultrasonographically was the proximal epiphysis of the metacarpal bone of the thumb. It started becoming occasionally visible in girls at the age of 12 months and was uniformly present at the age of 24 months, while it was absent in boys until 18 months of age, which translated into a significant difference at 18 and 24 months (odds ratio 5.75 [95%CI 1.73, 19.2] and 68.7 [95%CI 3.83, 1,231]; P < 0.01 at 18 and 24 months). Its frequent presence in girls at the age of 18 months did not translate into a significant difference (sign test for absence vs. presence at 18 months P = 0.42). More importantly, less than half of the boys (6/23) had this nucleus present at 24 months and those who had it showed a significantly smaller size than girls (0.8 mm [95%CI 0.46, 1.14] vs. 1.51 mm [95%CI 1.15, 1.87]; P = 0.026) (Fig. 2).
Triquetrum
Although the triquetrum was not part of the expected ossification nuclei to be evaluated at these ages, at 24 months it was seen in a minor percentage of girls and boys (5 of 26 and 3 of 30, respectively).
Discussion
Bone age estimation, most frequently by comparison with the radiographic Greulich and Pyle atlas, remains a cornerstone in the evaluation of suspected growth disorders. Ultrasonography, a quick and innocuous method, detects ossification centers through their characteristic echogenicity and acoustic shadow.
Studies evaluating the accuracy of specifically designed non-operator-dependent US devices have shown that it may be not accurate enough to replace radiologic standard methods [11, 12, 14]. This attractive, objective device estimates bone age through an algorithm that uses changes in the speed of US waves as a result of going through different structures [11]. A cross-sectional comparative study by Khan et al. [12] showed that the poorest correlation was seen when comparing the radiographic method (Greulich and Pyle) with the ultrasonographic method, but when the population was divided into normal, delayed or advanced bone age, the highest correlation was found in the normal bone age group. On the other hand, Mentzel et al. [11] with the same device showed good correlation coefficients of the distal radius and ulna with the Greulich and Pyle method. Both studies included patients with suspected or confirmed growth disorders [11, 12].
It has been proposed that radiographic maturation of carpal bones may vary between patients, and that metacarpal bones and phalanges may be more precise in the estimation of bone age [10, 15–17]. Bilgili et al. [10] showed that conventional ultrasonographic evaluation of the hand and wrist correlated adequately with the radiographic method, and that when ± 2 months was accepted as a reasonable difference, there was no statistical difference between the two methods. Moreover, when the population assessed was younger than 18 months the difference ranged between 1.36 ± 1.57 and 0.67 ± 1.28 months for boys and girls, respectively [10]. Some discrepancies have been found between chronological age and Greulich and Pyle standards regarding ethnicity, suggesting that ethnicity should be taken into account to estimate bone age with this method, particularly in late childhood and adolescence [18].
In our study, we evaluated the ultrasonographic emergence of the ossification centers of the hand and wrist in an age range not contemplated on the Greulich and Pyle atlas [3] (1 and 2 months) and a younger population than in other ultrasonographic studies [11, 12].
The chronological order of emergence of the hand and wrist was the same in girls as in boys; the capitate and hamate were the first to emerge followed by the epiphysis of the radius and the nuclei of the metacarpophalangeal joint of the index finger. Lastly, the metacarpal joint of the thumb was visible and occasionally the triquetrum. As seen on the Greulich and Pyle atlas, girls had a significantly earlier emergence of the evaluated nuclei than boys and in some cases a significant bigger size.
Although the differences between our study and Greulich and Pyle may be related to the relatively small sample size and the lack of comparison to a radiograph, these differences should be mentioned. Firstly, the nucleus of the proximal epiphysis of the thumb was frequently present on girls at the age of 18 months, not frequently enough to reach statistical significance though. Secondly, in our study, the capitate and hamate were present at 1 and 2 months of age. Although newborns were not evaluated by Greulich and Pyle, their radiographic atlas has these bones present at the age of 3 months. A comparison of both methods in newborns seems unlikely to happen given the need to use ionizing radiation on a healthy population. However, ultrasonography may be particularly useful to assess the impact of hypothyroidism in early life, given that ultrasonographic changes occur at 1 and 2 months of age, and it may be more sensitive to assess this impact than the 3-month radiograph. Thirdly, the triquetrum was found on some patients ages 24 months, although it was most likely to be absent (P < 0.001).
Unlike the specifically designed non-operator-dependent devices mentioned above, conventional US relies on the identification of structures, allows measurements to be taken and may be useful to identify bone abnormalities, if present. Although it was not the primary objective of the study to evaluate the size of the nuclei, ultrasonographic measurements were performed to evaluate the progressive growth of the different ossification centers and to consider US as a potentially accurate and harmless tool for future studies. Given the lack of use of ionizing radiation, it can be repeated as frequently as needed to aid in short-term follow-up if growth disorders are diagnosed and to monitor treatment responsiveness of patients receiving growth-hormone therapy. Although the preparation of a population-based growth chart of the evaluated ossification centers with their respective length-for-age percentiles was beyond the aim of this study, the data provided show that a study of that kind seems possible given the ability of US to perform measurements. Further studies are needed to validate the trueness and precision of US measurements on children.
Limitations of the study include the relatively small number of patients included to obtain a conclusion of the general population. A larger sample may allow the calculation of clinically useful percentile values. Ultrasonography was performed by experienced pediatric imaging specialists and although it was not time-consuming, it may require training in the field and is subject to interobserver variability. We acknowledge that no comparison with the gold-standard radiograph of the hand and wrist was made, mainly because patients included in this study were healthy individuals and X-ray exposure misbalanced the risk-benefit equation of a study of this kind. Another limitation was the lack of follow-up given the design of the study and the absence of an age-blinded physician performing the ultrasonographic evaluation and estimating the patients’ age according to the preliminary results.
We believe this data and images, added to the information provided in the study by Bilgili et al. [10], may represent a useful atlas of the ultrasonographic appearance of the ossification nuclei of the hand and wrist in the evaluated ages.
It remains uncertain if there are significant differences in the chronological emergence and size of the ultrasonographically evaluated nuclei between healthy patients and those with growth suspected or confirmed disorders.
Conclusion
The chronological emergence of the ossification centers of the hand and wrist of healthy infants may be determined with conventional ultrasonography, a quick, simple and most importantly innocuous method. These characteristics may allow safe follow-up of infants with growth disorders and may prove a useful tool toward a radiation-free clinical practice.
References
Growth Hormone Research Society (2000) Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH research society. J Clin Endocrinol Metab 85:3990–3993
Todd W (1937) Atlas of skeletal maturation --hand. The C.V. Mosby Company, St. Louis
Greulich W, Pyle S (1959) Radiographic atlas of skeletal development of the hand and wrist, 2nd edn. Stanford University Press, California
Castriota-Scanderbeg A, Sacco MC, Emberti-Gialloreti L et al (1998) Skeletal age assessment in children and young adults: comparison between a newly developed sonographic method and conventional methods. Skeletal Radiol 27:271–277
Tanner J, Oshman D, Bahhage F et al (1997) Tanner-Whitehouse bone age reference values for North American children. J Pediatr 131:34–40
Tanner J, Healy M, Goldstein H et al (2001) Assessment of skeletal maturation and prediction of adult weight (TW3 method), 3rd edn. WB Saunders, London
Gentili P, Trasimeni A, Giorlandino C (1984) Fetal ossification centers as predictors of gestational age in normal and abnormal pregnancies. J Ultrasound Med 3:193–197
Wagner UA, Diedrich V, Schmitt O (1995) Determination of skeletal maturity by ultrasound: a preliminary report. Skeletal Radiol 24:417–420
Castriota-Scanderbeg A, Micheli V (1995) Ultrasound of femoral head cartilage: a new method of assessing bone age. Skeletal Radiol 24:197–200
Bilgili Y, Hizel S, Kara SA et al (2003) Accuracy of skeletal age assessment in children from birth to 6 years of age with the ultrasonographic version of the greulich-pyle atlas. J Ultrasound Med 22:683–690
Mentzel H-J, Vilser C, Eulenstein M et al (2005) Assessment of skeletal age at the wrist in children with a new ultrasound device. Pediatr Radiol 35:429–433
Khan KM, Miller BS, Hoggard E et al (2009) Application of ultrasound for bone age estimation in clinical practice. J Pediatr 154:243–247
Lejarraga H, Guimarey L, Orazi V (1997) Skeletal maturity of the hand and wrist of healthy Argentinian children aged 4–12 years, assessed by the TWII method. Ann Hum Biol 24:257–261
Mentzel HJ, Vogt S, Vilser C et al (2005) Assessment of skeletal age using a new ultrasound method. Röfo 177:1699–1705
Carpenter CT, Lester EL (1993) Skeletal age determination in young children: analysis of three regions of the hand/wrist film. J Pediatr Orthop 13:76–79
Garn SM, Rohmann CG (1960) Variability in the order of ossification of the bony centers of the hand and wrist. Am J Phys Anthropol 18:219–230
Garn SM, Rohmann CG (1962) Parent–child similarities in hand-wrist ossification. Am J Dis Child 103:603–607
Ontell FK, Ivanovic M, Ablin DS et al (1996) Bone age in children of diverse ethnicity. AJR Am J Roentgenol 167:1395–1398
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Daneff, M., Casalis, C., Bruno, C.H. et al. Bone age assessment with conventional ultrasonography in healthy infants from 1 to 24 months of age. Pediatr Radiol 45, 1007–1015 (2015). https://doi.org/10.1007/s00247-014-3253-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-014-3253-0