
Abstract
Background: Determination of skeletal development in children is important. The most common method of evaluation uses the standards of Greulich and Pyle (G&P) to assess the left hand radiograph. Numerous assessments may be made during follow-up. Objective: The aim of our study was to compare the accuracy of a new sonographic method with the standard radiographic method. Materials and methods: Seventy consecutive patients (age 6–17 years; 34 girls, 36 boys) underwent radiography of the left hand, followed by sonographic examination of the same hand using the BonAge system (Sunlight Medical Ltd., Israel). This system evaluates the relationship between the velocity of sound passing thorough the distal radial and ulna epiphysis and growth, using gender- and ethnicity-based algorithms. One experienced paediatric radiologist analysed the radiograph and assigned bone age scores based on the G&P atlas for the whole left hand and for the distal radius alone. The radiologist was blinded to the chronological age (CA), height of the patient and the BonAge result. Correlation between BonAge and G&P was undertaken. Results: In 65 patients, BonAge measurement could be performed successfully. In five patients, the scanning process was impossible using the ultrasound device. The r2 (r is the Pearson correlation coefficient) of the BonAge ultrasound measurement and the G&P method was 0.82. The averaged accuracy (i.e. absolute difference in years between G&P reading and BonAge ultrasonic results) was calculated. Results were similar for boys and girls: 1.0±0.8 years for the whole left hand and 0.8±0.7 year for the distal radius. On average, the difference between BonAge and CA is the same as the difference between G&P and CA, i.e. 1.4 years. Conclusions: The BonAge device demonstrates the ability of ultrasound to produce an accurate assessment of bone age. The results are highly correlated with skeletal age evaluated conventionally using the G&P method. Obvious advantages of the ultrasound device are objectivity, lack of ionizing radiation, and easy accessibility.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Determination of skeletal development in children is important, especially for those suspected of growth disorders or patients with chronic diseases and possible retardation of growth. The use of radiographs of the hand to evaluate the maturation of the skeleton is one of the oldest applications of diagnostic radiography. The first report dates from 1898, when Poland [1] described in detail the radiographs of hands of British children. In 1959, Greulich and Pyle (G&P) [2] presented their technique that utilized an atlas in which they presented normal radiographs to which they assigned a skeletal age. All radiographs in this atlas were collected in Ohio, USA, in the period 1931–1942. Each standard film in the G&P atlas was selected from 100 radiographs of the same age and sex. Although many additional techniques have been described since G&P, currently up to 76% of paediatricians use the G&P technique to assess skeletal age [3]. For skeletal age assessment, the radiograph of the patient is compared with the representative radiographs in the atlas and a skeletal age is assigned. In recent years, some studies of healthy volunteers have dealt with the applicability of old radiographs in the G&P atlas to a modern population [4–8]. All have concluded that the G&P atlas is still applicable to the current population; mean differences between skeletal age evaluated by the G&P method and chronological age (CA) are less than 1 year, which is within the normal spread [7, 8]. A further widely accepted method for the evaluation of skeletal maturation is the method of Tanner and Whitehouse (TW2), which also requires the radiograph of the left hand and wrist [9]. The TW2 method depends on scoring the stage of bony development of 20 bones in the hand and wrist by comparison with a series of scored standards, thus producing a total score from which a skeletal age may be read directly from tables. The TW2 method is more flexible than the G&P method and more accurate since it derives from a more solid mathematical base, but it is more difficult to perform and is time-consuming. However, estimation of skeletal age using the G&P or the TW2 systems necessitates the use of ionizing radiation. Thus, several ultrasound-based techniques have been developed for the estimation of skeletal age without radiation [10–12].
The aim of this study was to compare the performance of a new ultrasound method at the wrist (BonAge, Sunlight Medical Ltd., Tel Aviv, Israel) with the most widely means of estimating bone age (G&P), by establishing the level of accuracy and correlation between both methods and the differences between the calculated skeletal age and CA.
Materials and methods
Patients
From February to April 2004, 70 subjects (34 girls, 36 boys) with proven or suspected growth disorder, who had undergone left hand and wrist radiography for skeletal age assessment, were also examined sonographically using the BonAge system. Radiography and ultrasound measurement were performed on the same day and on the same hand. Children younger than 4 years were excluded because the system could not return a reliable result in such young children. A history of previous fractures was verified by a questionnaire. Children who had fractures in both hand were excluded.
Informed consent from the parents and/or children, according to the guidelines stated in the Helsinki declaration, was obtained. The local ethics committee was informed and agreed to our study.
Radiographs
In all cases, conventional radiographs of the left hand were performed for the evaluation of skeletal age in accordance with the G&P method. The radiographs were obtained in a single centre. Standardized PA radiographs of the left hand were taken on a single film (Kodak Trimax Regula 400) using the following parameters: filter 1.0 mm aluminium and 0.1 mm copper, film focus distance 1 m, focal spot 0.6 mm, tube voltage 45 kVp, exposure 3.2–4 mAs.
Sonography
The BonAge is composed of a main unit that contains the user interface and algorithmic calculation software, and a measurement unit that includes an ultrasound probe (Fig. 1). The measurement unit consists of an ultrasound probe with two ultrasound transducers located on two stands at the sides of the measurement unit. Between the transducers, an armrest assists with immobilization of the patient’s hand and wrist. The measurement site is located in the region of the wrist. For correct positioning, the investigator has to mark the position of the distal tip of the ulna styloid process. This site includes centres of ossification that change with growth. However, since imaging is not included in the ultrasonic measurement, the path of ultrasound waves is not known in detail. The technique utilizes the physical properties of the epiphyses of the distal radius and ulna. Ultrasonic waves with a frequency of 750 kHz are transmitted through the left wrist; the ulnar-side transducer acts as the emitter while the other is the receiver. Eleven cycles of measurement are performed to ensure high precision, and the entire measurement takes about 5 min. The device calculates the speed of sound (SOS) and uses the distance between the transducers under known and controlled pressure conditions, and a proprietary gender- and ethnicity-based algorithm to provide a numeric result of the skeletal age in years and months that correlates to the G&P atlas. The gender- and ethnicity-based algorithms are available for male and female Caucasians and Chinese between the ages of 5 years and 18 years.

Measurement unit of the BonAge device. The unit consists of two ultrasound transducers (arrows). The armrest between the transducers helps to fix the patient‘s hand and wrist
Data analysis
A paediatric radiologist (H.-J.M.) evaluated all hand radiographs and determined the skeletal age in standard fashion according to the G&P atlas [2]. Interpretation of the radiographs was performed blindly without knowledge of the age and height of the patient and without knowledge of the BonAge result. A student (M.E.) performed all sonographic measurements. The device calculated the SOS and provided a numeric result in years and months. Data analysis was performed using the Statistical Package of Social Sciences (SPSS version 11.0, Chicago, Ill., USA). The Pearson correlation between BonAge and G&P was performed. Averaged accuracy was calculated.
Results
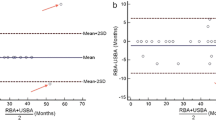
In 65 patients, BonAge measurement could be performed successfully. In five patients, all less than 6 years old, the scanning process was impossible and was aborted by the system. All patients tolerated the scanning process well; there were no adverse effects or discomfort reported in the questionnaire, which was added following the ultrasonographic investigation. The r2 (r is the Pearson correlation coefficient) of the BonAge ultrasound measurement and the G&P method of the left hand was 0.82 and the r2 of the BonAge and the G&P method of the distal radius and ulna alone was 0.86. The averaged accuracy (i.e. absolute difference in years between G&P reading and BonAge ultrasonic results) was calculated. Results were similar for boys and for girls—for the whole left hand 1.0±0.8 and for the distal radius 0.8±0.7 for boys and 0.9±0.7 for the girls (Table 1). On average, the difference between BonAge and CA was the same as the difference between G&P and CA, i.e. 1.4 years. In 28 (43%) cases out of 65, the difference between BonAge and G&P was greater than 1 year. However, in 95.4% of the subjects, the difference between BonAge and the whole left hand G&P estimation was within ±2 SD, i.e. ±2.6 years. A similar figure (96.9%) was obtained for the difference between BonAge and G&P bone age using the radius and ulna alone. In eight cases, both methods showed precocious values, but the difference between BonAge and the CA was larger than the difference between G&P and CA. In 15 of these 28 patients the BonAge and G&P methods showed the same trend (9 cases of precocious development and 6 cases of growth retardation), but in all cases the BonAge was further from the CA than G&P. In five cases, BonAge gave a result in the opposite direction to G&P and in two further cases, G&P gave an advanced bone age while BonAge was the same as the CA.
Discussion
There is an increasing interest for age estimations in living individuals. Bone age assessment is a valuable adjunct in clinical practice to provide more accurate information about developmental status and growth derangements in children and young adults than can be inferred from height, weight and age alone [13, 14]. At least 5% of children and adolescents undergo bone age assessment for several reasons, including short stature or growth abnormalities. These children have their skeletal maturity assessed as part of assessment of growth development. For children who are receiving growing hormone therapy, bone age estimation is used for monitoring the effects of therapy, and many follow-up examinations may be necessary. Among the many methods proposed for assessing skeletal maturity, those of G&P [2] and of TW2 [9], using radiographs of the left hand and wrist are most commonly used in clinical practice. As described above, the G&P method is easy and quick but subjective, whereas the TW2 method is more accurate and flexible, but time-consuming and difficult to perform. The reported 95% confidence interval for bone age from hand radiographs ranges from 0.6–0.9 years for early childhood and 2.1–2.8 years for later childhood, to 1.8–2.5 years for adolescence [5]. During adolescence and in the third decade of life, evaluation of skeletal age is undertaken from estimation of the appearance and fusion of the epiphyses of long bones and pelvis [15]. Not all epiphyses are of equal value in estimating skeletal age; the best indicators are proximal humerus, distal radius, femoral head, iliac crest, and medial clavicle.
In our study, sonographic evaluation using the BonAge method was performed in the region of the distal radius. The aim was to compare the results of this new sonographic technique with the established G&P method using a radiograph of the left hand and wrist. This method is based on the observation that maturation of an epiphysis, by virtue of enchondral ossification, is strongly related to systemic bone development. In the radius and ulna, as in other long bones, the development process begins with the appearance of ossification of the diaphysis, followed by ossification centres in the epiphyses and the formation of the physeal growth plates. The end of growth is marked by fusion of the growth plates. The impedance characteristics of cartilage differ from those of calcified bone, so ultrasound is conducted at different velocities through cartilage and calcified bone. The velocity of an ultrasound wave through cartilage is approximately 1,700 m/s, whereas it may reach values in the range of 2,200–4,500 m/s in calcified bone. If an ultrasound wave is transmitted through the epiphyses before the appearance of the centre of ossification, the resulting speed will be close to the speed of sound through cartilage. With the appearance of the centre of ossification and its subsequent growth, the velocity will increase until growth is complete. The velocity change depends on two processes: the physical size of the centre of ossification and its increasing density. Thus, the velocity of the ultrasound wave increases as the skeletal age of the patient increases. Exact positioning of the wrist during the scanning process is necessary to avoid mistakes in evaluation. Especially, for follow-up investigations it seems necessary to have a consistent point of measurement. This is one of the critical features of the BonAge system.
Our data suggest that the BonAge system has the capacity to produce accurate results. There was good correlation between the data from this system and the analysis according to the G&P method by a blinded paediatric radiologist. There were no significant differences between the results in girls and boys. The difference between the CA and the BonAge was the same as the difference between the CA and the G&P analysis. In particular, if we used the G&P atlas to estimate bone age using the distal radius and ulna only, the difference was very small (0.84 years for boys, 0.89 years for girls). However, in some cases there were greater differences. Thus, especially in patients with precocious development, we observed that the skeletal age estimated by the BonAge system was more advanced than the age evaluated by the G&P method. One possible explanation for this is that the increase of the speed of sound can be detected by the BonAge system earlier than can be identified from radiographs. However, we do not have an explanation for the other cases where the BonAge result was in the opposite direction to the G&P method.
We suggest that the BonAge system is an easily performed technique for the accurate estimation of skeletal age. A disadvantage is that children younger than 5 years of age cannot be analysed because the database includes only children older than 5 years. The reason for this is that the sonographic examination requires a degree of co-operation from the child, who is required to keep the arm still during the measurement. The method can theoretically be used for children younger than 5 years of age, and we would like to expand the target population in the future. However, most skeletal age assessment in clinical practice is undertaken on children between the ages of 5 years and 18 years. Other sonographic-based techniques such as the ultrasonographic version of the G&P atlas established by Bilgili et al. [12] are available, but are time consuming.
In conclusion, the BonAge device demonstrates the ability of ultrasound to produce an accurate assessment of skeletal age. The results are highly correlated with conventional skeletal age evaluation using the G&P method. Obvious advantages of the ultrasound device are objectivity, lack of ionizing radiation, and easy accessibility. Thus, this sonography-based technique may be a possible alternative to conventional methods for the assessment of skeletal age.
References
Poland J (1898) Skiagrapic atlas showing the development of bone of the wrist and hand. Smith Elder, London
Greulich WW, Pyle SI (1959) Radiographic atlas of skeletal development of the hand and wrist. Stanford University Press, Stanford
Buckler JM (1983) How to make the most of bone ages. Arch Dis Child 58:761–763
Loder RT, Estle DT, Morrison K, et al (1993) Applicability of the Greulich and Pyle skeletal age standards to black and white children of today. Am J Dis Child 147:1329–1333
Ontell FK, Ivanovic M, Ablin DS, et al (1996) Bone age in children of diverse ethnicity. AJR 167:1395–1398
Jimenez-Castellanos J, Carmona A, Catalina-Herrera CJ, et al (1996) Skeletal maturation of wrist and hand ossification centers in normal Spanish boys and girls: a study using the Greulich and Pyle method. Acta Anat (Basel) 155:206–211
Groell R, Lindbichler F, Riepl T, et al (1999) The reliability of bone age determination in central European children using the Greulich and Pyle method. Br J Radiol 72:461–464
van Rijn RR, Lequin MH, Robben SG, et al (2001) Is the Greulich and Pyle atlas still valid for Dutch Caucasian children today? Pediatr Radiol 31:748–752
Tanner JM, Whitehouse RH, Marshall WA, et al (1975) Assessment of skeletal maturity and prediction of adult height (TW2 method). Academic, New York
Castriota-Scanderbeg A, De Micheli V (1995) Ultrasound of femoral head cartilage: a new method of assessing bone age. Skeletal Radiol 24:197–200
Wagner UA, Diedrich V, Schmitt O (1995) Determination of skeletal maturity by ultrasound: a preliminary report. Skeletal Radiol 24:417–420
Bilgili Y, Hizel S, Kara SA, et al (2003) Accuracy of skeletal age assessment in children from birth to 6 years of age with the ultrasonographic version of the Greulich-Pyle atlas. J Ultrasound Med 22:683–690
Megremis S, Cavallo G, Michalakou M, et al (2004) Assessment of skeletal age with hand and wrist sonography: could a standardised method replace radiography? Eur Radiol 14:S514
Castriota-Scanderbeg A, Sacco MC, Emberti-Gialloreti L, et al (1998) Skeletal age assessment in children and young adults: comparison between a newly developed sonographic method and conventional methods. Skeletal Radiol 27:271–277
Kreitner KF, Schweden FJ, Riepert T, et al (1998) Bone age determination based on the study of the medial extremity of the clavicle. Eur Radiol 8:1116–1122
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mentzel, HJ., Vilser, C., Eulenstein, M. et al. Assessment of skeletal age at the wrist in children with a new ultrasound device. Pediatr Radiol 35, 429–433 (2005). https://doi.org/10.1007/s00247-004-1385-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-004-1385-3