
Abstract
Background
The diagnosis of intestinal malrotation is based on an upper gastrointestinal contrast series (UGI), which is considered the imaging reference standard. It may however be challenging even for experienced paediatric radiologists.
Objective
The purpose of this study was to demonstrate the agreement between UGI and US in assessing the position of the third portion of the duodenum (D3) and to show that a retroperitoneal duodenum indicates normal forgut rotation.
Materials and methods
In a prospective study, US assessment of the duodenum and the superior mesenteric vessels was performed in consecutive children who were referred for clinically indicated UGI at a single institution.
Results
Eighty-five children, 5 months to 14 years old, were studied. In 82/85 (96%), both US and UGI suggested normal forgut rotation. In three children, US demonstrated a normal position of the D3 whereas UGI showed an abnormal position of the duodeno-jejunal junction.
Conclusion
US is a non-invasive, easily performed technique for excluding malrotation. UGI may be reserved for situations where US does not demonstrate a normal position of the D3.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The diagnosis of intestinal malrotation based on an upper gastrointestinal contrast series (UGI), which has long been viewed as the gold standard imaging method, may be challenging even for experienced radiologists [1–12]. Since the late 1980s, several sonographic approaches have been proposed for excluding intestinal malrotation. The most widely studied criterion has been the superior mesenteric vascular relations [3, 4, 9, 12]. If the superior mesenteric vein (SMV) is not to the right of the superior mesenteric artery (SMA) in the axial plane at the level of the junction of the SMV with the portal vein, the findings are highly sensitive for intestinal malrotation, except if the vein is anterior to the artery [3, 4, 12]. However, inversion of the SMA and SMV may be present in normal rotation and a normal relationship may be present in children with abnormal rotation [13]. Others have considered the whirlpool sign highly sensitive for malrotation on US [14, 15].
Our experience suggests that the position of the duodenum and superior mesenteric vessels can easily be depicted by US.
More recently, based on anatomical and embryological principles, Yousefzadeh [16] suggested that a retroperitoneal third portion of the duodenum (D3) between the aorta and the SMA is an indicator for normal rotation [16]. The technical feasibility of this assessment has been demonstrated in newborns by the same author [17].
Our study had three purposes: (1) to assess the feasibility of US demonstration of a retromesenteric D3 in children 5 months to 14 years old, (2) to compare the ability of US and UGI in indicating and excluding malrotation and (3) to prove that the retromesenteric position of D3 or lack thereof represent normal and abnormal rotation, respectively, of the primitive gut during embryonic development. This is the first study to correlate US findings with findings on UGI in the assessment of forgut rotation.
Materials and methods
Using a Philips iU22 US system (Philips, Bothell, WA, USA) and high-resolution linear (L12-5) and curvilinear (C9-4) transducers, US was prospectively performed to assess the position of D3. The study was performed between April 2008 and April 2011 in consecutive children who had undergone UGI before an anti-reflux procedure or gastrostomy tube placement or with recurrent respiratory tract infection possibly related to gastroesophageal reflux. None was excluded from the study. The US parameters included feasibility of demonstration of the D3 between the SMA and the abdominal aorta, and the position of the SMV in relation to the SMA on the clock face model with the vein located to the right of the artery referred to as 9 o’clock and in front of the artery as 12 o’clock.
Transverse and sagittal images of the aortomesenteric angle were aided by applying gradual compression. The D3 was identified by its course around the head of the pancreas and by its proximity to the uncinate process.
UGI and US were consecutively performed by two senior paediatric radiologists (M.R., 11 years’ experience in paediatric radiology; C.P., 25 years’ experience in paediatric radiology). The US operator was masked to the results of the UGI throughout the studies.
Residual barium was not an obstacle for the depiction of D3 but rather helpful for the US follow-through of the duodenal anatomy. However, in our previous experience, gradual compression without filling of the stomach has been equally feasible.
On UGI, to prevent the duodenum to be masked by the more-distal contrast-filled small bowel loops, a straight frontal view of the first passage of the barium through the duodenum was captured. On UGI, the position of the duodeno-jejunal junction was considered normal only if it was located to the left of the left vertebral pedicle, at the level of the inferior margin of the duodenal bulb [11, 18]. Lateral views were systematically used to assess the posterior position of the D3.
Informed consent was obtained from parents for each patient and the study protocol was approved by an institutional review board.
Results
Eighty-five children were included. The male/female ratio was 47/38, and children ranged from 5 months to 14 years of age.
Position of the third portion of the duodenum
US demonstrated the aorto-mesenteric angle, the SMV/SMA orientation and at least the first centimetre of the SMA in all 85 children. The UGI/US correlation is shown in Table 1.
In 79/85 (93%) children, US displayed the D3 between the SMA and the aorta and UGI demonstrated a normal duodenal sweep and position of the duodeno-jejunal junction (DJJ) (Fig. 1).

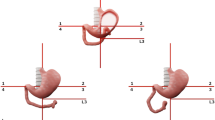
Normal imaging findings in a 30-month-old girl. a US demonstrates the third portion of the duodenum (D3) between the superior mesenteric artery (A) and vein (V), and the aorta (AO). JV jejunal vein. b Upper gastrointestinal contrast study demonstrates a normal course of the D3 and a normal site of the duodeno-jejunal flexure (DJJ)
In three children with a history of surgery for gastroschisis, omphalocele or Ladd procedure for intestinal malrotation, the D3 was not situated between the SMA and the aorta on US and UGI showed an abnormal position of the D3 and the DJJ.
In the remaining 3/85 (3.5%) children, US demonstrated a normal position of the D3 whereas UGI showed an abnormal position of the DJJ, medial and anterior to the spine in two and to the right of the spine in one. It was located at the level of the inferior margin of the duodenal bulb in all three. Two of these three children had a severe spinal left-convex curvature (Fig. 2). The third had normally related superior mesenteric vessels situated to the right of the aorta (Fig. 3).

Upper gastrointestinal contrast study (UGI) and US in a 12-year-old boy. a Due to scoliosis, the duodeno-jejunal flexure (DJJ) does not reach the left vertebral pedicles on UGI, which may be interpreted as malrotation. b US shows a normal position of the third portion of the duodenum (D3), suggesting normal rotation

Upper gastrointestinal contrast study (UGI) and US in a 20-month-old boy. a The duodeno-jejunal flexure (DJJ) does not reach the left pedicle on UGI. b US shows a normal position of D3, suggestive of normal rotation. The superior mesenteric vessels are seen to the right of the aorta. UP uncinate process of the pancreas
Superior mesenteric vascular relationship
Figure 4 shows the histogram of the SMV/SMA relationship in the 80/85 (94%) patients with a normal duodenum position for UGI and US on the clock-face model. In 77/80 (96%) of these, the SMV was identified to the right of the SMA, between 7 and 11 o’clock. In the remaining 3/80 (4%), one had an SMV posterior to the SMA (6 o’clock), one anterior to SMA (12 o’clock) and one to the left of the SMA (4 o’clock). In these three children, the position of the D3 on US and the position of the DJJ on UGI were undoubtedly both normal according to our criteria.

The superior mesenteric vein/superior mesenteric artery (SMV/SMA) relationship in 79/85 children with a normal duodenal position on upper gastrointestinal contrast study (UGI) and US. X-axis: Position of the SMV relative to the SMA on a clock-face model with the clock facing inferiorly, so that 9 signifies a 9 o’clock-position, i.e. SMV to the right of the SMV. Y-axis: number of children
For the three children with abnormal duodenum position suggested by both techniques, the SMV was situated in front of the artery in one child (12 o’clock) and to the left of the artery in two children (2 and 4 o’clock).
In all three children with a normal position of D3 on US and abnormal or questionable on UGI, the position of the SMV was to the right of the SMA (9 o’clock).
Over the three years of the study, we encountered three additional patients: one girl (17 months old) and a boy (12 years old) with symptoms of recurrent vomiting and abdominal pain, and a one-day old with atrio-ventricular canal defect in whom the D3 was not demonstrable in the aorto-mesenteric angle. The SMV was situated at the 11 o’clock position in one patient (Fig. 5) and to the left of the SMA at the 3 o’clock position in the other two. In these three patients UGI confirmed the abnormal position of the D3 and DJJ (Fig. 6). In the newborn, dilatation of the stomach and the proximal duodenum suggested duodenal atresia. Surgery confirmed the malrotation in the 17-month-old girl and in the 12-year-old boy, and nonrotation associated with duodenal atresia was confirmed in the newborn.

US in a 17-month-old girl. Although there is no inversion of the superior mesenteric vein/superior mesenteric artery (SMV/SMA) relationship, the duodenum does not run between the SMA and the aorta

Upper gastointestinal contrast study in same child as in Fig. 5. The duodenum and proximal jejunal loops lie to the right of the midline without a clearly outlined duodeno-jejunal flexure (DJJ), suggesting malrotation
Discussion
Successful sonographic visualization of the aorta, the SMA and the aorto-mesenteric angle in all children in the study demonstrates the feasibility of the technique in children up to 15 years old, extending well beyond the immediate postnatal age group previously demonstrated [17].
Among 79 children with a normal position of the D3 and DJJ on UGI, US demonstrated a normally sited D3 between the SMA and the aorta with no false positive, similar to what has previously been shown in newborns [17]. In the three children whose duodenum was not retromesenteric on US, UGI met the published criteria for malrotation on the frontal view. In these three children, an unusual relationship between the SMV and the SMA strongly suggested intestinal malrotation. In three false-positive studies with questionable positions of the DJJ on UGI, US showed rightwards displacement of the D3 but with a retromesenteric position between the SMA and the aorta. In two of these three children, the abnormal duodenal position on UGI was associated with severe scoliosis. In the third child, who has a normal spine, the SMA was shifted rightwards and truncated with the SMV in a normal 9 o’clock position.
In children with an abnormal position of the duodenum and DJJ on UGI, the aorto-mesenteric angle, the SMA and the aorta were clearly visualised without the duodenum passing in between.
In three children, abnormal SMA/SMV relationships were not correlated with an abnormal position of the duodenum on UGI. Demonstration of the D3 between the SMA and the aorta by US is clinically feasible, and seems to obviate other imaging studies or surgical exploration to exclude malrotation.
Recently, Taylor [19] reviewed abdominal CTs in 100 normal subjects and in 38 children with surgically proven malrotation and demonstrated the position of the D3 between the SMA and the aorta in all studies of normally rotated gut without any false-positive findings. In his group of 38 children with surgically proven malrotation, only one had a normally positioned D3. We fully agree with Yousefzadeh’s [20] expressed reservations regarding the use of CT. Based on embryological and anatomical principles we believe US is the modality of choice to assess the position of the D3 for indicating or excluding malrotation with high accuracy.
One of the limitations of our study is the low rate of abnormal rotation. A prospective series with more symptomatic patients and a higher frequency of malrotation is required to validate our findings. Another limitation was the lack of a reference standard to confirm the normal rotation in children with abnormal UGI and normal US; however, none of these children was clinically suspected to have malrotation.
Conclusion
Using a graded compression-technique, demonstrating the D3 between the SMA and aorta is feasible in children up to 15 years old. Based on anatomical and embryological arguments, a retromesenteric D3 excludes intestinal malrotation. Non-depiction of the D3 between the SMA and the aorta correlated well with an abnormal position of the DJJ on UGI in our study, but the frequency of abnormal findings was low. US is suggested as the initial modality of choice to assess for malrotation, depending on the limitations posed by the child’s body habitus. UGI may be reserved for those in whom US is not feasible, or when a retromesenteric D3 cannot be demonstrated by US.
References
Yousefzadeh DK, Soper RT, Jackson JH Jr (1980) Diagnostic advantages of manual compression fluoroscopy in the radiologic work-up of vomiting neonates. J Pediatr Surg 15:270–278
Katz ME, Siegel MJ, Shackelford GD et al (1987) The position and mobility of the duodenum in children. AJR 148:947–951
Loyer E, Eggli KD (1989) Sonographic evaluation of superior mesenteric vascular relationship in malrotation. Pediatr Radiol 19:173–175
Dufour D, Delaet MH, Dassonville M et al (1992) Midgut malrotation, the reliability of sonographic diagnosis. Pediatr Radiol 22:21–23
Millar AJ, Rode H, Brown RA et al (1987) The deadly vomit: malrotation and midgut volvulus. A review of 137 cases. Pediatr Surg Int 2:172–174
Rescorla FJ, Shedd FJ, Grosfeld JL et al (1990) Anomalies of intestinal rotation in childhood: analysis of 447 cases. Surgery 108:710–715
Long FR, Kramer SS, Markowitz RI et al (1996) Intestinal malrotation in children: tutorial on radiographic diagnosis in difficult cases. Radiology 198:775–780
Dilley AV, Pereira J, Shi EC et al (2000) The radiologist says malrotation: does the surgeon operate? Pediatr Surg Int 16:45–49
Ashley LM, Allen S, Teele RL (2001) A normal sonogram does not exclude malrotation. Pediatr Radiol 31:354–356
Strouse PJ (2004) Disorders of intestinal rotation and fixation ("malrotation"). Pediatr Radiol 34:837–851
Applegate KE, Anderson JM, Klatte EC (2006) Intestinal malrotation in children: a problem-solving approach to the upper gastrointestinal series. Radiographics 26:1485–1500
Orzech N, Navarro OM, Langer JC (2006) Is ultrasonography a good screening test for intestinal malrotation? J Pediatr Surg 41:1005–1009
Daneman A (2009) Malrotation: the balance of evidence. Pediatr Radiol 39(Suppl 2):S164–S166
Pracros JP, Sann L, Genin G et al (1992) Ultrasound diagnosis of midgut volvulus: the "whirlpool" sign. Pediatr Radiol 22(1):18–20
Shimanuki Y, Aihara T et al (1996) Clockwise whirlpool sign at color Doppler US: an objective and definite sign of midgut volvulus. Radiology 199(1):261–264
Yousefzadeh DK (2009) The position of the duodenojejunal junction: the wrong horse to bet on in diagnosing or excluding malrotation. Pediatr Radiol 39(Suppl 2):S172–S177
Yousefzadeh DK, Kang L, Tessicini L (2010) Assessment of retromesenteric position of the third portion of the duodenum: an US feasibility study in 33 newborns. Pediatr Radiol 40:1476–1484
Applegate KE (2009) Evidence-based diagnosis of malrotation and volvulus. Pediatr Radiol 39(Suppl 2):S161–S163
Taylor GA (2011) CT appearance of the duodenum and mesenteric vessels in children with normal and abnormal bowel. Pediatr Radiol 41:1378–1383
Yousefzadeh DK (2011) Regarding online publication of ‘CT appearance of the duodenum and mesenteric vessels in children with normal and abnormal bowel’. Pediatr Radiol 41:1481–1482
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Menten, R., Reding, R., Godding, V. et al. Sonographic assessment of the retroperitoneal position of the third portion of the duodenum: an indicator of normal intestinal rotation. Pediatr Radiol 42, 941–945 (2012). https://doi.org/10.1007/s00247-012-2403-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-012-2403-5