
Abstract
We describe a case of Gomez-Lopez-Hernandez syndrome in an 18-month-old boy. Imaging findings included rhombencephalosynapsis with a single dentate nucleus. In addition, MR angiography revealed an azygous anterior cerebral artery. The clinical presentation, MRI findings and pathogenesis are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gomez-Lopez-Hernandez (GLH) syndrome, or cerebello-trigeminal-dermal dysplasia, is a rare condition characterized by the triad of parietal alopecia, trigeminal anesthesia and rhombencephalosynapsis. Rhombencephalosynapsis is a cerebellar anomaly characterized by fusion of the cerebellar hemispheres and absence of the cerebellar vermis.
Case report
An 18-month-old Asian-Indian boy presented with a history of delayed milestones. The child was not able to walk or speak. He was the first-born child of a non-consanguineous couple. The labor was an uncomplicated spontaneous vaginal delivery. He was noted to have dysmorphic features including midfacial hypoplasia and symmetric, bilateral bands of temporal alopecia (Fig. 1). The parents reported jerky side-to-side movements of the head. No seizure activity was noted. However, bilateral trigeminal anesthesia was noted. The child had no signs of any neurocutaneous stigmata and possessed no obvious cardiovascular, respiratory, genitourinary or musculoskeletal abnormalities.

Right temporal alopecia
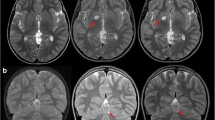
MR imaging demonstrated fusion of the cerebellar hemispheres with midline fusion of the folia and interfoliate sulci involving both the gray and white matter, consistent with rhombencephalosynapsis (Fig. 2). The single dentate nucleus was horseshoe-shaped, with midline fusion and an absent posterior cerebellar notch. The vallecula was present; however, the primary fissure of the cerebellum was absent. The vermis was absent or severely hypoplastic. The fourth ventricle was narrow and keyhole-shaped with upward rounding of the fastigial recesses on sagittal sections. The supratentorial brain was normal; however, MR angiography revealed a single anterior cerebral artery (ACA), consistent with an azygous ACA (Fig. 3). Although this finding could be a coincidence, previous studies have not included detailed vascular studies; therefore, this fusion anomaly could represent an expansion of the phenotype.

MRI. Axial (a) and coronal (b) T1- weighted and axial T2-weighted (c) MR images demonstrate absence of the vermis and fusion of the cerebellar hemispheres involving the gray and white matter (large arrow) and a single dentate nucleus (pointed arrow)

MR angiography. 3-D time-of-flight, base (a) and sagittal oblique (b) projections demonstrate an azygous anterior cerebral artery (arrow)
Discussion
Gomez [1] reported the first case of cerebello-trigeminal-dermal dysplasia (later called Gomez-Lopez-Hernandez syndrome) in 1979, and in 1982 Lopez-Hernandez reported two more cases [2]. In all, ten such cases have been reported in the literature, of which five children were of Brazilian origin [3–5]. The prominent characteristics of the syndrome include the triad of midline rhombencephalosynapsis, trigeminal anesthesia and bilateral bands of temporal alopecia [4]; however, various supratentorial parenchymal fusion anomalies have been reported. Phenotypic manifestations include midfacial hypoplasia, oxycephaly, short stature, delayed motor development, variable mental retardation, low-set ears, fifth-finger clinodactyly, ataxia, scarring of the face [4], and psychiatric difficulties [1].
MR imaging findings typically include rhombencephalosynapsis, with an atretic keyhole-shaped fourth ventricle, vermian agenesis and midline dentate fusion. The occipital horns are distended, with thinning of the posterior periventricular white matter [4]. In our patient, MR angiography revealed an azygous ACA. None of the previous patients have shown an azygous ACA on MR angiography. This could be an incidental finding, as an azygous ACA is known to be a normal variant, or MR angiography might not have been pursued or reported in the other cases. As stated by Lopez-Hernandez, poor motor development with ataxia is likely attributable to the cerebellar malformation, whereas trigeminal anesthesia implies partial or complete absence of the spinal trigeminal nucleus [2].
The diagnosis of this syndrome is based on identifying the triad of rhombencephalosynapsis, trigeminal nerve anesthesia and the parietal alopecia. Whenever a prenatal diagnosis of rhombencephalosynapsis is made, a postnatal review of the clinical findings is essential in order to exclude this syndrome [5].
The etiology of this syndrome is likely genetic in nature. This is corroborated by the fact that all reported cases have been sporadic. According to Patel and Barkovich [6], the initial defect in rhombencephalosynapsis is likely a result of the failure of induction of midline structures, not failure of fusion [6]. In cerebellar development, the isthmic organizer, a strip of neuroepithelium between the mesencephalon and metencephalon, helps guide the development of midline cerebellar structures [7]. Failure to induce the midline structures could be caused by the failure of patterning centers to express, or to express sufficient levels of, appropriate growth factors such as FGF8 [6] or various homeobox-containing factors or signaling molecules [7].
The treatment of Gomez-Lopez-Hernandez syndrome is still developing. Currently, it is supportive, including the treatment of comorbidities such as psychiatric problems [1] and the use of physical therapy to assist in motor control and development.
In conclusion, we report a case of Gomez-Lopez-Hernandez syndrome in an 18-month-old boy who had the triad of rhombencephalosynapsis, trigeminal anesthesia and bilateral bands of temporal alopecia. An additional finding in our patient was that of an azygous ACA, which could be an incidental finding, although an association with the syndrome is possible and needs to be explored.
References
Gomez MR (1979) Cerebello-trigeminal and focal dermal dysplasia: a newly recognized neurocutaneous syndrome. Brain Dev 1:253–256
Lopez-Hernandez A (1982) Craniosynostosis, ataxia, trigeminal anesthesia and parietal alopecia with pons-vermis fusion anomaly (atresia of the fourth ventricle). Neuropediatrics 13:99–102
Brocks D, Irons M, Sadeghi-Najad A, et al (2000) Gomez-Lopez-Hernandez syndrome: expansion of the phenotype. Am J Med Genet 94:405–408
Munoz M, Santos A, Graziadio C, et al (1997) Cerebello-trigeminal-dermal dysplasia (Gomez-Lopez-Hernandez syndrome): description of three new cases and review. Am J Med Genet 72:34–39
Tan TY, McGillivray G, Goergen SK, et al (2005) Prenatal magnetic resonance imaging in Gomez-Lopez-Hernandez syndrome and review of the literature. Am J Med Genet A 138:369–373
Patel S, Barkovich AJ (2002) Analysis and classification of cerebellar malformations. AJNR 23:1074–1087
Yachnis AT (2002) Rhombencephalosynapsis with massive hydrocephalus: case report and pathogenetic considerations. Acta Neuropathol 103:301–304
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Whetsell, W., Saigal, G. & Godinho, S. Gomez-Lopez-Hernandez syndrome. Pediatr Radiol 36, 552–554 (2006). https://doi.org/10.1007/s00247-006-0150-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-006-0150-1