
Abstract
The two main theories regarding the pathogenesis of coarctation of the aorta are the Skodaic hypothesis of ductal tissue constricting the aorta at the level of the insertion of the ductus arteriosus and the flow theory of decreased ascending aortic blood flow in the fetus, which results in associated isthmic narrowing and a localized shelf. To document that ectopic ductal tissue constriction can cause coarctation of the aorta in the absence of a patent ductus arteriosus, we report three cases of infants presenting with critical coarctation who responded to prostaglandin E1 infusion without opening the ductus arteriosus.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The role of the ductus arteriosus in the pathogenesis of coarctation of the aorta (CoA) has been supported by the presence of ectopic ducal tissue in the aorta at the level of the isthmus (Skodaic hypothesis) [7]. An alternative mechanism postulated for the development of coarctation involves abnormal fetal hemodynamics explaining the association of coarctation with other left-sided obstructive lesions, especially the frequent presence of a bicuspid aortic valve [4]. Both mechanisms may play a role in the etiology of the lesion. Although there is clear anatomic evidence of an infolding of the dorsal aortic wall opposite the ductus arteriosus in patients with CoA [8, 10], the additive role of ductal constriction cannot be underestimated in neonates with critical coarctation. Prostaglandin E1 is routinely used to relieve the aortic obstruction by reopening the ductus arteriosus. To support the theory that ectopic ductal tissue constriction also contributes to the development of coarctation, we report three cases of infants presenting with critical CoA who responded to prostaglandin E1 infusion without opening the ductus arteriosus.
Case Reports
Case 1
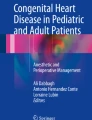
A full-term male was noted to have decreased femoral pulses at 2 days of life during a predischarge physical exam. The heart rate was 140 beats per minute (bpm), and blood pressure was 70/59 mmHg in the right arm and 40/20 mmHg in the left leg. A grade I/VI systolic murmur was audible at the left sternal border. The infant was well perfused and in no respiratory distress. The remainder of the physical exam was unremarkable. A two-dimensional echocardiogram demonstrated CoA with a posterior shelf in the juxtaductal area, with turbulent blood flow. The descending aorta flow profile showed a typical narrowed pulse pressure pattern (Fig. 1A). The aortic valve was normal, as was ventricular function. A patent ductus arteriosus was not visualized. The infant was initially treated with prostaglandin E1 infusion at 0.05 µg/kg/min and then the dose was increased to 0.2 µg/kg/min. No inotropic medications were administered. Subsequently, the femoral pulses improved and there was resolution of the blood pressure gradient between the upper and lower extremities. A repeat echocardiogram demonstrated no significant acceleration of color Doppler flow across the juxtaducatal region and pulsatile flow profile in the descending aorta (Fig. 1B). Again, no patent ductus arteriosus was visualized. The infant underwent repair of the coarctation with an extended end-to-end anastomosis. The ductus arteriosus was noted to be barely open despite the use of prostaglandin E1.

Doppler interrogation of the descending aorta. (A) Narrow pulse pressure pattern before prostaglandin E1 infusion. (B) Improved, pulsatile flow after initiation of prostaglandin E1.
Case 2
A 3-week-old female infant was brought to the emergency room because of respiratory distress. She was a full-term infant who had been doing well until 2 days prior to admission when she started to have decreased oral intake and increased respiratory rate. In the emergency room of the referring hospital, the infant was dusky with poor perfusion, in severe respiratory distress, and unresponsive to stimulation. The initial blood gas demonstrated severe metabolic acidosis with a pH of 6.9. The patient was intubated and ventilated. She received volume expansion and bicarbonate and was treated with dopamine and dobutamine through an intraosseous line. A chest x-ray demonstrated moderate cardiomegaly. A two-dimensional echocardiogram demonstrated a juxtaductal CoA (Fig. 2A) and a moderate-sized subaortic ventricular septal defect. The ductus arteriosus was not patent and the aortic valve was normal. Shortening fraction was 28%. She was treated with a 0.1 µg/kg/min prostaglandin E1 infusion and transported to our institution. On admission, the heart rate was 142 bpm; there was a 20- to 30-mmHg gradient between the right arm and the legs. The femoral pulses were palpable but decreased. Arterial oxygen saturation was 100% pre- and postductaly; pH was 7.3. The serum creatinine and liver enzymes were elevated. A repeat two-dimensional echocardiogram confirmed the anatomy with improved flow across the aortic arch compared to the first study; a patent ductus was not present (Fig. 2B). The infant was managed medically with prostaglandin E1, dopamine, and diuretics. Five days later, when renal and liver functions were normalized, an end-to-end coarctation repair was performed. The ligamentum arteriosum was ligated and ductal tissue of the isthmus was removed. The ventricular septal defect was not repaired.

Two-dimensional echocardiogram from the suprasternal view. (A) Demonstration of juxtaductal CoA. (B) Improved diameter of the juxtaductal area after initiation of prostaglandin E1 infusion.
Case 3
A 7-week-old female infant was brought to an outside emergency room because of decreased feedings, vomiting, respiratory distress, and cool extremities for 2 days. She was born at full term. Since 2 weeks of age, the infant had not been eating as well as the twin sister. On exam, the infant was noted to be cool peripherally, with capillary refill >3 seconds. The heart rate was 168 bpm, and blood pressure was 77/48 mmHg in the right arm and 37/21 mmHg in the right leg. Femoral pulses were not palpable. A III/VI holosystolic murmur was heard at the apex. The liver was palpable 3 cm below the costal margin. Initial evaluation demonstrated metabolic acidosis with a pH of 7.25 and a base deficit of −17. A chest x-ray demonstrated moderate cardiomegaly and pulmonary edema. The infant received intravenous fluids and bicarbonate; she was intubated and mechanically ventilated. Dopamine was administered at 10 µg/kg/min. A two-dimensional echocardiogram showed a discrete juxtaductal coarctation, decreased left ventricular function, moderate mitral valve regurgitation, and no patent ductus arteriosus. The aortic valve was trileaflet. She was started on prostaglandin E1 at 0.2 µg/kg/min and transferred to our institution.
On arrival, at physical examination the heart rate was 160 bpm, and blood pressure was 78/45 mmHg in the right arm and 61/45 mmHg in the right leg. The femoral pulses were palpable but decreased, and the acidosis had been corrected. A repeat two-dimensional echocardiogram demonstrated increased flow across the juxtaductal region with no patent ductus arteriosus. On the following morning, the coarctation was repaired with end-to-end anastomosis, and ligamentum arteriosus was divided.
Discussion
Coarctation of the aorta is a common congenital heart lesion, but it is a rare finding in congenital heart defects associated with decreased pulmonary blood flow and normal or increased aortic blood flow [12]. In contrast, in lesions with obviously decreased aortic isthmus flow, there is a high incidence of CoA [4, 8, 10]. These findings support the hemodynamic theory of reduced antegrade aortic flow that has been proposed to explain the clinical features of patients with CoA, such as isthmal narrowing, a localized juxtaductal shelf, bicuspid aortic valve, and other associated left heart obstructive lesions [4]. However, a dynamic postnatal process, probably ductal closure, may be responsible for the onset of obstruction. In most cases, infusion of prostaglandin E1 reopens the ductus arteriosus and relieves the obstruction.
The concept that ectopic ductal tissue is present in the aorta and its constriction produces the localized lesion was first illustrated by Skoda in 1855 and has persisted through the years (Skodaic theory). Histological studies demonstrated that ductal tissue comprised a substantial portion of the coarctation lesion and completely surrounded the aortic lumen [7]. Ductal tissue patterns were analyzed by Russell et al. [11] in 23 infants who were operated on for CoA. A circumferential sling of ductal tissue was identified in 22 of the 23 patients. In the remaining patient, the obstruction was due to long tubular hypoplasia.
This report describes three infants who presented at 2 days and 3 and 7 weeks of life, respectively, with aortic coarctation. There was significant hemodynamic improvement after initiation of prostaglandin E1 infusion, despite the absence of a patent ductus arteriosus. This implies that ductal tissue relaxation in the area of coarctation, and not simply opening the ductus arteriosus, relieves the obstruction. Subsequently, complete or almost complete closure of the ductus was confirmed during surgery.
The typical response to prostaglandin E1 in infants with CoA is to open the ductus arteriosus and thereby improve flow across the narrowed coarctation site. Severe coarctation in infants is often a ductal-dependent lesion, and relief of obstruction depends on patency of the ductus arteriosus. In the three patients described here, relief of the obstruction was obtained with prostaglandin E1 without simultaneous opening of the ductus arteriosus. These patients can be recognized as having a “prostaglandin-dependent” coarctation [2].
Callahan et al. [1] reported a case of a 9-day-old infant with CoA and a 20-mmHg arm-to-leg blood pressure gradient who responded to a prostaglandin E1 infusion with resolution of the gradient without evidence of a patent ductus arteriosus. Hascoët et al. [5] reported a case of a very low-birth-weight infant (900 g) whose ductus arteriosus had previously been ligated and later developed CoA with signs of congestive heart failure. Prostaglandin E1 infusion resulted in improvement of femoral pulses. The infant was able to grow until surgical repair could be performed. The authors suggested that the beneficial effect of prostaglandin E1 in this patient was secondary to relaxation of ductal tissue in the aorta.
The effect of prostaglandin E1 has been determined to be greater when used in patients younger than 96 hours old; the decreased response in older patients suggests that anatomic closure of the ductus arteriosus has occurred [3]. However, there have been reported cases of a “late” effect of prostaglandin E1 on the ductus arteriosus [6, 9]. In one of our patients, the effect of prostaglandin E1 on ductal tissue was seen at 7 weeks of age, even with complete anatomical closure of the ductus.
Although it could be suggested that the clinical improvement in the three patients reported here was secondary to the use of inotropic support and mechanical ventilation, the increase in aortic caliber at the site of the coarctation area (Fig. 2) can only be explained by ductal tissue relaxation after prostaglandin E1 infusion was begun. Our report, as well as the previously reported cases, supports the theory that ductal tissue constriction plays a major role in the development of discrete CoA in some patients. The administration of prostaglandin E1 can relax ductal tissue present at the coarctation site, relieving obstruction and improving symptoms, even when fibrosis has already formed within the ductus arteriosus. Although it is possible that the clinical improvement was obtained due to dilatation of the ductal ampulla, the echocardiographic pictures were not supportive of this fact.
In summary, prostaglandin E1 infusion has been shown to be effective in relieving obstruction due to CoA even in cases in which the ductus arteriosus is not patent. These findings suggest that the presence of ectopic ductal-like tissue in the aorta may contribute to the development of CoA.
References
PF Callahan ES Quivers LM Bradley JE Sell GR Martin (1998) ArticleTitleEchocardiographic evidence for ductal tissue sling causing discrete coarctation of the aorta in the neonate: case report. Pediatr Cardiol 19 182–184 Occurrence Handle10.1007/s002469900276 Occurrence Handle1:STN:280:DyaK1c7lsVartQ%3D%3D Occurrence Handle9565515
KC Chan (1995) ArticleTitleEditorial comment. Int J Cardiol 49 212–213
MD Freed MA Heymann AB Lewis SL Roehl RC Kensey (1981) ArticleTitleProstaglandin E1 in infants with ductus arteriosus-dependent congenital heart disease. Circulation 64 899–905
WM Gersony (1983) Coarctation of the aorta. . Adams . Emmanoulides (Eds) Heart Disease in Infants, Children and Adolescents, 3rd edn. Williams & Wilkins Baltimore 188–199
JM Hascoët F Didier P Monin P Vert (1992) ArticleTitleEfficiency of prostaglandin E1 in a tiny baby with coarctation of the aorta and ligated ductus arteriosus. Acta Paediatr 81 938–940 Occurrence Handle1467620
MA Heymann W Berman AM Rudolph V Whitman (1979) ArticleTitleDilatation of the ductus arteriosus by prostaglandin E1 in aortic arch abnormalities. Circulation 59 169–173
SY Ho RH Anderson (1979) ArticleTitleCoarctation, tubular hypoplasia, and the ductus arteriosus. Br Heart J 41 268–274 Occurrence Handle1:STN:280:CSaC2crhtVw%3D Occurrence Handle426975
GM Hutchins (1971) ArticleTitleCoarctation of the aorta explained as a branch-point of the ductus arteriosus. Am J Pathol 63 203–221 Occurrence Handle1:STN:280:CS6B3s7lslA%3D Occurrence Handle5090637
JM Neutze MB Starling RB Elliott BG Barratt-Boyes (1977) ArticleTitlePalliation of cyanotic congenital heart disease in infancy with E-type prostaglandins. Circulation 55 238–241
AM Rudolph MA Heymann U Spitznas (1972) ArticleTitleHemodynamic considerations in the development of narrowing of the aorta. Am J Cardiol 30 514–525 Occurrence Handle1:STN:280:CSyD3cbntFU%3D Occurrence Handle4672503
GA Russell PJ Berry K Watterson JP Dhasmana JD Wisheart (1991) ArticleTitlePatterns of ductal tissue in coarctation of the aorta in the first three month of life. J Thorac Cardiovasc Surg 102 596–601 Occurrence Handle1:STN:280:By2D3Mnlt1I%3D Occurrence Handle1921436
HG Whitley LW Perry (1990) Coarctation. WA Long (Eds) Fetal and Neonate Cardiology. Saunders Philadelphia 477–486
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liberman, L., Gersony, W., Flynn, P. et al. Effectiveness of Prostaglandin E1 in Relieving Obstruction in Coarctation of the Aorta Without Opening the Ductus Arteriosus . Pediatr Cardiol 25, 49–52 (2004). https://doi.org/10.1007/s00246-003-0549-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-003-0549-5