
Abstract
This paper summarises my experience, over 14 years, treating over 1350 patients suffering from lumbar disc pathology, using minimally invasive intradiscal decompressive percutaneous techniques. The vast majority underwent the method introduced by Onik in 1985, referred to as "automated" since it involves a mechanical probe, working by a "suction and cutting" action for removal of the nucleus pulposus. Postoperative follow-up of at least 6 months was available for 1047 patients aged 15–92 years, who underwent this procedure up to June 2002. Results, based on a patient satisfaction, have been good in 58% of patients at 2 months and in 67.5% at 6 months; they have been particularly favourable in some subgroups such as elderly people (79.5% of excellent or good results), patients previously operated upon (78%) and those with "discogenic" low back pain (79%). Complication rates have been extremely low (less than 1%) and all complications cleared up without sequelae. In comparison with other percutaneous disc treatments, Onik's achieves the best compromise between clinical efficacy, comfort for the patient and low invasiveness.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Low back pain and sciatica are major causes of morbidity in industrialised countries, and in many cases symptoms are related to disc disease, mainly a tendency for the nucleus pulposus and other inner disc material to protrude beyond the limits of the disc space, through tears in the annulus fibrosus; for such conditions, open surgical discectomy is the traditional treatment, despite the lack of reliable controlled and randomised trials confirming its long-term safety and efficacy. Because of its many disadvantages, a minimally invasive percutaneous approach has been a goal since the early sixties, when Lyman Smith [1, 2] proposed the injection of an enzyme for chemolysis of the nucleus pulposus and its protruding fragments compressing a nerve root. From the seventies onwards, many other different techniques have been advocated; they may involve manual removal of the nucleus pulposus, with different types of instrument, with or without fibrescopic vision, or different types of energy (radiofrequency, laser, coblation, etc.) for reduction of the disc or to destroy protruding components [3, 4, 5, 6, 7, 8, 9].
Minimally invasive treatments for disc protrusions have faced fierce opposition from the surgical community, while enjoying a very high level of psychological acceptance by patients; potential patients are very numerous, given that up to 80% of the population may have at least one episode of acute low back pain during their active life [10].
The main goal of percutaneous procedures, other then effective treatment, is safety. While open surgery is effective, it has well-known disadvantages, including epidural scarring, damage to bone, denervation of paraspinal muscles with consequent lumbar instability, long postoperative inactivity and the frequent "failed back-surgery syndrome". Patients with the latter, often untreatable and severely disabled, are so numerous that they represent the best advertisement for minimally invasive procedures, particularly given the high tendency of disc protrusions to self-healing.
I started work in this field in the early eighties, using chymopapain and manual techniques for percutaneous removal of the nucleus pulposus. In 1987 [11, 12, 13, 14] I adopted the technique introduced by Onik in 1985 [15, 16, 17], called "automated" percutaneous lumbar discectomy (APLD), since it involves a mechanical probe with a vacuum generator, which removes the nucleus pulposus by a "suction and cutting" action [15].
From June 1987 to June 2002, I treated 1308 discs in 1158 patients with low-back pain and/or sciatica, with the aim of internal decompression of the disc and relief of nerve-root compression. During this time I modified the indications for treatment and patient selection criteria from those originally proposed by Onik. After a period of variable results related to a technical learning curve and uncertainty with regard to indications, with wrong selection of patients, the rate of good or excellent clinical results has always been high, with an extremely low complication rate.
I have tried other techniques at the same time, such as laser discectomy, coblation nucleoplasty, alcohol chemonucleolysis, manual discectomy with fibrescopic direct vision of the inside of the disc, and still use some of these in selected cases. However, they have never proved superior to Onik's method overall in terms of a single procedure offering the best compromise between simplicity, safety, low invasiveness, efficacy and short- and long-term clinical results. I review my personal experience with Onik's method.
Materials and methods
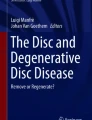
From June 1987 to June 2002, I performed 1158 percutaneous discectomies in 1146 patients; in 12 a new procedure was undertaken 2 years or more after the first, for recurrence of pain. The procedures involved 1308 discs: 771 (59%) at L4/5, 438 (33.5%) at L5/S1 and 99 (7.5%) at other levels, mainly L3/4. In 140 patients (12%) two discs, usually L4/5 and L5/S1, were treated simultaneously, and in five I treated three: L3/4, 4/5 and L5/S1 in four, and L2/3, 3/4 and 4/5 in one (Fig. 1).

Sagittal T2-weighted MRI of a 22 year-old sportswoman complaining of back and leg pain. There are large, extruded disc protrusions at L2/3, 3/4 and 4/5. The shape of the lesions is not a good indication for percutaneous treatment, but automated percutaneous lumbar discectomy (APLD) was offered to the patient given that open surgery at this age could be devastating. APLD was performed at three levels in one session, with an acceptably good result, even if the patient could not resume her sporting activity
The patients' age ranged from 15 to 92 years. I carried out 670 procedures on 663 males and 488 on 483 females. I directly recruited all patients, met them personally, visited them and informed them before the procedure. I was therefore the only person directly responsible for the indications to treat, even in the patients referred by and discussed with the orthopaedic or neurosurgical colleagues. I also followed all patients when necessary after the procedure, telling them to consult me about of any problem, complication or question.
All patients complained of low back pain and/or sciatica, lasting in most cases for 6 months or more, and each had a lumbar bulging or protruding disc, not sequestrated or migrated (following the "Nomenclature and classification of lumbar disc pathology—Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology)" 18, 19, 20], seen definitely on CT and/or MRI, or in doubtful cases confirmed by discography or CT discography.
Technique and instrumentation remained substantially as described by Onik [21], with some modifications. I perform all the procedures with the patient lying on one side, using a posterolateral approach on the side of any leg pain, under local anaesthesia with light sedation; this, together with knowledge of and attention to radiographic landmarks for probe positioning, eliminates the risks of neural or dural injury. Aspiration averages 12–18 minutes, and is stopped when the flow of nuclear material from the probe clearly decreases or when a considerable amount of blood starts coming, signalling that the vascularised discovertebral cartilage is denuded. A soft silicon gel cushion is positioned under the patient's hip and used to bend the lumbar spine in order to lower the iliac crest on the entry side, thus uncovering the L5/S1 disc from the pelvic bone. I give 2 g prophylactic cephalosporin intravenously prior to the operation.
After aspirating and withdrawing the probe, I inject 80 mg methylprednisolone acetate and 1 ml bupivacaine 0.5% in the disc, through an 18 G needle replacing the probe, placed over a 0.8 mm. Kirshner wire left in place as a guide. When there has been marked preoperative radiculopathy with intense leg pain, I also inject 40 mg methylprednisolone acetate and 1 ml bupivacaine around the root in the intervertebral foramen during withdrawal of the 18 G needle.
The procedure is performed on an outpatient basis; the patient remains under observation for about 2 h and is then sent home with a prescription for a nonsteroidal anti-inflammatory, usually a Cox-2 inhibitor, and diazepam at bedtime as a muscle relaxant, for 10–15 days. Patients are encouraged to move, stand and walk from the third day; for a 2–3 week period they are advised against prolonged sitting or driving.
Before being sent home patients are given two evaluation forms, and asked to fill them in and return them after 2 and 6 months. They are asked to give a personal judgement on the result of the procedure, with a choice of five grades (excellent, good, fair, poor or null and bad or worse); and about resumption of work or normal daily activities; to describe any persistent symptoms, if they are still taking pain-killers, and if they have been operated upon after the procedure; there is also space for free comment or questions. I try to keep in contact with patients who do not return the evaluation forms, usually by phone, at least to obtain crucial information such as open surgery following percutaneous discectomy. I personally followed several patients, usually those (and probably almost all) with a poor clinical result, as is routine after unsuccessful treatment, and keep a record (history, examination, imaging, treatment and possibly follow-up) of every patient treated since 1987. Patients completely lost to follow-up are relatively few: 63 (5.5%) at 2 months and 111 (9.6%) at 6 months.
Results
The procedure was always possible at L4/5 and other more cranial discs; in only three of 670 attempts in men was I unable to position the probe correctly in the L5/S1 disc, because the iliac crest was too high; in women the approach to L5/S1 is easier because of their flatter and wider iliac crests and discectomy was always possible. In four cases, three at L5/S1 and one at L4/5, the approach was impossible from one side because of repeated, unavoidable contact with the nerve root, but was possible from the opposite side; this was probably due to a unilateral, double root origin covering the disc space or to flattening and enlargement of a root compressed against the protruding annulus.
A clinical result is defined as excellent with complete resolution of symptoms or good with marked reduction in pain, and general satisfaction of the patient, who could return to work or usual daytime activities, taking analgesics seldom or not at all. The results were excellent or good in 635 (58%) of the 1095 procedures in which 2-month follow-up was available. Favourable results tend to improve, and there was an overall positive evaluation by 707 (67.5%) of the 1047 patients followed at 6 months. There were no statistically significant differences with sex or level of discectomy.
Results are better in three subgroups. Among the 1047 patients with a 6-month follow-up, the result was excellent or good in 66 (79.5%) of 83 aged 70 years or more; 83 (78%) of 106 who had previously undergone open disc surgery at the same level and had a recurrent disc protrusion after 6 months or more; and in 149 (79%) of 188 with purely "discogenic" low-back pain.
Excluding these subgroups, excellent or good results were achieved in 409 (61%) of the 670 patients seen at 6 months. Of the 1047 patients, 125 (12%) underwent open surgery after APLD.
I saw very few complications. I had two cases of discitis (0.17%), probably infective: one, in my very early experience, was severe, with back pain for months and marked narrowing of the disc, and a recent, very mild one, which cleared completely clinically and radiologically in 2 months without sequelae, and a good result at 6 months. There was one acute haematoma of the iliopsoas muscle, very painful for 2 days but clearing up completely within a few weeks. In eight patients (0.7%), included among the 125 who underwent open surgery after the APLD, the disc protrusion appeared more bulky, extruded or sequestrated after the percutaneous procedure.
Discussion
All the percutaneous techniques for central disc decompression, APLD included, are based on the principle that in an enclosed space a reduction in volume, even partial, confers a much greater reduction in pressure; this leads to decreased pressure on the nerve root, and relief of sciatica, even without a radiographically evident reduction in total disc volume [22]. After weeks or months, the partial vacuum causes the protruded portion of nucleus pulposus (or other disc material) to move away from the nerve root back towards the centre of the disc, pushed by partially intact fibres and ligaments of the outer annulus; this process, along with regeneration of a more fibrous nucleus pulposus, favours restoration of the inner fibres of the annulus and decreases the tendency to further protrusion towards the spinal canal. The success of the procedure depends to a great extent on selecting lesions to treat: the protruding nucleus pulposus must be at least partially contained by the external fibres of the disc, without a large extrusion or migrated or sequestrated fragments. Such contained lesions are often circumferential bulges or protrusions, which appear broad on axial MRI or CT [20, 23, 24] (Fig. 2). Since MRI and CT do not usually enable distinction of a contained from an uncontained prolapse, in doubtful cases, discography or CT discography may help in assessing annular tears and extruded lesions. CT discography may also show the size of the "neck" connecting the protruded part of the disc with the central nucleus pulposus: the wider the connection, the more likely efficient transmission of pressure towards the centre of the disc [24, 25, 26] (Fig. 2B).

CT discography. A There is a broad-based, central posterior protrusion with contrast medium spreading around the periphery of the annulus from the nucleus via a midline radial tear. B In another patient the nucleus communicates with a lateral protrusion with a well-contained intra- and extraforaminal extension; the "neck" between the central nucleus and the protruding component is relatively wide
The patient selection criteria defined initially by Onik remain largely valid: patients with more leg pain (possibly associated with neurological signs of root compression) than back pain; a contained disc protrusion clearly documented by imaging; no previous open surgery, spinal stenosis or other bone lesions which could compress a root; and no workmen's' compensation claims. I think that a purely clinical criterion is also very important. Patients with a contained herniation, a good indication for percutaneous treatment, typically have a relatively long history (6 months or more) of back and/or leg pain of variable intensity, more intense under loading of the lumbar spine and particularly in a sitting position (typically, driving a car). The pain is not disabling, but becomes more and more incompatible with a good quality of life, in part because of a progressive reduction in the psychological threshold of pain tolerance. It is probable that these features correlate with a contained disc lesion, root compression becoming evident only when a static or dynamic load on the spine provokes outward transmission of pressure from the centre of the disc through rents in the inner fibres of the annulus, with secondary increase in the external diameter of the disc. The pressure within the disc and its volume decrease with rest, thanks to integrity of the outer annular fibres and ligaments. Given these conditions APLD achieves as good a decompression of the disc as open surgery, without the latter's risks. Clinical failure of APLD (or other percutaneous treatments) could also mean a failure of open surgery.
Uncontained extrusions of the nucleus pulposus or sequestrated or migrated fragments, which are not a good indication for APLD, cause sustained, firmer compression of the nerve root (probably together with inflammatory phenomena primed by the presence of nucleus pulposus in the vascular epidural space), and therefore more constant and intense pain, often disabling. These clinical landmarks, when they last for at least 6–8 weeks, justify open surgery as the treatment of choice.
My experience confirms a good clinical outcome in 707 (67.5%) of 1047 with 6-month follow-up, given the clinical and radiological features described above. Given its low morbidity, however, APLD may also be a therapeutic option in extruded, uncontained prolapses, even if with a lower expected success rate, and can thus be offered ethically to the patient, when the risks of open surgery are higher because of age, general medical conditions or spinal contraindications such as bone lesions (Fig. 1.). This typically applies to patients who have already undergone open surgery at the same level, because of the possibility of symptomatic epidural scar. In my experience this is a subgroup of patients highly suitable for APLD; I recorded excellent or good results in 83 (78%) of 106 patients (10% of those with a 6-month follow-up). The good results can be attributed to several reasons: firm epidural fibrosis from the previous surgery, firmer than the normal, highly vascular epidural tissue, decreasing the likelihood of a large extrusion or migration of the nucleus pulposus; less decompression necessary for a nerve root already confined by postsurgical scar in a smaller space; a lesser degree of pain relief demanded by a patient who has already experienced open surgery and has a long history of pain.
Similar considerations explain the good results in elderly people, in whom less space is available to the nerve root because of arthropathic bone degeneration with osteophyte formation; acquired stenosis of the lumbar canal and intervertebral foramina is frequent, and even a small reduction in the volume of the disc by APLD may result in radicular decompression and clinical amelioration. Elderly patients' less active life style and lower expectations, may also play a role.
Another group of patients, not originally included by Onik, for whom I believe APLD may be the treatment of choice, consists of those with chronic discogenic back pain. When the intervertebral disc is the only source of the pain, the results are very good, as detailed above.
These matters merit some consideration. The intervertebral disc is innervated only at the most peripheral annular fibres; in normal conditions the physiological raise in pressure within the disc from dynamic loading is painless, not being transmitted to the outer annulus, which is protected by intact inner fibres. Early degeneration of the disc, typically with tears of the inner fibres, allows outward transmission of pressure and stimulation of the nociceptors of the outer annulus and spinal ligaments. Only radial tears affect each layer of the annulus [20, 27, 28], and affecting the biomechanics of the disc and its innervated portions, provoke symptoms. Concentric and transverse tears are probably incidental rather than clinically significant findings. The pain produced is lumbar, migrating and often radiating bilaterally to the groin or thighs, but not below the knees, typically provoked by sitting and by flexion of the lumbar spine, while zygoapophyseal pain is evoked by extension and lateral flexion; mild, often migrating sciatic pain from root compression may be associated. A very evocative sign is pain elicited by extension of the previously flexed lumbar spine against resistance, e.g., a hand pushing against the shoulders. To confirm that the pain is purely or predominantly discogenic, a disc bulge or broad-based protrusion (evidence of raised pressure within the disc) must be evident on MRI, usually with low signal on T2 weighting, evidence of radial tears and early degeneration of the disc [29] (Fig. 3). Modic 0 or 1 changes [30, 31] may be present, but not Modic 2 or 3. The discogenic origin must be confirmed at discography, reproducing the patient's pain by injection of a small amount of contrast medium into the disc, raising the pressure within it. Other causes of lumbar pain (posterior intervertebral joint arthropathy, spondylolisthesis, etc.) must be excluded and before APLD these patients should have had conservative treatment for at least 18 months, with no improvement.

T2-weighted sagittal MRI showing a contained posterior bulge of the L4/5 disc, with decreased signal related to radial tears and early degeneration. Discs with these appearances usually respond well to conservative treatment, but if typical back pain becomes chronic, may become an indication for APLD, although not for other forms of percutaneous treatment
The good results of APLD on discogenic pain are probably explained by lowering the pressure within the disc and scar formation, reinforcing the annulus with more fibrous tissue; this may also contribute to stabilisation in cases of instability. A positive role for inner disc scarring seems confirmed by the fact that good results are obtained only in relatively young patients, less than 50–55 years old; in older people, the mucoid matrix of the nucleus is progressively replaced by fibrous tissue, discs become harder and stiffer, radial tears are absent [32] and the conditions described for pressure-related discogenic pain are no longer met.
In early degeneration there is sprouting of vessels, accompanied by nociceptive fibres, from the outer towards the inner disc, and this becomes painful owing to the presence of nodules of "granulation" tissue, sometimes evident on MRI as zones of high signal, usually in the posterior annulus [33] (Fig. 4); since granulation tissue is vascularised, early bleeding occurs during aspiration. Probably the good results after APLD are due in these cases to ablation of this painful, innervated, "degenerate" tissue, replaced over time by a more physiological, fibrous scar. Injection of steroids, which can be repeated weeks after APLD, presumably also reduces inflammatory phenomena inside the disc.

Sagittal T2-weighted image showing high signal in the posterior annulus at L4/5, probably representing painful, vascular and innervated "granulation" tissue, which can be effectively removed by APLD
Overall, good results improve from 58% at 2 to 67.5% at 6 months. I usually follow and personally visit most patients with residual pain after the intervention, and found this residual pain to often be different from the preoperative pain: it is mainly lumbar and probably due to vertebral instability, caused by many factors, mainly the iatrogenic disc lesion and the prolonged disuse of the lumbar spine and muscles. This "articular" pain, no longer due to disc pathology itself, usually regresses with physiotherapy and, I presume, thanks to the internal scarring of the disc, which takes months. Physiotherapy greatly helps in reducing lumbar pain due to wasting and prolonged disuse of the back muscles, while the scarring within the disc may help where back pain is also due to instability. A new, large, "healthy" fibrous scar replacing a degenerate, fissured disc may stabilise the adjoining segments, eliminating or delaying in many cases the need for more aggressive, surgical fixation. In this respect APLD is, in my experience, far superior to other decompressive procedures such as laser, coblation or chemonucleolysis, in which scarring within the disc, given the physical principles of ablation of the nucleus, is absent, poor or sometimes even bad, as it happen with thermal tissue necrosis in laser discectomy.
After APLD, early activity is not only possible but also useful, counteracting muscle wasting and being psychologically motivating. The patient must be warned to avoid as much as possible, for 3–4 weeks, prolonged car driving, prolonged sitting, heavy weight-lifting with back flexion and sports. Regression of leg pain may take weeks, owing to "remodelling" of the disc and regression of inflammation at the surgical site. Progressive return to heavy activities or sports is usually possible in 4–6 weeks; for sportsmen, especially professionals, the absence after APLD of bone damage, muscle denervation or ligament destabilisation is very important.
I was not able to define clearly which patients would have been included in Onik's original selection protocol [17]; however, the rate of excellent or good results in the 670 patients closest to his selection criteria is 61%, similar to most published series [23, 24, 25, 34, 35, 36, 37]. Good results were obtained in 67.5% overall, thanks to the three subgroups previously described, most of whom would not have met Onik's criteria, and are different from the patients in most published series; sensible comparisons is therefore impossible. Nevertheless, reporting good results in these patients, previously not clearly identified as suitable for percutaneous procedures, is the main purpose of this article.
Poor results are reported in the only two randomised and controlled studies on APLD: 37% success rate at 1 year [38] and 29% [39]. However these studies, like others reporting very poor results [40, 41, 42], have limitations and features which make the patient populations and technical conditions different from those I describe. First, the numbers of patients are low: 32 treated by one operator [39] and 69 treated by many operators in a multicentre study [38]. The authors do not state how experienced the operators were, i.e. how many APLD procedures each had already performed. I believe that the learning curve of APLD is flatter than usually thought, and good quantities of nucleus pulposus, in the right places, are correctly and effectively aspirated only after many procedures. The disc at L5/S1 is safely and reliably approached only by operators having performed no fewer than 40–50 procedures at higher levels. It is highly likely that the operators in the two studies mentioned above were much more experienced in open surgery or chemonucleolysis. My better results may also be related to modifications of the technique, as described.
Second is patient selection. As explained, purely clinical criteria are fundamental and there is little overlap with indications for APLD and those for open surgery or chemonucleolysis, so that randomised trials comparing these procedures would not be logical. The patients recruited in the two trials mentioned above are likely to have extruded, uncontained protrusions, not good indications for APLD.
For some time I have customarily used the curved cannula provided with the surgical kit at every level, since I find it very helpful not only in reaching the L5/S1 disc when partially covered by the iliac crest, but also in allowing greater mobility of the probe inside whichever disc, with consequent aspiration of greater amounts of nucleus pulposus, even in more posterior or posterolateral positions, where the nerve root is compressed. I first use the straight cannula, to aspirate more centrally and anteriorly, for 5–9 min, followed by the curved cannula for the rest of the procedure.
The initial centre for aspiration, which corresponds to the path of the guiding trocar and initial working position of the probe, is in the midline, at the junction of the middle and posterior thirds of the disc, where the normal nucleus lies; in cases of large, posterior protrusions invading the spinal canal, a little more posterior position of the probe is aimed at.
During aspiration the probe is constantly subjected to double rotation, to make its end move in larger and larger circles, while keeping the port external to the circle itself; using the straight and curved cannulae, at least two large tunnels are excavated in the disc.
When treating discogenic back pain, aspiration is never stopped before blood starts coming from the disc (from granulation tissue or end-plate cartilage), since this should favour subsequent scarring; this is always possible with the "double rotation" technique. Bleeding is not, however, necessary when treating root compression; aspiration is stopped when the amount of disc material obtained greatly decreases. In such cases, at the end of the procedure the side-port of the probe is positioned close to the protruding parts of the disc in the neural foramen, trying to aspirate the protruding material itself. This "topographical" criterion guides my aspiration; the probe is not positioned to work only in the centre of the disc, as originally described by Onik, but thoroughly directed to look for the main bulk of the nucleus pulposus and its protruding components. As long as the height of the disc is preserved radiologically, at least a moderate amount of nuclear material must always come by aspiration; if, after an apparently correct first positioning of the probe inside the disc, nuclear material does not come freely, the probe must be moved to find it, and the intervention not stopped until nucleus is found and removed.
The safety of the procedure is extremely high, even if lesions of nerve roots, vessels or the ureter are reported [43, 44, 45]. I believe that, in experienced hands, with thorough knowledge of and attention to radiographic landmarks for probe positioning, vascular, neural or dural injury is very unlikely. The operator must at every moment be absolutely sure of the anatomical position of the instruments, and this requires perfect knowledge of the radiological projections, along with the ability to make a three-dimensional mental reconstruction from the flat, two-dimensional fluoroscopic image. These are skills possessed by radiologists accustomed to interventional percutaneous procedures, and not always by surgeons; having taught the procedure to many dozens of operators, I think it is learnt more rapidly and more safely (like endovascular interventional procedures) by radiologists than by "open" surgeons.
My overall complication rate was 0.95%. There were no injuries to nerve roots, dura mater, ureters, major vessels or bowel. Study of the preoperative imaging excludes the presence in the path of the instruments of bowel behind the psoas muscle, which could be perforated, with the risk of peritoneal or disc infection [46, 47]. The use of only local anaesthesia, with or even without light sedation, highly decreases the risk of nerve-root injuries.
The acute haematoma in the iliopsoas, from injury to a small artery, resolved without sequelae in about 1 month. Psoas muscle haematomas are more largely reported after nonautomated percutaneous discectomies [48].
There were eight patients with presumably iatrogenic extrusion or sequestration of fragments after treatment for contained lesions, who were subsequently operated upon. I do not think extrusion is due to weakening annulus [49], but to the probe in the disc pushing out an already partly extruded nucleus pulposus, resulting in complete extrusion. I base this on the fact that this complication never occurred in patients treated for discogenic back pain, who did not have lateral, focal disc prolapses compressing the nerve root. I therefore think it riskier to approach some bulky lesions from the opposite side, as proposed by Dullerud and Nakstad [49], since this carries a greater risk of pushing out disc material, in addition to it not being possible to aspirate extruded disc in the region of the neural foramen.
Two complications in this series are related to discitis, probably infective. One severe case occurred very early, when we used to resterilise the instruments once. The second was very recent; the radiological signs were very mild and the patient complained of back pain 2 weeks after treatment, after a sharp rotation of the low back. He was given antibiotics and his symptoms resolved completely in 1 month.
Dosimetry studies indicate a very low radiation exposure for the operator and the patient [50].
I underline again the absence of epidural fibrosis, the main cause of the "failed back surgery syndrome". An important safety factor of APLD, even compared to other percutaneous methods, is the internal cutting action of the device, whose external blunt portion prevents damage to structures other than the nucleus pulposus.
The only noteworthy side effect is increased back pain. Most patients with a surgical wound have pain, and that applies to percutaneous discectomy, because of damage to muscle and fascia in the trajectory of the device and to the innervated annulus and disc cartilage. I warn patients that back pain may last 3–4 weeks; I also warn patients without back pain before treatment that they must expect it. Injection of steroids into the disc immediately after APLD is helpful in reducing the back pain in the early postdiscectomy period. Despite the pain, patients are always allowed to be mobile immediately, to stand and walk.
This study evidently has many scientific limitations. It was not randomised and not externally controlled; both conditions are impossible to meet in large studies of numerous patients over a long period. It is also a single-author study, so that the effects of the author's conceptual bias or technical limitations are amplified. My aim is only to expose experience developed over years with, I believe, an honest and unbiased attitude, looking for the best compromise between patients' desire for relief of their pain and most harmless way to achieve that. My research was conducted in different directions, exploring approaches, techniques and devices, but I believe I have given an acceptable rate of satisfaction to a large number of patients.
Other limitations are the 9.6% rate of cases lost to follow-up at 6 months (even if it is perhaps unlikely that all or most of them had a poor result), and the relatively short—6-month—follow-up. Another is that the greater part of the results is derived not from direct consultation but from postal questionnaires, and this might imply positive or negative bias on the part of the patients responding; moreover, interpretation of the real clinical status on the basis of a form is not always clear-cut, borders between different conditions being blurred. Criteria of self-evaluation and satisfaction therefore predominate; however, this seems reasonably acceptable in a disease whose natural history is almost always favourable, which is not function-threatening and in which the main and often the only symptom, pain, is subjective.
References
Smith L, Garvin PJ, Jennings RB (1963) Enzyme dissolution of nucleus pulposus. Nature 198: 1398–1400
Smith L (1964) Enzyme dissolution of nucleus pulposus in humans. JAMA 187: 137–140
Choy DS (1998) Percutaneous laser disc compression (PLDD): twelve years' experience with 752 procedures in 518 patients. J Clin Laser Med Surg 16: 325–31
Friedman WA (1983) Percutaneous discectomy. An alternative to chemonucleolysis? Neurosurgery 13: 542–547
Hijikata S, Yamagishi M, Nakayama T, Oomori K (1975) Percutaneous nucleotomy: a new treatment method for lumbar disk herniation. J Toden Hosp 5: 5–13
Hijikata S (1989) Percutaneous nucleotomy: a new concept technique and 12 years' experience. Clin Orthop 238: 9–23
Kambin P, Gellmann H (1983) Percutaneous lateral discectomy of the lumbar spine. A preliminary report. Clin Orthop 174: 127–132
Schreiber A, Suezawa Y (1986) Transdiscoscopic percutaneous nucleotomy in disc herniation. Orthop Rev 15: 75–78
Yeung AT (2000) The evolution of percutaneous spinal endoscopy and discectomy: state of the art. Mt Sinai J Med 67: 327–32
Lucas PR (1983) Low back pain. Surg Clin North Am 63: 515–528
Belloni G, Bonaldi G, Moschini L, Porta M (1989) La discectomia percutanea per aspirazione. Riv Neuroradiol 1: 91–100
Bocchi L, Ferrata P, Passarello F, et al (1989) La nucleoaspirazione secondo Onik nel trattamento dell'ernia discale lombare. Analisi multicentrica dei primi risultati su oltre 650 trattamenti. Riv Neuroradiol 2 [Suppl 1]: 119–122
Bonaldi G, Belloni G, Prosetti D, Moschini L (1991) Percutaneous discectomy using Onik's method: 3 years' experience. Neuroradiology 33: 516–519
Bonaldi G, Minonzio G, Belloni G, et al 1994) Percutaneous cervical diskectomy: preliminary technical experience. Neuroradiology 36: 483–486
Onik G, Helms CA, Ginsburg L, Hoaglund FT, Morris J (1985) Percutaneous lumbar diskectomy using a new aspiration probe. AJNR 6: 290–293
Maroon JC, Onik G (1987) Percutaneous automated discectomy: a new method for lumbar disc removal. J Neurosurg 66: 143–146
Onik G, Maroon JC, Helms CA, et al (1987) Automated percutaneous discectomy: initial patient experience. Radiology 162: 129–132
Milette PC (1997) The proper terminology for reporting lumbar intervertebral disk disorders. AJNR 8: 1859–1866
Fardon DF, Milette PC (2001) Nomenclature and classification of lumbar disc pathology. Recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine 26: E93-E113
Fardon DF, Milette PC (2003) Nomenclature and classification of lumbar disc pathology—recommendations of the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. American Society of Neuroradiology, www.asnr.org
Onik G (1988) Percutaneous automated discectomy: technique. In: Onik G, Helms CA (eds) Automated percutaneous lumbar discectomy. Radiology Research and Education Foundation, University of California, San Francisco, pp 77–110
Shea M, Takeuchi TY, Wittenberg RH, White AA 3 rd, Hayes WC (1994) A comparison of the effects of automated percutaneous diskectomy and conventional diskectomy on intradiscal pressure, disk geometry, and stiffness. J Spinal Disord 7: 317–325
Castro WH, Jerosch J, Hepp R, Schulitz KP (1992) Restriction of indication for automated percutaneous lumbar discectomy based on computed tomographic discography. Spine 17: 1239–1243
Moon CT, Cho J, Chang SK (1995) Availability of discographic computed tomography in automated percutaneous lumbar discectomy. J Korean Med Sci 10: 368–372
Dullerud R, Amundsen T, Lie H, Juel NG, Magnaes B (1995) CT-diskography, diskomanometry and MR imaging as predictors of the outcome of lumbar percutaneous automated nucleotomy. Acta Radiol 36: 613–619
Onik GM (2000) Percutaneous diskectomy in the treatment of herniated lumbar disks. Neuroimaging Clin North Am 10: 597–607
Milette PC, Raymond J, Fontaine S (1990) Comparison of high-resolution computed tomography with discography in the evaluation of lumbar disc herniations. Spine 15: 525–533
Milette PC, Fontaine S, Lepanto L, Breton G (1995) Radiating pain to the lower extremities caused by lumbar disk rupture without spinal nerve root involvement. AJNR 16: 1605–1615
Milette PC, Fontaine S, Lepanto L, Cardinal E, Breton G (1999) Differentiating lumbar disc protrusions, disc bulges, and discs with normal contour but abnormal signal intensity. Magnetic resonance imaging with discographic correlations. Spine 24: 44–53
Modic MT, Masaryk TJ, Ross JS, Carter JR (1988) Imaging of degenerative disk disease. Radiology 168: 177–186
Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR (1988) Degenerative disc disease. Assessment of changes in vertebral body marrow with MRI. Imaging Radiology 166: 194–199
Kieffer SA, Stadlan EM, Mohandas A, Peterson HO (1969) Discographic-anatomical correlation of developmental changes with age in intervertebral disc. Acta Radiol 9: 733–739
Aprill C, Bobduk N (1992) High intensity zone: a diagnostic sign of painful lumbar disc on magnetic resonance imaging. Br J Radiol 65: 361–369
Dullerud R, Amundsen T, Lie H, Juel NG, Abdelnoor M, Magnaes B (1995) Clinical results after percutaneous automated lumbar nucleotomy. A follow-up study. Acta Radiol 36: 418–424
Grevitt MP, McLaren A, Shackleford IM, Mulholland RC (1995) Automated percutaneous lumbar discectomy. An outcome study. J Bone Joint Surg Br 77: 626–629
Sortland O, Kleppe H, Aandahl M, Blikra G (1996) Percutaneous lumbar discectomy. Technique and clinical result. Acta Radiol 37: 85–90
Bernd L, Schiltenwolf M, Mau H, Schindele S (1997) No indications for percutaneous lumbar discectomy? Int Orthop 21: 164–168
Revel M, Payan C, Vallee C, et al (1993) Automated percutaneous lumbar discectomy versus chemonucleolysis in the treatment of sciatica. A randomized multicenter trial. Spine 18: 1–7
Chatterjee S, Foy PM, Findlay GF (1995) Report of a controlled clinical trial comparing automated percutaneous lumbar discectomy and microdiscectomy in the treatment of contained lumbar disc herniation. Spine 20: 734–738
Shapiro S (1995) Long-term follow up of 57 patients undergoing automated percutaneous discectomy. Neurosurgery 83: 31–33
Lee SH, Lee SJ, Park KH, et al (1996) Comparison of percutaneous manual and endoscopic laser diskectomy with chemonucleolysis and automated nucleotomy. Orthopäde 25: 49–55
Ramberg N, Sahlstrand T (2001) Early course and long-term follow-up after automated percutaneous lumbar discectomy. J Spinal Disord 14: 511–516
Schreiber A, Suezawa Y, Leu H (1989) Does percutaneous nucleotomy with discoscopy replace conventional discectomy? Eight years of experience and results in treatment of herniated lumbar disc. Clin Orthop 238: 35–42
Stern MB (1989) Early experience with percutaneous lateral discectomy. Clin Orthop 238: 50–55
Flam TA, Spitzenpfeil E, Zerbib M, Steg A, Debré B (1992) Complete ureteral transection associated with percutaneous lumbar disk nucleotomy. J Urol 148: 1249–1250
Hopper KD, Sherman JL, Luethke JM, Ghaed N (1987) Retrorenal colon in the supine and prone patient. Radiology 162: 443–446
Prassopoulos P, Raissaki M, Daskalogiannaki M, Gourtsoyiannis N (1998) Retropsoas positioned bowel: incidence and clinical relevance. J Comput Assist Tomogr 22: 304–307
Monteiro A, Lefevre R, Pieters G, Wilmet E (1989) Lateral decompression of a pathological disc in the treatment of lumbar pain and sciatica. Clin Orthop 238: 56–63
Dullerud R, Nakstad PH (1997) Side effects and complications of automated percutaneous lumbar nucleotomy. Neuroradiology 39: 282–285
Contento G, Fabris G, Leonardi M, Belloni G, Bonaldi G (1989) Dose al paziente nelle procedure neuroradiologiche per il trattamento dell'ernia discale lombare. Riv Neuroradiol 2 [Suppl 1]: 55–59
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bonaldi, G. Automated percutaneous lumbar discectomy: technique, indications and clinical follow-up in over 1000 patients. Neuroradiology 45, 735–743 (2003). https://doi.org/10.1007/s00234-003-1066-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-003-1066-1