
Abstract
This chapter presents a comprehensive review of disk degeneration and lumbar stenosis disease, diagnosis, and percutaneous image-guided decompressive spinal techniques.
Clinical presentation and radiological findings are evaluated in the beginning of the chapter.
Percutaneous image-guided techniques for spinal decompression and disk decompression are described in detail, setting the state of the art and future directions for each procedure.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Disk herniation
- Lumbar spine stenosis
- Image-guided percutaneous techniques
- Corticosteroid injections
- Lumbar spinal canal decompression
- Interspinous spacers
- Platelet-rich plasma
- Disc decompression
Introduction
Degenerative changes of the lumbar spine are one of the major causes of pain, disability, fall, and depression in the elderly. There is an associated negative impact on the quality of life comparable to other conditions such as cardiovascular disease, cerebrovascular disease, or respiratory disease [1, 2]. Direct and indirect economic costs ranging from $560 to $630 billion are related to the decrease in productivity, treatments, and comorbidities in the United States alone [3, 4]. Disk degeneration and spinal canal stenosis are the two most frequent diagnoses seen in patients with degenerative spine disease [5].
Disk degeneration is a frequent diagnosis affecting at least 40% of patients with stable axial low-back pain (LBP) [6] and the most frequent cause of stable LBP in the young adult. Other frequent pain generators in stable axial LBP are related to facet joint syndrome (~15–30%) and sacroiliac dysfunction (~13–19%). Frequently, combinations of all the above pain generators are seen together.
A combination of disk and facet degeneration will often result in spinal canal stenosis [7]. Given the wide variation in accepted criteria for defining lumbar spinal stenosis and the frequent prevalence of asymptomatic imaging finding, especially asymptomatic disk degeneration [8], treatment of such lumbar conditions is solely driven by the patient’s symptoms. Most frequently, the first line of treatment should include conservative management with physiotherapy; should there be no improvement with time, many minimally invasive interventional techniques are now available. The following chapter will review some of the minimally invasive techniques available to alleviate pain related to these frequent spinal diagnoses.
Disease and Clinical Diagnosis
Disk Degeneration
Intervertebral disk (IVD) degeneration is associated with disk disruption, phenotype alteration of healthy cells, and the release of pro-inflammatory cytokines such as lactate and other pain mediators [9]. This process is influenced by factors such as changes in diffusion of nutrients and oxygen across the IVD matrix, variations in soluble regulators of cell function, genetic predisposition, aging and senescence, and mechanical load [10]. A pathologic disk becomes densely innervated, compared to its healthy state, with an increase in neurotrophins. These neurotrophins play a pro-inflammatory role and contribute to amplifying the pain cascade [11,12,13].
The diagnostic criteria for patients with discogenic pain remain unclear; most frequently, various testing is needed to make an accurate diagnosis. The best combination of tests is lumbar magnetic resonance imaging (MRI) performed with a provocative discography. Physical examination is not sensitive or specific for discogenic back pain [14].
Macroscopic changes can be seen on MRI with a grading system that helps quantify disk degeneration [15, 16]. Using this system, disk degeneration can be graded on MRI T2 spin-echo weighted images. The acquired signal intensity correlates with water and proteoglycan content. This system was first described by Pfirrmann et al., describing five grades of disk degeneration (Table 19.1) [15], and subsequently modified by Griffith et al., further dividing the grading system into eight categories (Table 19.2) [16].
Disk Herniation
Disk herniation happens when the pressure contained by the disk nucleus pulposus surpasses the concentric forces of the annulus fibrosus. Annular fissure is considered to mark the first step of the degeneration cascade resulting in herniation. Mechanical loading and genetic susceptibility are important markers in this degeneration cascade. Also, major risk factors for disk herniation include male gender, age (30–50 years), heavy lifting or twisting, stressful occupation, lower income, and cigarette smoking. The majority of lumbar disk herniation happens within the lowest segments with 95% at L4–L5 or L5–S1 and only 5% at L3–L4.
Disk herniations are classified as protrusions or extrusions. Disk protrusions are contained by the annulus fibrosus and involve less than 25% of the disk circumference. The criterion for disk protrusion is that the greatest dimension between the edges of the disk material presenting beyond the disk space is less than the distance between the edges of the base of that disk material that extends outside the disk space. On the other hand, disk extrusion is defined as disk material migrating through the annulus fibrosus but contained by the posterior longitudinal ligament. This type of herniation appears in at least one plane; any one distance between the edges of the disk material beyond the disk space is greater than the distance between the edges of the base measured in the same plane, or when no continuity exists between the disk material beyond the disk space and that within the disk space. An extruded disk fragment is referred to as sequestrated if there is no continuity with the disk origin.
The nomenclatures related to anatomic “zones” and “levels” of the disk herniations have been well defined in the literature [17]. On the horizontal (axial) plane, these landmarks determine the boundaries of the central zone, the subarticular zone (lateral recess), the foraminal zone, the extraforaminal zone, and the anterior zone. On the sagittal (craniocaudal) plane, they determine the boundaries of the disk level: the infrapedicular level, the pedicular level, and the suprapedicular level [17].
Spinal Canal Stenosis
In comparison to disk degeneration, which can be seen in younger patients, spinal canal stenosis tends to develop at a later stage in life. Two types of spinal canal stenoses are described: congenital or degenerative types. Congenital lumbar spinal stenosis has been largely attributed to an abnormal anatomic development of the spinal canal. A “normal” spinal canal for some unidentifiable reason does not fully develop, predisposing these patients to spinal stenosis with fewer degenerative changes [18].
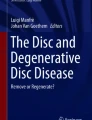
Degenerative lumbar spinal stenosis (DLSS) develops in the setting of normally developed spinal canal and may lead to narrowing of the central spinal canal and/or neuroforaminal stenosis. Disk degeneration, dehydration, and bulging contribute to this phenomenon by narrowing of the spinal canal, resulting in an increased instability of the spinal segments and incremental pressure between facets, which leads to degeneration and osteophyte formation, often more pronounced on the superior articular process [19,20,21,22]. These hypertrophic changes in addition to osteo-cartilaginous/ligamentous redundancy lead to neural and/or vascular compression [23, 24] (Fig. 19.1).

MR axial T2-weighted images demonstrate different causes of degenerative lumbar spine stenosis. Left: volumetric reconstruction. Right top corresponds with the space between lines C and D at left: central stenosis (white arrow) with involvement of the area between the facet joints occupied by the dura mater and its contents. Right middle corresponds with the space between lines B and C at left: lateral stenosis related to the involvement of foraminal area, also known as “Lee’s midzone,” [20] occupied by the ganglion and the ventral motor root (white arrow). Left bottom corresponds with the space between lines A and B at left: lateral stenosis represented by the involvement of the lateral recess, also known as “Lee’s entrance zone,” [20] anatomically described from the lateral border of the dura to the medial border of the pedicle (white arrow)
Clinical symptoms of patients with spinal canal stenosis include LBP, stiffness, leg paresthesia/weakness, lower-extremity radicular pain, and “neurogenic intermittent claudication” (NIC). Typically, lower-extremity pain associated with NIC is relieved by sitting and lumbar flexion [25].
DLSS based on the location of the pathological process can be classified as central canal, lateral recesses, and neuroforaminal stenoses. Although most patients have a combination of symptoms due to narrowing of more than one zone, the dominant zone affected may predispose to specific symptoms. For instance, patients with central canal stenosis caused by disk and facet degeneration frequently present with NIC and discomfort with standing. This is explained by mechanical compression of the veins, arteries, and descending nerve roots leading to ischemic neuritis (see Fig. 19.1) [26]. The patient’s ability to walk a long distance can be increased by ambulating with a flexed posture, often seen when pushing a shopping trolley [27], referred to as the “shopping cart sign.” On the other hand, patients with lateral recess narrowing have facet osteoarthritis, ligamentum flavum infolding, and paracentral disk bulging/protrusion/extrusion resulting in narrowing of the subarticular zone. These are often seen in conjunction with neuroforaminal narrowing (see Fig. 19.1) [19]. These patients experience pain in a dermatome distribution especially at rest or nighttime. Also, they tend to have a greater walking tolerance in comparison to patients with central canal stenosis [20].
Radiologic findings of spinal canal stenosis do not always correlate with symptoms; the diagnosis is typically based on accurate clinical history and physical examination. Imaging studies are useful to confirm the diagnosis [28], while the degree of impingement on the nerve roots in the lateral recess and neuroforamina seen on imaging has better correlation with clinical symptoms [29, 30]. Patients with degenerative spondylolisthesis may benefit from functional radiographs with flexion-extension to determine the degree of instability.
MRI is seen as the most appropriate, noninvasive test to confirm the presence of spinal canal stenosis or nerve root impingement [25]. Computed tomography (CT) myelography can also be performed as a great alternative. This technique is considered to be as good as the lumbar MRI; however, it requires an intrathecal injection of iodine contrast. In a patient with spinal hardware or contraindication to MRI, this technique improves the accuracy of the diagnosis [31]. When MRI and CT myelography are contraindicated, inconclusive, or inappropriate, CT scan imaging is the preferred modality to confirm the presence of spinal canal stenosis and/or nerve root impingement [25].
Upright MRI is a vertical open magnet able to scan an anatomical region with a weight-bearing position. It has been demonstrated to be useful to assess more accurately lumbar spine instability in patients with concomitant spondylolisthesis and lumbar spinal canal stenosis [32].
Multiple DLSS grading systems have been proposed, but no system has been demonstrated to be superior to another [33, 34]. Most commonly, subjective qualitative criteria are used. Other objective, measurable, and quantitative criteria have been developed (Tables 19.3 and 19.4).
The average spinal canal size has been defined as having a mid-sagittal diameter of more than 11.5 mm and an area of more than 1.45 cm2 [20]. An absolute stenosis is reported when the mid-sagittal diameter of the canal is less than 10 mm and relative stenosis when the mid-sagittal diameter of the canal is between 10 and 13 mm [20].
Image-Guided Percutaneous Techniques for Degenerative Lumbar Spinal Canal Stenosis
Physical therapy, self-care, and medication are the first steps to manage the symptoms of spinal canal stenosis prior to any intervention [24]. However, when conservative treatments fail to improve the patient’s pain, function, and quality of life, interventional therapies can be considered. Several options are now available for patients with spinal canal stenosis: corticosteroid injections, percutaneous image-guided lumbar decompression, interspinous spacers, and surgical decompression. As with all interventional therapies, the success of the intervention highly depends on patient selection [30]. Patient history, physical examination, and accurate imaging review are keys to adequately select the treatment plan [35].
Corticosteroid Injections
Corticosteroid injections are widely used in the treatment of spinal pain due to their effect on local inflammation and subsequent pain decrease [35, 36]; various medication regimens are described in the literature, varying from injection of anesthetic alone to various concentrations of anesthetic and steroids [37]. Also, analysis of the lumbar corticosteroid injection literature is challenging due to significant variation in randomized controlled trial (RCT) design. For instance, variation in approaches (transforaminal, interlaminar, or caudal), control design (active control versus placebo control), technical performance (with or without fluoroscopy), alternative techniques, and outcomes assessment are seen in published papers.
Interlaminar epidural steroid injection (ESI) demonstrated improvement of short to intermediate length for pain related to lumbar spinal stenosis. Systematic reviews support the benefit of caudal, ESI, and transforaminal injections (TFESI) performed with anesthetic alone or with anesthetic in addition to steroid [38,39,40,41,42,43,44]. In a recent systematic review, caudal/interlaminar injections received a Level 2 recommendation, and TFESI received a Level 3 recommendation for the treatment of symptomatic lumbar spinal stenosis [38]. RCTs assessing the efficacy of epidural injections in lumbar central spinal stenosis are described in Table 19.5 [41, 45,46,47,48,49].
Image-guided injections are preferred over blindly performed procedures: blindly performed caudal epidural injections have a rate of inaccurate needle tip placement ranging from 25 to 53%, and lumbar interlaminar epidural injections have a rate of inaccurate placement ranging from 17% to 30% [38, 40]. Image guidance is most frequently performed with fluoroscopy or CT, although other techniques such as ultrasound and MR guidance have been described in the literature [50] (Fig. 19.2a, b). Fusion imaging is also gaining in momentum; these post-processing techniques are able to integrate different imaging modalities, such as ultrasound, with cross-sectional imaging such as MR and/or CT images [36, 51] (Fig. 19.2c).

Image-guided injections. (a) Anteroposterior view of epidural injection fluoroscopically guided. (b) Axial computed tomography (CT)-guided injection; fusion imaging ultrasound CT with virtual needle positioning
The ESI can be performed via interlaminar approach using an 18- or 20-gauge Tuohy needle; after passing the ligamentum flavum, an epidurogram is obtained with a small amount of iodine contrast to confirm the adequate needle tip position within the epidural space [36]; when the needle is correctly placed, injection of 1.0–1.5 mL of particulate long-acting steroid solution (i.e., triamcinolone acetonide or methylprednisolone acetate) mixed with 3 mL of bupivacaine 0.25% and 7 cc of normal saline 0.9% is done [36] (Fig. 19.3). Although rare, severe complications such as infections and epidural hematoma have been reported. The most frequent adverse effect related to ESI is a dural puncture (2.5%) with or without transient headache (2.3%) [52].

Image-guided epidural steroid injection (ESI). (a) Anteroposterior (AP) and lateral view of ESI via interlaminar approach using a 22-gauge needle. (b) AP and lateral view of ESI via trans-articular approach with epidurogram
The TFESI is performed via an oblique posterolateral approach, slipping along the lateral border of the facet joints and targeting the most inferior part of the foramen in order to avoid the nerve root and the arterial vessel [36] (Fig. 19.4). A small amount of iodine contrast is injected in order to verify adequate positioning of the 22-gauge Quincke needle, followed by slow injection of 1.0–1.5 mL of particulate-free steroid solution (i.e., dexamethasone sodium phosphate) mixed with 1 ml of lidocaine 1% or bupivacaine 0.25%. Dexamethasone sodium phosphate particle size is approximately 10 times smaller than red blood cells, the particles do not aggregate, and they have the lowest density compared to other commonly used steroid preparations (e.g., triamcinolone acetonide, methylprednisolone acetate, betamethasone sodium phosphate, and betamethasone acetate). The use of particulate-free corticosteroid has not been related to paraplegia/neurological deficit or any other severe complication [52]. Also, the reported neurologic complications are most likely the results of injury on a low dominant radiculomedullary artery. Typically, the artery of Adamkiewicz is present between T9 and L1; however, in a minority of cases, it can be seen between T7 and L4. The use of particulate-free corticosteroid is recommended for TFESI above L3. One of the trade-offs to the use of a particulate-free corticosteroid may be a shorter duration of action and pain relief.

Image-guided transforaminal epidural steroid injection (TFESI). (a) Oblique (with “Scottie dog” visualization), anteroposterior, and lateral view in order to check the correct placement of the needle for TFESI. (b) Transverse oblique foraminal view for ultrasound-guided TFESI: M multifidus, E erector spinae, Q quadratus lumborum, P psoas, NF neuroforamen, FJ facet joint, VB vertebral body
Percutaneous Image-Guided Lumbar Spinal Canal Decompression
Percutaneous image-guided (CT or fluoroscopy) lumbar decompression (PILD) of the spinal canal is defined as a noninvasive technique to debulk the posterior elements of the spine (lamina and ligamentum flavum). It does not involve the use of implants and is performed ipsilaterally through a 6-gauge introducer. An epidurogram is performed to document the decompression of the spinal canal throughout the procedure and the improved contrast flow. This procedure can be performed bilaterally and at multiple levels. To our knowledge, MILD® (Minimally Invasive Lumbar Decompression, Vertos Medical, Aliso Viejo, CA, USA) is the only image-guided device currently available; moreover, it is the only PILD treatment that has been studied by RCT [19]. Within this study, at 1-year follow-up, Oswestry Disability Index (ODI), Numeric Pain Rating Scale (NPRS), and all three domains of the Zurich Claudication Questionnaire (ZCQ) (symptom severity, physical function, and patient satisfaction) demonstrated statistically significant superiority of MILD versus the active control [53].
Interspinous Spacers
Interspinous spacers or interspinous process devices (IPD) are minimally invasive devices placed under fluoroscopic guidance between two adjacent spinous processes. The goal of the IPD is to relieve nerve compression due to lumbar spinal canal stenosis using distractive forces applied by the spacer and resulting in subsequent segmental height restoration [54].
The IPD positioning decreases facet join overload through a “shock-absorber” mechanism, shifting forces to the posterior column and reducing the intradiscal pressure [54]. Segmental enlargement of the central canal and lateral recesses with the unloading of the facet joint and posterior annulus, resulting in the restoration of normal foraminal height, was reported in cadaveric studies after IPD placement [55, 56].
In the last 10 years, various IPD designs using different materials such as allograft, titanium, and polyetheretherketone (PEEK) have been proposed.
Based on their biomechanical characteristics, the IPDs can be divided into two groups:
-
Interspinous distraction devices (IDD) that act to separate adjacent spinous processes
-
Interspinous stabilizers devices (ISD) that are affixed statically (i.e., X-STOP® Spacer, Medtronic, Minneapolis, MN, USA; Wallis®, Zimmer Biomet, Warsaw, IN, USA; and Superion™, Vertiflex™, Clemente, CA, USA) or dynamically (i.e., coflex®, Paradigm Spine, New York, NY, USA, and Device for Intervertebral Assisted Motion, DIAM®, Medtronic)
A new, completely percutaneous device has been proposed (Lobster® Project, Techlamed, Firenze, Italy). However, no trial has yet been performed with this device (Fig. 19.5). IPDs are more effective than conservative treatments for DLSS. Complications seemed to be more frequent for the implant group compared to the conservative treatment [57, 58]. Table 19.6 summarizes the literature available on current IPDs [59,60,61,62,63,64].

Lobster® device placement procedure. (a) Fluoroscopic anteroposterior (AP) and (b) lateral views show the dilatation tube placed between the spinous processes, keeping it parallel to the coronal plane and centered between the two spinous processes until it reaches the interspinous ligament, which gives a slightly increased resistance. (c) Fluoroscopic AP view shows dilatation tube 02 and the dilatation tube 03; (d) subsequently, the first two dilation tubes (01 and 02) are removed in order to implant the Lobster® device. (e) Fluoroscopic AP view shows the evaluation of the implant size with the probes, starting from the smallest size (yellow handle); the dilatation tube gently pushes the trial implant through the ligament between the two spinous processes in order to evaluate the correct size of the implant. (f) The Lobster® device is subsequently placed on the holder and inserted through the dilatation tube. (g) Fluoroscopic AP view shows the correct implant placement with the saddle reaching the spinous processes; (h) once the device is in the correct position, the wings can be opened. (i, l) Fluoroscopic lateral and AP views show the correct placement of the Lobster® device with the saddle between the two spinous processes. (m) Axial and (n) sagittal multiplanar reformation (MPR) computed tomography shows the correct placement of the device
Low-quality evidence indicated that the pain, function, and quality of life outcomes are comparable when comparing IPD with surgical procedures. However, treatment failure is significantly higher in the IPD group in comparison to decompressive surgery. This is due to device dislocation and spinous process erosion/fracture [58, 62,63,64,65]. Some of those complications are also device and patient dependent; also, spinous process fractures can be avoided with PMMA spinoplasty. Indeed, a retrospective evaluation of 256 patients treated with IPD alone in comparison to 432 patients treated with IPD + PMMA spinoplasty found that the symptom recurrence rate from complications in the spinoplasty group was significantly reduced at 9 years (<1% versus 11.3%) [66]. Also, laminectomy, the alternative intervention, can effectively decompress the offending neural elements and provide symptom relief. However, it can destabilize the spine, leading to re-emergence of symptoms requiring reoperation with instrumented fusion. A recent RCT reported that one-third of laminectomy patients required reoperation with fusion within 4 years [67, 68]. The cost-effectiveness of IPD is still debated [69].
Image-Guided Percutaneous Techniques for Disk Degeneration
Multiple treatments for discogenic back pain are currently under investigation. A significant interest for orthobiologics was seen in the last few years. Although the treatment protocols are not yet clearly defined, it is thought that low-to-intermediate-grade disk degeneration (i.e., modified Pfirrmann grade 3–6) could potentially benefit from intradiscal platelet-rich plasma (PRP) treatments or stem cell treatments. For more advanced disk degeneration (modified Pfirrmann grade 7 and 8) and/or patients with painful endplate degenerative changes Modic type I or II, basivertebral plexus ablation can be performed.
Platelet-Rich Plasma
Platelet-rich plasma is a concentrated form of plasma containing higher content of platelets (approximatively 400% the peripheral blood platelet count). PRP is initially derived from blood by centrifugation, and various protocols can be used to concentrate the number of platelets in the plasma. Until now, PRP was mainly used to treat lesions of the cartilage, ligaments, and tendons [70]. By injecting PRP, various growth factors are released from the platelet α-granules, including epidermal growth factor, fibroblastic growth factor, insulin-like growth factor 1 (IGF-1), vascular endothelial growth factor, platelet-derived epidermal growth factor, transforming growth factor (TGF-β), and platelet-derived epidermal growth factor [71]. Other proteins, cytokines, and chemokines are also released from the α-granules in the platelet cytoplasm. These proteins and growth factors, when activated, participate in complex physiological events leading to tissue repair and regeneration [72].
The use of intradiscal PRP injection for promoting regeneration in patients with IVD disease is relatively new and still controversial. In vivo and in vitro intradiscal PRP injection studies have demonstrated some promising results [12]. For example, TGF-β1 promotes the synthesis of proteoglycans [73, 74] and stimulates the proliferation of annulus fibrosus cells [75]. TGF-β1 and IGF-1 could stimulate the synthesis of sulfated glycosaminoglycans in addition to collagen types I and II [76]. Intradiscal PRP injection was used to decrease LBP in a clinical trial for 14 patients with degenerative disk disease. Patients included in this study had at least one lumbar disk affected that was confirmed with MRI (more than Pfirrmann grade III), and they must have been symptomatic for more than 3 months. The PRP was injected into the center of the nucleus pulposus under fluoroscopic guidance. No imaging abnormalities were found after injection of PRP. No adverse effects were observed, and the pain scores were profoundly decreased at 1 month and sustained throughout the observation period (6 months). Nonetheless, other RCTs should be explored to enable evaluating the efficiency of this method [77].
Another RCT involving 47 patients demonstrated significant pain relief at 8 weeks and significant function improvement at 12 months after the injection of intradiscal PRP [78]. Adipose tissue-derived stem cells suspended in PRP were also used for treating degenerative disk disease, and the benefits of these treatments are currently being studied in ongoing clinical trials [79]. Other clinical studies have demonstrated the potential of using PRP, but RCTs are needed to fully evaluate the efficacy of this treatment [77, 80].
Mesenchymal Stem Cells
Although the amount of published data on intradiscal injection of mesenchymal stem cells (MSCs) is still limited, clinical studies that employed cell therapy have demonstrated promising results across multiple stem cell injectable strategies [79, 81]. For instance, injection of autologous MSCs was previously evaluated in patients with discogenic back pain and degenerative disk disease. Significant improvement in terms of pain and disability was observed. Also, improvement in disability and disk hydration was seen, although disk height was not restored [82]. Containment of MSCs within the disk after percutaneous injection was demonstrated [83].
Similarly, injection of autologous disk-derived chondrocytes resulted in reduced pain and better hydration of the disk but, again, no change in disk height [84]. The injection of colony-forming unit fibroblasts of marrow aspirate also seems to provide significant pain relief in patients with discogenic back pain [85]. The inclusion/exclusion criteria for intradiscal injection of MSC are not yet clearly defined; however, it is likely that those will rely heavily on MRI. For instance, novel clinical trials utilize the modified Pfirrmann grading system to determine eligibility of patients (i.e., modified Pfirrmann grade 3–6) [16].
Basivertebral Plexus Ablation
Intraosseous ablation of the basivertebral nerve (BVN) is a safe and effective minimally invasive treatment for the relief of chronic axial LBP (Modic type I and II endplate degenerative changes). Patients with severely degenerated and painful disks (modified Pfirrmann grading 7 and 8) also have high incidence of endplate degeneration and might be candidates for this minimally invasive procedure.
The BVN exits the vertebral body posteriorly via the basivertebral foramen before communicating with the sinuvertebral nerve and then the ventral rami of the spinal nerves or by nerves derived from the gray rami communicantes. In patients with endplate degeneration, higher density of nerve termination is seen within the endplates [86]. By performing ablation of the BVNs above and underneath the degenerated endplates/disk, there is interruption on the painful afferents passing through the BVNs [80]. The procedure is supported by Level I evidence, including two RCTs demonstrating a statistically significant decrease in pain and an improvement in function with outcomes sustained to at least 24 months [87].
Image-Guided Percutaneous Techniques for Disk Herniation
Percutaneous treatments can be used in the treatment of small- to medium-sized hernias of intervertebral disks. This is achieved by reducing the volume of the nucleus pulposus. Various methods are described, including mechanical, thermal, or chemical techniques. Reduction of the compression/irritation on the nerve root is noted after the intervention [49, 88].
Indications of percutaneous ablative techniques are the following: small- to medium-sized contained intervertebral disk herniation confirmed by MRI; back pain of discogenic origin; sciatica or crural pain that limits activity for at least 6 weeks (leg pain should be of greater intensity than back pain); specific dermatomal pain distribution; neurologic findings referring to a single nerve root involvement (positive Lasègue sign; decreased tendon reflex, sensation, motor responses); no significant improvement after conservative therapy (6 weeks of bed rest, analgesics, anti-inflammatory drugs, muscle relaxants, physiotherapy)—significant improvement is defined as any pain reduction and mobility improvement of >3 units on the Visual Analogue Scale; reproduction of patient’s usual pain in the cases in which provocative discography is performed before any percutaneous intervertebral disk ablative technique [54].
Contraindications include sequestered (free) disk fragment, segmental instability (spondylolisthesis), stenosis of neural foramen or spinal canal, asymptomatic intervertebral disk bulging discovered as incidental finding in CT or MRI, infection and/or diskitis, and pregnancy (radiation exposure of the fetus must be avoided) [54].
Imaging-guided percutaneous intervertebral disk therapies can be divided according to the following techniques.
Percutaneous Mechanical Disk Decompression
Percutaneous disk decompression (PDD) utilizes the Archimedes pump principle in physics to extract a small portion of nucleus pulposus. One example is the Dekompressor® (Stryker, Kalamazoo, MI, USA), which uses a 1.5 mm diameter cannula after insertion of a hollow 17G needle into the disk. This technique does not accelerate disk degeneration (Fig. 19.6) [89].

Dekompressor® procedure. (a) Axial and (b) sagittal multiplanar reformation (MPR) computed tomography (CT) shows the placement of the device. (c) Coronal MPR CT shows the correct placement of the device reaching the nucleus pulposus central portion. (d) Dekompressor® device utilizes the Archimedes pump principle in physics to extract a small portion of nucleus pulposus
Percutaneous Laser Disk Decompression
Percutaneous laser disk decompression (PLDD), performed with a laser fiber introduced fluoroscopically, results in vaporization of a small portion of the nucleus pulposus (Fig. 19.7). PLDD involves inserting an 18-gauge needle into the nucleus pulposus followed by an optical fiber through which a laser is activated. There are several types of laser such as Nd:YAG, KTP, CO2, Ho:YAG, and diode.

Percutaneous laser disk decompression procedure. (a) Fluoroscopic anteroposterior (top) and sagittal (bottom) images show the needle placement. (b) Coronal (top), axial (bottom), and (c) sagittal images show the vaporization of a small portion of nucleus pulposus performed with a laser fiber introduced fluoroscopically into the nucleus pulposus
Percutaneous laser disk coagulation therapy (PDCT) is characterized by a particular targeted laser source, so-called plasma light (range of 550–1800 nm), condensed at the tip of the fiber with a typical dome shape; the temperature ranges from 160 °C (center of the fiber) to 164 °C (3 mm round the fiber) and less than 40 °C at over 3 mm around the fiber in order to accomplish coagulation, evaporation, and disk decompression.
Euthermic diskolysis with holmium (Ho) yttrium-aluminum-garnet (YAG) (Ho:YAG) laser is performed with a particular cool laser (average temperature <45 °C) able to extract pieces but also the fluid portion of the nucleus pulposus, sparing the peripheral portion and the anatomical location of the residual viable fibroblasts, thus avoiding disk collapse.
Percutaneous Disk Decompression with Radiofrequency
Disk nucleoplasty (NP) (Coblation®, ArthroCare Spine, Sunnyvale, CA, USA) is a RF ablation with focused high energy able to destroy intra-molecular bonds within the nucleus; it is a non-heat-driven process, so thermal damage and tissue necrosis are avoided.
Continuous or pulsed radiofrequency generates an electrical current able to obtain necrosis of target tissue through a generator with two electrodes—an active electrode placed in the center of the disk and a dispersive electrode positioned on the patient’s skin. Continuous radio frequency (CRF) involves the constant output of pulses, while pulsed radiofrequency (PRF) consists of short RF pulses applied in the target area with interval of pauses, able to reach below the temperature of 42 °C (temperature of tissue necrosis).
Quantum molecular resonance disk decompression (QMR) is a new RF that combines different frequencies—alternating current with high-frequency waves dispensed through a bipolar electrode (fundamental wave at 4 MHz followed by waves at 8, 12, 16 MHz) in order to destroy the molecular bonds of the nucleus pulposus, sparing the adjacent tissue.
Chemodiskolisys
Chemodiskolysis with ethanol gel (DiscoGel®, Gelscom SAS, Champhol, France) utilizes ethyl alcohol and cellulose derivative products associated with a contrast agent (tungsten); the injection of ethanol gel within the nucleus pulposus causes molecular scission of proteoglycans and glycosaminoglycans, leading to degradation of these components and loss of their water-retaining capacity, resulting in dehydration and chemical decompression of the disk.
Chemodiskolysis with oxygen-ozone is able to reduce inflammation as a result of its oxidizing effect on pain-producing mediators; moreover, the injection of ozone can also inhibit synthesis and secretion of collagen molecules, leading to rapid pain relief. The ozone has direct action on the mucopolysaccharides of the nucleus pulposus with rupture of water molecules and shrinkage of the disk exerting compression on the nerve roots; moreover, it improves microcirculation due to resolution of venous stasis and lack of oxygenated blood supply following mechanical compression of the herniated disk and disk protrusion on the vessel components.
Intradiscal Electrothermal Therapy
Intradiscal electrothermal therapy (IDET) is performed by placing a thermal catheter in the posterior part of the annulus fibrosus by an introducer needle connected to a generator; the fiber achieves 90° for 17 minutes in order to obtain thermocoagulation of nerve fibers and nocireceptors.
A 17-gauge Crawford needle is used for NP, PDD, QMR, and IDET, the 18- or 21-gauge Chiba needle for PLDD, and an 18-gauge Chiba for chemodiskolysis with ethanol gel and Ho:YAG laser, while a 21-gauge Chiba needle is necessary for chemodiskolysis with oxygen ozone.
The intradiscal advancement of the needle is monitored fluoroscopically by anteroposterior and lateral projections, since the tip must reach the nucleus pulposus central portion. The operator can expect mild/hard elastic resistance in crossing the annulus, which the patient may possibly experience as pain in this highly innervated zone [54].
A recent review demonstrated that PDD and NP have the best level of evidence with a score of 2B+ [82]. The PDD series demonstrated good clinical outcomes in a selected population, with success rate up to 75%; the NP series reported a success rate of 80% with a complication rate of 1.8% [90]. The other techniques are supported mainly by observational studies with scores ranging between 0 and 2B± [89].
PLDD reported a high success rate (78%), with improvement of patient function with immediate and sustained significant pain relief (up to 71% at 53 months of follow-up). However, a high rate of complication is seen in comparison to the other laser treatments [91].
PDCT has recently demonstrated a high effective and safety profile for cervical and lumbar hernia resistant to conservative treatment [92].
Research publications devoted to Ho:YAG laser treatment demonstrated pain relief and improvement of quality of life with a success rate of 80%. Moreover, the technique showed a high safety profile, as it delivers less energy in comparison with conventional PLDD, which adopts a non-selective laser. Thus, Ho:YAG laser interventions are recommended for young patients and with a single-level disease [93].
PRF is more effective than CRF in discogenic LBP; however, its efficacy decreases with time. At 6 months, 22.9% of patients have 50% of pain relief versus 13.1% at 12 months. Other studies reported a good efficacy of DRG-PRF to treat chronic sciatic pain [94].
References
Otani K, Kikuchi S, Yabuki S, Igarashi T, Nikaido T, Watanabe K, Konno S. Lumbar spinal stenosis has a negative impact on quality of life compared with other comorbidities: an epidemiological cross-sectional study of 1862 community-dwelling individuals. ScientificWorldJournal. 2013;2013:590652.
Abdi S, Datta S, Trescot AM, Schultz DM, Adlaka R, Atluri SL, et al. Epidural steroids in the management of chronic spinal pain: a systematic review. Pain Physician. 2007;10(1):185–212.
Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–74.
Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–24.
Ravindra VM, Senglaub SS, Rattani A, Dewan MC, Härtl R, Bisson E, Park KB, Shrime MG. Degenerative lumbar spine disease: estimating global incidence and worldwide volume. Global Spine J. 2018;8(8):784–94.
DePalma MJ, Ketchum JM, Saullo T. What is the source of chronic low back pain and does age play a role? Pain Med. 2011;12(2):224–33.
Kalichman L, Cole R, Kim DH, Li L, Suri P, Guermazi A, Hunter DJ. Spinal stenosis prevalence and association with symptoms: the Framingham Study. Spine J. 2009;9(7):545–50.
Jensen MC, Brant-Zawadzki MN, Obuchowski N, Modic MT, Malkasian D, Ross JS. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med. 1994;331(2):69–73.
Keshari KR, Lotz JC, Link TM, Hu S, Majumdar S, Kurhanewicz J. Lactic acid and proteoglycans as metabolic markers for discogenic back pain. Spine (Phila Pa 1976). 2008;33(3):312–7.
Antoniou J, Steffen T, Nelson F, Winterbottom N, Hollander AP, Poole RA, et al. The human lumbar intervertebral disc: evidence for changes in the biosynthesis and denaturation of the extracellular matrix with growth, maturation, ageing, and degeneration. J Clin Invest. 1996;98(4):996–1003.
García-Cosamalón J, del Valle ME, Calavia MG, García-Suárez O, López-Muñiz A, Otero J, Vega JA. Intervertebral disc, sensory nerves and neurotrophins: who is who in discogenic pain? J Anat. 2010;217(1):1–15.
Wang SZ, Rui YF, Tan Q, Wang C. Enhancing intervertebral disc repair and regeneration through biology: platelet-rich plasma as an alternative strategy. Arthritis Res Ther. 2013;15(5):220.
Pezet S, McMahon SB. Neurotrophins: mediators and modulators of pain. Annu Rev Neurosci. 2006;29(1):507–38.
Malik KM, Cohen SP, Walega DR, Benzon HT. Diagnostic criteria and treatment of discogenic pain: a systematic review of recent clinical literature. Spine J. 2013;13(11):1675–89.
Pfirrmann CWA, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976). 2001;26(17):1873–8.
Griffith JF, Wang YX, Antonio GE, Choi KC, Yu A, Ahuja AT, Leung PC. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine (Phila Pa 1976). 2007;32(24):E708–12.
Fardon DF, Williams AL, Dohring EJ, Murtagh FR, Gabriel Rothman SL, Sze GK. Lumbar disc nomenclature: version 2.0: recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology, and the American Society of Neuroradiology. Spine (Phila Pa 1976). 2014;39(24):E1448–65.
Singh K, Samartzis D, Vaccaro AR, Nassr A, Andersson GB, Yoon ST, et al. Congenital lumbar spinal stenosis: a prospective, control-matched, cohort radiographic analysis. Spine J. 2005;5(6):615–22.
Lee SY, Kim TH, Oh JK, Lee SJ, Park MS. Lumbar stenosis: a recent update by review of literature. Asian Spine J. 2015;9(5):818–28.
Lee CK, Rauschning W, Glenn W. Lateral lumbar spinal canal stenosis: classification, pathologic anatomy and surgical decompression. Spine (Phila Pa 1976). 1988;13(3):313–20.
Buckwalter JA. Aging and degeneration of the human intervertebral disc. Spine (Phila Pa 1976). 1995;20(11):1307–14.
Epstein JA, Epstein BS, Lavine LS, Carras R, Rosenthal AD, Sumner P. Lumbar nerve root compression at the intervertebral foramina caused by arthritis of the posterior facets. J Neurosurg. 1973;39(3):362–9.
Schroeder GD, Kurd MF, Vaccaro AR. Lumbar spinal stenosis: how is it classified? J Am Acad Orthop Surg. 2016;24(12):843–52.
Backstrom KM, Whitman JM, Flynn TW. Lumbar spinal stenosis-diagnosis and management of the aging spine. Man Ther. 2011;16(4):308–17.
Kreiner DS, Shaffer WO, Baisden JL, Gilbert TJ, Summers JT, Toton JF, et al. North American Spine Society. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update). Spine J. 2013;13(7):734–43.
Rydevik B, Brown MD, Lundborg G. Pathoanatomy and pathophysiology of nerve root compression. Spine (Phila Pa 1976). 1984;9(1):7–15.
Issack PS, Cunningham ME, Pumberger M, Hughes AP, Cammisa FP. Degenerative lumbar spinal stenosis: evaluation and management. J Am Acad Orthop Surg. 2012;20(8):527–35.
Amundsen T, Weber H, Lilleas F, Nordal HJ, Abdelnoor M, Magnaes B. Lumbar spinal stenosis. Clinical and radiologic features. Spine (Phila Pa 1976). 1995;20(10):1178–86.
Deer TR, Grider JS, Pope JE, Falowski S, Lamer TJ, Calodney A, et al. The MIST guidelines: the lumbar spinal stenosis consensus group guidelines for minimally invasive spine treatment. Pain Pract. 2019;19(3):250–74.
Buy X, Gangi A. Percutaneous treatment of intervertebral disc herniation. Semin Intervent Radiol. 2010;27(2):148–59.
Bischoff RJ, Rodriguez RP, Gupta K, Righi A, Dalton JE, Whitecloud TS. A comparison of computed tomography-myelography, magnetic resonance imaging, and myelography in the diagnosis of herniated nucleus pulposus and spinal stenosis. J Spinal Disord. 1993;6(4):289–95.
Splendiani A, Perri M, Grattacaso G, Di Tunno V, Marsecano C, Panebianco L, et al. Magnetic resonance imaging (MRI) of the lumbar spine with dedicated G-scan machine in the upright position: a retrospective study and our experience in 10 years with 4305 patients. Radiol Med. 2016;121(1):38–44.
Andreisek G, Imhof M, Wertli M, Winklhofer S, Pfirrmann CW, Hodler J, Steurer J, Lumbar Spinal Stenosis Outcome Study Working Group Zurich. A systematic review of semiquantitative and qualitative radiologic criteria for the diagnosis of lumbar spinal stenosis. AJR Am J Roentgenol. 2013;201(5):W735–46.
Andreisek G, Hodler J, Steurer J. Uncertainties in the diagnosis of lumbar spinal stenosis. Radiology. 2011;261(3):681–4.
Palmer WE. Spinal injections for pain management. Radiology. 2016;281(3):669–88.
Marcia S, Zini C, Hirsch JA, Chandra RV, Bellini M. Steroids spinal injections. Semin Intervent Radiol. 2018;35(4):290–8.
Knezevic NN, Jovanovic F, Voronov D, Candido KD. Do corticosteroids still have a place in the treatment of chronic pain? Front Pharmacol. 2018;9:1229.
Manchikanti L, Kaye AD, Manchikanti K, Boswell M, Pampati V, Hirsch J. Efficacy of epidural injections in the treatment of lumbar central spinal stenosis: a systematic review. Anesthesiol Pain Med. 2015;5(1):34–41.
Manchikanti L, Buenaventura RM, Manchikanti KN, Ruan X, Gupta S, Smith HS, et al. Effectiveness of therapeutic lumbar transforaminal epidural steroid injections in managing lumbar spinal pain. Pain Physician. 2012;15(3):E199–245.
Benyamin RM, Manchikanti L, Parr AT, Diwan S, Singh V, Falco FJ, Datta S, Abdi S, Hirsch JA. The effectiveness of lumbar interlaminar epidural injections in managing chronic low back and lower extremity pain. Pain Physician. 2012;15(4):E363–404.
Manchikanti L, Cash KA, McManus CD, Pampati V, Fellows B. Results of 2-year follow-up of a randomized, double-blind, controlled trial of fluoroscopic caudal epidural injections in central spinal stenosis. Pain Physician. 2012;15(5):371–84.
Manchikanti L, Cash KA, McManus CD, Damron KS, Pampati V, Falco FJE. A randomized, double-blind controlled trial of lumbar interlaminar epidural injections in central spinal stenosis: 2-year follow-up. Pain Physician. 2015;18(1):79–92.
Ammendolia C, Stuber K, de Bruin LK, Furlan AD, Kennedy CA, Rampersaud YR, et al. Nonoperative treatment of lumbar spinal stenosis with neurogenic claudication: a systematic review. Spine (Phila Pa 1976). 2012;37(10):E609–16.
Parr AT, Manchikanti L, Hameed H, Conn A, Manchikanti KN, Benyamin RM, et al. Caudal epidural injections in the management of chronic low back pain: a systematic appraisal of the literature. Pain Physician. 2012;15(3):E159–98.
Manchikanti L, Cash KA, McManus CD, Pampati V, Benyamin RM. Thoracic interlaminar epidural injections in managing chronic thoracic pain: a randomized, double-blind, controlled trial with a 2-year follow-up. Pain Physician. 2014;17(3):E327–38.
Lee JH, An JH, Lee SH. Comparison of the effectiveness of interlaminar and bilateral transforaminal epidural steroid injections in treatment of patients with lumbosacral disc herniation and spinal stenosis. Clin J Pain. 2009;25(3):206–10.
Wilson-MacDonald J, Burt G, Griffin D, Glynn C. Epidural steroid injection for nerve root compression: a randomised, controlled trial. J Bone Joint Surg Br. 2005;87-B(3):352–5.
Fukusaki M, Kobayashi I, Hara T, Sumikawa K. Symptoms of spinal stenosis do not improve after epidural steroid injection. Clin J Pain. 1998;14(2):148–51.
Nam HS, Park YB. Effects of transforaminal injection for degenerative lumbar scoliosis combined with spinal stenosis. Ann Rehabil Med. 2011;35(4):514–23.
Shim E, Lee JW, Lee E, Ahn JM, Kang Y, Kang HS. Fluoroscopically guided epidural injections of the cervical and lumbar spine. Radiographics. 2017;37(2):537–61.
Provenzano DA, Narouze S. Sonographically guided lumbar spine procedures. J Ultrasound Med. 2013;32(7):1109–16.
Van Boxem K, Cheng J, Patijn J, van Kleef M, Lataster A, Mekhail N, Van Zundert J. 11. Lumbosacral radicular pain. Pain Pract. 2010;10(4):339–58.
Benyamin RM, Staats PS. MILD® is an effective treatment for lumbar spinal stenosis with neurogenic claudication: MiDAS ENCORE randomized controlled trial. Pain Physician. 2016;19(4):229–42.
Kelekis AD, Somon T, Yilmaz H, Bize P, Brountzos EN, Lovblad K, et al. Interventional spine procedures. Eur J Radiol. 2005;55(3):362–83.
Hirsch C, Breque C, Ragot S, Pascal-Mousselard H, Richer JP, Scepi M, Khiami F. Biomechanical study of dynamic changes in L4–L5 foramen surface area in flexion and extension after implantation of four interspinous process devices. Orthop Traumatol Surg Res. 2015;101(2):215–9.
Richards JC, Majumdar S, Lindsey DP, Beaupré GS, Yerby SA. The treatment mechanism of an interspinous process implant for lumbar neurogenic intermittent claudication. Spine (Phila Pa 1976). 2005;30(7):744–9.
Anderson PA, Tribus CB, Kitchel SH. Treatment of neurogenic claudication by interspinous decompression: application of the X STOP device in patients with lumbar degenerative spondylolisthesis. J Neurosurg Spine. 2006;4(6):463–71.
Gala RJ, Russo GS, Whang PG. Interspinous implants to treat spinal stenosis. Curr Rev Musculoskelet Med. 2017;10(2):182–8.
Zucherman JF, Hsu KY, Hartjen CA, Mehalic TF, Implicito DA, Martin MJ, Johnson DR 2nd, Skidmore GA, Vessa PP, Dwyer JW, Puccio ST, Cauthen JC, Ozuna RM. A multicenter, prospective, randomized trial evaluating the X STOP interspinous process decompression system for the treatment of neurogenic intermittent claudication: two-year follow-up results. Spine (Phila Pa 1976). 2005;30(12):1351–8.
Azzazi A, Elhawary Y. Dynamic stabilization using X-Stop® versus transpedicular screw fixation in the treatment of lumbar canal stenosis; comparative study of the clinical outcome. Neurosurg Q. 2010;20(3):165–9.
Strömqvist BH, Berg S, Gerdhem P, Johnsson R, Möller A, Sahlstrand T, et al. X-STOP® versus decompressive surgery for lumbar neurogenic intermittent claudication: randomized controlled trial with 2-year follow-up. Spine (Phila Pa 1976). 2013;38(17):1436–42.
Davis RJ, Errico TJ, Bae H, Auerbach JD. Decompression and coflex interlaminar stabilization compared with decompression and instrumented spinal fusion for spinal stenosis and low-grade degenerative spondylolisthesis: two-year results from the prospective, randomized, multicenter, food and drug. Spine (Phila Pa 1976). 2013;38(18):1529–39.
Moojen WA, Arts MP, Jacobs WC, van Zwet EW, van den Akker-van Marle ME, Koes BW, et al. Leiden The Hague Spine Intervention Prognostic Study Group (SIPS). IPD without bony decompression versus conventional surgical decompression for lumbar spinal stenosis: 2-year results of a double-blind randomized controlled trial. Eur Spine J. 2015;24(10):2295–305.
Lønne G, Johnsen LG, Rossvoll I, Andresen H, Storheim K, Zwart JA, Nygaard ØP. Minimally invasive decompression versus X-STOP® in lumbar spinal stenosis: a randomized controlled multicenter study. Spine (Phila Pa 1976). 2015;40(2):77–85.
Pintauro M, Duffy A, Vahedi P, Rymarczuk G, Heller J. Interspinous implants: are the new implants better than the last generation? A review. Curr Rev Musculoskelet Med. 2017;10(2):189–98.
Manfre L, De Vivo AE, Al Qatami H, Own A, Ventura F, Zhou K, et al. Successful use of percutaneous interspinous spacers and adjunctive spinoplasty in a 9 year cohort of patients. J Neurointerv Surg. 2020;12(7):673–7.
Nunley PD, Patel VV, Gorndorff D, Lavelle WF, Block JE, Geisler FH. Five-year durability of stand-alone interspinous process decompression for lumbar spinal stenosis. Clin Interv Aging. 2017;12:1409–17.
Ghogawala Z, Dziura J, Butler WE, Dai F, Terrin N, Magge SN, et al. Laminectomy plus fusion versus laminectomy alone for lumbar spondylolisthesis. N Engl J Med. 2016;374(15):1424–34.
Zini C, Bellini M, Masala S, Marcia S. Percutaneous interspinous spacer in spinal-canal-stenosis treatment: pros and cons. Medicina. 2019;55(7):1–9.
Arora S, Agnihotri N. Platelet derived biomaterials for therapeutic use: review of technical aspects. Indian J Hematol Blood Transfus. 2017;33(2):159–67.
Kon E, Filardo G, Di Martino A, Marcacci M. Platelet-rich plasma (PRP) to treat sports injuries: evidence to support its use. Knee Surg Sports Traumatol Arthrosc. 2011;19(4):516–27.
Golebiewska EM, Poole AW. Platelet secretion: from haemostasis to wound healing and beyond. Blood Rev. 2015;29(3):153–62.
Nishida K, Kang JD, Gilbertson LG, Moon SH, Suh JK, Vogt MT, et al. Modulation of the biologic activity of the rabbit intervertebral disc by gene therapy: an in vivo study of adenovirus-mediated transfer of the human transforming growth factor beta 1 encoding gene. Spine (Phila Pa 1976). 1999;24(23):2419–25.
Müller T, Bain G, Wang X, Papkoff J. Regulation of epithelial cell migration and tumor formation by β-catenin signaling. Exp Cell Res. 2002;280(1):119–33.
Gruber HE, Fisher EC, Desai B, Stasky AA, Hoelscher G, Hanley EN. Human intervertebral disc cells from the annulus: three-dimensional culture in agarose or alginate and responsiveness to TGF-β1. Exp Cell Res. 1997;235(1):13–21.
Hayes AJ, Ralphs JR. The response of foetal annulus fibrosus cells to growth factors: modulation of matrix synthesis by TGF-β1 and IGF-1. Histochem Cell Biol. 2011;136(2):163–75.
Akeda K, Ohishi K, Masuda K, Bae WC, Takegami N, Yamada J, et al. Intradiscal injection of autologous platelet-rich plasma releasate to treat discogenic low back pain: a preliminary clinical trial. Asian Spine J. 2017;11(3):380–9.
Tuakli-Wosornu YA, Terry A, Boachie-Adjei K, Harrison JR, Gribbin CK, LaSalle EE, et al. Lumbar intradiscal platelet-rich plasma (PRP) injections: a prospective, double-blind, randomized controlled study. PM R. 2016;8(1):1–10; quiz 10.
Pennicooke B, Moriguchi Y, Hussain I, Bonssar L, Härtl R. Biological treatment approaches for degenerative disc disease: a review of clinical trials and future directions. Cureus. 2016;8(11):e892.
Levi D, Horn S, Tyszko S, Levin J, Hecht-Leavitt C, Walko E. Intradiscal platelet-rich plasma injection for chronic discogenic low back pain: preliminary results from a prospective trial. Pain Med. 2016;17(6):1010–22.
Sakai D, Schol J. Cell therapy for intervertebral disc repair: clinical perspective. J Orthop Translat. 2017;9:8–18.
Orozco L, Soler R, Morera C, Alberca M, Sánchez A, García-Sancho J. Intervertebral disc repair by autologous mesenchymal bone marrow cells: a pilot study. Transplantation. 2011;92(7):822–8.
Prologo JD, Pirasteh A, Tenley N, Yuan L, Corn D, Hart D, et al. Percutaneous image-guided delivery for the transplantation of mesenchymal stem cells in the setting of degenerated intervertebral discs. J Vasc Interv Radiol. 2012;23(8):1084–8.e6.
Meisel HJ, Siodla V, Ganey T, Minkus Y, Hutton WC, Alasevic OJ. Clinical experience in cell-based therapeutics: disc chondrocyte transplantation A treatment for degenerated or damaged intervertebral disc. Biomol Eng. 2007;24(1):5–21.
Pettine KA, Murphy MB, Suzuki RK, Sand TT. Percutaneous injection of autologous bone marrow concentrate cells significantly reduces lumbar discogenic pain through 12 months. Stem Cells. 2015;33(1):146–56.
Antonacci MD, Mody DR, Heggeness MH. Innervation of the human vertebral body: a histologic study. J Spinal Disord. 1998;11(6):526–31.
Lorio M, Clerk-Lamalice O, Beall DP, Julien T. International Society for the Advancement of Spine Surgery Guideline—Intraosseous ablation of the basivertebral nerve for the relief of chronic low back pain. Int J Spine Surg. 2020;14(1):7002.
Kelekis AD, Filippiadis DK, Martin JB, Brountzos E. Standards of practice: quality assurance guidelines for percutaneous treatments of intervertebral discs. Cardiovasc Intervent Radiol. 2010;33(5):909–13.
Ong D, Chua NHL, Vissers K. Percutaneous disc decompression for lumbar radicular pain: a review article. Pain Pract. 2016;16(1):111–26.
Ren DJ, Liu XM, Du SY, Sun TS, Zhang ZC, Li F. Percutaneous nucleoplasty using coblation technique for the treatment of chronic nonspecific low back pain: 5-year follow-up results. Chin Med J. 2015;128(14):1893–7.
Gangi A, Dietemann JL, Ide C, Brunner P, Klinkert A, Warter JM. Percutaneous laser disk decompression under CT and fluoroscopic guidance: indications, technique, and clinical experience. Radiographics. 1996;16(1):89–96.
Zini C, Notaro D, Sadotti G, Zini G, Monti L, Bellini M. Percutaneous intervertebral disc coagulation therapy (pdct) by plasma light: preliminary data from the first experience in Europe. Cardiovasc Intervent Radiol. 2020;43(1):94–102.
Agarwal S, Bhagwat AS. Ho: Yag laser-assisted lumbar disc decompression: a minimally invasive procedure under local anesthesia. Neurol India. 2003;51(1):35–8.
Van Boxem K, de Meij N, Patijn J, Wilmink J, van Kleef M, Van Zundert J, Kessels A. Predictive factors for successful outcome of pulsed radiofrequency treatment in patients with intractable lumbosacral radicular pain. Pain Med. 2016;17(7):1233–40.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Marcia, S., Zini, C., Bellini, M., Clerk-Lamalice, O. (2021). Minimally Invasive Percutaneous Treatment of Lumbar Disk Degeneration and Stenosis. In: Khan, M., Kushchayev, S.V., Faro, S.H. (eds) Image Guided Interventions of the Spine. Springer, Cham. https://doi.org/10.1007/978-3-030-80079-6_19
Download citation
DOI: https://doi.org/10.1007/978-3-030-80079-6_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-80078-9
Online ISBN: 978-3-030-80079-6
eBook Packages: MedicineMedicine (R0)