
Abstract
Purpose
The effect of prehospital epinephrine on neurological outcome in out-of-hospital cardiac arrest (OHCA) is still controversial. We sought to determine whether prehospital epinephrine administration was associated with improved outcomes in adult OHCA.
Methods
A nationwide, population-based, propensity score-matched study of OHCA patients from January 1, 2011, to December 31, 2012, in Japan was conducted. We included adult OHCA patients treated by emergency medical service personnel without an excessive delay. The primary outcome was neurologically favorable survival 1 month after OHCA.
Results
A total of 237,068 patients (16,616 with a shockable rhythm and 220,452 with a non-shockable rhythm) were included in the final cohort. A total of 4024 out of the 16,616 shockable OHCAs and 29,393 out of the 220,452 non-shockable OHCAs received prehospital epinephrine. In the propensity score-matched cohort, prehospital epinephrine was associated with a decreased chance of neurologically favorable survival (shockable OHCA 7.6 vs. 17.9 %, OR 0.38 [95%CI 0.33–0.43]; non-shockable OHCA 0.6 vs. 1.2 %, OR 0.47 [95%CI 0.39–0.56]). In the subgroup analyses, prehospital epinephrine was significantly associated with poor neurological outcome in all subgroups. In the ancillary analyses, although the neurological outcome was worse as the number of epinephrine doses increased or the time to epinephrine increased, patients had a greater chance of a favorable neurological outcome only when a single dose of epinephrine was administered within 15 min of the emergency call in shockable OHCA.
Conclusions
Among adult OHCA patients, prehospital epinephrine was associated with a decreased chance of neurologically favorable survival. Situations in which prehospital epinephrine is effective may be extremely limited.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although recommendations on epinephrine for out-of-hospital cardiac arrest (OHCA) have been weakened with each revision of the international guidelines on cardiopulmonary resuscitation (CPR), standard-dose epinephrine (1 mg every 3 to 5 min) is nevertheless still recommended in the 2015 guidelines [1, 2]. While numerous studies have shown that epinephrine administration in OHCA increases prehospital return of spontaneous circulation (ROSC) and hospital admission, they conversely suggest that it may also result in adverse survival and neurological outcomes [3–6]. However, epinephrine may have a favorable effect on survival and neurological outcome depending on initial cardiac rhythm or bystander witness status [7]. Additionally, its effect may differ depending on the timing or frequency of administration [8–10]. Thus, while it may be that the weak recommendation of epinephrine in the resuscitation algorithm was retained due to numerous remaining uncertainties, providing an epinephrine recommendation as a simple, standardized method may not be reasonable. Moreover, many studies on the effects of epinephrine reflect the resuscitation practices prior to 2010, and their applicability to current circumstances (after 2010) is questionable.
We therefore investigated the effects of epinephrine using national administrative data from 2011 to 2012. Because prior studies have suggested that the effects of epinephrine depend on differences in initial cardiac rhythm, we investigated the effects of epinephrine in both shockable and non-shockable rhythms. We furthermore examined the effects of the timing and frequency of administration on patient outcome.
Materials and methods
Study design, setting, and participants
We used the All-Japan Utstein Registry database. The database is managed by the Fire and Disaster Management Agency (FDMA). The details of the registry and the emergency medical service (EMS) system in Japan have been described previously [6, 7, 11–13]. In brief, the All-Japan Utstein Registry database is a nationwide, population-based, prospective registry of all OHCAs. All patients with OHCA (defined as pulselessness, apnea, and unresponsiveness) for whom resuscitation was attempted by EMS personnel were identified and followed, including patients with do-not-resuscitate (DNR) orders. In Japan, EMS personnel are legally obliged to attempt resuscitation, except in specific situations, such as decapitation, rigor mortis, livor mortis, and decomposition. Therefore, almost all OHCA patients are transported to an emergency hospital.
The registry uses standardized Utstein-style templates for OHCA to facilitate uniform reporting with precisely defined variables and outcomes [14, 15]. The data are collected from three sources: 119 dispatch centers, fire stations, and receiving hospitals. The data forms are completed by EMS personnel, and the data are integrated into the All-Japan Utstein Registry system on the FDMA database server. The integrity of data is ensured through rigorous certification by a data entry specialist, and the completeness and accuracy of the data are checked by standardized software.
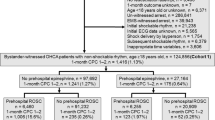
The cohort included data submitted to the All-Japan Utstein Registry from January 1, 2011, to December 31, 2012. We included adult patients aged 18 years or older. Patients with a delay in treatment (the time from call to contact with patient or epinephrine administration >60 min and the time from contact with patient to hospital arrival >120 min) were excluded because they may had abnormal prehospital setting and outcomes. In addition, patients with missing, incomplete, inconsistent, or unknown data on time, first documented rhythm, etiology of cardiac arrest, or prehospital advanced life support were excluded from the analysis. Patients with missing or unknown data accounted for approximately 5.3 % of the total patients (Fig. 1).

Patient flow chart
This study was conducted in accordance with the amended Declaration of Helsinki. The institutional review board of the University of Tokyo approved the study with a waiver of informed consent because of the anonymous nature of the data (no. 10096).
Data collection
Data concerning sex, age, bystander witness, bystander CPR, public-access automated external defibrillator (AED), first documented rhythm, etiology of cardiac arrest, and prehospital advanced life support (i.e., information on epinephrine administration and advanced airway management) were collected. A series of EMS times (call receipt, vehicle arrival at the scene, contact with patient, initiation of CPR, epinephrine administration, prehospital ROSC, and hospital arrival) were also recorded. The etiology of cardiac arrest for patients admitted to the hospital was probed during the hospital stay. On the other hand, for patients who died without hospital admission, the etiology of cardiac arrest was determined by the attending physicians at the emergency department in collaboration with the EMS personnel or coroners based on the witness information, clinical course, medical history, physical findings, examination findings, imaging, and autopsy. If there were no evidence that suggested a noncardiac etiology, then the etiology was presumed to be cardiac [15].
Patients were followed up at 1 month by the EMS personnel to collect data on 1-month survival and neurological status and to reconfirm the etiology of cardiac arrest. The medical control director of the hospital provided information on the patient unless the patient was transferred to another hospital within 1 month. If transferred, then the EMS personnel conducted the follow-up investigation.
The primary outcome was favorable neurological status at 1 month after OHCA. The secondary outcomes were 1-month survival, prehospital ROSC, and time from contact with patient to hospital arrival. The neurological status was assessed with the Glasgow-Pittsburgh cerebral performance category (CPC) scores by the attending physician in charge of the patient. A CPC score of 1 or 2 (good performance or moderate disability, respectively) was defined as a favorable neurological outcome, and a CPC score of 3, 4, or 5 (severe disability, vegetative state, or death, respectively) as a poor neurological outcome [15, 16].
Statistical analysis
The baseline characteristics were described as counts with proportions for categorical variables and means with standard deviations for continuous variables. The t test was used to compare continuous variables, and the χ 2 test was used to compare categorical variables.
Because the data lacked randomization, a propensity score approach was used to control for selection bias and confounding. A propensity score for prehospital epinephrine administration for each patient was estimated by using a multivariable logistic regression model. The following variables were included in the model: sex, age, bystander witness, bystander CPR, public-access AED (PAD), first documented rhythm, etiology of cardiac arrest, prehospital advanced airway management, and time from call to contact with patient. The c statistic was used to assess goodness-of-fit. A 1:1 nearest-neighbor matching was performed on the propensity score with a caliper ≤0.2 and without replacement between patients who received and did not receive prehospital epinephrine [17]. We assessed the success of the propensity-matching procedure by comparing the distribution of patient characteristics in the matched cohort.
In the propensity score-matched cohort, we used a univariable logistic regression model to compare the frequency of each outcome for patients who received and did not receive prehospital epinephrine and to estimate odds ratios (OR) with 95 % confidence intervals (CI). We further examined the association between prehospital epinephrine administration and the outcomes of various subgroups based on sex (male or female), age (18–64 or ≥65 years), bystander witness (presence or absence), bystander CPR (presence or absence), etiology of cardiac arrest (cardiac or noncardiac), cardiac rhythm (VF or VT for shockable rhythm, and PEA or asystole for non-shockable rhythm), and time from call to contact with patient (< 7 or ≥7 min). For each subgroup, the association of epinephrine administration with each outcome was estimated in a logistic regression model that included a treatment variable (with or without prehospital epinephrine administration) and the same covariates listed previously for the estimation of the propensity score, and adjusted ORs with 95 % CIs were reported.
In addition, we performed ancillary analyses that focused on the frequency of epinephrine administration and the time to epinephrine administration. We calculated the ORs with 95 % CIs for each outcome depending on the number of epinephrine doses, with no epinephrine administration as the reference. For patients who received epinephrine, the ORs for a 1-min increment of time to epinephrine administration and their 95 % CIs for each outcome were calculated for the total cohort and for subgrouped cohorts with and without witness. In addition, to estimate the time limit for successful epinephrine administration, we evaluated the association of time to epinephrine administration (0–15, 16–20, 21–25, 26–30, or ≥31 min after emergency call) with favorable outcomes, depending on the number of epinephrine doses (1, 2, ≥3 times). No adjustments were made for ancillary analyses, and thus, the findings from those analyses were exploratory.
All of the tests were two sided at a significance level of 0.05. All of the statistical analyses were performed with JMP Pro 11.0.0 software (SAS Institute Inc., Cary, NC, USA).
Results
During the study period, we identified 237,068 adult OHCA patients who received treatment without a delay (Fig. 1); 16,616 (7.0 %) had a shockable initial rhythm, and 220,452 (93.0 %) had a non-shockable initial rhythm. Of the 16,616 shockable OHCAs, 4024 (24.2 %) received epinephrine and 4020 patients who received epinephrine were matched with 4020 patients who did not. Of the 220,452 non-shockable OHCA, 29,393 (13.3 %) received epinephrine and 29,380 patients who received epinephrine were matched with 29,380 who did not receive.
The baseline characteristics of the total cohort and the propensity score-matched cohort in the shockable OHCA group are shown in Table 1, and those in the non-shockable OHCA group are in Table 2. In both shockable and non-shockable OHCA, there were imbalances between the groups with and without epinephrine administration in the unmatched cohort. In the propensity score-matched cohorts, the baseline characteristics were similar between the two groups.
The clinical outcomes of patients who received and did not receive epinephrine in the propensity score-matched cohort are summarized in Table 3. Although prehospital epinephrine administration was associated with increased prehospital ROSC after non-shockable OHCA, patients who received epinephrine had a poorer 1-month neurological outcome than those who did not (0.6 vs. 1.2 %, OR 0.47 [95%CI 0.39–0.56]). In shockable OHCA, prehospital epinephrine administration was associated with a decreased 1-month survival (16.4 vs. 27.0 %, OR 0.53 [95%CI 0.47–0.59]) and a poorer neurological survival (7.6 vs. 17.9 %, OR 0.38 [95%CI 0.33–0.43]) compared with those who had no prehospital epinephrine administration, and not associated with prehospital ROSC (P = 0.0524). In addition, patients with prehospital epinephrine administration had approximately a 5-min delay in hospital arrival compared with those without.
In the subgroup analyses, prehospital epinephrine administration was significantly associated with poor neurological outcome in all subgroups (online-only supplemental Tables 1, 2, and 3). Prehospital epinephrine administration was associated with increased 1-month survival only in unwitnessed non-shockable OHCA cases and asystole cases.
In the ancillary analysis that focused on the number of epinephrine doses, an increased dose was generally associated with a stepwise decrease in 1-month survival and neurologically favorable survival (online-only supplemental Figure). In shockable OHCA, patients with single dose of epinephrine had a better chance of prehospital ROSC than those without epinephrine (OR 1.28, 95%CI 1.12–1.46). In non-shockable OHCA, compared with no epinephrine administration, epinephrine administration was associated with increased prehospital ROSC, regardless of the number of doses. In addition, a single dose of epinephrine for non-shockable OHCA was associated with improved 1-month survival (OR 1.67, 95%CI 1.51–1.84). In another ancillary analysis that focused on patients with prehospital epinephrine, all of the outcomes were better as the time from call to epinephrine administration was shorter, regardless of cardiac rhythm or bystander witness (online-only supplemental Table 4).
As an additional analysis, we investigated the association of the timing of epinephrine administration with 1-month survival and neurologically favorable survival, depending on the number of epinephrine doses (Table 4). Only when the time interval from call to epinephrine was up to 15 min, patients who received a single dose of epinephrine had a more favorable neurological outcome than those who did not receive epinephrine in shockable OHCA (OR 1.95, 95%CI 1.37–2.72). In addition, a single dose of epinephrine administered within 20 min in a shockable OHCA case and within 25 min in a non-shockable OHCA case was associated with increased 1-month survival.
Discussion
In this nationwide, population-based study of OHCA, prehospital epinephrine administration was associated with a decreased chance of neurological favorable survival, regardless of the initial cardiac rhythm. In addition, prehospital epinephrine administration was associated with a poor neurological outcome in all subgroups. The neurological outcome became worse as the number of epinephrine doses increased or the time to epinephrine increased. Patients had greater chance of favorable neurological outcome only when single-dose epinephrine was administered within 15 min of the emergency call in shockable OHCA.
To our knowledge, this is the first and largest cohort study to assess in detail the effect of prehospital epinephrine administration on the outcomes of OHCA after the 2010 CPR guideline update. Our findings were robust due to the population-based study design, the use of propensity score matching and regression modeling to control for selection bias and potential confounding, and the subgroup analyses. Therefore, although this was an observational study, our findings strongly suggest that prehospital epinephrine may be harmful in OHCA, with the exception of an early single dose of epinephrine in a shockable OHCA case.
Although epinephrine is known to increase ROSC, there are some concerns about its detrimental effect on survival and neurological outcome [3–6]. Epinephrine can contribute to ROSC through strong alpha-adrenergic actions that result in macrovascular coronary and cerebral perfusion. On the other hand, its beta-adrenergic actions may be involved in poorer survival and neurological outcomes. Inotropic and chronotropic effects may cause an imbalance between the oxygen supply and the demand from the myocardium, which may result in post-cardiac arrest myocardial dysfunction [18, 19]. In addition, epinephrine is also reported to impair microvascular perfusion, including cerebral microcirculation [20, 21]. The majority of our findings also showed positive effects on ROSC and negative effects on survival and neurological outcomes. In the subgroup analysis, while there was no subgroup in which neurological outcome improved due to epinephrine administration, in the unwitnessed, non-shockable OHCA and asystole subgroups, 1-month survival increased (online-only supplemental Tables 1 and 2). Yet for such subgroups where lifesaving would not be possible without the use of epinephrine, these results suggest the discomfiting possibility that epinephrine may lead to undue futile salvage. Considering that the mere increase in 1-month survival without a favorable neurological status means failure of cerebral resuscitation in spite of successful cardiopulmonary resuscitation, we might have to refrain from reckless epinephrine administration.
The optimal dose of epinephrine is not known, although increasing the cumulative dose of epinephrine may worsen survival and neurological outcomes [8, 10]. However, repeated doses signified the prolonged time needed for resuscitation. Moreover, the adverse effects of epinephrine are possibly stronger post-resuscitation. Therefore, we must ascertain when, during the course of cumulative administration, the harms begin to overweigh the benefits. On the other hand, the time to administration is also important. Indeed, some studies suggested the possibility that the earlier epinephrine is administered in cardiac arrest, particularly in non-shockable OHCA, the greater its effect [9, 22–24]. Therefore, we conducted ancillary analyses to probe the boundaries of timing and frequency that should be considered in epinephrine administration (online-only supplemental Figure, online-only supplemental Table 4, and Table 4). Compared with cases where epinephrine was not administered, only shockable OHCA cases in which epinephrine was administered within 15 min of the emergency call had an improved neurological outcome. In cases of shockable OHCA and non-shockable OHCA in which epinephrine was administered only once within 20 and 25 min, respectively, 1-month survival increased without any significant deterioration in neurological outcome. Contrary to the recommendations from the guidelines (1 mg epinephrine every 3 to 5 min), our study results suggest that epinephrine is effective only in an extremely limited number of situations in OHCA: that is to say that (1) repeated epinephrine administration may be harmful, (2) a delay in initial administration of epinephrine may be harmful even with a single dose, and (3) epinephrine may only lead to undo futile salvage without a favorable neurological outcome. Whether early single-dose epinephrine in shockable OHCA improves neurological outcome is inconclusive because the findings from the ancillary analyses were exploratory. Therefore, further studies that focused on these issues are needed.
Our study results also indicated that prehospital epinephrine administration delayed hospital arrival. Delayed hospital arrival may be fatal. Resuscitation practices have changed dramatically over the past several decades. Not only have there been increases in prehospital AED and bystander CPR implementation rates [25, 26], but also there have been striking advancements in in-hospital and post-resuscitation care (e.g., cardiovascular intervention, targeted temperature management, and extracorporeal life support) [27, 28]. A delay in in-hospital and post-resuscitation care may have a great impact on outcomes after OHCA [29].
Although this study, which focused on OHCA patients who were treated with recent CPR practices, has extreme importance, there could be selection bias and potential confounding in spite of propensity score matching and regression modeling. An RCT comparing epinephrine and a placebo for OHCA is ongoing and may provide further clarification (PARAMEDIC 2: ISRCTN73485024).
This study has several limitations. First, this is an observational study. Although we tried to control for selection bias and potential confounding by performing propensity score matching and regression modeling, the possibility of residual confounding remains. Therefore, the findings of this study might only indicate association and not causality. Second, the generalizability of our findings is uncertain. Although the All-Japan Utstein Registry data includes mostly people of Japanese ethnicity, the effect of epinephrine might differ in different ethnic groups. In addition, we excluded a small number of patients based on missing, incomplete, inconsistent, or unknown data. Although only 5.3 % of the total patients were excluded, that might also decrease the generalizability of our findings. Third, our study cohort included patients with DNR orders. These patients might distort the findings of our study. However, it is impossible to distinguish patients with DNR orders from those without DNR orders in this national registry. Further studies that collect data on DNR orders are needed. Fourth, we were unable to assess the quality of CPR. Although prehospital CPR should be provided in accordance to Japanese CPR guidelines, there might be variability among EMS personnel. In addition, information on the interruption of CPR during epinephrine administration was unavailable. Fifth, the All-Japan Utstein Registry data does not collect information on in-hospital/post-resuscitation care. Such care might have a critical impact on the outcomes, and therefore, it could be an unmeasured confound.
Conclusion
In conclusion, prehospital epinephrine administration was associated with a decreased chance of neurologically favorable survival in OHCA, although prehospital epinephrine might have positive effects only when early single-dose epinephrine is administered in shockable OHCA. In addition, neurological outcome became worse as the number of epinephrine doses increased or the time to epinephrine increased.
References
Link MS, Berkow LC, Kudenchuk PJ, Halperin HR, Hess EP, Moitra VK, Neumar RW, O'Neil BJ, Paxton JH, Silvers SM, White RD, Yannopoulos D, Donnino MW (2015) Part 7: adult advanced cardiovascular life support: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 132(18 Suppl 2):S444–S464
Soar J, Nolan JP, Böttiger BW, Perkins GD, Lott C, Carli P, Pellis T, Sandroni C, Skrifvars MB, Smith GB, Sunde K, Deakin CD, Adult advanced life support section Collaborators (2015) European Resuscitation Council guidelines for resuscitation 2015: section 3 adult advanced life support. Resuscitation 95:100–147
Olasveengen TM, Sunde K, Brunborg C, Thowsen J, Steen PA, Wik L (2009) Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trial. JAMA 302:2222–2229
Jacobs IG, Finn JC, Jelinek GA, Oxer HF, Thompson PL (2011) Effect of adrenaline on survival in out-of-hospital cardiac arrest: a randomised double-blind placebo-controlled trial. Resuscitation 82:1138–1143
Olasveengen TM, Wik L, Sunde K, Steen PA (2012) Outcome when adrenaline (epinephrine) was actually given vs. not given—post hoc analysis of a randomized clinical trial. Resuscitation 83:327–332
Hagihara A, Hasegawa M, Abe T, Nagata T, Wakata Y, Miyazaki S (2012) Prehospital epinephrine use and survival among patients with out-of-hospital cardiac arrest. JAMA 307:1161–1168
Nakahara S, Tomio J, Takahashi H, Ichikawa M, Nishida M, Morimura N, Sakamoto T (2013) Evaluation of pre-hospital administration of adrenaline (epinephrine) by emergency medical services for patients with out of hospital cardiac arrest in Japan: controlled propensity matched retrospective cohort study. BMJ 347:f6829
Dumas F, Bougouin W, Geri G, Lamhaut L, Bougle A, Daviaud F, Morichau-Beauchant T, Rosencher J, Marijon E, Carli P, Jouven X, Rea TD, Cariou A (2014) Is epinephrine during cardiac arrest associated with worse outcomes in resuscitated patients? J Am Coll Cardiol 64:2360–2367
Koscik C, Pinawin A, McGovern H, Allen D, Media DE, Ferguson T, Hopkins W, Sawyer KN, Boura J, Swor R (2013) Rapid epinephrine administration improves early outcomes in out-of-hospital cardiac arrest. Resuscitation 84:915–920
Arrich J, Sterz F, Herkner H, Testori C, Behringer W (2012) Total epinephrine dose during asystole and pulseless electrical activity cardiac arrests is associated with unfavourable functional outcome and increased in-hospital mortality. Resuscitation 83:333–337
Fukuda T, Yasunaga H, Horiguchi H, Ohe K, Fushimi K, Matsubara T, Yahagi N (2013) Health care costs related to out-of-hospital cardiopulmonary arrest in Japan. Resuscitation 84:964–969
Fukuda T, Matsubara T, Doi K, Fukuda-Ohashi N, Yahagi N (2014) Predictors of favorable and poor prognosis in unwitnessed out-of-hospital cardiac arrest with a non-shockable initial rhythm. Int J Cardiol 176:910–915
Fukuda T, Ohashi-Fukuda N, Matsubara T, Doi K, Kitsuta Y, Nakajima S, Yahagi N (2015) Trends in outcomes for out-of-hospital cardiac arrest by age in Japan: an observational study. Medicine (Baltimore) 94:e2049
Cummins RO, Chamberlain D, Hazinski MF, Nadkarni V, Kloeck W, Kramer E, Becker L, Robertson C, Koster R, Zaritsky A, Bossaert L, Ornato JP, Callanan V, Allen M, Steen P, Connolly B, Sanders A, Idris A, Cobbe S (1997) Recommended guidelines for reviewing, reporting, and conducting research on in-hospital resuscitation: the in-hospital ‘Utstein style’. Am Heart Assoc Circ 95:2213–2239
Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE, Bossaert L, Cassan P, Coovadia A, D'Este K, Finn J, Halperin H, Handley A, Herlitz J, Hickey R, Idris A, Kloeck W, Larkin GL, Mancini ME, Mason P, Mears G, Monsieurs K, Montgomery W, Morley P, Nichol G, Nolan J, Okada K, Perlman J, Shuster M, Steen PA, Sterz F, Tibballs J, Timerman S, Truitt T, Zideman D, International Liaison Committee on Resuscitation, American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation; Resuscitation Councils of Southern Africa, ILCOR Task Force on Cardiac Arrest and Cardiopulmonary Resuscitation Outcomes (2004) Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation 110:3385–3397
Jennett B, Bond M (1975) Assessment of outcome after severe brain damage. Lancet 1:480–484
Rosenbaum PR, Donald BR (1985) Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am Stat 39:33–38
Tang W, Weil MH, Sun S, Gazmuri RJ, Bisera J (1993) Progressive myocardial dysfunction after cardiac resuscitation. Crit Care Med 21:1046–1050
Angelos MG, Butke RL, Panchal AR, Torres CA, Blumberg A, Schneider JE, Aune SE (2008) Cardiovascular response to epinephrine varies with increasing duration of cardiac arrest. Resuscitation 77:101–110
Ristagno G, Tang W, Huang L, Fymat A, Chang YT, Sun S, Castillo C, Weil MH (2009) Epinephrine reduces cerebral perfusion during cardiopulmonary resuscitation. Crit Care Med 37:1408–1415
Fries M, Tang W, Chang YT, Wang J, Castillo C, Weil MH (2006) Microvascular blood flow during cardiopulmonary resuscitation is predictive of outcome. Resuscitation 71:248–253
Goto Y, Maeda T, Goto Y (2013) Effects of prehospital epinephrine during out-of-hospital cardiac arrest with initial non-shockable rhythm: an observational cohort study. Crit Care 17:R188
Donnino MW, Salciccioli JD, Howell MD, Cocchi MN, Giberson B, Berg K, Gautam S, Callaway C, American Heart Association’s Get With The Guidelines-Resuscitation Investigators (2014) Time to administration of epinephrine and outcome after in-hospital cardiac arrest with non-shockable rhythms: retrospective analysis of large in-hospital data registry. BMJ 348:g3028
Andersen LW, Berg KM, Saindon BZ, Massaro JM, Raymond TT, Berg RA, Nadkarni VM, Donnino MW, American Heart Association Get With the Guidelines–Resuscitation Investigators (2015) Time to epinephrine and survival after pediatric in-hospital cardiac arrest. JAMA 314:802–810
Iwami T, Kitamura T, Kiyohara K, Kawamura T (2015) Dissemination of chest compression-only cardiopulmonary resuscitation and survival after out-of-hospital cardiac arrest. Circulation 132:415–422
Blom MT, Beesems SG, Homma PC, Zijlstra JA, Hulleman M, van Hoeijen DA, Bardai A, Tijssen JG, Tan HL, Koster RW (2014) Improved survival after out-of-hospital cardiac arrest and use of automated external defibrillators. Circulation 130:1868–1875
SOS-KANTO 2012 Study Group (2015) Changes in treatments and outcomes among elderly patients with out-of-hospital cardiac arrest between 2002 and 2012: a post hoc analysis of the SOS-KANTO 2002 and 2012. Resuscitation 97:76–82
Tagami T, Matsui H, Fushimi K, Yasunaga H (2016) Changes in therapeutic hypothermia and coronary intervention provision and in-hospital mortality of patients with out-of-hospital cardiac arrest: a Nationwide database study. Crit Care Med 44:488–495
Anderson ML, Nichol G, Dai D, Chan PS, Thomas L, Al-Khatib SM, Berg RA, Bradley SM, Peterson ED, American Heart Association’s Get With the Guidelines-Resuscitation Investigators (2016) Association between hospital process composite performance and patient outcomes after In-hospital cardiac arrest care. JAMA Cardiol 1:37–45
Acknowledgments
This study was supported by the University of Tokyo. We thank all of the EMS personnel and participating physicians in Japan as well as the FDMA for their generous cooperation in establishing and maintaining the All-Japan Utstein Registry. The FDMA oversees/approves data queries and manuscript submissions. However, the author group is responsible for the conception of the project, all data analyses, and manuscript writing. TF, as the principal investigator, participated in the study concept and design; acquisition, analysis, or interpretation of data; drafting of the manuscript; and critical revision of the manuscript for important intellectual content. O-F N, MT, GM, KY, and YN participated in acquisition, analysis, or interpretation of data and critical revision of the manuscript for important intellectual content. TF performed statistical analysis. All authors approved the final version. TF had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was conducted in accordance with the amended Declaration of Helsinki. The institutional review board of the University of Tokyo approved the study with a waiver of informed consent because of the anonymous nature of the data (no. 10096).
Conflict of interest
The authors declare that they have no competing interests.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 58.3 kb)
Rights and permissions
About this article

Cite this article
Fukuda, T., Ohashi-Fukuda, N., Matsubara, T. et al. Effect of prehospital epinephrine on out-of-hospital cardiac arrest: a report from the national out-of-hospital cardiac arrest data registry in Japan, 2011–2012. Eur J Clin Pharmacol 72, 1255–1264 (2016). https://doi.org/10.1007/s00228-016-2093-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-016-2093-2