
Abstract
The potential toxicity of beryllium at low levels of exposure means that a biological and/or air monitoring strategy may be required to monitor the exposure of subjects. The main objective of the work presented in this manuscript was to develop and validate a sensitive and reproducible method for determining levels of beryllium in human urine and to establish reference values in workers and in non-occupationally exposed people. A chelate of beryllium acetylacetonate formed from beryllium(II) in human urine was pre-concentrated on a SPE C18 cartridge and eluted with methanol. After drying the eluate, the residue was solubilised in nitric acid and analysed by atomic absorption spectrometry and/or inductively coupled plasma mass spectrometry. The proposed method is 4 to 100 times more sensitive than other methods currently in routine use. The new method was validated with the concordance correlation coefficient test for beryllium concentrations ranging from 10 to 100 ng/L. Creatinine concentration, urine pH, interfering compounds and freeze–thaw cycles were found to have only slight effects on the performance of the method (less than 6 %). The effectiveness of the two analytical techniques was compared statistically with each other and to direct analysis techniques. Even with a detection limit of 0.6 ng/L (obtained with inductively coupled plasma mass spectrometry), the method is not sensitive enough to detect levels in non-occupationally exposed persons. The method performance does however appear to be suitable for monitoring worker exposure in some industrial settings and it could therefore be of use in biological monitoring strategies.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Beryllium (Be) is a steel-grey metal which exhibits extraordinary chemical and physical properties as strength (six times harder than steel) and lightness (three times lighter than aluminium) [1]. Because of these unique properties, Be has become an essential component in many industries, including aerospace, electronics, the nuclear industry, the automotive industry, telecommunications, computers, jewellery and ceramics [2, 3]. It has also been used in the dental laboratory as a component in dental amalgams and prostheses [4].
Beryllium and its compounds exhibit an extreme toxicity to human health, with lung as the main target organ. Cases of acute beryllium disease (ABD), an inflammation of the respiratory tract, were reported as early as the 1930s in beryllium extraction and processing industries. The implementation of new occupational air standards, notably a reduction of the US workplace threshold limit value from 2.0 to 0.05 μg m−3, has drastically reduced the prevalence of ABD. However, a chronic pathology, continues to occur today. The sensitisation of workers has been observed even at low levels (around 0.5 μg m−3) of exposure. The development of biomonitoring of exposed workers is therefore necessary for controlling low exposure and preventing onset of the disease.
Beryllium exposure occurs through ingestion and inhalation. In the general population and in some workers, urinary beryllium levels are usually reported as undetectable. The lack of new knowledge in the biological monitoring of Be is undoubtedly related to the absence of adequate analytical methods for determining Be in human urine at an appropriate level. The aim of this study is to validate a method for determining Be in human urine with a low quantification limit in order to be able to quantify beryllium in the urine of both exposed and non-exposed healthy persons [2, 3].
Among the different techniques used for the determination of urinary beryllium, the most sensitive and most commonly used are graphite furnace atomic absorption spectrometry (GF-AAS) [5, 6] and inductively coupled plasma mass spectrometry (ICP-MS) [7–10].
The use of a fluorimetric reagent, 10-hydroxybenzo[h]quinoline-7-sulfonate (HBQS) under alkaline conditions (pH~12) has also been proposed for Be analysis [11]. The interest of HBQS in both applications in the fields of industrial hygiene (measurement of Be in air) [12] and biomedical sciences [13] has been demonstrated. Fluorimetric methods with HBQS after extraction with ammonium bifluoride offer detection limits in the range of atomic spectroscopy methods [12].
Activated carbon [14], silica gel [15], salicylate chelating resin [16], anion exchange resin [17] and mixed micelle-mediated extraction [18] have been used to selectively separate and concentrate trace amounts of beryllium in natural waters. A particular advantage of these methods is that they allow metal ions to be determined at nanogram level in natural waters.
In this paper, we describe a method of solid phase extraction (SPE) coupled with spectrometry for the determination of ultratrace urinary beryllium. The procedure is based on the pre-concentration of chelated beryllium on a C18 silica cartridge, followed by either GF-AAS or ICP-MS determination of beryllium after elution.
Experimental method
Apparatus
A Varian AA280Z atomic absorption spectrophotometer, equipped with a Zeeman background corrector, was used for the atomic absorption measurement of beryllium at 234.9 nm with a slit width of 1.0 nm. A hollow cathode lamp of Be (photron) was operated at 5 mA. Uncoated graphite tube cuvettes were purchased from Schunk Kohlenstofftechnik (Germany).
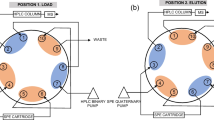
A Varian 820-MS ICP-MS with an external sample introduction assembly with Peltier-cooled spray chamber, glass concentric nebuliser, peristaltic pump mounted outside the torch box and SPS3 auto sampler was applied. A discrete dynode electron multiplier detector provides nine decades of dynamic range in an all-digital pulse design. The Varian 820-MS system also features a collision reaction interface (CRI) providing fast, flexible, interference-free analysis using simple collision and reaction gases.
A Radiometer PHM64 pH meter was used for pH measurements. SPE products were purchased from Interchim (REC18-360/6). Creatinine levels were determined in all urine samples using an automated alkaline picrate method on a Daytona (Randox, Ireland) analyser [19, 20].
Reagents and solutions
All chemicals used in the study were of analytical grade or higher. Nitric acid was used to prepare 2 % HNO3 (v/v) with ultrapure water. All single element stock solutions (1,000 mg/L) were delivered by SCP Science and certified for purity and concentration. From these stock solutions, a mixed working standard solution with a concentration of 10 mg/L for each element was prepared by adding 1 mL of each stock solution into a 100-mL measuring flask, adding 5 mL of purified HNO3 and diluting to 100 mL with ultrapure water (MilliQ, Millipore, Germany).
Beryllium standard solutions for ICP-MS calibration were prepared, at concentration levels of 2, 4, 8, 10, 30, 50 and 100 ng/L, by diluting a 10 g/L beryllium standard stock solution (140.061.041, SCP Science) with 2 % v/v HNO3. An internal standard solution containing 100 μg/L of Sc was prepared by diluting a 1,000 mg/L internal standard stock solution (140.051.211, SCP Science) with 2 % v/v HNO3. The internal standard was added to all samples and standard solutions.
Quality control materials (such as standard or certified reference materials) are commonly used in routine analytical laboratories to ensure the accuracy of the instrument and analytical procedure. In this work, three urine metal control materials were used [Seronorm Urine Metal Control (LOT 511545), Lyphocheck Urine Metal Control, Level 1 (LOT 69131) and Level 2 (LOT 69132), Bio-Rad Laboratories, Irvine, CA, USA].
External quality assurance was performed by participation in the following international comparison programmes and quality assessment schemes:
-
German External Quality Assessment Scheme (G-EQUAS) from the Institute and Out-Patient Clinic for Occupational, Social and Environmental Medicine at Friedrich-Alexander-University Erlangen-Nuremberg, Germany.
-
Quebec Multielement External Quality Assessment Scheme (QMEQAS) at the Canadian Institut National de Santé Publique du Québec.
Two hundred millilitres of Nash Reagent containing 30 g of ammonium acetate (99.99 %, Aldrich), 600 μL of acetic acid (99.99 %, Aldrich) and 24.0 mL of acetylacetone (99.99 %, Aldrich) (i.e. 2.0 M ammonium acetate buffer at pH 6.0 together with 12 % acetylacetone (v/v)) was prepared weekly.
Human urine samples
For the Be tests, a unique urine sample was obtained by collecting urine from four adults over a 24-h period. Samples were collected in pre-cleaned polyethylene bottles and were refrigerated at −20 °C while not in use. Samples for measuring urinary Be concentrations from occupationally exposed subjects were collected over 10 days for the purpose of a separate biological monitoring study not presented in this paper.
Direct analysis of Be in urine samples using ICP-MS
Direct analysis of beryllium in urine was conducted using a Varian 820-MS. The typical method parameters (including CRI settings) used for the urine analyses are listed in Table 1. The concentration of the internal standard was 50 μg/L Rh in all sample and calibration solutions. For beryllium determinations with the Varian 820-MS, the urine solutions were further diluted by a factor of 1:10 by adding 1 mL of the urine into a pre-cleaned tube containing 9 mL of 2 % v/v HNO3 and 0.01 % v/v Triton X-100. This diluted urine solution was used as the sample for the direct ICP-MS analysis. Beryllium calibration solutions were prepared in 2 % v/v HNO3 and 0.01 % v/v Triton X-100.
Direct analysis of Be in urine samples using GF-AAS
In order to decrease sample viscosity and to dispense the sample more evenly in the graphite tube, an aliquot containing 14 μL 2 % v/v HNO3, 2 μL of chemical modifier (2 g/L Mg(NO3)2 + 1 g/L La(NO3)3) and 20 μL of urine sample was introduced to a graphite tube and atomized according to a set temperature programme (Table 2). Peak areas in absorbance were used for quantitative analysis.
Analytical procedure for Be in urine
After addition of the Nash reagent (1 mL) and a small amount of HCl solution (300 μL, 0.2 % (v/v)) to unknown samples (10 mL) or appropriate amounts (0–40.0 ng) of Be(II) standard solutions, each solution had a final pH of around 5.5. After mixing, each solution was left to stand at room temperature for approximately 1 h. Sep-Pak® C18 cartridges (Waters Associates Co, USA) were preconditioned with 3 mL methanol and 3 mL distilled water. Cartridges were loaded with samples on vacuum manifold (pump flow rate 1 mL/min). During the optimization phase, the influence of a washing step with distilled water was assessed. Finally, the Be(acac)2 chelate in the cartridge was eluted with 4 × 1 mL of methanol, and the methanol was then evaporated under a stream of nitrogen at room temperature. After evaporation, 1 mL 2 % v/v HNO3 was introduced to the 4-mL tube (Supelco) for easy analysis by GF-AAS and/or ICP-MS.
Validation of the method
Detection limit, quantification limit, linearity limit, replicability, reproducibility, repeatability, accuracy and sensitivity were determined in order to validate the analytical method.
Detection limits correspond to three times the standard deviation of a sample at a concentration of five to seven times the estimated detection limit. The standard deviation is calculated from ten replicates of a sample at the correct concentration. The quantification limit is equal to ten times the standard deviation. According to the recommendation given by the International Union of Pure and Applied Chemistry (IUPAC) [21, 22], the limit of detection, expressed as the concentration cL or the quantity qL, is derived from the smallest measured XL that can be detected with reasonable certainty for a given analytical procedure.
The value of XL is given by the equation:
where Xbl and sbl are the mean and standard deviation of the blank measurements, respectively, and k is a numerical factor chosen according to the confidence level desired.
The IUPAC recommends a value of 3 for k, which gives a confidence level of about 98 %.
In ICP-MS, the Xbl is the mean cps of the blank measurements, and a typical ICP-MS calibration plot can be expressed using the following equation:
where XA is the cps measured at an analyte concentration of CA, and m is the sensitivity (i.e. the slope of the calibration plot). Hence, the value of XL in ICP-MS can also be given as:
From Eqs. (1) and (3), the concentration CL can be calculated using:
Both detection and quantification limits are dependent on the recovery. For a particular batch of analysis, the limits are equal to quotient of the theoretical limits (i.e. with 100 % of recovery) by the recovery. The linearity limit is the highest value of a concentration range where the correlation coefficient is equal to at least 0.995.
Fidelity consists of replicability, repeatability and reproducibility. The replicability at a given level is defined as the degree of concordance of individual results obtained from successive analyses of the same sample, tested in a single laboratory, by the same analyst, on the same equipment, with all analyses conducted on the same day.
The repeatability at a given level is the degree of concordance between individual results obtained from the same sample tested in the same laboratory, but where at least one of the following varies: analyst, equipment or day.
The reproducibility at a given level is the degree of concordance between individual results obtained from the same sample tested by different analysts in different laboratories, using different equipment. The analyses can be performed on the same or different days.
The accuracy at a given level is the degree of concordance between the value certified by a recognised organisation and the mean result achieved by applying the experimental procedure ten times (n = 10 replicates). The accuracy is measured at a given level of concentration in the area quantifiable practice of the method and is expressed by the relative error.
The sensitivity at a given concentration is the ratio of the measured variable to the corresponding value of the concentration of the element to be determined.
Comparison of the analytical methods
The reliabilities of the three most sensitive analytical techniques available (direct ICP-MS, GF-AAS after pre-concentration (C18-GF-AAS) and ICP-MS after pre-concentration (C18-ICP-MS)) were compared statistically using spiking experiments. Urine samples were spiked with beryllium concentrations ranging from 10 to 100 ng/L and the samples were analysed using each of the analytical methods.
The concordance correlation coefficient (CCC) [23] was then calculated for each method to evaluate reproducibility and the agreement between observed measurements and theoretical values based on both accuracy and precision measurements. The CCC combines measurements of precision and accuracy to determine how far observed measurements deviate from the line of perfect concordance (i.e. a 45° line on a square scatterplot). The CCC increases in value as a function of the proximity of the data’s reduced major axis to the line of perfect concordance (the accuracy of the data) and of the tightness of the data about its reduced major axis (the precision of the data).
Results and discussion
Optimization of acetylacetone concentration
Different concentrations of acetylacetone were tested in order to evaluate the efficiency of the concentration procedure of Be(II) as Be(acac)2 chelate retained on a SPE C18 cartridge. Two measurements were made for each concentration. The results (Fig. 1) indicate that the percentage recovered increases as a function of the proportion of acetylacetone in the Nash reagent. Liquids are immiscible at over 15 % acetylacetone. Because beryllium was quantitatively recovered (82 %) with 12 % acetylacetone, a fixed amount of acetylacetone (24 mL for 200 mL of Nash reagent) was selected.

Effect of acetylacetone concentration in the Nash reagent on recovery of Be. The beryllium concentration in urine was set at 200 ppt
The effect of “washing”
Loading of the sample mixture into the cartridge is normally followed by a “washing” phase in which retained proteins and/or interfering agents are eluted for analysis. An aqueous washing phase was chosen for this study. The influence of the wash step was studied at 12 different urinary Be concentrations, ranging from 5 to 100 ng/L. The maximum recovery difference was 7.2 % for a beryllium concentration of 100 ng/L and the mean difference for all concentrations was 2.5 %. As the washing step was shown to have no significant effect on recovery, it was not included in the method.
Linearity
Following the proposed method, a calibration curve was derived from ten Be standard analyses per day over a 10-day period. The mean calibration curve equation was 0.00079x + 0.00222, with a linear range of 2–500 ng/L and a correlation coefficient of 0.999. The recovery percentage fluctuated slightly around 80 % (Fig. 2).

Effect of Be concentration on recovery. Observations at 20, 30, 40, 60, 80, 90 and 200 μg/L are duplicate, at 500 μg/L is uniplicate and others are n > 10
The effect of creatinine
Experiments were performed to determine whether elevated levels of excreted creatinine influence the determination of Be (Fig. 3). A stock solution of 500 ppt beryllium was split into 13 samples in which the concentration of creatinine was adjusted between 0.15 and 3.0 g/L. Be recovery ranged from 75 to 89 %. For a so-called valid creatinine concentration (0.5 to 3.0 g/L), the recovery ranged from 78 to 83 %, less than the analytical uncertainty. Creatinine therefore appears to have a slight effect on the detection of beryllium in urine samples. Creatinine may compete somewhat with beryllium complex on C18 cartridge reactive sites.

Effect of creatinine concentration on Be recovery
Interference elution
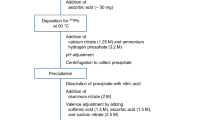
Interference elution aims to selectively remove undesired compounds from the sorbent without eluting analytes. Aluminium, zirconium and thorium can be complexed with acetylacetone in the same way as beryllium [24, 25]. First, aluminium acetylacetonate (Al(acac)3), zirconium acetylacetonate (Zr(acac)4·10H2O) and thorium acetylacetonate (Th(acac)4) were prepared by treatment of acetylacetone with hydrous aluminium oxide [25], zirconyl nitrate [26] and thorium nitrate [27, 28], respectively. As Al, Zr and Th can form acetylacetonate complexes, and can therefore exhibit similar behaviour to Be on the C18 column, it was necessary to examine possible interference of these ions on the Be dosage. The effect of these foreign cations was examined at different concentrations ([Al] = [Zr] = [Th] = 1, 10, 100 and 1,000 μg/L) when 1 ppb of Be was determined in urine samples. Beryllium recoveries were 86 % for interferent concentrations of 1 and 10 μg/L, and 84 and 80 % for interferent concentrations of 100 and 1,000 μg/L, respectively. As was the case for creatinine, suspected interferences of aluminium, zirconium and thorium are only slight. Trace amounts of Be could be recovered quantitatively and selectively using our proposed procedure even with simultaneously high concentrations of Al, Zr and Th.
Urine pH effect on recovery percentage
pH control is usually considered to be very important in ensuring the development of a robust method. Due to the presence of free silanol groups in non-polar sorbents, a combination of non-polar and cation exchange retention mechanisms is often the norm when extracting from aqueous samples. The secondary silanol interactions can also be valuable in providing an extra retention mechanism. pH control of the sample is essential to avoid problems caused by variable matrix effects when utilising secondary silanol interactions. The analytical protocol proposed here includes the addition of ammonium acetate to buffer the sample. In order to check the efficiency of the protocol and the influence of pH on recovery, different urine pH levels were tested (Fig. 4). A small amount of hydrochloric acid solution and sodium hydroxide was added to urine samples to obtain pH levels ranging from 4 to 8. Recovery was shown to be greater (>90 %) at acidic pH compared to basic pH (<90 %). Thus, pH appears to have an influence on the retention capacity of the cartridge in the protocol conditions.

Effect of pH on recovery of Be in urine. The beryllium concentration in urine was set to 100 ppt
The protocol involves a buffer solution at pH 5.5. Urine pH is usually between 4.0 and 6.0. In this range, recoveries are shown to be between 88 and 92 %, which are acceptable according to the literature [29, 30].
Effect of freezing on Be stability in urine and extractant
The stability of Be in urine and the effects of freeze–thaw cycle was assessed in two experiments. Firstly, flasks (10 mL) of urine were frozen at −20 °C together. After 84 days, beryllium was still quantitatively measurable (Fig. 5). The use of long-term frozen storage without chemical additives is the most prudent option for beryllium analysis. Refrigerating or freezing of urine samples has already been advised for the storage and ICP-MS analysis of many trace elements [9].

Stability of Be in urine. The concentration of beryllium in urine samples is expressed as the mean ± standard deviation. Urine samples were spiked with 500 ppt of beryllium
Secondly, the stability of the analyte was verified after going through successive freeze–thaw cycles. Twelve flasks (10 mL) of stock solution of Be in urine (1 μg/L) were stored together at −20 °C. Each time a flask was removed for analysis, all flasks were thawed. The last flask which had undergone ten freeze–thaw cycles during long-term frozen storage (253 days) exhibited a Be recovery percentage after extraction of 91.7 %, which is similar to the extract yield observed for freshly collected urines. Freezing can therefore be concluded to have no significant effect on beryllium stability in urine samples.
A stability check on the extractant was also conducted. After 117 days, the percentage of Be recovered after extraction was 97.0. Considering the analytical errors, we conclude that freezing has no effect on beryllium stability in the extractant solution.
Performance of the method
After optimisation of the ability of the cartridge to concentrate beryllium in urine, two analytical techniques were chosen for either direct analysis of the urine or analysis of diluted nitric acid from the concentration procedure. Table 3 presents the detection limits, quantification limits, linearity limits, replicability, repeatability, reproducibility, accuracy and sensitivity of the following: (1) direct analysis of Be in urine by ICP-MS, (2) direct analysis of Be in urine by GF-AAS, (3) analysis of Be after SPE by ICP-MS and (4) analysis of Be after SPE by GF-AAS. The detection limit of the GF-AAS method was 30 ng/L, whereas the corresponding value for ICP-MS is about 1 order of magnitude lower (Table 3). This clearly demonstrates the superiority of ICP-MS compared to GF-AAS for determination of occupational or environmental beryllium levels in urine. The ability of the C18 cartridge to concentrate beryllium allows us to decrease the quantification limits by a factor of ten (from 101 to 12 ng/L for GF-AAS and from 20 to 2.5 ng/L for ICP-MS). Replicability, repeatability, reproducibility, accuracy and sensitivity were determined with diluted Lyphocheck reference materials at two beryllium concentrations after completing the concentration procedure. The overall Be recovery was calculated to be 80.6 %. The accuracy was also assessed with target values obtained in the frame of two international programmes of inter-laboratory comparison for the external quality control (QMEQAS and G-EQUAS). The laboratory successfully participated in those two international inter-laboratory comparison programmes. Relative errors (RE%) were determined and plotted against target values (Fig. 6). For all observations but one, the results meet our criteria of acceptance (RE% < 15 %) [30]

Relative error on beryllium determination plotted against targeted values (international programmes of inter-laboratory comparison)
Concordance of the analytical techniques
Beryllium concentrations in spiked urine samples were determined by the three most sensitive analytical techniques available: ICP-MS (direct ICP-MS), C18-GF-AAS and C18-ICP-MS.
Concordance correlation coefficients were calculated to characterise the agreement between observed measurements and the theoretical values. The calculated CCC are 0.97, 0.97 and 0.99 for direct ICP-MS, C18-GF-AAS and C18-ICP-MS, respectively. In light of these results, we conclude that the three analytical methods are all effective for estimating urinary beryllium. The C18-ICP-MS protocol, which yields a better quantification limit and CCC index, is the preferred method of the three.
Application of C18-ICP-MS methods for biological monitoring
The technique was applied to two groups of urine obtained from workers employed at a primary aluminium production site (n = 15) and at an opto-electronics industry site (n = 23). At each site, workers who were not involved in processes involving beryllium exposure were used as controls. Based on air measurements, the sites were defined as high- and low-level beryllium exposure, respectively (data not shown). The quantification limit of the technique was 2.6 ng/L.
At the high-level exposure site, 657 urine samples were collected from workers. Of the samples, 89.6 % were quantified. From the low-level exposure site, none of the 1,111 samples could be quantified; 622 urine samples were below the detection limit and 489 samples were between the detection and quantification limits. All of the control subjects, from both sites, were found to have urinary Be levels below the detection limit (<0.6 ng/L). With a detection limit of 0.6 ng/L, the method is therefore not sensitive enough to detect levels in non-occupationally exposed people.
Compared to previous studies (Table 4) that reported means and 90th percentile of urinary beryllium for non-occupationally exposed populations, the method should be appropriate for environmental exposure. Indeed, our method presents a quantification limit which is the lowest of the reviewed studies.
In previous studies, the mean Be concentrations reported were generally close to [32], or even below [7, 8, 10, 34, 36, 38–40], the limit of quantification. As stated by Apostoli and Schaller [7], the detection limits in numerous studies are probably inadequate for estimation of environmental and occupational exposure. Moreover, Apostolli and Schaller estimate that the normal reference values proposed in the literature are too high. Our results, obtained from control subjects in the two industrial sites investigated, confirm these observations. The “normal reference value” in non-occupationally exposed populations is therefore assumed to be lower than the detection limit of 0.6 ng L−1.
The protocol could be slightly improved by increasing the volume of urine passing through the column and/or decreasing the extractant volume. It might also be possible to reduce the quantification limit by performing multiple injections in the GF-AAS graphite furnace. Higher performances could be achieved with low-temperature electrothermal vaporisation-ICP-MS, using benzoylacetone as both extractant and chemical modifier [42]. This method demands a substantive investment and highly skilled users.
Conclusions
The aim of this study was to develop and validate a method for determining Be in human urine. The proposed method provides high reproducibility and a limit of detection that is lower than that previously proposed for urine samples. It allows analysis and detection of beryllium in human urine samples down to 2 and 0.6 ng/L, respectively.
The proposed method provides rapid and simple determination of ultratrace amounts of beryllium in human urine samples and is appropriate for the biomonitoring of occupationally exposed people in the beryllium-using industry.
Improvements in the technique could allow the level of detection required for environmental biomonitoring to be reached.
Abbreviations
- ABD:
-
Acute beryllium disease
- acac:
-
Acetylacetonate
- ACGIH-TLV-TWA:
-
American Conference of Governmental Industrial Hygienists—Threshold Limit Value—Time Weighted Average
- CCC:
-
Concordance correlation coefficient
- CPS:
-
Counts per second
- CRI:
-
Collision reaction interface
- GF-AAS:
-
Graphite furnace atomic absorption spectroscopy
- ICP-MS:
-
Inductively coupled plasma mass spectrometry
- SPE:
-
Solid phase extraction
References
Taylor TP, Sauer NN (2002) Beryllium colorimetric detection for high speed monitoring of laboratory environments. J Hazard Mater 93(3):271–283
Bruce RM, Odin M (2001) Concise international chemical assessment document 32: beryllium and beryllium compounds. United Nations Environment Programme, International Labour Organization, World Health Organization, Geneva
Sharma P, Johri S, Shukla S (2000) Beryllium-induced toxicity and its prevention by treatment with chelating agents. J Appl Toxicol 20:313–318
Kotloff RM, Richman PS, Greenacre JK, Rossman MD (1993) Chronic beryllium disease in a dental laboratory technician. Am Rev Respir Dis 147:205–207
Thorat DD, Bhat PN, Mahadevan TN, Marayan S, Subramanian G (1995) Determination of beryllium in urine by graphite furnace atomic absorption spectrophotometry. Anal Lett 28(11):1947–1958
Wang HC, Peng HW, Kuo MS (2001) Determination of beryllium and selenium in human urine and of selenium in human serum by graphite furnace atomic absorption spectrophotometry. Anal Sci 17:527–532
Apostoli P, Schaller KH (2001) Urinary beryllium—a suitable tool for assessing occupational and environmental beryllium exposure? Int Arch Occup Environ Heal 74:162–166
Heitland P, Köster HD (2004) Fast, simple and reliable routine determination of 23 elements in urine by ICP-MS. J Anal At Spectrosc 19:1552–1558
Bornhorst JA, Hunt JW, Urry FM, McMillin GA (2005) Comparison of sample preservation methods for clinical trace element analysis by inductively coupled plasma mass spectrometry. Am J Clin Pathol 123:578–583
Morton J, Leese E, Cotton R, Warren N, Cocker J (2011) Beryllium in urine by ICP-MS: a comparison of low level exposed workers and unexposed persons. Int Arch Occup Environ Heal 84:697–704
Matsumiya H (2001) A novel fluorescence reagent, 10-hydroxybenzo[h]quinoline-7-sulfonate, for selective determination of beryllium(II) ion at pg cm(−3) levels. Analyst 126(11):2082–2086
Ashley K (2007) Ultra-trace determination of beryllium in occupational hygiene samples by ammonium bifluoride extraction and fluorescence detection using hydroxybenzoquinoline sulfonate. Anal Chim Acta 584:281–286
Zheng Y (2011) Analysis of beryllium to biomolecule binding using a metal specific fluorescent probe and competitive assay. Talanta 85(1):638–643
Okutani T, Tsuruta Y, Sakuragawa A (1993) Determination of a trace amount of beryllium in water samples by graphite furnace atomic absorption spectrometry after preconcentration and separation as a beryllium–acetylacetonate complex on activated carbon. Anal Chem 65:1273–1276
Szczepaniak W, Szymanski A (1996) Sorption and preconcentration of trace amounts of beryllium from natural waters on silica gel with immobilized morin prior to its determination by ETA-AAS method. Chem Anal 41:193–199
Kubova J, Nevoral V, Stresko V, Fresenius Z (1994) Determination of beryllium trace contents in mineral waters after preconcentration on a chelating ion-exchanger. J Anal Chem 348:287–290
Afkhami A, Madrakian T, Assl AA, Sehhat AA (2001) Spectrophotometric determination of beryllium in water samples after micelle-mediated extraction preconcentration. Anal Chim Acta 437:17–22
Beiraghi A (2007) Cloud-point formation based on mixed micelles for the extraction, preconcentration and spectrophotometric determination of trace amounts of beryllium in water samples. Anal Sci 23:527–531
Jaffe M (1886) Ueber den Niederschlag welchen Pikrinsäure in normalen Harn erzeugt and über eine neue Reaction des Kreatinins. Z Physiol Chem 10:391–400
Murray RL (1984) Creatinine. In: Kaplan LA, Pesce AJ (eds) Clinical chemistry: theory, analysis and correlation. Mosby, St. Louis, pp 1247–1253
Inczedy J, Lengyel T, Ure AM (1998) Compendium of analytical nomenclature (definitive rules 1997), IUPAC chemical nomenclature series, 3rd edn. Blackwell, Oxford
Gonzalez AG, Herrador MA (2007) A practical guide to analytical method validation, including measurement uncertainty and accuracy profiles. Trends Anal Chem 26:227–238
Lin LI-K (1989) A concordance coefficient to evaluate reproducibility. Biometrics 45(1):255–268
Conard Fernelius W (1946) Inorganic syntheses, vol 2. McGraw Hill, New York
Combes (1887) Comptes rendus hebdomadaires des séances de l’Académie des sciences, 106: 869–871. http://www.biodiversitylibrary.org/item/26775#page/876/mode/1up Accessed 11 Mar 2013
Biltz W, Clinch JA (1904) Notizen über acetylacetone. Z Anorg Chem 40:218–224
Urbain G (1896) Contribution à l’étude du thorium. Bull Soc Chim 3(15):338–347
Urbain G (1900) Recherche sur la séparation des terres rares. Ann Chim Phys 7(19):223–232
Organisation for Economic Co-operation and Development (2007) Guidance document on pesticide residue analytical methods. OECD Paris (France)
Levine KE, Tudan C, Grohse PM, Weber FX, Levine MA, Kim YS (2011) Aspects of bioanalytical method validation for the quantitative determination of trace elements. Bioanalysis 3(15):1699–1712
Grewal DS, Kern FX (1977) A simple and rapid determination of small amounts of beryllium in urine by flameless atomic absorption. At Absorpt Newsl 16:131–132
Minoia C, Sabbioni E, Apostoli P, Pietra R, Poxxoil L, Gallorini M, Nicolaou G, Alessio L, Capodaglio E (1990) Trace element reference values in tissues from inhabitants of the European community I. A study of 46 elements in urine, blood and serum of Italian subjects. Sci Total Environ 95:89–105
Apostoli P, Minoia C, Gilberti ME (1992) Application of Zeeman graphite furnace atomic absorption spectrometry in chemical laboratory and toxicology. Pergamon, London, pp 495–516
Paschal DC, Ting BG, Morrow JC, Pirkel JL, Jackson RJ, Sampson EJ, Miller DT, Caldwell KL (1998) Trace metals in urine of United States residents: reference range concentrations. Environ Res Sect A 76:53–59
Wegner R, Heinrich-Ramm R, Nowak D, Olma K, Poschadel B, Szadkowski D (2000) Lung function, biological monitoring, and biological effect monitoring of gemstone cutters exposed to beryls. Occup Environ Med 57:133–139
Komaromy-Hiller G, Ash KO, Costa R, Howerton K (2000) Comparison of representative ranges based on US. Patient population and literature reference intervals for urinary trace elements. Clin Chim Acta 296:71–90
Horng CJ, Horng PH, Lin SC, Tsai JL, Lin SR, Tzeng CC (2002) Determination of urinary beryllium, arsenic, and selenium in steel production workers. Biol Trace Elem Res 88:235–246
Caldwell KL, Hartel J, Jarret J, Jones RL (2005) Inductively coupled plasma mass spectrometry to measure multiple toxic elements in urine in NHANES 1999–2000. At Spectrosc 26:1–7
Heitland P, Köster HD (2006) Biomonitoring of 30 trace elements in urine of children and adults by ICP-MS. Clin Chem Acta 365:310–318
Batista BL, Rodrigues JL, Tormen L, Curtius AD, Barbosa F Jr (2009) Reference concentrations for trace elements in urine for the Brazilian population based on q-ICP-MS with a simple dilute and shoot procedure. J Braz Chem Soc 20(8):1406–1413
DFG (2012) List of MAK and BAT values. http://onlinelibrary.wiley.com/book/10.1002/3527600418/topics. Accessed 11 Mar 2013
Xia L, Hu B, Jiang Z, Wu Y, Liang Y (2004) Single-drop microextraction combined with low-temperature electrothermal vaporization ICPMS for the determination of trace Be, Co, Pd, and Cd in biological samples. Anal Chem 76:2910–2915
Acknowledgments
The authors thank the National Institute for Research and Safety and especially the Laboratory for biological monitoring of inorganic exposure. We particularly acknowledge the efforts of Alice Williams and Samuel Müller.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Devoy, J., Melczer, M., Antoine, G. et al. Validation of a standardised method for determining beryllium in human urine at nanogram level. Anal Bioanal Chem 405, 8327–8336 (2013). https://doi.org/10.1007/s00216-013-7220-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-013-7220-7