
Abstract
We investigated the elimination routes for the 200 drugs that are sold most often by prescription count in the United States. The majority (78%) of the hepatically cleared drugs were found to be subject to oxidative metabolism via cytochromes P450 of the families 1, 2 and 3, with major contributions from CYP3A4/5 (37% of drugs) followed by CYP2C9 (17%), CYP2D6 (15%), CYP2C19 (10%), CYP1A2 (9%), CYP2C8 (6%), and CYP2B6 (4%). Clinically well-established polymorphic CYPs (i.e., CYP2C9, CYP2C19, and CYP2D6) were involved in the metabolism of approximately half of those drugs, including (in particular) NSAIDs metabolized mainly by CYP2C9, proton-pump inhibitors metabolized by CYP2C19, and beta blockers and several antipsychotics and antidepressants metabolized by CYP2D6. In this review, we provide an up-to-date summary of the functional polymorphisms and aspects of the functional genomics of the major human drug-metabolizing cytochrome P450s, as well as their clinical significance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The human genome comprises 57 cytochrome P450 (CYP) genes and about the same number of pseudogenes, which are grouped according to their sequence similarity into 18 families and 44 subfamilies (http://drnelson.utmem.edu/human.P450.table.html). Isozymes of families CYP1, CYP2 and CYP3 are collectively responsible for most phase I biotransformations of drugs and other xenobiotics in human liver [1, 2]. In contrast to CYPs of families CYP4 to CYP51, which are involved in endogenous metabolic pathways of steroids, fatty acids, prostaglandins, etc., the CYP1, 2 and 3 isozymes have broad and overlapping substrate specificities which usually provide for a robust elimination of lipophilic xenobiotics. Nevertheless, the extremely variable expressions and functions of these isozymes, typically exceeding 100-fold in a large population sample, lead to unforeseen drug responses, including over-reaction, toxicity, or lack of response in a considerable fraction of treated patients [3–5].
The major sources of interindividual and intraindividual variability in CYP activity are environmental influences, including inhibition or induction by concomitant medications (drug–drug interactions), biological factors including sex and physiological determinants, such as hormonal status, disease, and circadian rhythms, and genetic polymorphisms in cytochrome P450 genes and their regulators. There are large differences between the individual CYP isoforms regarding their susceptibility to these mechanisms. CYP1 family enzymes are commonly inducible by polycyclic aromatic hydrocarbons through the Ah-receptor/ARNT pathway, and those of families 2 and 3 are generally inducible, but to various extents, by a diverse class of structurally unrelated xenobiotics which are usually ligands of the orphan nuclear receptors pregnane X receptor (PXR) and constitutively active receptor (CAR) [6]. Sex differences in CYP expression are a controversial but intensely debated topic, and some CYPs, in particular CYP3A4, show significant differences in humans [7]. Circadian rhythms can have a strong influence on the cytochrome P450 systems of laboratory animals, and but their relevance to humans is not well known [8]. The impact of disease has been particularly well investigated in the context of inflammation, which generally leads to transcriptional repression that affects some isoforms more than others [9].
Genetic polymorphisms, although present in practically all human genes, only affect some CYP isoforms to a functionally relevant extent. Genetic variability particularly affects CYP2D6, which is barely influenced by inducing agents and other factors. On the other side of the spectrum are CYP1A2 and CYP3A4, with polymorphisms that do not generally penetrate to the phenotype level. CYP isoforms that are both inducible and significantly polymorphic include CYPs of the CYP2C and 2B subfamily. However, of the many hundreds of SNPs and other sequence variations reported to date, most are not functionally relevant, i.e., they do not cause marked changes in expression, substrate selectivity or enzymatic activity (CYP allele nomenclature homepage at http://www.cypalleles.ki.se). The focus of this article is on providing an update on the functionally relevant polymorphisms of the human drug-metabolizing P450 forms and their role in the metabolism of the most often prescribed drugs.
Biotransformation of the 200 most widely used drugs
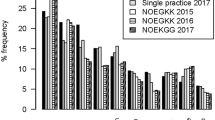
The routes of elimination for the 200 drugs most often prescribed (“top 200”) in the United States according to the RxList data listed in April 2008 (http://www.rxlist.com) were investigated. Among the top 200 drugs, the vast majority were found to be subject to hepatic elimination by either metabolism or excretion into bile, the latter contributing to a minor proportion of hepatic processes. Approximately 25% of the drugs are excreted unchanged into the urine via the kidneys, and no detailed information about the exact elimination pathway was available in the literature for 5% of them. Metabolism via CYP-mediated reactions represented the absolute majority of hepatic biotransformation processes (Table 1). Members of the CYP3A family contributed to the metabolism of 37% of the drugs, followed by CYP2C9 (17%), CYP2D6 (15%), CYP2C19 (10%), CYP1A2 (9%), and CYP2C8 (6%). CYP2B6 and other CYP isoforms (CYP2A6 and CYP2E1) participated in the metabolism of 4% and 2% of the drugs, respectively. An overview of these findings is given in Fig. 1. Table 2 summarizes the general features of these CYP enzymes. The most clinically well-established CYP polymorphisms of CYP2C9, CYP2C19, and CYP2D6 are involved in approximately half of these top 200 drugs, since many of the drugs used in high-prevalence diseases and conditions in the Western world are known to be metabolized by these CYPs. In particular, these include NSAIDs metabolized mainly by CYP2C9, proton-pump inhibitors metabolized by CYP2C19, and beta blockers and several antipsychotics and antidepressants metabolized by CYP2D6.

The routes of elimination for the 200 drugs sold in the greatest quantities top 200 drugs by prescription in the United States according to the RxList data listed in April 2008 (http://www.rxlist.com). Adapted from [247]
Functional genomics of human drug metabolizing cytochromes P450
We limited this part to the P450s that are reported as the major forms involved in the metabolism of at least one of the top 200 drugs. These are CYPs 1A2, 2B6, 2C8, 2C9, 2C19, 2D6, and 3A4/5. We furthermore aimed to focus our attention on the more common polymorphisms, i.e., those that occur with frequencies of >5% in at least one population. Nevertheless, rare alleles with functional impacts and other important drug substrates are mentioned when appropriate. We generally favored newer literature. For older studies, the reader is referred to specialized reviews or to the references given in the newer papers. Although genetic polymorphisms exist for CYP2A6, this isozyme was not included, because no major clinical drug substrate has been identified. However, it is known to play a major role in the C-oxidation of nicotine, and its expression and function are influenced by numerous genetic polymorphisms. Readers interested in CYP2A6 are referred to a recent review article [2, 110]. Similarly, CYP2E1 is significantly expressed in human liver and plays a major role in hepatotoxicity by metabolically activating a large number of toxicants and carcinogens [111], but due to the absence of clinically used drug substrates and the lack of predictive polymorphisms it was also omitted from this review.
CYP1A2
The CYP1 family genes are located on chromosome 15 and they encode the three P450 functional enzymes CYP1A1, CYP1A2, and CYP1B1. Their expression is coordinately regulated at the transcriptional level involving the aryl hydrocarbon receptor (AhR) pathway. Only CYP1A2 is expressed predominantly in liver, where it contributes on average ~10% of the total microsomal P450 pool. The substrate specificities of the CYP1 enzymes include many polycyclic aromatic hydrocarbons, with CYP1A2 showing a preference for N-hydroxylation of aromatic amines and heterocyclic compounds. Endogenous substrates are also known, e.g., prostaglandins, estrogens and retinoic acid. Only CYP1A2 metabolizes a significant number of the top 200 and other important drugs, including caffeine and theophylline, antipsychotics (olanzapine, clozapine), antidepressants (duloxetine), and others (Tables 1 and 2).
Genetic polymorphisms have been found in all human CYP1 genes, and earlier work mainly concentrated on their associations with various forms of cancer, because many of their substrates occur in industrial combustion products, cigarette smoke and charred food, and are carcinogenic or are at least converted into carcinogens. There is a long history of investigations into genetic influences on CYP1A2 variability [112]. By studying a large sample of mono- and dizygotic twins selected to exclude the influence of smoking, oral contraceptives and gender, a strong overall heritability of 0.72 was found for the CYP1A2-related caffeine metabolic ratio, supporting the expectation of a strong genetic contribution [113]. Indeed, numerous SNPs in coding and noncoding regions exist in the CYP1A2 gene in various haplotypes, but only two common SNPs are currently considered to be of potential predictive value. These are a 5′-upstream variant -3860G>A (CYP1A2*1C) and an intron 1 polymorphism -163C>A (CYP1A2*1F) located downstream of the untranslated first exon. The CYP1A2*1C allele has been associated with decreased caffeine 3-demethylation in Japanese smokers [114], and the CYP1A2*1F allele was correlated to increased activity in German [115] and Swedish [116] smokers, indicating the an opposite influence of these SNPs that probably modulate on CYP1A2 inducibility. Consistent with these findings, the combined genotype CYP1A2*1C/*1F was shown to be uninduced by omeprazole [117]. Contradictory findings were, however, reported for caffeine metabolism in nonsmoking breast cancer patients [118], and studies with other substrates have not been able to reproduce these findings for clozapine [119], haloperidol [120], and trazodone [121]. As amino acid promoter variations are unlikely to contribute substrate-dependent effects, it may be more likely that ethnically diverse haplotype patterns contribute to these discrepancies.
For some rare variants, a proven impact on activity has also been shown. For example, one lack of function mutation is the R431W substitution (CYP1A2*6), which is located in the “meander” peptide region critical to the maintenance of protein tertiary structure [122]. However, they are of limited practical use for genetic testing due to their rare occurrence. Newly discovered SNPs of CYP1A2 have not, so far, changed the overall picture. In Chinese subjects phenotyped with caffeine, a common haplotype containing the novel SNP -3113G>A had significantly lower metabolic activity, but it remained unclear as to whether this SNP, which is located in a proposed regulatory element, or other SNPs found on the same haplotype are responsible for the observed functional difference [123]. In a recent study, the human CYP1A1-CYP1A2 locus was resequenced in five major phenotyped ethnicities, revealing a total of 85 SNPs, 57 of which occurred more than once [124]. Attempts to relate the most common of these SNPs to phenotype in genotyped volunteers were disappointing, and it was concluded that an SNP or haplotype in the CYP1A2 gene that has a clear predictive value is yet to be identified. In conclusion, it is still possible that undiscovered common SNPs (probably in introns or in the 5′- or 3′-parts of the gene) and/or unrecognized haplotypes exist which strongly affect the CYP1A2 phenotype. The strong genetic component may, however, also be explained by genetic variations in other genes that contribute to the regulation of CYP1A2 expression, in particular the Ah receptor pathway. Although AhR polymorphisms have been reported [125], systematic investigations are lacking.
CYP2B6
The CYP2B6 gene together with the expressed pseudogene CYP2B7 is located within a 350-kb CYP2ABFGST gene cluster on chromosome 19 that contains genes and pseudogenes of the CYP2A, 2B, 2F, 2G, 2S and 2T subfamilies [126]. Studies in human liver microsomes suggest that the average CYP2B6 content in human liver is about 3–6% of the total microsomal P450 pool, and the between-individual variability in protein levels is approximately 100-fold [127]. Like the rodent phenobarbital-inducible CYP2B genes, human CYP2B6 is strongly inducible by numerous drugs and chemicals, including rifampin, barbiturates, cyclophosphamide, artemisinin, carbamazepine, efavirenz and nevirapine, and metamizole [128]. Clinically important drug substrates include the antidepressant and smoking cessation agent bupropion, the synthetic opioid methadone, as well as the cytostatic cyclophosphamide, the HIV drugs efavirenz and nevirapine, the antimalarial artemisinin, and the anesthetics propofol and ketamine [129].
Recent work from our group and from others has shown that CYP2B6 belongs to the most polymorphic CYP genes in humans, with over 100 documented DNA variations, including numerous nonsynonymous mutations as well as silent, promoter and intronic changes, with many of them showing extensive linkage disequilibrium, giving rise to distinct haplotypes [130]. The most common variant allele, CYP2B6*6, occurs with frequencies of between 15 and 60% across different populations and changes two amino acids (Q172H, K262R, Table 3) which are associated with an up to 75% decrease in hepatic protein expression [131, 132]. The mechanism of deficient expression of this variant has been shown to be caused by the c.516G>T [Q172H] polymorphism [127]. Although this amino acid change in exon 4 may also affect substrate specificity or turnover, it primarily prevents the correct splicing of the CYP2B6 pre-mRNA, thus leading to a shorter mature mRNA that lacks exons 4–6 and codes for a deficient enzyme. Whereas this SNP rarely occurs by itself (allele *9), the K262R variant also occurs as an own allele *4 (Table 3). Another functionally deficient allele that should be included if black subjects are investigated is CYP2B6*18, a nonsynonymous allele that did not form a functional protein in transfected mammalian cells and may thus be a null allele [133]. It is absent in Caucasian populations, but consistently found among black subjects [134].
HIV-infected patients homozygous for CYP2B6*6 have strongly elevated plasma levels of efavirenz, and in some studies presented with increased risk for neurotoxicity (summarized in [135]). Determinations of less frequent loss of function alleles, including *11 and *18 and the newly identified *27, *28, and *29, improved the prediction of high efavirenz plasma levels [136, 137]). In a recent study with Japanese HIV patients, it was shown for the first time that prospective, genotype-based dose adjustment successfully reduced the therapeutic dose of efavirenz and succeeded in improving CNS-related side effects [138]. The CYP2B6 genotype also affects plasma levels of nevirapine, another NNRTI drug [139]. However, some other substrates of CYP2B6 behave differently. A single-dose pharmacokinetic study in 121 healthy male volunteers revealed that the total bupropion clearance via alleles *1, *2, *5 and *6 did not differ, although Cmax, AUC and metabolic ratio for hydroxybupropion were considerably lower in *6/*6 and *1/*6 compared to *1/*1 [140]. A 1.66-fold higher clearance was, however, found for allele *4, consistent with the higher activity of the K262R variant. Interestingly, the *4 allele was also found to have a dominant enhancing effect on the nicotine metabolism rate, while *5 and *6 alleles had no influence [141]. Whether the CYP2B6 genotype affects bupropione smoking cessation outcome is a complex question, because hydroxybupropione is an active metabolite. An influence of the *5 allele was recently reported [142].
Cyclophosphamide, one of the most widely used anticancer and immunosuppressant drugs, requires biotransformation as a prodrug by P450 enzymes, mainly CYP2B6 and CYP2C19, to yield the active 4-hydroxy metabolite, which is further decomposed chemically to the ultimate cytotoxic metabolite phosphoramide mustard. Limited studies reported that cyclophosphamide bioactivation may be enhanced by the c.516G>T allele in white subjects [143], whereas a certain promoter haplotype appears to affect Japanese subjects [144].
The metabolism of the synthetic µ-opioid receptor agonist methadone, which is used as a maintenance treatment for opioid addiction, depends on CYP2B6 [23, 24]. (S)-Methadone metabolism and to a lesser extent (R)-methadone metabolism are influenced by CYP2B6 genotype, and (S)-methadone plasma levels were about twice as high in *6/*6 carriers compared to the unmutated genotype. The authors argued that this is unlikely to have a major impact on µ-opioid receptor activation, which is mainly due to (R)-methadone [145]. However, in a recent follow-up study, it was shown that (S)-methadone is more potent than the (R)-enantiomer at blocking the voltage-gated hERG potassium channel, which plays a crucial role in the repolarization and duration of the cardiac action potential [146]. As discussed in this study, the blockage of hERG by methadone and other structurally diverse drugs can cause a prolonged QT interval, and this was indeed found in carriers of the *6/*6 genotype as compared to all other genotypes, indicating a higher risk of severe cardiac arrhythmias and sudden death for individuals carrying this genotype. Great inter-patient variability also exists in the dose of propofol required for efficient anesthetization. Common haplotypic differences in CYP2B6 and GABRE genes did not, however, account for a large part of the inter-patient variability [147].
In conclusion, CYP2B6 pharmacogenetics has only recently been considered. CYP2B6 genotyping predicts elevated plasma concentrations of efavirenz and nevirapine in HIV-infected individuals. This is in agreement with the lower activities of a number of alleles. However, as amino acid variants are common, substrate-dependent effects have to be expected. There is a lack of in vitro data for several important substrates which would provide a useful basis for further pharmacogenetic studies.
CYP2C subfamily
The human CYP2C subfamily consists of the four genes CYP2C18, 2C19, 2C9 and 2C8, which are localized in this order in a gene cluster on chromosome 10q24 [148]. Of these, CYP2C18 is highly expressed in liver as mRNA, but for as-yet unknown reasons the mRNA does not get efficiently translated into protein [149]. Its contribution to drug metabolism is therefore limited. The other three members are expressed in the order CYP2C9>CYP2C8»CYP2C19, together constituting on average between 30 and 40% of the microsomal hepatic P450 pool. They are also expressed at lower levels but as functional enzymes in the human small intestine, where they are independently regulated [150]. All three expressed CYP2C enzymes are inducible by ligands of the PXR/CAR and glucocorticoid (GR) nuclear receptor pathways through different cis-acting elements in their upstream regulatory regions [151–153]. Given their strong relatedness with respect to DNA and protein sequence (>82%) and their common mechanisms of transcriptional regulation, it is quite surprising just how unique each enzyme is in terms of substrate specificity and clinical significance. All four CYP2C genes are genetically polymorphic, but only the CYP2C19 polymorphism comprises null alleles of sufficiently high frequency to produce a poor metabolizer phenotype, whereas the more common CYP2C8 and CYP2C9 polymorphisms result in functional amino acid variants. The CYP2C subfamily enzymes also metabolize arachidonic acid and some steroids, and they are expressed in endothelial cells, where they are implicated in the regulation of vascular tone [154].
CYP2C8
Among the top 200 drugs, CYP2C8 is mainly responsible for the metabolism of the antidiabetics rosiglitazone and pioglitazone, the antiarrhythmic amiodarone, and retinoic acid drugs used in acne and cancer treatment; it also participates in the metabolism of some drugs also metabolized by CYP2C9, e.g., ibuprofen (Table 1). Additional important drug oxidations catalyzed primarily by CYP2C8 are the 6-alpha hydroxylation of the natural anticancer drug paclitaxel and the deethylation of the antimalarial amodiaquine, both of which are useful probe drugs for CYP2C8 phenotyping. CYP2C8 plays a major role in metabolizing antimalarials, as chloroquine and dapsone are also substrates [155]. The clinical significance of CYP2C8 became clear after cerivastatin had to be removed from the market following fatal drug interactions which were in part due to its potent inhibition by gemfibrozil acyl-glucuronide, ultimately leading to rhabdomyolysis [156, 157]. Other potent inhibitors at clinically relevant concentrations include antiretroviral drugs, such as efavirenz, saquinavir, lopinavir, and tipranavir.
Apart from rare variants with no (*5, *7), reduced (*8) or unknown activity, there are three more common alleles CYP2C8*2, *3, and *4, which code for functional amino acid variants of the protein (Table 3). The frequency of the *2 allele is highest in black subjects, with reported frequencies of 15–20%, but much lower and absent, respectively, in Caucasians and Asians [158–161]. The variant had twofold increased intrinsic clearance for paclitaxel due to increased K m, but no significant in vivo associations were reported. The *3 allele occurs more frequently in white subjects (13–23%) and is virtually absent in Africans and Asians [158–162], whereas the *4 allele, which is not well investigated from a functional point of view, also occurs in Caucasians (~8%) and is practically absent in the other major races. The CYP2C8.3 variant was initially shown to reduce the metabolism of arachidonic acid and paclitaxel hydroxylation in vitro by ~40% and ~80%, respectively [158]. Recent clinical studies involving patients treated with paclitaxel [163] as well as amodiaquine [161] did not, however, find any evidence for altered pharmacokinetics, toxicity, or efficacy of these drugs in carriers of any of these alleles. It should be noted that the CYP2C8*3 variant is in partial linkage disequilibrium with the CYP2C9*2 allele, which should be of particular importance for substrates metabolized by both enzymes such as ibuprofen. Indeed, CYP2C8*3 genotypes were associated, together with CYP2C9*2 and *3 alleles, with reduced clearance of ibuprofen [164]. Functional effects of CYP2C8*3 appear to be substrate-dependent, because a higher metabolic capacity was observed for repaglinide [165] and rosiglitazone [166]. In conclusion, the CYP2C8 polymorphisms show high interethnic variation, with three nonsynonymous alleles *2, *3, and *4 having frequencies of between 7.5 and 20%. Their functional effects appear to be substrate-dependent.
CYP2C9
This P450, which is very abundantly expressed hepatically, accepts many weakly acidic substances like the anticoagulant warfarin, the anticonvulsants phenytoin and valproic acid, cardiovascular drugs like rosuvastatin and losartan, and several nonsteroidal anti-inflammatory drugs (NSAIDs, Table 1). Many of these drugs have a narrow therapeutic index, and variations in CYP2C9 activity are thus among the recognized factors for adverse drug reactions.
The *2 and *3 alleles were discovered first and have been investigated more thoroughly than the more recently identified alleles. These two alleles are present in approximately 35% of Caucasian individuals, but are much less prevalent in black and Asian populations [167]. In vitro data have consistently demonstrated that the CYP2C9*2 and *3 alleles are associated with significant but highly variable reductions in intrinsic clearance, depending on the particular substrate [168]. The *3 allele is more strongly affected than *2, and the reduction in activity can be up to 90% for some substrates. Other alleles with decreased function but rare occurrence are *5, *6, *8, *11 and several promoter variants with as-yet unclear significances [169]. Numerous clinical studies have demonstrated the clinical significance of the CYP2C9*2 and *3 polymorphisms for most of the drug substrates mentioned above. For example, carriers of *2 and *3 alleles were reported to experience higher incidences of adverse drug reactions like hypoglycemia from hypoglycemic drugs [170], gastrointestinal bleeding from NSAIDs [171], and serious bleeding from warfarin treatment, where anticoagulant response also depends on variants of vitamin K epoxide reductase [172].
CYP2C19
This CYP2C isozyme, the least expressed, was the first to be discovered due to its marked genetic polymorphism, resulting in (S)-mephenytoin-poor (PM) and extensive metabolizer (EM) phenotypes. Although not initially of any particular clinical interest, the CYP2C19 isozyme was later found to show a marked preference for proton-pump inhibitors (PPI) like omeprazole and pantoprazole, and numerous additional important drugs have been identified as major CYP2C19 substrates in recent years (Table 1). The PM phenotype results from two null alleles, leading to the absence of functional CYP2C19 protein, whereas extensive metabolizers carry at least one functional allele. About 3–5% of white and black populations but up to 20% of Asians are carriers of two null alleles. The two most common null alleles are CYP2C19*2, which occurs almost exclusively in Caucasians, and CYP2C19*3, which occurs primarily in Asians [173]. A promoter variant has recently been identified which appears to be related to increased substrate turnover by an as-yet unexplained mechanism [174]. CYP2C19 plays a prominent role in the metabolism of several first- and second-generation antidepressants [175, 176]. Pharmacokinetic effects of the CYP2C19 genotype have been observed, for example for clomipramine [177], citalopram [178], and amitriptyline [179]. These were sometimes related to adverse side effects, but an influence on pharmacodynamic outcome has not been apparent in the studies performed so far.
The effect of the CYP2C19 polymorphism on H. pylori eradication therapy is a particularly intriguing example of the clinical application of pharmacogenetics. The common eradication strategy involves the application of two antibiotics, e.g., amoxicillin and clarithromycin, together with the proton-pump inhibitor. The rationale for this combination is that acid suppression not only contributes to accelerated ulcer healing and improvement in symptoms, but it also increases the effectiveness of the antibiotics. The PPI-induced increase in the intragastric pH value depends on the plasma concentrations achieved over time, which are strongly influenced by CYP2C19 polymorphism. In several studies in Asia and Europe, it was shown that, in this case, PM subjects benefit from their lower metabolism rate because their drug levels stay higher for longer periods [180–182]. Other studies also confirmed the beneficial influence of CYP2C19-deficient alleles in the treatment of gastroesophageal reflux disease (GERD) with PPIs [183]. Esomeprazole-induced healing of GERD, however, appears to be unrelated to the CYP2C19 genotype, which can be explained by the metabolic shift toward the CYP3A4-mediated pathway [184]. Therefore, these data suggest that subjects with the *1/*1 genotype should receive higher doses of these PPIs in order to achieve stronger acid suppression compared to *1/*2 and *2/*2 subjects.
In contrast to the increased response to PPIs, CYP2C19 PMs were shown to have a significantly lower antiplatelet effect due to clopidogrel. Several studies found that CYPC19*2 is a major determinant of clopidogrel plasma levels and inter-individual variability in response [185–188]. The activation of clopidogrel by P450-dependent oxidation has been investigated, but CYP3A and not CYP2C19 have been identified as the major contributor [58]. Moreover, as clopidogrel is a potent inhibitor of both CYP2C19 and CYP2B6 [189], the basis for the influence of CYP2C19 genotype on the clopidogrel treatment effect awaits further investigation.
CYP2D6
This was the first P450 for which a classical pharmacogenetic polymorphism became known, and is the most intensely studied polymorphic P450. CYP2D6 is primarily expressed in the liver, but it is also localized in brain neurons, where it may participate in local drug metabolism and/or in certain endogenous biotransformations. Among all of the P450s discussed here, CYP2D6 is undoubtedly the one with the biggest genetic influence and, as environmental factors are of minor importance, the CYP2D6 drug oxidation phenotype, usually determined from the urinary metabolic ratio of a test drug, represents a stable and reproducible personal parameter. Debrisoquine, dextromethorphan, metoprolol, sparteine, and tramadol have been used for this purpose. For historical and basic facts about CYP2D6 polymorphism and allele frequencies, the reader is referred to recent specific review articles [190, 191].
About 5–10% of Caucasians carry two null alleles and are thus PMs, whereas this phenotype has a frequency of only 0–1% in Africans and Asians. The most frequent null allele is *4, with an allele frequency of about 20–25% in Caucasians, where it is responsible for 70–90% of all PMs. The absence of a PM phenotype in Oriental populations is due to the virtual absence of the *4 allele. In African and in African-American populations it is present with frequencies that are intermediate between those for Asians and Caucasians. The CYP2D6 gene deletion allele *5 is present at a similar frequency of 3–5% in most populations. The null alleles *3 and *6 are present at frequencies of slightly above 1% in Caucasians, but all other null alleles appear to be very rare (see the CYP allele nomenclature homepage). Recent studies in our lab have concentrated on the so-called intermediate metabolizer phenotype, which occurs in about 10–15% of white individuals. We found that most Caucasian IMs carry the partially defective allele *41 in combination with either a null allele or the same or another partially defective allele [192]. The mechanism by which the *41 allele reduces function is through a mutation 2988G>A in intron 6 of *41, which leads to erroneous splicing, resulting in only a fraction of the correctly spliced mRNA [193]. In Africans and Asians, there are other partially defective alleles, termed *17 and *10, respectively. In black populations the *17 allele is present at frequencies of up to 30%, whereas the *10 variant occurs at levels of up to 50% in Asians.
The CYP2D locus on chromosome 22 also includes two pseudogenes, CYP2D7 and CYP2D8P. Unequal crossover between these genes, involving a certain repetitive sequence also present in the c-myc gene, leads to recombination events that result in gross structural variants where the functional gene can be either deleted (*5) or duplicated, leading to the UM phenotype due to overexpression in liver [194–196]. CYP2D6 gene duplications are now known to have occured with various alleles, including *1,*2, *4, *6, *10, *17, *29, *35,*41, *43 and *45. The frequency of the gene duplications varies between 10 and over 50% in some ethnic populations, including certain Arabian, Eastern African and Pacific populations, whereas in Europe it is usually between 1 and 5%. It has been speculated that the remarkable preference of CYP2D6 for plant alkaloids may have been the result of natural selection in some East African populations that depended on food with toxic alkaloids, thereby leading to the accumulation of alleles with increased copy number and higher activity, and probably also because an efficient induction mechanism was not available for this enzyme [195]. An assay based on TaqMan real-time quantification of CYP2D6 in relation to albumin as an internal reference gene was shown to correctly measure the overall number of CYP2D6 gene copies in a variety of genetic constellations [197]. It was also demonstrated that the strategy of copy number determination in combination with SNP analysis is sufficient for correct phenotype prediction. The CYP2D6 variants that we recommend for inclusion in regular genotyping are summarized in Table 3.
Recent studies on the impact of the CYP2D6 genotype on treatment outcome and/or adverse drug reactions included metoprolol [198], propafenone [199], amitriptyline [179], and other antidepressants [176, 200]. In the case of prodrugs, metabolism leads to the pharmacologically active substance, as is the case for codeine, which is O-demethylated by CYP2D6 to morphine. An increased effectiveness of codeine with sometimes life-threatening opioid intoxication was observed in patients with multiple CYP2D6 gene copies, consistent with the UM phenotype [201–203].
An important example of cancer therapy where CYP2D6 pharmacogenetics appears to have a major impact is the adjuvant treatment of breast cancer with tamoxifen, an antiestrogen that is extensively metabolized in the liver to several primary and secondary metabolites. Two of these, 4-hydroxytamoxifen and the secondary metabolite endoxifen, are mainly formed by CYP2D6, and they show high affinity to the estrogen receptor and are thought to be mainly responsible for the antiestrogenic effect [204, 205]. Several recent retrospective and prospective studies demonstrated a significant impact of the CYP2D6 genotype on the plasma concentrations of the active tamoxifen metabolites, treatment outcome and adverse effects (reviewed by [206]). According to these studies, patients with PM (*null/*null) and IM (e.g., *41/*null) genotypes (i.e., those with low metabolic activation rates) have extremely low levels of the active metabolites and thus profit less from the treatment. They have a shorter time to recurrence and worse relapse-free survival relative to patients with the EM genotype [207, 208]. These recent findings do not yet allow us to design new treatment strategies. However, with appropriately conducted prospective studies, they may open up new paths to more and better treatment alternatives for woman with breast cancer.
CYP3A subfamily
CYP3A enzymes are responsible for the metabolism of approximately 37% of the top 200 and many other important drugs, including drugs from all therapeutic categories, like the immunosuppressants cyclosporin A and tacrolimus, macrolide antibiotics like erythromycin, anticancer drugs like taxol, benzodiazepines, HMG-CoA reductase inhibitors like simvastatin and atorvastatin, anesthetics, and many more [209]. Besides drugs, CYP3A4 also plays an important role in the metabolism of several endogenous substances, including testosterone, progesterone, androstenedione and bile acids [210, 211].
The CYP3A subfamily consists of the four genes 3A4, 3A5, 3A7, and 3A43, which are located on chromosome 7. This subfamily contributes to the metabolism of the most diverse group of substrates of all human P450s, as their active sites are large and flexible enough to bind and metabolize many preferentially lipophilic compounds with comparatively large structures [212]. The expressions of the three isoforms CYP3A5, CYP3A7 and CYP3A43 are generally much lower than that for CYP3A4, and CYP3A7 is more abundantly expressed in fetal liver than in adult liver, whereas CYP3A43 is practically undetectable. Several pathways contribute to the complex regulation of CYP3A enzymes, primarily at the transcriptional level. Following exposure to a number of structurally diverse drugs that bind as ligands to the nuclear receptor PXR (pregnane X receptor), the gene transcription rate is enhanced as PXR/RXR heterodimers interact with PXR responsive elements (PXRE) located in the proximal promoter and in the XREM region located −8 kb upstream [213]. Another recognized pathway for the transcriptional regulation of CYP3A4 expression is via inflammatory signaling pathways [214]. Furthermore, CYP3A4 is the only human drug-metabolizing P450 that shows a significant sex difference, in that women express approximately 1.5- to 2-fold more CYP3A4 than men do [215]. This contributes to a higher in vivo clearance of several typical CYP3A4 drug substrates [7]. The mechanism(s) behind the sex differences in expression are presumably transcriptional in nature and they may be related to the sex differences in plasma growth hormone profiles [216]. One study also indicated gene–sex interactions for some polymorphisms at the CYP3A locus [217].
It has been proposed that genetic factors play a major role in CYP3A4 phenotype determination [218]. However, there is currently little evidence for a significant contribution of CYP3A4 gene polymorphisms in determining CYP3A4 activity. Besides a number of rare amino acid variants [219], no polymorphisms with a clear genotype–phenotype relationship have so far been described for the CYP3A4 gene, although a number of large-scale sequencing and phenotype–genotype correlation studies have been carried out [217, 220, 221]. The most extensively studied polymorphism is the -392A>G proximal promoter variant (CYP3A4*1B), which has a frequency in white populations of about 4%, but a much higher frequency in black subjects (Table 3). Its functional effect remains controversial [222, 223]. A few common defective alleles of CYP3A5 and CYP3A7 restrict their expression to the fraction of the population who carry the respective functional *1 allele [220, 224–226]. The CYP3A5*1 frequency is rather low in Caucasians, but in Africans it is the more frequent variant, leading to a higher average proportion of CYP3A5 in the total liver CYP3A pool in subjects of black origin (Table 3). The mechanism leading to lower expression from the *3 and *6 alleles involves aberrant splicing [220, 224].
CYP3A4*1B was initially discovered through its association with high-grade prostate cancer [227], and with a reduced risk for treatment-related leukemia [228]. Because CYP3A5 is the major form expressed in the prostate, where it may contribute to andogen metabolism, and because the CYP3A4*1B allele and the functional CYP3A5*1 allele are in partial linkage disequilibrium, it has been suggested that the reported association between the CYP3A4*1B allele and high-grade prostate cancer could also be explained by increased CYP3A5 expression rather than by altered expression or activity of CYP3A4 [229, 230]. Although the impact of polymorphic CYP3A5 is generally low due to the absence of specific substrates, and because of the large contribution of nongenetic mechanisms to variability, effects of CYP3A5 expression status have recently been found for therapy with the immunosuppressant tacrolimus [231, 232] the antihypertensive verapamil [233], and the HIV protease inhibitor saquinavir [234].
In the absence of clearly predictive polymorphisms in the CYP3A4 gene, recent studies have pointed out that other genes may effectively influence CYP3A4 basal and inducible expression phenotype. The MDR1 2677T (Ser893) allele resulted in higher basal CYP3A4 expression and activity, whereas the 2677G allele showed a higher rifampin induction ratio in primary hepatocytes [235]. Moreover, polymorphisms mostly located in promoter or intron 1 regions of PXR were found to be associated with CYP3A4 basal expression levels and to influence inducibility, depending to some extent on sex [236]. Candidate gene approaches with a broad coverage of genes that potentially influence constitutive and inducible CYP3A4 gene expression in phenotypically well-defined tissues or volunteers may thus help to advance the functional genomics of CYP3A4.
Conclusions and future perspectives
Eight human cytochrome P450 enzymes from five subfamilies (1A, 2B, 2C, 2D, 3A) are responsible for the vast majority of oxidative drug metabolisms of the most important clinical drugs. Among the 200 drugs sold in the greatest quantities in the US, about 80% are cleared primarily by these CYPs. Cytochromes P450 CYP1A2, CYP2C8 and CYP3A4, which lack major functional polymorphisms, are responsible for about half of these (52%), whereas the rest take metabolic routes that are significantly influenced by gene polymorphisms in the CYP2B6, CYP2C9, CYP2C19 and CYP2D6 genes. For these polymorphic enzymes, probably most of the functional polymorphisms that are common (>5%) in Caucasians may have been identified, although in other races there may still be important undiscovered alleles. From an analytical point of view, there are numerous reliable genotyping methods, from low to high throughput, including real-time PCR for individual SNPs or determination of gene copy number [197], pyrosequencing [237], MALDI-TOF mass spectrometry [238], as well as dedicated microarrays [239] that are now available. Impressive examples of genotype–phenotype or genotype–clinical outcome relationships have been elucidated for these polymorphic CYPs over the past few years which warrant clinical application. Nevertheless, these studies emphasize the complexities that arise at the level of basic mechanisms (null alleles, partially functional alleles, substrate-dependent effects, linkage disequilibrium, etc.), as well as the pharmacological and clinical levels (PD versus PK, adverse reactions, prodrugs, etc.). Drug toxicity and treatment outcome depend on many additional genetic and nongenetic factors, not just on a single genotype. Only in a few instances, with particular drugs and treatment schemes, will the patient have a clearly predictable benefit from simple genotyping. In the majority of clinical situations, multigene or multifactorial approaches will be needed to achieve an overall improvement in drug therapy, which implies minimizing the risk of adverse reactions while increasing the chances of effective treatment. To progress, well-designed studies are required that take an integrated approach in order to consider not only validated gene polymorphisms but also other recognized factors, depending on the particular drug or disease studied, as exemplified by our recent study on fluorouracil toxicity [240]. Regarding the less predictable genes, especially CYP1A2 and CYP3A4, the inclusion of multiple external candidate genes which influence their expression along different pathways may lead to the discovery of novel polymorphisms within those genes, although it is expected that these will be genes/polymorphisms that have only minor impacts, comparable to the situation in multifactorial diseases. Similarly, full-genome scans with high-density SNP microarrays have also not been applied so far in order to identify further genes of interest for functional prediction, neither in cytochrome P450 research in the narrow sense nor in the general sense of phamacogenetics/genomics. Other largely unexplored areas of future research with particular relevance to unexplained variability in drug-metabolizing enzyme function include epigenetics [241] and RNA silencing mechanisms [2, 242], but also protein phosphorylation, which was shown to affect, for example, the activity of rat CYP2B1 [243]. The integrations of such diverse data into comprehensive models of metabolic and gene regulatory networks, not only within ADME genes but especially with respect to their connections to central cellular metabolism, cholesterol homeostasis [244] and other cellular processes, is a further challenge that may be accomplished by systems biology approaches [245, 246].
Abbreviations
- ADME:
-
Absorption, distribution, metabolism, excretion
- CAR:
-
Constitutive androstane receptor
- CYP:
-
Cytochrome P450
- MALDI-TOF:
-
Matrix-assisted laser desorption ionisation-time of flight
- NNRTI:
-
Non-nucleosidic reverse transcriptase inhibitor
- NSAID:
-
Nonsteroidal antiinflammatory drug
- PD:
-
Pharmacodynamics
- PK:
-
Pharmacokinetics
- PPI:
-
Proton pump inhibitor
- PXR:
-
Pregnane X receptor
- XREM:
-
Xenobiotic-responsive enhancer module
References
Lewis DF (2004) Pharmacogenomics 5:305–318
Ingelman-Sundberg M, Sim SC, Gomez A, Rodriguez-Antona C (2007) Pharmacol Ther 116:496–526
Meyer UA (2004) Nat Rev Genet 5:669–676
Eichelbaum M, Ingelman-Sundberg M, Evans WE (2006) Annu Rev Med 57:119–137
Gardiner SJ, Begg EJ (2006) Pharmacol Rev 58:521–590
Pascussi JM, Vilarem MJ (2008) Med Sci (Paris) 24:301–305
Cotreau MM, von Moltke LL, Greenblatt DJ (2005) Clin Pharmacokinet 44:33–60
Levi F, Schibler U (2007) Annu Rev Pharmacol Toxicol 47:593–628
Aitken AE, Richardson TA, Morgan ET (2006) Annu Rev Pharmacol Toxicol 46:123–149
Prescott LF (2000) Br J Clin Pharmacol 49:291–301
Elkader A, Sproule B (2005) Clin Pharmacokinet 44:661–680
Tang C, Shou M, Mei Q, Rushmore TH, Rodrigues AD (2000) J Pharmacol Exp Ther 293:453–459
Vree TB, Verwey-van Wissen CP (1992) Biopharm Drug Dispos 13:445–460
Leemann T, Transon C, Dayer P (1993) Life Sci 52:29–34
Tougou K, Gotou H, Ohno Y, Nakamura A (2004) Xenobiotica 34:449–461
Feierman DE, Lasker JM (1996) Drug Metab Dispos 24:932–939
Hutchinson MR, Menelaou A, Foster DJ, Coller JK, Somogyi AA (2004) Br J Clin Pharmacol 57:287–297
Benetton SA, Borges VM, Chang TK, McErlane KM (2004) Xenobiotica 34:335–344
Hamman MA, Thompson GA, Hall SD (1997) Biochem Pharmacol 54:33–41
Nakajima M, Inoue T, Shimada N, Tokudome S, Yamamoto T, Kuroiwa Y (1998) Drug Metab Dispos 26:261–266
Chesne C, Guyomard C, Guillouzo A, Schmid J, Ludwig E, Sauter T (1998) Xenobiotica 28:1–13
Ramirez J, Innocenti F, Schuetz EG, Flockhart DA, Relling MV, Santucci R, Ratain MJ (2004) Drug Metab Dispos 32:930–936
Gerber JG, Rhodes RJ, Gal J (2004) Chirality 16:36–44
Totah RA, Sheffels P, Roberts T, Whittington D, Thummel K, Kharasch ED (2008) Anesthesiology 108:363–374
Tracy TS, Marra C, Wrighton SA, Gonzalez FJ, Korzekwa KR (1997) Eur J Clin Pharmacol 52:293–298
Lalovic B, Kharasch E, Hoffer C, Risler L, Liu-Chen LY, Shen DD (2006) Clin Pharmacol Ther 79:461–479
Takanashi K, Tainaka H, Kobayashi K, Yasumori T, Hosakawa M, Chiba K (2000) Pharmacogenetics 10:95–104
Somogyi AA, Menelaou A, Fullston SV (2004) Xenobiotica 34:875–887
Subrahmanyam V, Renwick AB, Walters DG, Young PJ, Price RJ, Tonelli AP, Lake BG (2001) Drug Metab Dispos 29:1146–1155
Ghahramani P, Ellis SW, Lennard MS, Ramsay LE, Tucker GT (1997) Br J Clin Pharmacol 43:137–144
Venkatakrishnan K, Schmider J, Harmatz JS, Ehrenberg BL, von Moltke LL, Graf JA, Mertzanis P, Corbett KE, Rodriguez MC, Shader RI, Greenblatt DJ (2001) J Clin Pharmacol 41:1043–1054
Hendset M, Hermann M, Lunde H, Refsum H, Molden E (2007) Eur J Clin Pharmacol 63:1147–1151
Hesse LM, Venkatakrishnan K, Court MH, von Moltke LL, Duan SX, Shader RI, Greenblatt DJ (2000) Drug Metab Dispos 28:1176–1183
Faucette SR, Hawke RL, Lecluyse EL, Shord SS, Yan B, Laethem RM, Lindley CM (2000) Drug Metab Dispos 28:1222–1230
Hiemke C, Hartter S (2000) Pharmacol Ther 85:11–28
Lobo ED, Bergstrom RF, Reddy S, Quinlan T, Chappell J, Hong Q, Ring B, Knadler MP (2008) Clin Pharmacokinet 47:191–202
Rochat B, Amey M, Gillet M, Meyer UA, Baumann P (1997) Pharmacogenetics 7:1–10
Fang J, Baker GB, Silverstone PH, Coutts RT (1997) Cell Mol Neurobiol 17:227–233
Timmer CJ, Sitsen JM, Delbressine LP (2000) Clin Pharmacokinet 38:461–474
Stormer E, von Moltke LL, Shader RI, Greenblatt DJ (2000) Drug Metab Dispos 28:1168–1175
Ring BJ, Catlow J, Lindsay TJ, Gillespie T, Roskos LK, Cerimele BJ, Swanson SP, Hamman MA, Wrighton SA (1996) J Pharmacol Exp Ther 276:658–666
DeVane CL, Nemeroff CB (2001) Clin Pharmacokinet 40:509–522
Yasui-Furukori N, Hidestrand M, Spina E, Facciola G, Scordo MG, Tybring G (2001) Drug Metab Dispos 29:1263–1268
Rotzinger S, Fang J, Baker GB (1998) Drug Metab Dispos 26:572–575
Shams ME, Arneth B, Hiemke C, Dragicevic A, Muller MJ, Kaiser R, Lackner K, Hartter S (2006) J Clin Pharm Ther 31:493–502
Prakash C, Kamel A, Cui D, Whalen RD, Miceli JJ, Tweedie D (2000) Br J Clin Pharmacol 49(Suppl 1):35S–42S
Neuvonen PJ, Niemi M, Backman JT (2006) Clin Pharmacol Ther 80:565–581
Miller DB, Spence JD (1998) Clin Pharmacokinet 34:155–162
Kirchheiner J, Brockmoller J (2005) Clin Pharmacol Ther 77:1–16
Jaakkola T, Laitila J, Neuvonen PJ, Backman JT (2006) Basic Clin Pharmacol Toxicol 99:44–51
Baldwin SJ, Clarke SE, Chenery RJ (1999) Br J Clin Pharmacol 48:424–432
Rodrigues AD, Roberts EM, Mulford DJ, Yao Y, Ouellet D (1997) Drug Metab Dispos 25:623–630
Wynalda MA, Hutzler JM, Koets MD, Podoll T, Wienkers LC (2003) Drug Metab Dispos 31:878–887
Watkins PB, Wrighton SA, Maurel P, Schuetz EG, Mendez-Picon G, Parker GA, Guzelian PS (1985) Proc Natl Acad Sci USA 82:6310–6314
Cribb AE, Spielberg SP, Griffin GP (1995) Drug Metab Dispos 23:406–414
Ohyama K, Nakajima M, Nakamura S, Shimada N, Yamazaki H, Yokoi T (2000) Drug Metab Dispos 28:1303–1310
Oldham HG, Clarke SE (1997) Drug Metab Dispos 25:970–977
Clarke TA, Waskell LA (2003) Drug Metab Dispos 31:53–59
Savi P, Combalbert J, Gaich C, Rouchon MC, Maffrand JP, Berger Y, Herbert JM (1994) Thromb Haemost 72:313–317
Bourrie M, Meunier V, Berger Y, Fabre G (1999) Drug Metab Dispos 27:288–296
Stearns RA, Chakravarty PK, Chen R, Chiu SH (1995) Drug Metab Dispos 23:207–215
Otton SV, Crewe HK, Lennard MS, Tucker GT, Woods HF (1988) J Pharmacol Exp Ther 247:242–247
Johnson JA, Herring VL, Wolfe MS, Relling MV (2000) J Pharmacol Exp Ther 294:1099–1105
Ji HY, Lee HW, Kim HH, Kim DS, Yoo M, Kim WB, Lee HS (2004) Xenobiotica 34:973–982
Fuhr U, Kober S, Zaigler M, Mutschler E, Spahn-Langguth H (2005) Int J Clin Pharmacol Ther 43:327–334
Nakashima A, Kawashita H, Masuda N, Saxer C, Niina M, Nagae Y, Iwasaki K (2005) Xenobiotica 35:589–602
Busse D, Cosme J, Beaune P, Kroemer HK, Eichelbaum M (1995) Naunyn Schmiedebergs Arch Pharmacol 353:116–121
Kroemer HK, Gautier JC, Beaune P, Henderson C, Wolf CR, Eichelbaum M (1993) Naunyn Schmiedebergs Arch Pharmacol 348:332–337
Kaminsky LS, Zhang ZY (1997) Pharmacol Ther 73:67–74
Wang B, Sanchez RI, Franklin RB, Evans DC, Huskey SE (2004) Drug Metab Dispos 32:1209–1212
Kobayashi K, Mimura N, Fujii H, Minami H, Sasaki Y, Shimada N, Chiba K (2000) Clin Cancer Res 6:3297–3303
Yamazaki H, Shimada T (1997) Arch Biochem Biophys 346:161–169
Abelo A, Andersson TB, Antonsson M, Naudot AK, Skanberg I, Weidolf L (2000) Drug Metab Dispos 28:966–972
Katsuki H, Hamada A, Nakamura C, Arimori K, Nakano M (2001) Eur J Clin Pharmacol 57:709–715
Desta Z, Wu GM, Morocho AM, Flockhart DA (2002) Drug Metab Dispos 30:336–343
Tanaka M, Ohkubo T, Otani K, Suzuki A, Kaneko S, Sugawara K, Ryokawa Y, Ishizaki T (2001) Clin Pharmacol Ther 69:108–113
VandenBranden M, Ring BJ, Binkley SN, Wrighton SA (1996) Pharmacogenetics 6:81–91
Warrington JS, Shader RI, von Moltke LL, Greenblatt DJ (2000) Drug Metab Dispos 28:392–397
Ring BJ, Patterson BE, Mitchell MI, VandenBranden M, Gillespie J, Bedding AW, Jewell H, Payne CD, Forgue ST, Eckstein J, Wrighton SA, Phillips DL (2005) Clin Pharmacol Ther 77:63–75
Kamimura H, Oishi S, Matsushima H, Watanabe T, Higuchi S, Hall M, Wood SG, Chasseaud LF (1998) Xenobiotica 28:909–922
Othman AA, Syed SA, Newman AH, Eddington ND (2007) J Pharmacol Exp Ther 320:344–353
Kerr BM, Thummel KE, Wurden CJ, Klein SM, Kroetz DL, Gonzalez FJ, Levy RH (1994) Biochem Pharmacol 47:1969–1979
Tiseo PJ, Perdomo CA, Friedhoff LT (1998) Br J Clin Pharmacol 46(Suppl 1):30–34
Yasumori T, Chen LS, Li QH, Ueda M, Tsuzuki T, Goldstein JA, Kato R, Yamazoe Y (1999) Biochem Pharmacol 57:1297–1303
Kiang TK, Ho PC, Anari MR, Tong V, Abbott FS, Chang TK (2006) Toxicol Sci 94:261–271
Yasuda SU, Zannikos P, Young AE, Fried KM, Wainer IW, Woosley RL (2002) Br J Clin Pharmacol 53:519–525
Akutsu T, Kobayashi K, Sakurada K, Ikegaya H, Furihata T, Chiba K (2007) Drug Metab Dispos 35:72–78
Pearce RE, Leeder JS, Kearns GL (2006) Drug Metab Dispos 34:1035–1040
Benedetti MS, Plisnier M, Kaise J, Maier L, Baltes E, Arendt C, McCracken N (2001) Eur J Clin Pharmacol 57:571–582
Yumibe N, Huie K, Chen KJ, Snow M, Clement RP, Cayen MN (1996) Biochem Pharmacol 51:165–172
Chiba M, Xu X, Nishime JA, Balani SK, Lin JH (1997) Drug Metab Dispos 25:1022–1031
Manchee GR, Eddershaw PJ, Ranshaw LE, Herriott D, Park GR, Bayliss MK, Tarbit MH (1996) Drug Metab Dispos 24:555–559
Greenblatt DJ, von Moltke LL, Harmatz JS, Ciraulo DA, Shader RI (1993) J Clin Psychiatry 54:4–11 Suppl
Dalen P, Alvan G, Wakelkamp M, Olsen H (1996) Pharmacogenetics 6:387–394
Wang RW, Liu L, Cheng H (1996) Drug Metab Dispos 24:786–791
Andersson T, Miners JO, Veronese ME, Birkett DJ (1994) Br J Clin Pharmacol 38:131–137
Najib J (2006) Clin Ther 28:491–516
Granfors MT, Backman JT, Laitila J, Neuvonen PJ (2004) Br J Clin Pharmacol 57:349–353
Pichard L, Gillet G, Bonfils C, Domergue J, Thenot JP, Maurel P (1995) Drug Metab Dispos 23:1253–1262
Bach MV, Coutts RT, Baker GB (1999) Xenobiotica 29:719–732
Ring BJ, Gillespie JS, Eckstein JA, Wrighton SA (2002) Drug Metab Dispos 30:319–323
Kivisto KT, Lamberg TS, Kantola T, Neuvonen PJ (1997) Clin Pharmacol Ther 62:348–354
Butler MA, Iwasaki M, Guengerich FP, Kadlubar FF (1989) Proc Natl Acad Sci USA 86:7696–7700
Tomlinson ES, Lewis DF, Maggs JL, Kroemer HK, Park BK, Back DJ (1997) Biochem Pharmacol 54:605–611
Marill J, Capron CC, Idres N, Chabot GG (2002) Biochem Pharmacol 63:933–943
Robertson P Jr, Hellriegel ET (2003) Clin Pharmacokinet 42:123–137
Nakamura K, Yokoi T, Inoue K, Shimada N, Ohashi N, Kume T, Kamataki T (1996) Pharmacogenetics 6:449–457
Luque CA, Rey JA (1999) Ann Pharmacother 33:968–978
McSorley LC, Daly AK (2000) Biochem Pharmacol 60:517–526
Mwenifumbo JC, Tyndale RF (2007) Pharmacogenomics 8:1385–1402
Gonzalez FJ (2007) Drug Metab Dispos 35:1–8
Landi MT, Sinha R, Lang NP, Kadlubar FF (1999) IARC Sci Publ 148:173–195
Rasmussen BB, Brix TH, Kyvik KO, Brosen K (2002) Pharmacogenetics 12:473–478
Nakajima M, Yokoi T, Mizutani M, Kinoshita M, Funayama M, Kamataki T (1999) J Biochem 125:803–808
Sachse C, Brockmoller J, Bauer S, Roots I (1999) Br J Clin Pharmacol 47:445–449
Ghotbi R, Christensen M, Roh HK, Ingelman-Sundberg M, Aklillu E, Bertilsson L (2007) Eur J Clin Pharmacol 63:537–546
Han XM, Ouyang DS, Chen XP, Shu Y, Jiang CH, Tan ZR, Zhou HH (2002) Br J Clin Pharmacol 54:540–543
Long JR, Egan KM, Dunning L, Shu XO, Cai Q, Cai H, Dai Q, Holtzman J, Gao YT, Zheng W (2006) Pharmacogenet Genomics 16:237–243
van der WJ, Steijns LS, van Weelden MJ (2003) Pharmacogenetics 13:169–172
Shimoda K, Someya T, Morita S, Hirokane G, Yokono A, Takahashi S, Okawa M (2002) Prog Neuropsychopharmacol Biol Psychiatry 26:261–265
Mihara K, Kondo T, Suzuki A, Yasui-Furukori N, Ono S, Otani K, Kaneko S (2001) Pharmacol Toxicol 88:267–270
Zhou H, Josephy PD, Kim D, Guengerich FP (2004) Arch Biochem Biophys 422:23–30
Chen X, Wang L, Zhi L, Zhou G, Wang H, Zhang X, Hao B, Zhu Y, Cheng Z, He F (2005) Clin Pharmacol Ther 78:249–259
Jiang Z, Dragin N, Jorge-Nebert LF, Martin MV, Guengerich FP, Aklillu E, Ingelman-Sundberg M, Hammons GJ, Lyn-Cook BD, Kadlubar FF, Saldana SN, Sorter M, Vinks AA, Nassr N, von RO, Jin L, Nebert DW (2006) Pharmacogenet Genomics 16:359–367
Harper PA, Riddick DS, Okey AB (2006) Biochem Pharmacol 72:267–279
Hoffman SM, Nelson DR, Keeney DS (2001) Pharmacogenetics 11:687–698
Hofmann MH, Blievernicht JK, Klein K, Saussele T, Schaeffeler E, Schwab M, Zanger UM (2008) J Pharmacol Exp Ther 325:284–292
Saussele T, Burk O, Blievernicht JK, Klein K, Nussler A, Nussler N, Hengstler JG, Eichelbaum M, Schwab M, Zanger UM (2007) Clin Pharmacol Ther 82:265–274
Turpeinen M, Raunio H, Pelkonen O (2006) Curr Drug Metab 7:705–714
Zanger UM, Klein K, Saussele T, Blievernicht J, Hofmann MH, Schwab M (2007) Pharmacogenomics 8:743–759
Lang T, Klein K, Fischer J, Nussler AK, Neuhaus P, Hofmann U, Eichelbaum M, Schwab M, Zanger UM (2001) Pharmacogenetics 11:399–415
Desta Z, Saussele T, Ward BA, Blievernicht J, Li L, Klein K, Flockhart DA, Zanger UM (2007) Pharmacogenomics 8(6):547–558
Klein K, Lang T, Saussele T, Barbosa-Sicard E, Schunck WH, Eichelbaum M, Schwab M, Zanger UM (2005) Pharmacogenet Genomics 15:861–873
Mehlotra RK, Bockarie MJ, Zimmerman PA (2007) Br J Clin Pharmacol 64(3):391–395
Telenti A, Zanger UM (2008) Annu Rev Pharmacol Toxicol 48:227–256
Rotger M, Tegude H, Colombo S, Cavassini M, Furrer H, Decosterd L, Blievernicht J, Saussele T, Gunthard HF, Schwab M, Eichelbaum M, Telenti A, Zanger UM (2007) Clin Pharmacol Ther 81:557–566
Rotger M, Saumoy M, Zhang K, Flepp M, Sahli R, Decosterd L, Telenti A (2007) Pharmacogenet Genomics 17:885–890
Gatanaga H, Hayashida T, Tsuchiya K, Yoshino M, Kuwahara T, Tsukada H, Fujimoto K, Sato I, Ueda M, Horiba M, Hamaguchi M, Yamamoto M, Takata N, Kimura A, Koike T, Gejyo F, Matsushita S, Shirasaka T, Kimura S, Oka S (2007) Clin Infect Dis 45:1230–1237
Penzak SR, Kabuye G, Mugyenyi P, Mbamanya F, Natarajan V, Alfaro RM, Kityo C, Formentini E, Masur H (2007) HIV Med 8:86–91
Kirchheiner J, Klein C, Meineke I, Sasse J, Zanger UM, Murdter TE, Roots I, Brockmoller J (2003) Pharmacogenetics 13:619–626
Johnstone E, Benowitz N, Cargill A, Jacob R, Hinks L, Day I, Murphy M, Walton R (2006) Clin Pharmacol Ther 80:319–330
David SP, Brown RA, Papandonatos GD, Kahler CW, Lloyd-Richardson EE, Munafo MR, Shields PG, Lerman C, Strong D, McCaffery J, Niaura R (2007) Nicotine Tob Res 9:821–833
Xie H, Griskevicius L, Stahle L, Hassan Z, Yasar U, Rane A, Broberg U, Kimby E, Hassan M (2006) Eur J Pharm Sci 27:54–61
Nakajima M, Komagata S, Fujiki Y, Kanada Y, Ebi H, Itoh K, Mukai H, Yokoi T, Minami H (2007) Pharmacogenet Genomics 17:431–445
Crettol S, Deglon JJ, Besson J, Croquette-Krokkar M, Gothuey I, Hammig R, Monnat M, Huttemann H, Baumann P, Eap CB (2005) Clin Pharmacol Ther 78:593–604
Eap CB, Crettol S, Rougier JS, Schlapfer J, Sintra GL, Deglon JJ, Besson J, Croquette-Krokar M, Carrupt PA, Abriel H (2007) Clin Pharmacol Ther 81:719–728
Iohom G, Ni CM, O'Brien JK, Cunningham AJ, Fitzgerald DF, Shields DC (2007) Eur J Anaesthesiol 24:912–919
Goldstein JA (2001) Br J Clin Pharmacol 52:349–355
Lofgren S, Baldwin RM, Hiratsuka M, Lindqvist A, Carlberg A, Sim SC, Schulke M, Snait M, Edenro A, Fransson-Steen R, Terelius Y, Ingelman-Sundberg M (2008) Drug Metab Dispos 36(5):955–962
Lapple F, von RO, Fromm MF, Richter T, Thon KP, Wisser H, Griese EU, Eichelbaum M, Kivisto KT (2003) Pharmacogenetics 13:565–575
Pascussi JM, Gerbal-Chaloin S, Drocourt L, Maurel P, Vilarem MJ (2003) Biochim Biophys Acta 1619:243–253
Ferguson SS, Lecluyse EL, Negishi M, Goldstein JA (2002) Mol Pharmacol 62:737–746
Ferguson SS, Chen Y, Lecluyse EL, Negishi M, Goldstein JA (2005) Mol Pharmacol 68:747–757
Chehal MK, Granville DJ (2006) Can J Physiol Pharmacol 84:15–20
Gil JP, Gil BE (2007) Pharmacogenomics 8:187–198
Ogilvie BW, Zhang D, Li W, Rodrigues AD, Gipson AE, Holsapple J, Toren P, Parkinson A (2006) Drug Metab Dispos 34:191–197
Backman JT, Kyrklund C, Neuvonen M, Neuvonen PJ (2002) Clin Pharmacol Ther 72:685–691
Dai D, Zeldin DC, Blaisdell JA, Chanas B, Coulter SJ, Ghanayem BI, Goldstein JA (2001) Pharmacogenetics 11:597–607
Rower S, Bienzle U, Weise A, Lambertz U, Forst T, Otchwemah RN, Pfutzner A, Mockenhaupt FP (2005) Trop Med Int Health 10:1271–1273
Nakajima M, Fujiki Y, Noda K, Ohtsuka H, Ohkuni H, Kyo S, Inoue M, Kuroiwa Y, Yokoi T (2003) Drug Metab Dispos 31:687–690
Parikh S, Ouedraogo JB, Goldstein JA, Rosenthal PJ, Kroetz DL (2007) Clin Pharmacol Ther 82:197–203
Bahadur N, Leathart JB, Mutch E, Steimel-Crespi D, Dunn SA, Gilissen R, Houdt JV, Hendrickx J, Mannens G, Bohets H, Williams FM, Armstrong M, Crespi CL, Daly AK (2002) Biochem Pharmacol 64:1579–1589
Henningsson A, Marsh S, Loos WJ, Karlsson MO, Garsa A, Mross K, Mielke S, Vigano L, Locatelli A, Verweij J, Sparreboom A, McLeod HL (2005) Clin Cancer Res 11:8097–8104
Garcia-Martin E, Martinez C, Tabares B, Frias J, Agundez JA (2004) Clin Pharmacol Ther 76:119–127
Niemi M, Leathart JB, Neuvonen M, Backman JT, Daly AK, Neuvonen PJ (2003) Clin Pharmacol Ther 74:380–387
Kirchheiner J, Thomas S, Bauer S, Tomalik-Scharte D, Hering U, Doroshyenko O, Jetter A, Stehle S, Tsahuridu M, Meineke I, Brockmoller J, Fuhr U (2006) Clin Pharmacol Ther 80:657–667
Garcia-Martin E, Martinez C, Ladero JM, Agundez JA (2006) Mol Diagn Ther 10:29–40
Lee CR, Goldstein JA, Pieper JA (2002) Pharmacogenetics 12:251–263
King BP, Khan TI, Aithal GP, Kamali F, Daly AK (2004) Pharmacogenetics 14:813–822
Holstein A, Plaschke A, Ptak M, Egberts EH, El-Din J, Brockmoller J, Kirchheiner J (2005) Br J Clin Pharmacol 60:103–106
Pilotto A, Seripa D, Franceschi M, Scarcelli C, Colaizzo D, Grandone E, Niro V, Andriulli A, Leandro G, Di MF, Dallapiccola B (2007) Gastroenterology 133:465–471
Flockhart DA, O'Kane D, Williams MS, Watson MS, Flockhart DA, Gage B, Gandolfi R, King R, Lyon E, Nussbaum R, O'Kane D, Schulman K, Veenstra D, Williams MS, Watson MS (2008) Genet Med 10:139–150
Desta Z, Zhao X, Shin JG, Flockhart DA (2002) Clin Pharmacokinet 41:913–958
Sim SC, Risinger C, Dahl ML, Aklillu E, Christensen M, Bertilsson L, Ingelman-Sundberg M (2006) Clin Pharmacol Ther 79:103–113
Brosen K (2004) Therapie 59:5–12
Bertilsson L (2007) Clin Pharmacol Ther 82:606–609
Nielsen KK, Brosen K, Hansen MG, Gram LF (1994) Clin Pharmacol Ther 55:518–527
Rudberg I, Mohebi B, Hermann M, Refsum H, Molden E (2008) Clin Pharmacol Ther 83:322–327
Steimer W, Zopf K, von AS, Pfeiffer H, Bachofer J, Popp J, Messner B, Kissling W, Leucht S (2005) Clin Chem 51:376–385
Furuta T, Shirai N, Takashima M, Xiao F, Hanai H, Sugimura H, Ohashi K, Ishizaki T, Kaneko E (2001) Clin Pharmacol Ther 69:158–168
Schwab M, Schaeffeler E, Klotz U, Treiber G (2004) Clin Pharmacol Ther 76:201–209
Klotz U (2006) Int J Clin Pharmacol Ther 44:297–302
Kawamura M, Ohara S, Koike T, Iijima K, Suzuki H, Kayaba S, Noguchi K, Abe S, Noguchi M, Shimosegawa T (2007) J Gastroenterol Hepatol 22:222–226
Schwab M, Klotz U, Hofmann U, Schaeffeler E, Leodolter A, Malfertheiner P, Treiber G (2005) Clin Pharmacol Ther 78:627–634
Hulot JS, Bura A, Villard E, Azizi M, Remones V, Goyenvalle C, Aiach M, Lechat P, Gaussem P (2006) Blood 108:2244–2247
Brandt JT, Close SL, Iturria SJ, Payne CD, Farid NA, Ernest CS, Lachno DR, Salazar D, Winters KJ (2007) J Thromb Haemost 5:2429–2436
Frere C, Cuisset T, Morange PE, Quilici J, Camoin-Jau L, Saut N, Faille D, Lambert M, Juhan-Vague I, Bonnet JL, Alessi MC (2008) Am J Cardiol 101:1088–1093
Kim K, Park P, Hong S, Park JY (2008) Clin Pharmacol Ther (in press)
Richter T, Murdter TE, Heinkele G, Pleiss J, Tatzel S, Schwab M, Eichelbaum M, Zanger UM (2004) J Pharmacol Exp Ther 308:189–197
Zanger UM, Raimundo S, Eichelbaum M (2004) Naunyn Schmiedebergs Arch Pharmacol 369:23–37
Ingelman-Sundberg M (2005) Pharmacogenomics J 5:6–13
Raimundo S, Toscano C, Klein K, Fischer J, Griese EU, Eichelbaum M, Schwab M, Zanger UM (2004) Clin Pharmacol Ther 76:128–138
Toscano C, Klein K, Blievernicht J, Schaeffeler E, Saussele T, Raimundo S, Eichelbaum M, Schwab M, Zanger UM (2006) Pharmacogenet Genomics 16:755–766
Johansson I, Lundqvist E, Bertilsson L, Dahl ML, Sjoqvist F, Ingelman-Sundberg M (1993) Proc Natl Acad Sci USA 90:11825–11829
Ingelman-Sundberg M (1999) Drug Metab Rev 31:449–459
Zanger UM, Fischer J, Raimundo S, Stuven T, Evert BO, Schwab M, Eichelbaum M (2001) Pharmacogenetics 11:573–585
Schaeffeler E, Schwab M, Eichelbaum M, Zanger UM (2003) Hum Mutat 22:476–485
Fux R, Morike K, Prohmer AM, Delabar U, Schwab M, Schaeffeler E, Lorenz G, Gleiter CH, Eichelbaum M, Kivisto KT (2005) Clin Pharmacol Ther 78:378–387
Morike K, Kivisto K, Schaeffeler E, Jagle C, Igel S, Drescher S, Fux R, Marx C, Hofmann U, Engel C, Wagner F, Delabar U, Meisner C, Bail D, Bohm J, Gleiter C, Ziemer G, Rein J, Hellberg K, Eichelbaum M, Schwab M (2008) Clin Pharmacol Ther 84(1):104–110
Kirchheiner J, Nickchen K, Bauer M, Wong ML, Licinio J, Roots I, Brockmoller J (2004) Mol Psychiatry 9:442–473
Gasche Y, Daali Y, Fathi M, Chiappe A, Cottini S, Dayer P, Desmeules J (2004) N Engl J Med 351:2827–2831
Koren G, Cairns J, Chitayat D, Gaedigk A, Leeder SJ (2006) Lancet 368:704
Kirchheiner J, Schmidt H, Tzvetkov M, Keulen JT, Lotsch J, Roots I, Brockmoller J (2007) Pharmacogenomics J 7:257–265
Dehal SS, Kupfer D (1997) Cancer Res 57:3402–3406
Johnson MD, Zuo H, Lee KH, Trebley JP, Rae JM, Weatherman RV, Desta Z, Flockhart DA, Skaar TC (2004) Breast Cancer Res Treat 85:151–159
Goetz MP, Kamal A, Ames MM (2008) Clin Pharmacol Ther 83:160–166
Borges S, Desta Z, Li L, Skaar TC, Ward BA, Nguyen A, Jin Y, Storniolo AM, Nikoloff DM, Wu L, Hillman G, Hayes DF, Stearns V, Flockhart DA (2006) Clin Pharmacol Ther 80:61–74
Schroth W, Antoniadou L, Fritz P, Schwab M, Muerdter T, Zanger UM, Simon W, Eichelbaum M, Brauch H (2007) J Clin Oncol 25:5187–5193
Liu YT, Hao HP, Liu CX, Wang GJ, Xie HG (2007) Drug Metab Rev 39:699–721
Yamazaki H, Shimada T (1997) Arch Biochem Biophys 346:161–169
Pikuleva IA (2006) Pharmacol Ther 112:761–773
Scott EE, Halpert JR (2005) Trends Biochem Sci 30:5–7
Burk O, Wojnowski L (2004) Naunyn Schmiedebergs Arch Pharmacol 369:105–124
Jover R, Bort R, Gomez-Lechon MJ, Castell JV (2002) FASEB J 16:1799–1801
Wolbold R, Klein K, Burk O, Nussler AK, Neuhaus P, Eichelbaum M, Schwab M, Zanger UM (2003) Hepatology 38:978–988
Waxman DJ, O'Connor C (2006) Mol Endocrinol 20:2613–2629
Schirmer M, Rosenberger A, Klein K, Kulle B, Toliat MR, Nurnberg P, Zanger UM, Wojnowski L (2007) Pharmacogenomics 8:443–453
Ozdemir V, Kalow W, Tang BK, Paterson AD, Walker SE, Endrenyi L, Kashuba AD (2000) Pharmacogenetics 10:373–388
Sata F, Sapone A, Elizondo G, Stocker P, Miller VP, Zheng W, Raunio H, Crespi CL, Gonzalez FJ (2000) Clin Pharmacol Ther 67:48–56
Kuehl P, Zhang J, Lin Y, Lamba J, Assem M, Schuetz J, Watkins PB, Daly A, Wrighton SA, Hall SD, Maurel P, Relling M, Brimer C, Yasuda K, Venkataramanan R, Strom S, Thummel K, Boguski MS, Schuetz E (2001) Nat Genet 27:383–391
Schirmer M, Toliat MR, Haberl M, Suk A, Kamdem LK, Klein K, Brockmoller J, Nurnberg P, Zanger UM, Wojnowski L (2006) Pharmacogenet Genomics 16:59–71
Westlind A, Lofberg L, Tindberg N, Andersson TB, Ingelman-Sundberg M (1999) Biochem Biophys Res Commun 259:201–205
Amirimani B, Ning B, Deitz AC, Weber BL, Kadlubar FF, Rebbeck TR (2003) Environ Mol Mutagen 42:299–305
Hustert E, Haberl M, Burk O, Wolbold R, He YQ, Klein K, Nuessler AC, Neuhaus P, Klattig J, Eiselt R, Koch I, Zibat A, Brockmoller J, Halpert JR, Zanger UM, Wojnowski L (2001) Pharmacogenetics 11:773–779
Burk O, Tegude H, Koch I, Hustert E, Wolbold R, Glaeser H, Klein K, Fromm MF, Nuessler AK, Neuhaus P, Zanger UM, Eichelbaum M, Wojnowski L (2002) J Biol Chem 277:24280–24288
Rodriguez-Antona C, Axelson M, Otter C, Rane A, Ingelman-Sundberg M (2005) J Biol Chem 280:28324–28331
Rebbeck TR, Jaffe JM, Walker AH, Wein AJ, Malkowicz SB (1998) J Natl Cancer Inst 90:1225–1229
Felix CA, Walker AH, Lange BJ, Williams TM, Winick NJ, Cheung NK, Lovett BD, Nowell PC, Blair IA, Rebbeck TR (1998) Proc Natl Acad Sci USA 95:13176–13181
Wojnowski L, Hustert E, Klein K, Goldammer M, Haberl M, Kirchheiner J, Koch I, Klattig J, Zanger U, Brockmoller J (2002) J Natl Cancer Inst 94:630–631
Vaarala MH, Mattila H, Ohtonen P, Tammela TL, Paavonen TK, Schleutker J (2008) Int J Cancer 122:2511–2516
Hesselink DA, van Schaik RH, van der Heiden IP, van der WM, Gregoor PJ, Lindemans J, Weimar W, van GT (2003) Clin Pharmacol Ther 74:245–254
Anglicheau D, Legendre C, Beaune P, Thervet E (2007) Pharmacogenomics 8:835–849
Jin Y, Wang YH, Miao J, Li L, Kovacs RJ, Marunde R, Hamman MA, Phillips S, Hilligoss J, Hall SD (2007) Clin Pharmacol Ther 82:579–585
Josephson F, Allqvist A, Janabi M, Sayi J, Aklillu E, Jande M, Mahindi M, Burhenne J, Bottiger Y, Gustafsson LL, Haefeli WE, Bertilsson L (2007) Clin Pharmacol Ther 81:708–712
Lamba J, Strom S, Venkataramanan R, Thummel KE, Lin YS, Liu W, Cheng C, Lamba V, Watkins PB, Schuetz E (2006) Clin Pharmacol Ther 79:325–338
Lamba J, Lamba V, Strom S, Venkataramanan R, Schuetz E (2008) Drug Metab Dispos 36:169–181
Skarke C, Kirchhof A, Geisslinger G, Lotsch J (2005) Eur J Clin Pharmacol 61:887–892
Blievernicht JK, Schaeffeler E, Klein K, Eichelbaum M, Schwab M, Zanger UM (2007) Clin Chem 53:24–33
Jain KK (2005) Mol Diagn 9:119–127
Schwab M, Zanger UM, Marx C, Schaeffeler E, Klein K, Dippon J, Kerb R, Blievernicht J, Fischer J, Hofmann U, Bokemeyer C, Eichelbaum M (2008) J Clin Oncol 26(13):2131–2138
Pozzi S, Rossetti S, Bistulfi G, Sacchi N (2006) Oncogene 25:1400–1407
Tsuchiya Y, Nakajima M, Takagi S, Taniya T, Yokoi T (2006) Cancer Res 66:9090–9098
Oesch-Bartlomowicz B, Oesch F (2002) Biol Chem 383:1587–1592
Rezen T, Contreras JA, Rozman D (2007) Drug Metab Rev 39:389–399
Johnson CD, Balagurunathan Y, Tadesse MG, Falahatpisheh MH, Brun M, Walker MK, Dougherty ER, Ramos KS (2004) Environ Health Perspect 112:403–412
Ekins S, Andreyev S, Ryabov A, Kirillov E, Rakhmatulin EA, Sorokina S, Bugrim A, Nikolskaya T (2006) Drug Metab Dispos 34:495–503
Wienkers LC, Heath TG (2005) Nat Rev Drug Discov 4:825–833
Acknowledgements
Supported by the Robert-Bosch Foundation, Stuttgart, and by the Academy of Finland (to MT).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zanger, U.M., Turpeinen, M., Klein, K. et al. Functional pharmacogenetics/genomics of human cytochromes P450 involved in drug biotransformation. Anal Bioanal Chem 392, 1093–1108 (2008). https://doi.org/10.1007/s00216-008-2291-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-008-2291-6