
Abstract
Rationale
Anhedonia, a deficit in reward processing, is an endophenotype of several neuropsychiatric conditions. Despite its prevalence and debilitating effects, treatments for anhedonia are lacking, primarily because its underlying mechanisms are poorly understood. Dopamine (DA) has been implicated in anhedonia through its role in reward-related learning; glucocorticoid systems may also be involved in that anhedonia is often preceded by chronic stress.
Objective
This study investigated DA and glucocorticoid systems in anhedonia using a rat version of the probabilistic reward task (PRT).
Methods
Adult male Wistar rats were trained on the PRT and then tested following: (1) activation or inhibition of DA activity induced by amphetamine (AMPH) or pramipexole (PRAMI) injections, (2) chronic mild stress (CMS), or (3) glucocorticoid system activation (dexamethasone (DEX)) or inhibition (mifepristone (MIFE)).
Results
AMPH increased and PRAMI decreased response bias, pointing to enhanced and diminished reward responsiveness with DA agonism and antagonism, respectively. CMS reduced response bias but only in a subpopulation of rats. DEX also decreased response bias, suggesting that glucocorticoid processes contribute to anhedonia, although glucocorticoid inhibition (MIFE) had no effect. None of the manipulations altered the ability to detect and respond to reward-paired stimuli.
Conclusions
These results confirm a role of DA in anhedonia and elucidate the contribution of the glucocorticoid system to this effect. In addition, chronic stress may interfere with normal DA functioning, leading to impaired reward-related learning in some animals. These findings may direct future treatment of anhedonia by targeting DA and glucocorticoid systems, as well as a possible interaction between the two.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anhedonia, a loss of pleasure in previously rewarding activities, is a component of several mood and personality disorders, as well as a hallmark symptom of schizophrenia and major depressive disorder (MDD; American Psychiatric Association 2013). Although anhedonia predicts poor treatment responses in depressive patients (Spijker et al. 2001), typical first-line pharmacotherapy for MDD (selective 5-HT reuptake inhibitor (SSRI)) is ineffective in treating this condition (Price et al. 2009). As a result, individuals with anhedonia may be forced to endure their symptoms untreated, leading to greater severity and duration of depressive symptoms (Atherton et al. 2015), and increased suicidality (Winer et al. 2016). The lack of effective treatments for this debilitating condition reflects the fact that the neurobiological underpinnings of anhedonia are poorly understood.
Anhedonia is predominantly characterized by dysfunction in the mesolimbic dopamine (DA) system (Keller et al. 2013), which plays a primary role in motivated behaviors (Wise 1980). These behaviors serve to bring an organism into contact with a goal: either a primary reinforcer (e.g., food or sex) or a conditioned reinforcer which has acquired motivational significance through association with a primary reinforcer (Wit and Dickinson 2009). Goal-directed behaviors depend on effective reward processing in which individuals must recognize the significance of a particular goal and coordinate cognitive and behavioral responses to achieve this goal. If reward processes are impaired (e.g., as seen in anhedonia), goal-directed behaviors could be disrupted.
Reward processing is also modified under conditions of repeated stress (Willner 2005), suggesting that alterations in glucocorticoid mechanisms may contribute to anhedonia. In support of this idea, the hypothalamic-pituitary-adrenal (HPA) axis is hyperactive in MDD patients, leading to hypercortisolemia or a prolonged release of cortisol into the circulatory system (Gillespie and Nemeroff 2005). In this condition, glucocorticoid receptors (GRs) are dysfunctional and no longer provide effective negative feedback to inhibit further glucocorticoid release from the adrenal glands (Pariante and Lightman 2008). The resulting increase in cortisol levels may impact DA system function, thereby altering reward processing. Consistent with this notion, rats that undergo chronic stress show reduced levels of DA in the nucleus accumbens (NAcc) shell (Gambarana et al. 1999), an area critical to the control of behavior by reward-paired cues (Parkinson et al. 1999).
An understanding of reward processing, including anhedonia, has advanced substantially in the last decade with the development of the probabilistic reward task (PRT) (Pizzagalli et al. 2005). In this paradigm, subjects select one of two stimuli to receive a monetary reward when the payoff provided by each stimulus is unknown. Over a series of trials, healthy humans display a response bias to the stimulus yielding a higher probability of reward but have no conscious awareness of the payoffs associated with each response (Pizzagalli et al. 2008; Pizzagalli 2014). Patients with anhedonia fail to develop a response bias: they respond equally to both stimuli, indicative of diminished reward responsiveness (Pizzagalli et al. 2008). A rodent analog of the PRT, designed and implemented by Markou and colleagues, confirmed that response bias increases following administration of the DA agonist, amphetamine (AMPH), and decreases following administration of pramipexole (PRAMI), a D2/D3 receptor agonist that decreases DA at low doses via autoreceptor stimulation (Der-Avakian et al. 2013). Moreover, rats repeatedly exposed to a potent naturalistic stressor (social defeat) exhibited reduced response bias in the PRT (Der-Avakian et al. 2017), supporting the idea that anhedonia may reflect a maladaptive interaction between the DA and glucocorticoid systems (Der-Avakian et al. 2017; Pizzagalli 2014; Vrieze et al. 2013).
The goal of our study was to further examine the role of DA and glucocorticoid systems in anhedonia using the rat-based PRT. Based on previous findings from human and rat studies (Der-Avakian et al. 2013; Pizzagalli et al. 2009; Santesso et al. 2008) and the fact that DA is highly implicated in reward responsiveness, we predicted that AMPH would potentiate response bias and PRAMI would reduce it. We then focused on the glucocorticoid system, hypothesizing that chronic exposure to unpredictable and mildly aversive stimuli (Willner et al. 1987) would reduce response bias in the PRT. We also tested the role of glucocorticoid systems, directly, hypothesizing that response bias would decrease following injections of dexamethasone (DEX), a glucocorticoid agonist that produces chronic activation of the HPA axis (Casarotto and Andreatini 2007), and increase following injections of mifepristone (MIFE), a glucocorticoid antagonist.
Materials and methods
Subjects
One hundred twenty male Wistar rats (Charles River, Quebec), weighing 250–275 g at the start of the experiments, were pair-housed in polycarbonate cages (40.0 × 25.0 × 22.0 cm) on a 12-h reverse light/dark cycle at 21 °C. Behavioral training and testing were conducted during the dark cycle. Water was available ad libitum in the home cage. Beginning 2 days before training, rats were food restricted (16 g/rat daily) for the remainder of the experiment. All experimental procedures were in compliance with the Canadian Council on Animal Care and were approved by the Queen’s University Animal Care Committee.
Apparatus
Behavioral training and testing was conducted using operant chambers (24 × 30 × 29 cm; Med Associates, USA). The chambers were enclosed by two Plexiglass walls and two steel walls which surround a metal grid floor. One of the steel walls contained two retractable levers (6 cm above the floor and 16 cm apart), a food receptacle situated between the two levers, and two stimulus lights (28-V; 4 cm above each lever). The second wall contained a house light (2 cm from ceiling) and a speaker. Chambers were located inside a large wooden enclosure, which ensured darkness and sound insulation. All responses were recorded electronically using MED-PC IV software.
Drugs
Rats were injected with D-amphetamine sulfate (AMPH; Sigma, St. Louis, MO) or pramipexole dihydrocloride (PRAMI; Sigma-Aldrich, USA) at doses of 0.1 mg/kg and 0.5 mg/kg, based on a previous study (Der-Avakian et al. 2013). Mifepristone (MIFE; Sigma-Aldrich, USA) was tested at doses of 15, 30, and 45 mg/kg (Mahoney et al. 2016) and dexamethasone (DEX; Sigma-Aldrich, USA) at a 5 mg/kg dose (Casarotto and Andreatini 2007). All drugs were dissolved in 0.9% physiological saline with the exception of MIFE, which was dissolved in 10% Tween 80 dissolved in saline. Control injections (i.e., 0 dose) were either saline or TWEEN, depending on the drug group. All drugs were administered in a volume of 1 ml/kg and injections were intraperitoneal with the exception of PRAMI, which was administered subcutaneously.
Procedure
Rats were trained and tested in the PRT using a protocol described previously (Der-Avakian et al. 2013). Briefly, all rats underwent five stages of training, as outlined below, and were then tested in one of three experiments.
Training
In stage 1, rats were trained to respond for sucrose pellets on a fixed ratio (FR) 1 schedule of reinforcement using the right or left lever (counterbalanced within groups). When rats received 100 rewards within a 60-min session, the procedure was repeated the next day with the other lever. The average duration of stage 1 training was 3 days.
In stage 2, rats learned to associate a 5 kHz, 60-dB tone of different durations (0.5 s or 2 s) with either the right or left lever (counterbalanced within groups). On each trial (separated by 5–8 s), one lever was extended, the corresponding tone sounded, and rats were reinforced for responding within 5 s. If no response was recorded in this period, the lever was retracted, the house light was illuminated, and an omission was recorded. Following a correct response, the lever retracted and a sucrose pellet was presented. Success was defined as 100 trials in 60 min with 80% success rate (< 20% omissions) for three consecutive days. The average duration of stage 2 training was 5 days.
In stage 3, both levers were extended and rats were reinforced only for responses on the correct lever (e.g., left lever for 0.5-s duration tone). Following an omitted or incorrect response, the previous trial was repeated until a correct response was recorded. Omissions or incorrect responses were signaled by illumination of the house light during the inter-trial interval. This stage of training continued for five sessions, regardless of accuracy.
In stage 4, both levers were extended and the two-tone durations were presented randomly throughout the session. Correct responses were reinforced with a sucrose pellet. Success was defined as 100 trials in 60 min with 70% accuracy (< 30% omissions or incorrect responses) for three consecutive days. The average duration of stage 4 training was 11 days.
In stage 5, the final stage, the house light no longer signaled an omitted or incorrect response. The criterion for completion of stage 5 training was 70% accuracy for five consecutive days. Rats were removed from the experiment if they did not reach this criterion within 15 days from the start of stage 5. The average duration of stage 5 training was 10 days.
Testing
Prior to testing, rats were randomly assigned to either experimental (drug or CMS) or control (SAL or no stress) conditions. During testing, the difference in tone durations was more ambiguous than during training (i.e., 0.9 s and 1.6 s). In addition, one stimulus was reinforced at 60% rate (rich stimulus) and one at 20% rate (lean stimulus) over 100 trials. This matches a 3:1 reinforcement ratio used in the human PRT (Pizzagalli et al. 2008). The assignment of tone duration to rich or lean stimuli was counterbalanced within groups.
Experiment 1: dopaminergic mechanisms in anhedonia
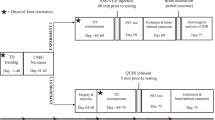
Thirty-six rats were divided into three groups: AMPH (n = 12), PRAMI (n = 12), or SAL (n = 12). To habituate rats to the injection procedure and drug, each animal received a saline injection 4 days prior to testing and a drug injection (AMPH, PRAMI, or SAL according to group assignment) 2 days prior to testing. On test day, AMPH was administered 15 min prior to testing and PRAMI was administered 60 min prior to testing. Half of the SAL group received injections at each time point.
Experiment 2: investigating chronic mild stress in anhedonia
Twenty-four rats were divided into chronic mild stress (CMS; n = 12) or no-stress (n = 12) groups. Following PRT training, all rats were free-fed until the stress regimen ended. The CMS group was transferred to a separate colony room and exposed to a variety of mild stressors, administered randomly over 21 days, following the protocol of Willner (2005) and Rossetti et al. (2016), and detailed in Table 1. In sum, the following stressors were applied each week with only one 10-h “no stress” period every 46 h: one period of food deprivation (12 h), one period of water deprivation (12 h), two periods of continuous overnight illumination (12 h × 2 = 24 h), two periods of 45° cage tilt (24 h × 2 = 48 h), two periods of soiled cage (250 ml of water in bedding; 16 h × 2 = 32 h), and two periods of low-intensity stroboscopic illumination (150 flashes/min) (9 h × 2 = 18 h).
CMS rats were returned to their original colony room at the end of the stress period. Control rats were left undisturbed in the colony room for 21 days, with the exception of bi-weekly cage changes and daily health checks. Body weight was recorded prior to and immediately following CMS treatment, as well as throughout testing. All rats were returned to food restriction starting 2 days prior to retraining sessions. The retraining sessions ensured they maintained 70% accuracy in responding in stage 5 of PRT training. The average duration of retraining was 3 days. All rats achieved sufficient accuracy during these sessions.
Experiment 3: investigating glucocorticoid mechanisms in anhedonia
Sixty rats were divided into five groups: DEX (n = 12), low-dose MIFE (n = 12), medium-dose MIFE (n = 12), high-dose MIFE (n = 12), or SAL (n = 12). Rats in the MIFE groups received habitutation injections as described previously; rats in the DEX group were habituated to the injection procedure using SAL but these animals were not habituated to the drug because DEX produces behavioral alterations for up to 16 days (Casarotto and Andreatini 2007). DEX or SAL (n = 6) was injected 48 h prior to testing; MIFE or TWEEN (n = 6) was injected 45 min prior testing.
Statistical analyses
Using MED-PC IV software, the total number of correct responses, incorrect responses, and omissions were recorded for each test trial. Data from individual rats were excluded from analyses if the animal achieved < 70% accuracy during training or < 30% accuracy during testing. The 100 test trials were statistically analyzed in four separate blocks of 25 trials. Response bias, discriminability, and accuracy were calculated for each block. Response bias reflects increased responding to the rich stimulus, even when the correct action is to respond to the lean stimulus. Response bias was calculated using the formula: log b = 0.5*log[([RichCorrect + 0.5] × [LeanIncorrect + 0.5])/([RichIncorrect + 0.5] × [LeanCorrect + 0.5])]. The formula includes a value of 0.5 added to each cell to adjust for cases where the cell value is zero. Discriminability assesses whether an animal is differentiating rich and lean stimuli and is a measure of task difficulty. Discriminability was calculated using the formula log d = 0.5 × log[([RichCorrect + 0.5] × [LeanCorrect + 0.5])/([RichIncorrect + 0.5] × [LeanIncorrect + 0.5])]. Accuracy is calculated as proportion of correct responses (number of correct responses/number of correct + incorrect responses) for each stimulus (lean and rich).
All measures in experiment 1 were analyzed using planned orthogonal comparisons, based on our prediction from previous work (Der-Avakian et al. 2013), that AMPH would potentiate response bias and PRAMI would attenuate it. We independently compared both drug groups (AMPH and PRAMI) to the SAL group on all three behavioral measures and examined group differences in blocks 1 and 4 to assess changes over time.
All behavioral measures in experiments 2 and 3 were analyzed using mixed model analysis of variance (ANOVA); body weight following CMS was compared across groups using a univariate analysis of covariance (ANCOVA) with pre-CMS body weight as a covariate. Block (1–4) and stimulus type (rich or lean) were included as the within-subject factors and treatment (drug or CMS) as the between-subject factor. All significant two- and three-way interactions were followed up using simple main effects analyses. Levene’s test was used to assess the homogeneity of variance assumption. When the assumption was not met, the appropriate correction was used to adjust the standard error and degrees of freedom of the estimate. The Greenhouse-Geisser correction was used for all within-subject factors to account for violations in sphericity. Statistical significance was defined as p < .05 unless otherwise specified. All pairwise comparisons were analyzed using Tukey’s HSD adjustment for familywise error unless otherwise specified.
Results
Experiment 1: amphetamine enhances reward responsiveness in the PRT
One rat in the SAL group was excluded due to insufficient accuracy (< 70%) during training. All remaining rats achieved sufficient accuracy on both tone stimuli during the test (i.e., > 30%). Thus, N = 35 rats were used in the final analyses. The mean (+ SEM) days to train rats for experiment 1 was 37.77 (± 2.65) days.
Response bias
Planned orthogonal comparisons revealed between-group differences in response bias in block 4, such that response bias in AMPH-treated rats was greater than SAL-treated rats, t(96) = 2.28, p = .03, ηp2 = 0.35. Response bias in PRAMI-treated rats did not significantly differ from SAL-treated controls, t(96) = 1.15, p = 0.26. Furthermore, response bias in AMPH- [t(96) = 2.44, p = .02, ηp2 = 0.33] and SAL- [t(96) = 2.08, p = .05, ηp2 = 0.30] treated rats significantly increased between blocks 1 and 4; however, response bias in PRAMI-treated rats did not change, t(96) = 0.80, p = .43 (Fig. 1a).

Behavioral effects in the probabilistic reward task (PRT) following administration of saline (SAL), amphetamine (AMPH), or pramipexole (PRAMI). a Response bias was blunted in PRAMI-treated rats and potentiated in AMPH-treated rats. b Discriminability did not differ between treatment groups. c Accuracy on the rich stimulus was greater than the lean stimulus in SAL- and AMPH-treated rats, but not in PRAMI-treated rats. *Statistical significance, p < .05. Error bars represent standard error of the mean
Discriminability
There were no between- or within-group differences in discriminability across the four blocks of trials, ts(96) ≤ 1.11, ps ≥ .35 (Fig. 1b).
Accuracy
In block 1, AMPH-treated rats showed significantly greater accuracy on the rich stimulus compared to the lean stimulus, t(96) = 2.36, p = .007, ηp2 = 0.26; however, PRAMI- and SAL-treated rats did not differ in accuracy between the rich and lean stimuli, ts(96) < 0.12, ps > .85 (Fig. 1c). In block 4, both SAL- and AMPH-treated rats showed greater accuracy on the rich stimulus compared to the lean stimulus, ts(96) ≥ 2.47, ps ≤ .02, but accuracy of PRAMI-treated rats did not differ between the two stimuli, t(96) = 1.18, p = .22.
Experiment 2: chronic mild stress impairs reward responsiveness in the PRT
Based on the distributional characteristics of the behavioral data, there were two distinct populations within the CMS group in block 4. Specifically, ~ 60% of the CMS group (n = 7) showed impaired response bias (i.e., response bias below zero) whereas ~ 40% (n = 5) showed normal responding (i.e., response bias above zero). As a comparison, only 2/12 control rats showed a negative response bias. Therefore, we conducted a median split such that CMS rats with a response bias in the lower 50% of the distribution were in the low response bias (LRB) group and rats with a response bias in the upper 50% of the distribution were in the high response bias (HRB) group.
All rats achieved sufficient accuracy during training (> 70%) and sufficient accuracy on both tone stimuli during the test (i.e., > 30%). Thus, N = 24 rats were used in the final analyses. The mean (+ SEM) days to train rats for experiment 2 was 28.42 (± 1.01) days. Following the CMS regimen, rats required 2.92 (± 0.79) days of retraining before final testing and there was no significant difference in this measure across groups, ps ≥ .88 (controls, M = 2.81 days; LRB, M = 2.86 days; HRB 3.01 days).
When controlling for pre-CMS body weight differences, body weight (g) on test day of LRB rats (M = 276.17 ± 7.60) was significantly lower than control rats (M = 290.83 ± 9.60), p = .004, but did not differ from HRB rats (M = 284.17 ± 7.06), p = .20. Body weight of control and HRB rats on the day of testing did not differ significantly, p = .10.
Response bias
A 4 × 3 mixed model ANOVA showed a significant block by group interaction, F(6,63) = 3.53, p = .004, ηp2 = 0.25. Follow-up analyses for the interaction showed a significant simple main effect of group within block 3, F(2,21) = 3.69, p = .04, ηp2 = .26 and block 4, F(2,21) = 8.12, p = .002, ηp2 = 0.44. Pairwise comparisons in block 3 and block 4 indicated that response bias in the LRB group was significantly lower than both the HRB group, ps < .001, and the no stress control group, ps < .005 (Fig. 2a).

Behavioral effects of chronic mild stress (CMS) in the probabilistic reward task (PRT) for rats with a high response bias (HRB), low response bias (LRB), and no stress controls. a Response bias was blunted in the LRB group. The HRB and no stress groups did not differ from each other. b Discriminability did not differ between treatment groups. c Accuracy on the rich stimulus was greater than the lean stimulus in the HRB and no stress groups, but not in the LRB group. *Statistical significance, p < .05. Error bars represent standard error of the mean
Furthermore, follow-up analyses revealed a simple main effect of block within the no stress group, F(3,19) = 3.10, p = .05, ηp2 = 0.33, and the HRB group, F(3,19) = 3.00, p = .04, ηp2 = 0.32. Pairwise comparisons revealed that both the HRB and the no stress control group showed higher response bias in block 4 relative to block 1, ps ≤ .02. In the HRB and no stress groups, response bias in block 3 was significantly higher than block 1, ps ≤ .008, and block 2, ps ≤ .05. Finally, in the HRB group, response bias in block 4 was significantly higher than block 2, p = .02, and block 3, p = .04.
Discriminability
There were no between- or within-group differences in discriminability across the four blocks (all Fs < 0.82, ps > .26) (Fig. 2b).
Accuracy
A 4 × 3 × 2 mixed model ANOVA revealed a significant main effect of stimulus type, F(1,21) = 5.26, p = .03, such that overall accuracy on the rich stimulus was greater than the lean stimulus (Fig. 2c). Furthermore, there was a significant three-way block by group by type interaction, F(6,63) = 3.99, p = .002, ηp2 = 0.28.
Follow-up analyses showed a simple main effect of group within block 4 on the rich stimulus, F(2,21) = 4.19, p = .03, ηp2 = 0.29, and the lean stimulus, F(2,21) = 5.21, p = .02, ηp2 = 0.33. Pairwise comparisons showed that accuracy in block 4 on the rich stimulus in the LRB group was lower than both the HRB group, p = .03, and the no stress group, p = .02. On the other hand, accuracy in block 4 on the lean stimulus in the LRB group was higher than the HRB group, p = .005, and the no stress group, p = .03.
There was also a significant simple main effect in the no stress group, F(1,21) = 11.34, p = .003, ηp2 = 0.35, such that accuracy on the rich stimulus was higher than the lean stimulus. There were significant simple main effects of type within block 4 in all three treatment groups, Fs(1,21) ≥ 5.60, ps ≤ .03, ηp2 ≥ 0.21. Pairwise comparisons showed that accuracy in block 4 on the rich stimulus was greater than the lean stimulus in the HRB and no stress groups; however, accuracy on the rich stimulus in the LRB group was lower than the lean stimulus.
Experiment 3: dexamethasone impairs reward responsiveness in the PRT
All rats achieved sufficient accuracy during training (> 70%) and sufficient accuracy on both tone stimuli during the test (i.e., > 30%). Thus, N = 60 rats were used in the final analyses. The mean (+ SEM) days to train rats for experiment 3 was 26.93 (± 1.51) days.
In order to assess whether there is a dose-response relationship between MIFE and PRT performance, we tested high (45 mg/kg), medium (30 mg/kg), and low (15 mg/kg) doses of the drug in separate groups (n = 12 per group). These groups did not significantly differ from each other on response bias, Fs < 1.09, ps > .35, discriminability, Fs < 1.49, ps > .24, or accuracy, Fs < 2.09, ps > .15 (Rich) and Fs < 2.26, ps > .13 (Lean). Therefore, the three doses were combined into a single group prior to analyses. Similarly, there were no differences on any behavioral measure between TWEEN- and SAL-treated rats [response bias: ts(10) ≤ .51, ps ≥ .30; discriminability: ts(10) ≤ 1.16, ps ≥ .18; accuracy: ts(10) ≤ .67, ps ≥ .12], so these control groups were combined into a single vehicle (VEH) group.
Body weight
Orthogonal planned comparisons revealed that there were no significant group differences in body weight on the day prior to injection day (day 27) or on injection day itself (day 28), ts(462) ≤ 0.87, ps ≥ .39. However, 48 h following their respective injections (day 30), the DEX-treated rats (M = 274.79, SD = 13.56) weighed significantly less than either the MIFE- (M = 291.66, SD = 12.08) or VEH-treated rats (M = 290.36, SD = 5.77), ts(462) ≥ 3.73, ps ≤ .001. These body weight differences were found despite the absence of between-group differences in food intake on days 27 to 30 (data not shown).
Response bias
A 4 × 3 mixed model ANOVA revealed a significant main effect of block, F(3,159) = 8.37, p < .001, and a block by group interaction, F(6,159) = 2.05, p = .05, ηp2 = 0.08 (Fig. 3a).

Behavioral effects in the probabilistic reward task (PRT) following administration of vehicle (VEH), mifepristone (MIFE), or dexamethasone (DEX). a Response bias was blunted in the DEX group only. b Discriminability did not differ between treatment groups. c Accuracy on the rich stimulus was greater than the lean stimulus in VEH- and MIFE-treated rats but not in DEX-treated rats. *Statistical significance, p < .05. Error bars represent standard error of the mean
Follow-up analyses for the interaction showed a significant simple main effect of group in block 3, F(2,53) = 3.24, p = .05, ηp2 = 0.11. Pairwise comparisons revealed that DEX-treated rats showed a lower response bias than VEH-treated rats in block 3 only, p = .02. In blocks 3 and 4, DEX-treated rats showed a lower response bias than MIFE-treated rats that approached statistical significance (both ps = .06).
Follow-up analyses also revealed a significant simple main effect of block within VEH-treated rats, F(3,51) = 5.18, p = .003, ηp2 = 0.23. Pairwise comparisons showed that response bias in block 1 was significantly lower than blocks 3 and 4, ps < .02. Likewise, response bias in block 2 was significantly lower than block 3, p = .004. In MIFE-treated rats, response bias in block 1 was significantly lower than blocks 2, 3, and 4, ps < .01. Likewise, response bias in block 2 was significantly lower than block 4, p = .007.
Discriminability
Mixed model ANOVA did not reveal significant between- or within-group differences in discriminability across the four blocks (all F < 1.64, p > .10) (Fig. 3b).
Accuracy
A 4 × 3 × 2 mixed model ANOVA showed a main effect of stimulus type, F(1,147) = 20.29, p < .001, such that overall accuracy on the rich stimulus was greater than the lean stimulus (Fig. 3c). Furthermore, the type by block interaction was also significant, F(3,147) = 8.60, p < .001, ηp2 = 0.15. There were simple main effects of stimulus type within blocks 2 to 4, Fs(1,147) ≥ 6.87, ps ≤ .01, ηp2 ≥ 0.15, such that accuracy on the rich stimulus was greater than the lean stimulus, collapsed across treatment groups.
There was also a significant three-way block by group by type interaction, F(6,147) = 2.65, p = .02, ηp2 = 0.10. In block 3, accuracy on the rich stimulus in DEX-treated rats was significantly lower than VEH-treated rats, p = .01. Furthermore, there was a significant simple main effect of group within block 1 on the lean stimulus, F(2,49) = 4.63, p = .01, ηp2 = 0.20. Pairwise comparisons revealed that accuracy on the lean stimulus in VEH-treated rats was greater than MIFE-treated rats, p = .02.
Finally, there was a significant simple main effect of stimulus type within blocks 2 to 4 in MIFE-treated rats, Fs(1,49) ≥ 7.80, ps ≤ .01, ηp2 ≥ 0.14, such that accuracy on the rich stimulus was higher than the lean stimulus. Likewise, there was a simple main effect of type within blocks 3 and 4 in VEH-treated rats, Fs(1,49) ≥ 6.52, ps ≤ .01, ηp2 ≥ 0.16, such that accuracy on the rich stimulus was higher than the lean stimulus.
Discussion
Consistent with previous work (Der-Avakian et al. 2013), response bias in the PRT was potentiated by DA agonism and attenuated by DA antagonism. Increases in response bias indicate that subjects are responding for the rich stimulus at higher rates than would be predicted by the reinforcement contingency of that alternative (i.e., 60%). In consequence, accuracy rates for the two stimuli diverge across testing, at least in normal controls. AMPH exacerbates this tendency producing a large discrepancy in correct responses for the two stimuli (see Fig. 1c, block 4). These findings match human experiments in which nicotine, an indirect DA agonist, increases response bias at the expense of accuracy (Barr et al. 2008). In contrast, PRAMI abolished the difference between accuracy on rich and lean stimuli, matching the behavioral pattern of anhedonic patients with MDD (Pizzagalli et al. 2009). Importantly, none of the drugs in our study altered discriminability, confirming that changes in response bias or accuracy cannot be explained by an underlying deficit in the ability to discriminate auditory stimuli.
Our finding that drugs which increase or decrease DA function have corresponding effects on response bias is consistent with a large body of evidence that DAergic mechanisms are critical in reward-related learning (Bardgett et al. 2009; Beninger and Phillips 1980; Wise 1980). We discuss the relationship between behavioral measures of reward (and by extension anhedonia) in a recent review article on animal models of addiction (Lamontagne and Olmstead 2018). Although we did not focus on a specific neural site, the effect we observed in the current study is likely mediated through mesolimbic DA projections to the NAcc: AMPH infusions into the NAcc enhance responding for a reward-paired cue and the effect is eliminated by mesolimbic DA lesions (Taylor and Robbins 1984). Intra-NAcc AMPH infusions also prime cue-triggered reward seeking, such that rats show a 100% increase in lever pressing for a cue previously associated with reward, but not for a neutral cue that was not associated with reward (Wyvell and Berridge 2000). In addition, AMPH-induced increases in responding for a conditioned stimulus are often accompanied by excessive cue-seeking behaviors (e.g., investigatory sniffing), suggesting that activation of mesolimbic DA increases the incentive value of conditioned cues (Berridge and Aldridge 2009).
It is also possible that alterations in response bias following DA manipulations reflect changes in the ability to detect reward prediction errors, or expectations of reward outcome based on reinforcement history (Schultz et al. 1997). This fits with evidence that midbrain DA neurons fire in response to appetitive events that are better than expected (i.e., positive prediction error), including situations that involve an increased probability of reinforcement (Linnet 2014). This increased DA activity, induced pharmacologically or by natural reinforcers, enhances reward-related learning, specifically the ability to detect deviations from previously learned outcomes (Song and Fellous 2014). Finally, elevated DA levels enhance the ability to update decisions based on prior prediction errors (Krugel et al. 2009), which may explain the rapid development of response bias we observed in AMPH-treated rats.
In line with our hypotheses, CMS impaired response bias supporting assertions that repeated and extended exposure to mildly aversive stimuli disrupts motivational and hedonic processing (Rossetti et al. 2016; Willner et al. 1992; Willner 2005). Similar findings using acute exposure to a naturalistic stressor (Der-Avakian et al. 2017) confirm that alterations in reward responsiveness are not restricted to a specific category of aversive stimuli. Given the similarities between effects of CMS and DA antagonism on response bias, it is possible that CMS alters the DAergic system (specifically, by downregulating DA), which produces anhedonic-like behavior. Indeed, adult animals exposed to chronic stress show blunted mesolimbic DA release and reduced DA transporter density in the NAcc (Isovich et al. 2000; Lucas et al. 2004). This suggests that DAergic agonists may alleviate an anhedonic state induced by CMS.
Notably, a subpopulation of CMS rats in our study (~ 40%) displayed normal increases in response bias over testing, matching proportions of animals that do not exhibit decreased sucrose preference following repeated stress (Bisgaard et al. 2007; Gronli et al. 2007; Henningsen et al. 2009; Jayatissa et al. 2010). This apparent resilience to stress is observed in other behavioral domains including memory and sexual behavior (Gronli et al. 2005), as well as depressive-like behavior in the forced swim test and increased submissiveness in the resident-intruder test (Strekalova et al. 2004). Physiological responses display a similar pattern with ~ 37% of CMS-exposed rats not exhibiting the typical decrease in extracellular 5-HT and neuronal density in the prefrontal cortex (Bergström et al. 2007; Gronli et al. 2007). Interestingly, a small but significant proportion of humans maintain stable and healthy levels of psychological and physical functioning in response to highly traumatic events, such as the death of a loved one (Bonanno 2004). Certain circumstances and dispositions, such as low social support or preexisting hyperarousal, could enhance the deleterious effects of chronic stress (Bisson et al. 1997; Bonanno 2004), and individual differences in coping and appraisal may help to explain differences in stress resilience (Strekalova et al. 2004).
The idea that glucocorticoid mechanisms contribute to anhedonia does not fit with our finding that MIFE administration had no effect on response bias. However, MIFE is typically used to reduce abnormally high plasma cortisol levels in individuals with Cushing’s syndrome (i.e., hypercortisolemia) (Heikinheimo et al. 2003), so effects may not be apparent in the absence of a hyperactive stress response. Rats in our study were trained for several weeks in an appetitive operant task under a predictable schedule (e.g., same experimenter and consistent time of day). Under these conditions (i.e., habituation), rats show reduced behavioral and physiological stress responses (Davis 1970; Pitman et al. 1988). Thus, it is possible that baseline glucocorticoid levels in our study were low during testing, minimizing the effects of a glucocorticoid antagonist (i.e., MIFE). This hypothesis could be examined in future studies by measuring plasma corticosterone in animals prior to testing and following drug administration.
An important line of further work is the study of sex differences in anhedonia, particularly as females display increased stress susceptibility (Lighthall et al. 2011; Bourke and Neigh 2011) and higher rates of MDD (Parker et al. 2014). This work will be facilitated and advanced by continued use of the PRT, as this paradigm provides a comprehensive assessment of the multifaceted nature of anhedonia (Slattery and Cryan 2017). More specifically, rather than examining hedonic responsiveness to single rewards (e.g., sucrose preference), the PRT examines the subjects’ ability to integrate reinforcement contingencies as a function of time. The task has also been validated as a translational measure in humans and rodents (Der-Avakian et al. 2013), which allows findings to be interpreted across species with greater confidence. In effect, this will encourage collaboration between neuroscience and clinical researchers to further elucidate the underlying mechanisms of anhedonia, thereby advancing effective and appropriate treatments for this debilitating condition.
References
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, fifth edition, text revision. American Psychiatric Association, Washington, DC
Atherton BD, Nevels RM, Moore MT (2015) Predicting symptoms of depression from social anhedonia and emotion regulation. J Nerv Ment Dis 203(3):170–174
Bardgett ME, Depenbrock M, Downs N, Points M, Green L (2009) Dopamine modulates effort-based decision making in rats. Behav Neurosci 123(2):242–251
Barr RS, Pizzagalli DA, Culhane MA, Goff DC, Evins AE (2008) A single dose of nicotine enhances reward responsiveness in nonsmokers: implications for development of dependence. Biol Psychiatry 63(11):1061–1065
Beninger RJ, Phillips AG (1980) The effect of pimozide on the establishment of conditioned reinforcement. Psychopharmacology 68(2):147–153
Bergström A, Jayatissa MN, Thykjaer T, Wiborg O (2007) Molecular pathways associated with stress resilience and drug resistance in the chronic mild stress rat model of depression: a gene expression study. J Mol Neurosci 33(2):201–215
Berridge KC, Aldridge JW (2009) Decision utility, incentive salience, and cue-triggered “wanting”. Oxf Ser Soc Cogn Soc Neurosci 2009:509
Bisgaard CF, Jayatissa MN, Enghild JJ, Sanchéz C, Artemychyn R, Wiborg O (2007) Proteomic investigation of the ventral rat hippocampus links DRP-2 to escitalopram treatment resistance and SNAP to stress resilience in the chronic mild stress model of depression. J Mol Neurosci 32(2):132–144
Bisson JI, Jenkins PL, Alexander J, Bannister C (1997) Randomised controlled trial of psychological debriefing for victims of acute burn trauma. Br J Psychiatry 171(1):78–81
Bonanno GA (2004) Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol 59(1):20–28
Bourke CH, Neigh GN (2011) Behavioral effects of chronic adolescent stress are sustained and sexually dimorphic. Horm Behav 60(1):112–120
Casarotto PC, Andreatini R (2007) Repeated paroxetine treatment reverses anhedonia induced in rats by chronic mild stress or dexamethasone. Eur Neuropsychopharmacol 17:735–742
Davis M (1970) Effects of interstimulus interval length and variability on startle-response habituation in the rat. J Comp Physiol Psychol 72(2):177–192
Der-Avakian A, D'souza MS, Pizzagalli DA, Markou A (2013) Assessment of reward responsiveness in the response bias probabilistic reward task in rats. Transl Psychiatry 3:297
Der-Avakian A, D’Souza MS, Potter DN, Chartoff EH, Carlezon WA, Pizzagalli DA, Markou A (2017) Social defeat disrupts reward learning and potentiates striatal nociceptin/orphanin FQ mRNA in rats. Psychopharmacology 234(9–10):1603–1614
Gambarana C, Masi F, Tagliamonte A, Scheggi S, Ghiglieri O, Graziella De Montis M (1999) A chronic stress that impairs reactivity in rats also decreases dopaminergic transmission in the nucleus accumbens: a microdialysis study. J Neurochem 72(5):2039–2046
Gillespie CF, Nemeroff CB (2005) Hypercortisolemia and depression. Psychosom Med 67:26–28
Gronli J, Murison R, Fiske E, Bjorvatn B, Sorensen E, Portas CM, Ursin R (2005) Effects of chronic mild stress on sexual behavior, locomotor activity and consumption of sucrose and saccharine solutions. Physiol Behav 84(4):571–577
Gronli J, Fiske E, Murison R, Bjorvatn B, Sørensen E, Ursin R, Portas CM (2007) Extracellular levels of serotonin and GABA in the hippocampus after chronic mild stress in rats. A microdialysis study in an animal model of depression. Behav Brain Res 181(1):42–51
Heikinheimo O, Kekkonen R, Lähteenmäki P (2003) The pharmacokinetics of mifepristone in humans reveal insights into differential mechanisms of antiprogestin action. Contraception 68(6):421–426
Henningsen K, Andreasen JT, Bouzinova EV, Jayatissa MN, Jensen MS, Redrobe JP, Wiborg O (2009) Cognitive deficits in the rat chronic mild stress model for depression: relation to anhedonic-like responses. Behav Brain Res 198(1):136–141
Isovich E, Mijnster MJ, Flügge G, Fuchs E (2000) Chronic psychosocial stress reduces the density of dopamine transporters. Eur J Neurosci 12(3):1071–1078
Jayatissa MN, Henningsen K, Nikolajsen G, West MJ, Wiborg O (2010) A reduced number of hippocampal granule cells does not associate with an anhedonia-like phenotype in a rat chronic mild stress model of depression. Stress 13(2):95–105
Keller J, Young CB, Kelley E, Prater K, Levitin DJ, Menon V (2013) Trait anhedonia is associated with reduced reactivity and connectivity of mesolimbic and paralimbic reward pathways. J Psychiatr Res 47(10):1319–1328
Krugel LK, Biele G, Mohr PN, Li SC, Heekeren HR (2009) Genetic variation in dopaminergic neuromodulation influences the ability to rapidly and flexibly adapt decisions. Proc Natl Acad Sci U S A 106(42):17951–17956
Lamontagne SJ, Olmstead MC (2018) Animal models in addiction research: a dimensional approach. Neurosci Biobehav Rev (in press)
Lighthall NR, Sakaki M, Vasunilashorn S, Nga L, Somayajula S, Chen EY, Mather M (2011) Gender differences in reward-related decision processing under stress. Soc Cogn Affect Neurosci 26:42
Linnet J (2014) Neurobiological underpinnings of reward anticipation and outcome evaluation in gambling disorder. Front Behav Neurosci 8:544
Lucas LR, Celen Z, Tamashiro KLK, Blanchard RJ, Blanchard DC, Markham C, McEwen BS (2004) Repeated exposure to social stress has long-term effects on indirect markers of dopaminergic activity in brain regions associated with motivated behavior. Neuroscience 124(2):449–457
Mahoney MK, Barnes JH, Wiercigroch D, Olmstead MC (2016) Pharmacological investigations of a yohimbine–impulsivity interaction in rats. Behav Pharmacol 27(7):585–595
Pariante CM, Lightman SL (2008) The HPA axis in major depression: classical theories and new developments. Trends Neurosci 31(9):464–468
Parker G, Fletcher K, Paterson A, Anderson J, Hong M (2014) Gender differences in depression severity and symptoms across depressive sub-types. J Affect Disord 167:351–357
Parkinson JA, Olmstead MC, Burns LH, Robbins TW, Everitt BJ (1999) Dissociation in effects of lesions of the nucleus accumbens core and shell on appetitive pavlovian approach behavior and the potentiation of conditioned reinforcement and locomotor activity by-amphetamine. J Neurosci Nurs 19(6):2401–2411
Pitman DL, Ottenweller JE, Natelson BH (1988) Plasma corticosterone levels during repeated presentation of two intensities of restraint stress: chronic stress and habituation. Physiol Behav 43(1):47–55
Pizzagalli DA (2014) Depression, stress, and anhedonia: toward a synthesis and integrated model. Annu Rev Clin Psychol 10:393–423
Pizzagalli DA, Jahn AL, O’Shea JP (2005) Toward an objective characterization of an anhedonic phenotype: a signal-detection approach. Biol Psychiatry 57(4):319–327
Pizzagalli DA, Iosifescu D, Hallett LA, Ratner KG, Fava M (2008) Reduced hedonic capacity in major depressive disorder: evidence from a probabilistic reward task. J Psychiatr Res 43(1):76–87
Pizzagalli DA, Holmes AJ, Dillon DG, Goetz EL, Birk JL, Bogdan R (2009) Reduced caudate and nucleus accumbens response to rewards in unmedicated individuals with major depressive disorder. Am J Psychiatry 166:702–710
Price J, Cole V, Goodwin GM (2009) Emotional side-effects of selective serotonin reuptake inhibitors: qualitative study. Br J Psychiatry 195(3):211–217
Rossetti AC, Papp M, Gruca P, Paladini MS, Racagni G, Riva MA, Molteni R (2016) Stress-induced anhedonia is associated with the activation of the inflammatory system in the rat brain: restorative effect of pharmacological intervention. Pharmacol Res 103:1–12
Santesso DL, Dillon DG, Birk JL, Holmes AJ, Goetz E, Bogdan R (2008) Individual differences in reinforcement learning. Neuroimage 42:807–816
Schultz W, Dayan P, Montague PR (1997) A neural substrate of prediction and reward. Science 275(5306):1593–1599
Slattery DA, Cryan JF (2017) Modelling depression in animals: at the interface of reward and stress pathways. Psychopharmacology 234(9–10):1451–1465
Song MR, Fellous JM (2014) Value learning and arousal in the extinction of probabilistic rewards: the role of dopamine in a modified temporal difference model. PLoS One 9(2):489–494
Spijker J, Bijl RV, de Graaf R, Nolan WA (2001) Determinants of poor 1-year outcome of DSM-III-R major depression in the general population: results of the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Acta Psychiatr Scand 103(2):122–130
Strekalova T, Spanagel R, Bartsch D, Henn FA, Gass P (2004) Stress-induced anhedonia in mice is associated with deficits in forced swimming and exploration. Neuropsychopharmacology 29(11):2007–2017
Taylor JR, Robbins TW (1984) Enhanced behavioural control by conditioned reinforcers following microinjections of d-amphetamine into the nucleus accumbens. Psychopharmacology 84(3):405–412
Vrieze E, Ceccarini J, Pizzagalli DA, Bormans G, Vandenbulcke M, Demyttenaere K (2013) Measuring extrastriatal dopamine release during a reward learning task. Hum Brain Mapp 34:575–586
Willner P (2005) Chronic mild stress (CMS) revisited: consistency and behavioural neurobiological concordance in the effects of CMS. Neuropsychobiology 52(2):90–110
Willner P, Towell A, Sampson D, Sophokleous S, Muscat R (1987) Reduction of sucrose preference by chronic unpredictable mild stress, and its restoration by a tricyclic antidepressant. Psychopharmacology 93(3):358–364
Willner P, Muscat R, Papp M (1992) Chronic mild stress-induced anhedonia: a realistic animal model of depression. Neurosci Biobehav Rev 16:525–534
Winer ES, Drapeau CW, Veilleux JC, Nadorff MR (2016) The association between anhedonia, suicidal ideation, and suicide attempts in a large student sample. Arch Suicide Res 20(2):265–272
Wise RA (1980) Action of drugs of abuse on brain reward systems. Pharmacol Biochem Behav 13:213–223
Wit S, Dickinson A (2009) Associative theories of goal-directed behaviour: a case for animal–human translational models. Psychol Res 73(4):463–476
Wyvell CL, Berridge KC (2000) Intra-accumbens amphetamine increases the conditioned incentive salience of sucrose reward: enhancement of reward “wanting” without enhanced “liking” or response reinforcement. J Neurosci Nurs 20(21):8122–8130
Acknowledgements
This work was supported by operating grants from the Canadian Institutes of Health Research (CIHR) and the Natural Sciences and Engineering Research Council of Canada (NSERC) to MCO, and by an NSERC Alexander Graham Bell Graduate Scholarship to SJL. We thank Dr. Andre Der-Avakian and Amanda Shamblaw for comments on the manuscript, and Lisa Willberforce and Roland Dupras for technical assistance. Queen’s University is situated on traditional Anishinaabe and Haudenosaunee Territory.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Lamontagne, S.J., Melendez, S.I. & Olmstead, M.C. Investigating dopamine and glucocorticoid systems as underlying mechanisms of anhedonia. Psychopharmacology 235, 3103–3113 (2018). https://doi.org/10.1007/s00213-018-5007-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-018-5007-4