
Abstract
Rationale
We examined whether memantine add-on to antipsychotic treatment is beneficial in schizophrenia treatment.
Objective
This systematic review and meta-analysis aimed to achieve stronger evidence on the efficacy and safety of memantine add-on for treating schizophrenia.
Methods
We analyzed double-blind, randomized, placebo-controlled trials of memantine add-on treatment in schizophrenia patients receiving antipsychotics. The primary outcomes were amelioration of negative symptoms and all-cause discontinuation. Dichotomous outcomes are presented as risk ratios (RRs), and continuous outcomes are presented as mean differences (MDs) or standardized mean differences (SMDs).
Results
Eight studies (n = 448) were included. Although memantine add-on treatment was superior to placebo for ameliorating negative symptoms (SMD = −0.96, p = 0.006, I 2 = 88%; N = 7, n = 367) in the Positive and Negative Syndrome Scale general subscale (MD = −1.62, p = 0.002, I 2 = 0%; N = 4, n = 151) and Mini-Mental Status Examination score (MD = −3.07, p < 0.0001, I 2 = 21%; N = 3, n = 83), there were no statistically significant differences in the amelioration of overall (SMD = −0.75, p = 0.06, I 2 = 86%; N = 5, n = 271), positive (SMD = −0.46, p = 0.07, I 2 = 80%; N = 7, n = 367), and depressive symptoms (SMD = −0.127, p = 0.326, I 2 = 0%; N = 4, n = 201); all-cause discontinuation (RR = 1.34, p = 0.31, I 2 = 0%; N = 8, n = 448); and individual adverse events (fatigue, dizziness, headache, nausea, constipation) between the groups. For negative symptoms, the significant heterogeneity disappeared when risperidone studies alone were considered (I 2 = 0%). However, memantine add-on treatment remained superior to placebo (SMD = −1.29, p = 0.00001). Meta-regression analysis showed that patient age was associated with memantine-associated amelioration of negative symptoms (slope = 0.171, p = 0.0206).
Conclusions
Memantine add-on treatment may be beneficial for treating psychopathological symptoms (especially negative symptoms) in schizophrenia patients. The negative-symptom effect size may be associated with younger adult schizophrenia patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Schizophrenia symptoms are characterized by positive, negative, cognitive, and affective symptoms (van Os and Kapur 2009). Although antipsychotics (most of which are dopamine antagonists) have beneficial effects on positive symptoms in typical schizophrenia patients, antipsychotics are less effective for negative symptoms or cognitive dysfunction (Miyamoto et al. 2012). Thus, research is needed to examine whether therapeutic targets other than dopamine receptors exist, for treating negative symptoms as well as cognitive decline.
Multiple lines of evidence from animal, genetic, and postmortem studies suggest that glutamate receptor [e.g., the N-methyl-d-aspartate (NMDA) receptor] hypofunction in the brain (particularly in the thalamus) may be associated with negative symptoms in schizophrenia patients (Beck et al. 2016; Gray and Roth 2007; Hoflich et al. 2015; Kondziella et al. 2006; Miyamoto et al. 2012; Vukadinovic 2014). NMDA-mediated neuronal cell death may play a role in the pathology of schizophrenia (Lakhan et al. 2013). Some studies reported that NMDA receptor modulators, such as glycine, d-serine, and sarcosine, a nonselective glycine reuptake inhibitor used as an adjunctive therapy in antipsychotic-treated schizophrenia, showed amelioration of negative symptoms (Hashimoto 2014). Memantine is postulated to exert its therapeutic effect through its action as a low-to-moderate affinity noncompetitive (open channel), nonselective, voltage-dependent, NMDA receptor antagonist, which binds preferentially to NMDA receptor-operated calcium channels (Berman et al. 2012; Kishi and Iwata 2013). Memantine has been approved worldwide for treating moderate to severe Alzheimer’s disease. Memantine blocks the effects of sustained, pathologically elevated levels of glutamate that may otherwise lead to neuronal dysfunction (Danysz and Parsons 2003; Di Iorio et al. 2017; Sani et al. 2012). Memantine may also upregulate NMDA receptor expression, causing activation in the presence of a strong stimulus (Joshi et al. 2007). From the above studies, memantine add-on to antipsychotic treatment may have a benefit for treating cognitive impairment and negative symptoms in schizophrenia patients (Di Iorio et al. 2017; Sani et al. 2012). Our previous meta-analysis showed that memantine add-on to antipsychotic treatment in schizophrenia showed a trend toward superior efficacy for ameliorating overall symptoms [standardized mean difference (SMD) = −0.99, 95% confidence intervals (95% CIs) = −2.04, 0.06, p = 0.06] and negative symptoms (SMD = −1.08, 95% CI = −2.21, 0.04, p = 0.06) over placebo (Matsuda et al. 2013). However, because the numbers of patients and studies included were small (four studies including 222 patients) (Matsuda et al. 2013), we considered our inability to accurately estimate the efficacy and safety of memantine add-on treatment because of a low statistical power (i.e., insufficient sample size) as a limitation of our previous meta-analysis (Folstein et al. 1975). Four double-blind, randomized, placebo-controlled trials of memantine add-on treatment in schizophrenia were published recently (Fakhri et al. 2016; Mazinani et al. 2017; Omranifard et al. 2015; Veerman et al. 2016). Because a meta-analysis can increase the statistical power for group comparisons and can overcome the limitation of sample size in underpowered studies (Higgins and Green 2011), we hypothesized that the meta-analysis updated with the four new studies could establish superiority of memantine add-on to antipsychotic treatment over placebo for ameliorating negative symptoms in schizophrenia. Therefore, we conducted an updated systematic review and meta-analysis to achieve more robust evidence regarding the efficacy for psychopathology (particularly negative symptoms) of memantine add-on to antipsychotic treatment in schizophrenia patients (eight studies, total of 448 patients).
Methods
This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Moher et al. 2009) (PRISMA 2009 checklist). The review has been registered with PROSPERO (http://www.crd.york.ac.uk/PROSPERO/. CRD42017058749).
Search strategy and inclusion criteria
To identify relevant studies, two of the authors (T.K. and Y.M.) independently searched MEDLINE, Cochrane library, and PsycINFO without language restrictions from the inception of their databases to March 14, 2017, using the following search strategy: memantine and schizophrenia. The authors also searched the Cochrane Central Register of Controlled Trials and clinical trial registries (http://clinicaltrials.gov/) to include randomized controlled trials as comprehensively as possible and to minimize the possibility of publication bias. Only double-blind, randomized, placebo-controlled trials of memantine add-on to antipsychotic treatment in schizophrenia patients lasting ≥2 weeks were included. Studies with a crossover design were allowed in this systematic review and meta-analysis. The same two authors independently assessed inclusion/exclusion criteria and selected the studies. The references of the included articles and review articles were also searched for citations of additional relevant published and unpublished studies, including conference abstracts.
Data synthesis and outcome measures
Our primary outcome measure for efficacy was the amelioration of negative symptoms, according to the Positive and Negative Syndrome Scale (PANSS) negative subscale (Kay et al. 1989) score and the Brief Psychiatric Rating Scale (BPRS) negative subscale (Overall and Gorham 1962) score. The secondary outcome measures for efficacy included improvements in overall scores (PANSS, BPRS), positive symptoms (PANSS, BPRS), PANSS general subscale score, depressive symptoms [Hamilton Rating Scale for Depression (Hamilton 1960), the Calgary Depression Scale for schizophrenia (Addington et al. 1990)], the Clinical Global Impression Severity Score (Guy and Bonato 1970), and the Mini-Mental Status Examination (MMSE) (Folstein et al. 1983) score as well as discontinuation due to inefficacy. Our primary outcome measure for safety was all-cause discontinuation. Secondary outcome measures for safety included discontinuation due to adverse events and the incidence of individual adverse events.
Data extraction
Two authors (T.K. and S.M.) independently extracted data from the included studies. Where possible, we used intention-to-treat (ITT) or modified ITT analysis. When such data were unavailable, the results for observed case (OC) analysis were extracted from each study. When the data required for meta-analysis were missing, we contacted the investigators of the relevant study and requested unpublished data.
Meta-analysis methods
The meta-analysis was conducted using Review Manager software (version 5.3 for Windows, Cochrane Collaboration, http://tech.cochrane.org/revman). The random effects model was selected for this meta-analysis because of the potential heterogeneity across studies. Dichotomous outcomes were presented as risk ratios (RRs) with 95% CIs. Continuous outcomes were analyzed using the mean difference (MD) or, when different studies used different scales, the SMD. Because lower numbers are worse for the MMSE scores in the meta-analytic program Review Manager (see below), we reversed the algebraic sign of the outcomes when higher numbers were negative (i.e., for MMSE scores). We assessed the methodological quality of the trials, according to the Cochrane risk-of-bias criteria in the Cochrane Handbook (version 5.1.0. Cochrane Collaboration, http://handbook.cochrane.org/front_page.htm). We also investigated study heterogeneity using the I 2 statistic, considering I 2 ≥50% to reflect considerable heterogeneity (Higgins et al. 2003). When considerable heterogeneity was observed in overall, positive, and negative symptoms, we performed sensitivity analyses for the following: scales (BPRS vs. PANSS), geographical region (Asia vs. other regions), second-generation antipsychotic (SGA) studies vs. first-generation antipsychotic (FGA) studies, clozapine studies vs. other antipsychotic studies, risperidone studies vs. other antipsychotic studies, analyzed population (ITT population vs. OC population), and sponsorship (industry vs. non-industry). In addition, we performed a meta-regression analysis to evaluate the association between the result of meta-analysis on the amelioration of the symptoms (overall, positive, and negative symptoms, PANSS general scores and MMSE scores) and certain modulators (patient age, sample size, study duration, publication year, and percent male using Comprehensive Meta-Analysis software version 2 (Biostat Inc., Englewood, NJ, USA)). Finally, we utilized funnel plots to explore potential publication bias. Egger’s regression test was used to detect publication bias in meta-analyses using the same software.
Results
Study characteristics
Of the 116 results obtained in our literature search, we excluded the following: 10 because they were duplicates, 81 after a review of the abstract or title review, and 17 articles after a review of the full text [13 review articles (de Bartolomeis et al. 2012; Di Iorio et al. 2017; Francis 2009; Kavirajan 2009; Kishi and Iwata 2013; Koch et al. 2005; Koola et al. 2014; Matsuda et al. 2013; Sani et al. 2012; Shim and Nadeem 2014; Stys and Lipton 2007; Veerman et al. 2014; Zdanys and Tampi 2008), one single-arm study (Veerman et al. 2017), one nonrandomized trial (Cerullo et al. 2007), and two short-duration studies (Bhakta et al. 2016; Swerdlow et al. 2016)]. We did not retrieve any studies by searching through the review articles (Fig. 1). In total, eight trials including 448 patients (study details in Table 1) (de Lucena et al. 2009; Fakhri et al. 2016; Lee et al. 2012; Lieberman et al. 2009; Mazinani et al. 2017; Omranifard et al. 2015; Rezaei et al. 2013; Veerman et al. 2016) were included in the meta-analysis. The mean duration of the studies was 10.25 weeks (range = 6–12 weeks), and the mean patient age was 38.6 years. All studies were double-blind, randomized, placebo-controlled trials, and all were published in English. There were no studies with a crossover design. All included patients in this study received memantine add-on vs. placebo to ongoing antipsychotic treatment. Two of the eight studies were clozapine studies (de Lucena et al. 2009; Veerman et al. 2016), two were risperidone studies (Mazinani et al. 2017; Rezaei et al. 2013), two were studies on various SGAs (Lieberman et al. 2009; Omranifard et al. 2015), one was an olanzapine study (Fakhri et al. 2016), and one study involved various FGAs (Lee et al. 2012). The dose of memantine was 20 mg/day in all studies. Four of the eight studies were conducted in Iran (Fakhri et al. 2016; Mazinani et al. 2017; Omranifard et al. 2015; Rezaei et al. 2013). Although two studies used OC populations in their analyses (Mazinani et al. 2017; Omranifard et al. 2015), we included these data in our meta-analysis to increase the sample size as much as possible. There were two studies that did not report the primary outcome of our study (Fakhri et al. 2016; Omranifard et al. 2015). Data from Omranifard et al. 2015 was used only for the following outcomes: discontinuation rate and individual adverse events (Omranifard et al. 2015). One of the eight studies was sponsored by a pharmaceutical company (Lieberman et al. 2009). Evaluations regarding the methodological quality of the included studies were performed according to the Cochrane risk-of-bias criteria and are shown in Supplementary Fig. 1.

Flowchart of literature review process
Results of the meta-analysis
Efficacy outcomes
Memantine add-on treatment was superior to placebo for ameliorating negative symptoms (SMD = −0.96, 95% CIs = −1.64 to −0.27, p = 0.006, I 2 = 88%; N = 7, n = 367; Fig. 2a), PANSS general subscale score (MD = −1.62, 95% CIs = −2.65 to −0.59, p = 0.002, I 2 = 0%; N = 4, n = 151; Fig. 2b), and MMSE scores (MD = −3.07, 95% CIs = −4.46 to −1.69, p < 0.0001, I 2 = 21%; N = 3, n = 83; Fig. 2c; Table 2). Although memantine add-on treatment showed a trend toward superiority over placebo for ameliorating overall (SMD = −0.75, 95% CIs = −1.52 to 0.03, p = 0.06, I 2 = 86%; N = 5, n = 271) and positive symptoms (SMD = −0.46, 95% CIs = −0.96 to 0.05, p = 0.07, I 2 = 80%; N = 7, n = 367), there were no statistically significant differences in depressive symptoms or CGI-S scores between the treatment groups (Table 2). The data in each treatment group were simulated with no publication bias (Egger’s test p values; overall symptoms = 0.163, positive symptoms = 0.298, negative symptoms = 0.0713).

The forest plots. MMSE Mini-Mental Status Examination, PANSS Positive and Negative Syndrome Scale
Sensitivity analysis on efficacy outcomes
Results of sensitivity analyses are shown in Table 3. Significant heterogeneities remained in all sensitivity analyses of overall symptoms. For positive symptoms, the significant heterogeneity disappeared when performing a sensitivity analysis using data from the risperidone studies alone (I 2 = 0%). Memantine add-on treatment was no more efficacious than placebo in these studies. For negative symptoms, the significant heterogeneity disappeared only when performing a sensitivity analysis using data from risperidone studies alone (I 2 = 0%). However, the superiority of memantine add-on treatment over placebo remained (SMD = −1.29, 95% CIs = −1.79 to −0.79, p = 0.00001; N = 2, n = 76) for negative symptoms.
Meta-regression analysis on efficacy outcomes
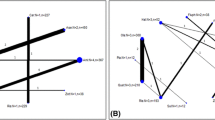
A meta-regression analysis showed that the effect size of memantine with respect to negative (slope = 0.171, 95% CIs = 0.0262–0.315, p = 0.0206; N = 7, n = 367; Fig. 3a) and overall symptoms (slope = 0.171, 95% CIs = 0.09835–0.324, p = 0.0206; N = 5, n = 271; Fig. 3b) increased in schizophrenia patients who were younger adults (Table 4).

The meta-regression analysis
Safety outcomes
There were no statistically significant differences in all-cause discontinuation (RR = 1.34, 95% CIs = 0.76–2.37, p = 0.31, I 2 = 0%; N = 8, n = 448; Fig. 2d), discontinuation due to adverse events, or the incidence of individual adverse events (fatigue, dizziness, headache, nausea, constipation) between the groups (Table 2). The data for all-cause discontinuation in each treatment group were simulated with no publication bias (Egger’s test p value = 0.707).
Discussion
This is an updated systematic review and meta-analysis of memantine add-on treatment to antipsychotic-treated schizophrenia patients. Memantine add-on to antipsychotic treatment was well tolerated, with no significant differences in any safety outcomes between the memantine add-on and placebo groups. Moreover, memantine add-on was more efficacious than placebo for ameliorating negative symptoms (effect size was reasonably large), PANSS general subscale score (effect size was small), and MMSE scores (effect size was reasonably large). Memantine add-on treatment also tended to be superior to placebo for ameliorating overall and positive symptoms. However, we detected significant heterogeneities in overall, positive, and negative symptoms. Sensitivity analyses (e.g., methodological quality: analyzed population and sponsorship) to detect confounding factors for the meta-analyses of these outcomes did not reveal any apparent explanation for the significant heterogeneity for ameliorating overall symptoms. However, the significant heterogeneity for the amelioration of positive and negative symptoms disappeared when sensitivity analyses were performed on risperidone studies alone. Because some medications (such as antipsychotics) may interfere with the actions of memantine on NMDA receptors (Di Iorio et al. 2017), pooling various antipsychotic studies may increase the significant heterogeneities in this outcome. Both risperidone studies were also similar to the current study characteristics in that the studies were conducted in Iran, duration of the studies was 4 and 6 weeks, sample size of the studies was 40 and 46 patients, and the studies were not industry sponsored. This risperidone subgroup also showed that the advantages of memantine add-on treatment over placebo remained for negative symptoms. Therefore, we conclude that memantine may have a benefit for negative symptoms in schizophrenia patients treated with risperidone, although the sample size in the risperidone subgroup was small (n = 76). Further studies are required to determine which antipsychotic should be used in association with memantine, because there are differences in the affinities for a variety of neurotransmitter receptor subtypes among the antipsychotics (Kishi et al. 2013). Further, although memantine is approved for use in those with moderate to severe Alzheimer’s disease, it was surprising that the effect size of memantine with respect to overall and negative symptoms increased in schizophrenia patients who were younger adults. However, we did not address multiple comparisons; this significant effect in younger adults may be a false-positive error arising from the number of meta-regression analyses performed (Higgins and Green 2011). However, there was no evidence for an association between the effect size of memantine and age in Alzheimer’s disease patients (Matsunaga et al. 2014, 2015).
There are strong lines of evidence indicating that dysfunction of glutamate receptors, such as NMDA receptors, may explain the pathophysiology of positive, negative, and cognitive symptoms of schizophrenia (Beck et al. 2016; Gray and Roth 2007; Hoflich et al. 2015; Kondziella et al. 2006; Miyamoto et al. 2012; Vukadinovic 2014). Our meta-analysis showed that memantine add-on was superior to placebo for the amelioration of negative symptoms, PANSS general subscale score, and MMSE scores. However, some phase III trials of other drugs (e.g., bitopertin and LY2140023) which are associated with the glutamate receptor hypofunction hypothesis for schizophrenia failed to significantly decrease schizophrenia symptoms compared to placebo (Beck et al. 2016). The discrepancy in the results may be explained by the following discussion: (1) the superiority of memantine add-on treatment over placebo in our meta-analysis may be influenced by a small study effect (Moreno et al. 2009). There was only one double-blind, placebo-controlled trial of memantine add-on treatment which was similar to the phase III trials of bitopertin and LY2140023; i.e., the memantine study included 138 schizophrenia patients and was conducted with industry sponsorship (Lieberman et al. 2009). This study showed that memantine add-on was not superior to placebo for ameliorating schizophrenia symptoms (Lieberman et al. 2009). (2) There were differences in those drugs’ profiles which may have influenced the results of our meta-analysis, because those drugs generally have affinities for a variety of neurotransmitter receptor subtypes, including glutamate, serotonin, dopamine, nicotinic, and acetylcholine receptors. Memantine is an antagonist for various receptors (NMDA receptors, serotonin-3 receptors, and nicotinic acetylcholine receptors, including alpha-7 receptor). Our previous meta-analysis showed that serotonin-3 receptor antagonist add-on to antipsychotics was superior to placebo for ameliorating negative symptoms (Kishi et al. 2014). The hypodopaminergic state in the prefrontal cortex and mesocortical pathways is related to the negative symptoms and cognitive dysfunction (Juckel 2016; Kambeitz et al. 2014). Because memantine is a dopamine D2 receptor agonist (Seeman et al. 2008) as well, memantine may restore the antipsychotic-induced hypodopaminergic state in the prefrontal cortex and mesocortical pathway. (3) There was no evidence from a meta-analysis of other glutamate-related drugs, such as bitopertin. The placebo response of recent clinical trials was large (Beck et al. 2016). Thus, because the effect size between drug and placebo responses was small, it may be difficult for a single trial to estimate the superiority of drugs over placebo on efficacy due to low statistical power (i.e., insufficient sample size) (Beck et al. 2016; Folstein et al. 1975).
Although we analyzed the combined data from studies of memantine and amantadine to obtain greater statistical power in our previous meta-analytic study (Matsuda et al. 2013), we found several differences in the pharmacological profiles of memantine and of amantadine (Shim and Nadeem 2014). Memantine is an antagonist for NMDA receptors, serotonin-3 receptors, and nicotinic acetylcholine receptor, including alpha-7 receptors; in addition, it is a dopamine D2 receptor agonist. On the other hand, amantadine is a weak NMDA receptor antagonist and an alpha-7 nicotinic acetylcholine receptor antagonist with its effects, including the release of dopamine and norepinephrine. This was a serious limitation of our previous study. However, because four additional memantine studies were published since then, we conducted this updated meta-analysis using only data from memantine studies to accurately estimate the efficacy and safety of memantine add-on to antipsychotic treatment.
Our previous meta-analysis showed a significant heterogeneity in overall, positive, and negative symptoms (Matsuda et al. 2013). However, when excluding the de Lucena et al. (2009) study, all significances of heterogeneity disappeared. Only the de Lucena et al. (2009) study used BPRS in the evaluation of psychopathology from all the studies examined. Therefore, the subgroup, excluding the de Lucena et al. (2009) study, was same as the subgroups using only PANSS data (Table 3). When excluding the de Lucena et al. (2009) study (i.e., subgroup using only PANSS data), all significances of heterogeneity remained in this study (Table 3). For MMSE score, when excluding the de Lucena et al. (2009) study, the superiority of memantine add-on over placebo remained (MD = −2.69, 95% CIs = −4.29 to −1.09, p = 0.001, I 2 = 27%; N = 2, n = 62).
This study had several limitations. First, although a greater number of patients were included in the meta-analysis than in the previous meta-analyses, the number of studies and patients remained insufficient (Trikalinos et al. 2004). Therefore, we cannot rule out a “small study effect,” in which smaller studies tend to show larger treatment effects than larger studies (Moreno et al. 2009). Second, patient characteristics differed between the studies examined, including symptom severity, inclusion criteria, race and ethnicity, and study duration. These differences could generate heterogeneity, when combining data for systematic review and meta-analysis. Third, because all studies evaluated had a short trial duration (mean = 10.25 weeks), we could not determine whether memantine add-on to antipsychotic treatment had any long-term effect on schizophrenia symptoms. Fourth, although we utilized a funnel plot to explore potential publication bias, this technique is generally used only when ≥10 studies are included in a meta-analysis and the current study examined only eight studies. Nevertheless, we did not detect any publication bias using Egger’s test (Table 4).
Conclusions
Our results suggest that memantine add-on to antipsychotic treatment demonstrated treatment efficacy for negative symptoms in schizophrenia patients and was well tolerated. The effect size of negative symptoms may be associated with schizophrenia patients who are younger adults. However, due to study limitations, a long-term study of memantine on a larger sample of schizophrenia patients is required.
References
Addington D, Addington J, Schissel B (1990) A depression rating scale for schizophrenics. Schizophr Res 3:247–251
de Bartolomeis A, Sarappa C, Magara S, Iasevoli F (2012) Targeting glutamate system for novel antipsychotic approaches: relevance for residual psychotic symptoms and treatment resistant schizophrenia. Eur J Pharmacol 682:1–11
Beck K, Javitt DC, Howes OD (2016) Targeting glutamate to treat schizophrenia: lessons from recent clinical studies. Psychopharmacology 233:2425–2428
Berman K, Brodaty H, Withall A, Seeher K (2012) Pharmacologic treatment of apathy in dementia. Am J Geriatr Psychiatr: Off J Am Assoc Geriatr Psychiatr 20:104–122
Bhakta SG, Chou HH, Rana B, Talledo JA, Balvaneda B, Gaddis L, Light GA, Swerdlow NR (2016) Effects of acute memantine administration on MATRICS Consensus Cognitive Battery performance in psychosis: testing an experimental medicine strategy. Psychopharmacology 233:2399–2410
Cerullo MA, Adler CM, Strakowski SM, Eliassen JC, Nasrallah HA, Nasrallah AT (2007) Memantine normalizes brain activity in the inferior frontal gyrus: a controlled pilot fMRI study. Schizophr Res 97:294–296
Danysz W, Parsons CG (2003) The NMDA receptor antagonist memantine as a symptomatological and neuroprotective treatment for Alzheimer’s disease: preclinical evidence. Int J Geriatr Psychiatr 18:S23–S32
Di Iorio G, Baroni G, Lorusso M, Montemitro C, Spano MC, di Giannantonio M (2017) Efficacy of memantine in schizophrenic patients: a systematic review. J Amino Acids 2017:7021071
Fakhri A, Pakseresht S, Haghdoost MR, Hekmatkhah N, Torkashvand M, Ghorbanzadeh B (2016) Memantine enhances the effect of olanzapine in patients with schizophrenia: a randomized, placebo-controlled study. Acta Med Iran 54:696–703
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Folstein MF, Robins LN, Helzer JE (1983) The mini-mental state examination. Arch Gen Psychiatry 40:812
Francis PT (2009) Altered glutamate neurotransmission and behaviour in dementia: evidence from studies of memantine. Curr Mol Pharmacol 2:77–82
Gray JA, Roth BL (2007) Molecular targets for treating cognitive dysfunction in schizophrenia. Schizophr Bull 33:1100–1119
Guy W, Bonato RR (1970) Manual for the ECDEU assessment battery, 2nd edn. Chevy Chase, Md, National Institute of Mental Health
Hamilton M (1960) A rating scale for depression. J Neurol Neurosurg Psychiatry 23:56–62
Hashimoto K (2014) Targeting of NMDA receptors in new treatments for schizophrenia. Expert Opin Ther Targets 18:1049–1063
Higgins J, Green S (2011) Cochrane handbook for systematic reviews of interventions version 5.1.0 The Cochrane Collaboration. www.cochrane-handbook.org.
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Hoflich A, Hahn A, Kublbock M, Kranz GS, Vanicek T, Windischberger C, Saria A, Kasper S, Winkler D, Lanzenberger R (2015) Ketamine-induced modulation of the thalamo-cortical network in healthy volunteers as a model for schizophrenia. Int J Neuropsychopharmacol 18.
Joshi I, Yang Y-M, Wang L-Y (2007). Cellular/molecular coincident activation of metabotropic glutamate receptors and NMDA receptors (NMDARs) downregulates perisynaptic/extrasynaptic NMDARs and enhances high-fidelity neurotransmission at the developing calyx of the held synapse. Journal of Neuroscience 27, 9989–9999
Juckel G (2016) Inhibition of the reward system by antipsychotic treatment. Dialogues Clin Neurosci 18:109–114
Kambeitz J, Abi-Dargham A, Kapur S, Howes OD (2014) Alterations in cortical and extrastriatal subcortical dopamine function in schizophrenia: systematic review and meta-analysis of imaging studies. Br J Psychiatry 204:420–429
Kavirajan H (2009) Memantine: a comprehensive review of safety and efficacy. Expert Opin Drug Saf 8:89–109
Kay SR, Opler LA, Lindenmayer JP (1989) The Positive and Negative Syndrome Scale (PANSS): rationale and standardisation. The British journal of psychiatry Supplement: 59–67.
Kishi T, Iwata N (2013) NMDA receptor antagonists interventions in schizophrenia: meta-analysis of randomized, placebo-controlled trials. J Psychiatr Res 47:1143–1149
Kishi T, Matsuda Y, Nakamura H, Iwata N (2013) Blonanserin for schizophrenia: systematic review and meta-analysis of double-blind, randomized, controlled trials. J Psychiatr Res 47:149–154
Kishi T, Mukai T, Matsuda Y, Iwata N (2014) Selective serotonin 3 receptor antagonist treatment for schizophrenia: meta-analysis and systematic review. NeuroMolecular Med 16:61–69
Koch HJ, Uyanik G, Fischer-Barnicol D (2005) Memantine: a therapeutic approach in treating Alzheimer’s and vascular dementia. Current drug targets CNS and neurological disorders 4:499–506
Kondziella D, Brenner E, Eyjolfsson EM, Markinhuhta KR, Carlsson ML, Sonnewald U (2006) Glial-neuronal interactions are impaired in the schizophrenia model of repeated MK801 exposure. Neuropsychopharmacology: Off Publ Am College Neuropsychopharmacol 31:1880–1887
Koola MM, Buchanan RW, Pillai A, Aitchison KJ, Weinberger DR, Aaronson ST, Dickerson FB (2014) Potential role of the combination of galantamine and memantine to improve cognition in schizophrenia. Schizophr Res 157:84–89
Lakhan SE, Caro M, Hadzimichalis N (2013) NMDA receptor activity in neuropsychiatric disorders. Front Psychiatry 4:52
Lee JG, Lee SW, Lee BJ, Park SW, Kim GM, Kim YH (2012) Adjunctive memantine therapy for cognitive impairment in chronic schizophrenia: a placebo-controlled pilot study. Psychiatry investigation 9:166–173
Lieberman JA, Papadakis K, Csernansky J, Litman R, Volavka J, Jia XD, Gage A, Group M-M-S (2009) A randomized, placebo-controlled study of memantine as adjunctive treatment in patients with schizophrenia. Neuropsychopharmacology: Off Publ Am College Neuropsychopharmacol 34:1322–1329
de Lucena D, Fernandes BS, Berk M, Dodd S, Medeiros DW, Pedrini M, Kunz M, Gomes FA, Giglio LF, Lobato MI, Belmonte-de-Abreu PS, Gama CS (2009) Improvement of negative and positive symptoms in treatment-refractory schizophrenia: a double-blind, randomized, placebo-controlled trial with memantine as add-on therapy to clozapine. J Clin Psychiatr 70:1416–1423
Matsuda Y, Kishi T, Iwata N (2013) Efficacy and safety of NMDA receptor antagonists augmentation therapy for schizophrenia: an updated meta-analysis of randomized placebo-controlled trials. J Psychiatr Res 47:2018–2020
Matsunaga S, Kishi T, Iwata N (2014) Combination therapy with cholinesterase inhibitors and memantine for Alzheimer’s disease: a systematic review and meta-analysis. Int J Neuropsychopharmacol 18.
Matsunaga S, Kishi T, Iwata N (2015) Memantine monotherapy for Alzheimer’s disease: a systematic review and meta-analysis. PLoS One 10:e0123289
Mazinani R, Nejati S, Khodaei M (2017) Effects of memantine added to risperidone on the symptoms of schizophrenia: a randomized double-blind, placebo-controlled clinical trial. Psychiatry Res 247:291–295
Miyamoto S, Miyake N, Jarskog LF, Fleischhacker WW, Lieberman JA (2012) Pharmacological treatment of schizophrenia: a critical review of the pharmacology and clinical effects of current and future therapeutic agents. Mol Psychiatry 17:1206–1227
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535
Moreno SG, Sutton AJ, Ades AE, Stanley TD, Abrams KR, Peters JL, Cooper NJ (2009) Assessment of regression-based methods to adjust for publication bias through a comprehensive simulation study. BMC Med Res Methodol 9:2
Omranifard V, Rajabi F, Mohammadian-Sichani M, Maracy M (2015) The effect of add-on memantine on global function and quality of life in schizophrenia: a randomized, double-blind, controlled, clinical trial. Adv Biomed Res 4:211
van Os J, Kapur S (2009) Schizophrenia. Lancet 374:635–645
Overall JE, Gorham DR (1962) The brief psychiatric rating scale. Psychol Rep 10:799–812
Rezaei F, Mohammad-Karimi M, Seddighi S, Modabbernia A, Ashrafi M, Salehi B, Hammidi S, Motasami H, Hajiaghaee R, Tabrizi M, Akhondzadeh S (2013) Memantine add-on to risperidone for treatment of negative symptoms in patients with stable schizophrenia: randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol 33:336–342
Sani G, Serra G, Kotzalidis GD, Romano S, Tamorri SM, Manfredi G, Caloro M, Telesforo CL, Caltagirone SS, Panaccione I, Simonetti A, Demontis F, Serra G, Girardi P (2012) The role of memantine in the treatment of psychiatric disorders other than the dementias: a review of current preclinical and clinical evidence. CNS drugs 26:663–690
Seeman P, Caruso C, Lasaga M (2008) Memantine agonist action at dopamine D2High receptors. Synapse 62:149–153
Shim SS, Nadeem R (2014) Are NMDA receptor antagonists beneficial in the treatment of schizophrenia? J Psychiatr Res 51:19–20
Stys PK, Lipton SA (2007) White matter NMDA receptors: an unexpected new therapeutic target? Trends Pharmacol Sci 28:561–566
Swerdlow NR, Bhakta S, Chou HH, Talledo JA, Balvaneda B, Light GA (2016) Memantine effects on sensorimotor gating and mismatch negativity in patients with chronic psychosis. Neuropsychopharmacology: Off Publ Am College Neuropsychopharmacol 41:419–430
Trikalinos TA, Churchill R, Ferri M, Leucht S, Tuunainen A, Wahlbeck K, Ioannidis JP, project E-P (2004) Effect sizes in cumulative meta-analyses of mental health randomized trials evolved over time. J Clin Epidemiol 57:1124–1130
Veerman SR, Schulte PF, de Haan L (2014) The glutamate hypothesis: a pathogenic pathway from which pharmacological interventions have emerged. Pharmacopsychiatry 47:121–130
Veerman SR, Schulte PF, Smith JD, de Haan L (2016) Memantine augmentation in clozapine-refractory schizophrenia: a randomized, double-blind, placebo-controlled crossover study. Psychol Med 46:1909–1921
Veerman SR, Schulte PF, Deijen JB, de Haan L (2017) Adjunctive memantine in clozapine-treated refractory schizophrenia: an open-label 1-year extension study. Psychol Med 47:363–375
Vukadinovic Z (2014) NMDA receptor hypofunction and the thalamus in schizophrenia. Physiol Behav 131:156–159
Zdanys K, Tampi RR (2008) A systematic review of off-label uses of memantine for psychiatric disorders. Prog Neuro-Psychopharmacol Biol Psychiatry 32:1362–1374
Acknowledgments
We thank Dr. S. R. T. Veerman (Mental Health Service Organization North Holland North, Community Mental Health Division, Flexible Assertive Community Treatment, Alkmaar, The Netherlands) and Dr. David de Lucena (Programa de Pós-Graduação, em Medicina: Psiquiatria, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil) for providing information for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Drs. Kishi, Matsuda, and Iwata declare that they have no direct conflicts of interest relevant to this study. No grant support or other sources of funding were used to conduct this study or prepare this manuscript.
Dr. Kishi has received speaker’s honoraria from Daiichi Sankyo, Dainippon Sumitomo, Eisai, Eli Lilly, Janssen, Otsuka, Meiji, MSD, Tanabe-Mitsubishi (Yoshitomi), and Pfizer, and has a Fujita Health University School of Medicine research grant.
Dr. Matsuda has received speaker’s honoraria from Dainippon Sumitomo, Eisai, Eli Lilly, GlaxoSmithKline, Otsuka, Tanabe-Mitsubishi and Pfizer, and has a Grant-in-Aid for Young Scientists (B).
Dr. Iwata has received speaker’s honoraria from Astellas, Dainippon Sumitomo, Eli Lilly, GlaxoSmithKline, Janssen, Yoshitomi, Otsuka, Meiji, Shionogi, Novartis, and Pfizer, and had research grants from GlaxoSmithKline, Meiji, and Otsuka.
Contributors
Drs. Kishi and Matsuda had complete access to all the data used in the study and take responsibility for the integrity of the data and accuracy of the data analysis. Study concept and design were performed by Dr. Kishi. The manuscript was written by Drs. Kishi, Matsuda, and Iwata. Dr. Iwata supervised the review.
Role of the funding source
None
Electronic supplementary material
Supplementary Figure 1
Risk-of-bias summary (GIF 12 kb)
Rights and permissions
About this article

Cite this article
Kishi, T., Matsuda, Y. & Iwata, N. Memantine add-on to antipsychotic treatment for residual negative and cognitive symptoms of schizophrenia: a meta-analysis. Psychopharmacology 234, 2113–2125 (2017). https://doi.org/10.1007/s00213-017-4616-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-017-4616-7