
Abstract
Background
We investigated anticipatory and consummatory reward processing in cocaine addiction. In addition, we set out to assess whether task-monitoring systems were appropriately recalibrated in light of variable reward schedules. We also examined neural measures of task-monitoring and reward processing as a function of hedonic tone, since anhedonia is a vulnerability marker for addiction that is obviously germane in the context of reward processing.
Method
High-density event-related potentials were recorded while participants performed a speeded response task that systematically varied anticipated probabilities of reward receipt. The paradigm dissociated feedback regarding task success (or failure) from feedback regarding the value of reward (or loss), so that task-monitoring and reward processing could be examined in partial isolation. Twenty-three active cocaine abusers and 23 age-matched healthy controls participated.
Results
Cocaine abusers showed amplified anticipatory responses to reward predictive cues, but crucially, these responses were not as strongly modulated by reward probability as in controls. Cocaine users also showed blunted responses to feedback about task success or failure and did not use this information to update predictions about reward. In turn, they showed clearly blunted responses to reward feedback. In controls and users, measures of anhedonia were associated with reward motivation. In cocaine users, anhedonia was also associated with diminished monitoring and reward feedback responses.
Conclusion
Findings imply that reward anticipation and monitoring deficiencies in addiction are associated with increased responsiveness to reward cues but impaired ability to predict reward in light of task contingencies, compounded by deficits in responding to actual reward outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In non-clinical populations, reward processing and task-monitoring systems operate in an interactive fashion (Sturmer et al. 2011), allowing individuals to evaluate potential reward outcomes and to monitor and adjust ongoing actions to maximize reward (Morie et al. 2014c). In substance abusers, however, the integrity of these systems is impaired and may contribute to the risk-taking behaviors and poor decision-making that typify the actions of this population.
Task monitoring has been shown to be nearly universally impaired in addiction. Current users of cocaine demonstrate problems with registering and responding to their own errors (Franken et al. 2007b; Sokhadze et al. 2008; Morie et al. 2014a) and with controlling their own behaviors (Garavan and Hester 2007; Garavan et al. 2008; Everitt 2014). These monitoring deficits likely contribute to persistent use of addictive substances despite obviously adverse outcomes.
Reward processing is typically investigated by examining the response to reward cues, which is considered the “anticipatory” reward response, and by examining the response to receipt of reward, which is considered the “consummatory” reward response. The enhanced anticipatory reward response of substance abusers to drug cues is well established (see meta-analyses by Chase et al. 2011; Kuhn and Gallinat 2011). However, findings concerning whether cocaine users experience blunted or heightened anticipatory and consummatory reward responses to non-drug rewards have been mixed. Work using a stop task that employed rewarding feedback revealed that cocaine users, both currently using and recently abstinent, show blunted sensitivity to reward and to cues predicting reward, going so far as to appear insensitive to differing reward amounts (Goldstein et al. 2008; Parvaz et al. 2012). Conversely, imaging research has demonstrated enhanced activity in the ventral striatum of cocaine abusers in response to rewarding outcomes (Jia et al. 2011). In addition, electrophysiological research has shown that gambling addicts demonstrate increased reward-related responses in a gambling task (Hewig et al. 2010), and research focusing on the skin conductance response (SCR) has also revealed dramatically larger responses to reward in a gambling task in cocaine users compared to controls (Bechara et al. 2002).
A possible explanation for some of the mixed findings may relate to the fact that reward-seeking behaviors may be driven by the need to alleviate negative affective states. An absence of positive affect, so-called anhedonia, is characterized by blunted subjective enjoyment of everyday situations and inputs. In substance abuse, however, anhedonia may be accompanied by increased anticipatory reward responses toward sources of intense reward, such as drugs of abuse. Cocaine users and thrill seekers demonstrate higher levels of anhedonia than the general population (Erlenmeyer-Kimling et al. 1993; Janiri et al. 2005; Franken et al. 2006), and these anhedonic tendencies may also exist as a vulnerability marker (Dorard et al. 2008). In addition, work in our laboratory has shown that cocaine-abusing individuals scoring high on anhedonia show increased severity of drug use (Morie et al. 2014a). Anhedonia may raise the threshold for subjective enjoyment of received reward while also increasing motivation toward possible rewards. In cocaine abusers, the presence of anhedonia may drive them to alleviate it via reward-seeking behaviors, hence the increased anticipatory response. However, the presence of anhedonia itself may lessen the consummatory reward response.
Anhedonia may contribute to more than just altered processing of reward. While work in our laboratory has demonstrated that anhedonia is not explicitly correlated with cognitive control in cocaine abusers (Morie et al. 2014a), it is possible that task monitoring in the context of reward may be specifically affected. The increased preoccupation with sources of intense reward brought about by the desire to alleviate anhedonia may come at the expense of closely monitoring the outcomes of actions taken to obtain rewards or even go so far as to impair the ability to predict, and update predictions of, future rewards. This may be a contributor to the loss of control over drug use seen in addiction.
The first goal of the current study was to investigate the integrity of cocaine users’ reward-processing and task-monitoring mechanisms, as well as the interaction between these mechanisms, with a focus on current users of cocaine. We employed a cued reward paradigm that required speeded responses, while high-density event-related potentials (ERPs) were recorded. The paradigm allowed for the possibility to win or lose points that translated to real-world value (gift cards). Participants received cues that predicted likelihood of reward. After responding, participants received immediate feedback that informed them if they had responded successfully within an allotted time window, a task that was titrated online to remain difficult to perform. This first instance of feedback gave no information about reward or loss amounts, but only about task success or failure. After a delay, participants then received a second instance of feedback informing them of the actual magnitude of their losses or gains. When performing a task with the goal of receiving a reward, actions taken to receive the reward must be monitored. The outcomes of these actions must also be monitored and information taken into account along the way in order to update reward predictions. This design allowed us to measure reward monitoring capability, while also allowing us to investigate anticipatory and consummatory reward response. This paradigm was previously used to examine the interaction of reward- and task-monitoring processes in a cohort of healthy controls (Morie et al. 2014c), where it was revealed that healthy controls can integrate information about task performance to re-update reward predictions within very quick time frames.
Toward the goal of understanding these processes in cocaine users, the same set of fronto-central ERP components that was examined in Morie et al. (2014c) was examined here for the purposes of group comparisons. For the measures of anticipatory reward and reward motivation, we examined the cue-related negativity (CRN), a negativity that arises 230–250 ms over fronto-central areas after a cue predicting reward (Yu et al. 2011), and the subsequent contingent negative variation, a sustained negativity that arises at approximately 400 ms which is thought to represent task preparation and motivation (Leynes et al. 1998). To examine task-monitoring mechanisms, we focused on the P2, an early positive potential that arises 200–250 ms after feedback about task success or failure and is thought to play a role in cognitive control (Benikos et al. 2013). The subsequent P300 was also examined, which is associated with attention to task (Polich and Kok 1995) and with the processing of reward-related information (Yeung and Sanfey 2004; Wang et al. 2014) and here is thought to represent later processing and updated reward predictions. Finally, to examine consummatory reward responses, we focused on the feedback-related negativity (FRN) after participants received information about reward or loss magnitude. The FRN is a negativity that arises between 200 and 250 ms and has been found to represent reward prediction errors (Baker and Holroyd 2011). The P300 was also examined after receipt of reward, as the P300 has also been implicated in the processing of details about received reward (Sato et al. 2005; Wu and Zhou 2009). It is hoped that pulling apart the reward response into these two stages of processing (reward monitoring and reward receipt) will shed light on these two distinct processes and help to resolve some of the conflicting findings concerning the response to rewards in cocaine abusers.
The second goal of this study was to explore the effect of anhedonia on the anticipatory and consummatory stages of reward processing as well as task monitoring in cocaine users. To this end, we collected information about levels of anhedonia using the Chapman Physical (PAS) and Social (SAS) Anhedonia Scales (Chapman et al. 1976) as well as the Snaith Hamilton Pleasure Scale (SHPS) (Franken et al. 2007a).
The central prediction of this work was that drug abusers would demonstrate increased anticipatory responses to reward cues (associated with increased amplitudes of the CRN and contingent negative variation (CNV)), along with blunted consummatory responses to receipt of salient rewards and losses (associated with decreased amplitudes of the FRN and P300 components in response to reward receipt), and that ERP indices of these responses would correlate with trait anhedonia. It was also hypothesized that task monitoring would be generally impaired in cocaine users when compared to controls (evidenced by decreased amplitudes of the P2 and P300 in response to task feedback) and that a correlation between ERP indices of task monitoring and anhedonia would be present in drug users as they invested more resources in the processing of reward at the expense of monitoring. Finally, it was predicted that cocaine users would fail to update reward prediction based upon task feedback as effectively as controls.
Methods
Participants
Twenty-four (mean age = 39; 7 female) participants with no drug use history were recruited using advertisements on Craigslist and through word of mouth. Twenty-three (mean age = 44; 7 female) current cocaine abusers were recruited using Craigslist (N = 14) and from the Next STEPs programs at Waters Place and Port Morris (N = 9), which are outpatient treatment programs located in wellness centers in the Bronx and affiliated with the Albert Einstein College of Medicine. All potential participants were given the Structured Clinical Interview for the DSM-IV as well as screening questionnaires related to their overall physical and mental health. Exclusion criteria for cocaine users and controls were as follows: (1) any DSM IV, Axis 1 diagnosis (excluding cocaine dependence in cocaine users); (2) head trauma resulting in loss of consciousness for longer than 30 min; (3) presence of any past or current brain pathology; (4) a diagnosis of HIV; and (5) age above 55 years and below 18 years. Because of the high rates of comorbidity of alcohol and drug abuse among the cocaine-using population, cocaine users were not excluded if they reported periodic use of other drugs or alcohol. However, cocaine users were excluded if cocaine was not their primary drug of choice. Years of drug use were recorded during the screening and the Addiction Severity Index (ASI) interview. Controls were excluded if they had any major Axis 1 disorder or alcohol/drug dependence diagnosis, including nicotine dependence, or if any family members had an alcohol/drug dependence diagnosis. Participants were paid for their participation in the form of one $12 gift card per hour of experiment time. All participants also received the same amount of extra money as winnings on the reward task, which was awarded in extra gift cards. All participants signed an informed consent document administered by HIPAA-certified staff. A urine screen was performed on all participants to test for the presence of metabolites related to cocaine, THC, or opiates. Groups did not significantly differ in age, sex, or years of education. All procedures were approved by the Institutional Review Board of the Albert Einstein College of Medicine. The study conformed to the principles outlined in the Declaration of Helsinki.
Clinical measurements
A trained researcher administered the urine screen to cocaine-abusing participants. Two questionnaires were administered in order to obtain a more complete picture of participants’ addiction history and severity level. The Addiction Severity Index (ASI) is a structured interview that addresses medical history, legal history, psychiatric history, family history, and social life, as well as alcohol and drug use (McLellan et al. 1985). The second was the Cocaine Selective Severity Index (CSSA) assessing withdrawal symptoms from cocaine in the previous 24 h, including irritability and anhedonia (Kampman et al. 1998). All participants also filled out the Snaith Hamilton Pleasure Scale (SHPS; Franken et al. 2007a) as well as the Chapman Physical and Social Anhedonia Scales, to obtain state and trait measures of anhedonia (Chapman et al. 1976).
Electrophysiological recording procedures
The recording and stimulus presentation procedures are identical to those used in Morie et al. (2014c), and the reader is referred to that paper for detailed descriptions. In short, participants were seated in a dimly lit, sound-attenuated, electrically shielded room during electrophysiological recordings. Participants completed one mandatory practice block. Twenty experimental blocks were run, each lasting ∼5 min, for a total of 2000 trials (100 trials per block). The task itself took up to 110 min of continuous recording. Participants took 30-s breaks between blocks and were permitted to take longer breaks when needed to reduce fatigue and concentration lapses.
Task design
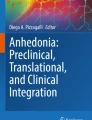
Task design is identical to the task used in Morie et al. (2014c), and is described in detail in that paper and in the supplementary materials. Figure 1 illustrates the order of stimuli and what one succession of trials consisted of for one of four possible conditions.

a Timing of the stimulus presentation in each trial. A cue is presented, followed by a blank screen. During the short duration that the small x is presented, the participant must make a button press. After the response, a tone is played letting them know if they responded in time. After the tone, the actual outcome is displayed. b Succession of events for each of the four possible outcomes. The disc cue informs participants of the probability of being rewarded or penalized depending upon performance. Upon a successful response that falls into the time window within which the small x is presented, they will hear a high-pitched tone informing them and see one of three outcomes: a small win, a large win, or a neutral outcome. Upon a response that does not fall into the time window within which the small x is presented, they will hear a low-pitched tone informing them and then see one of three outcomes: a small loss, a large loss, or a neutral outcome
In brief, participants were informed they would be performing a response time task for which they would receive reward. Four colored discs served as reward cues that would indicate one of four probabilities of receiving reward on that trial, based upon the participant successfully clicking the mouse in response to a target. Table 1 illustrates the probabilities. Participant performance was titrated online at 70 %. After the cue, the target would appear, which required a response within a specified time window that would lengthen or shorten depending on participant’s performance. After the participant responded, they would receive the first instance of feedback, which was a tone informing them of task success or failure. Afterwards, they would then receive the second instance of feedback, which could be one of a set of five potential feedback outcomes (small rewards, large rewards, small losses, large losses, and no change). The probability of receiving neutral feedback as opposed to an actual reward or loss depended on the color of the disc at the beginning of each trial. Participants were rewarded with gift cards for their performance. For a detailed breakdown of the task stimuli, including a breakdown of the performance titration method and reward and loss probabilities and magnitudes associated with the task, the reader is referred to the supplementary materials.
Electrophysiological data recording
Data collection was identical to procedures used in Morie et al. (2014c), and the reader is referred to that paper for a more detailed description. In short, event-related potentials (ERPs) were acquired from a 168-channel montage at a digitization rate of 512 Hz with a pass-band of 0.05–100 Hz using the BioSemi Amplifier System. Data were referenced offline to the average reference. Epochs of 900 ms, including a 100 ms pre-stimulus baseline, were analyzed for both feedback conditions (i.e., the tone indicating task success or failure and the pictorial representation of the task reward/loss), and epochs of 1100 ms, including a 100 ms pre-stimulus baseline, were analyzed for the cue condition (i.e., the colored disc stimuli). Trials with eye movements and blinks were rejected offline based on vertical and horizontal EOG recordings. An automatic artifact rejection criterion of +/− 70 μV was used at all other scalp sites.
Behavioral data analysis
The ASI was scored using the composite scores manual. Student’s t tests were employed to test for between-group differences on anhedonia. Reaction times and accuracy on the reward task were assessed using a repeated measurement analysis of variance (ANOVA) with group as between-subject factor and probability condition as within-subject factor. Correlation coefficients were computed to assess the relationship between ERP components and measures of anhedonia. For the purposes of correlations, conditions were collapsed across probability.
Electrophysiological data analysis
In order to obtain a comprehensive understanding of reward processing and task monitoring in drug abuse, we employed three analyses. The goal of the first analysis was to investigate the effect of drug abuse on reward anticipation and task preparation, and thus, we focused our analysis on the responses associated with the presentation of the colored discs that cued different reward probabilities. The purpose of the second analysis was to investigate task performance feedback and its interaction with reward prediction and how this interaction changed in drug abusers. Thus, we focused the analysis on the responses associated with the presentation of the feedback tone. The purpose of the final analysis was to examine the effect of drug abuse on the response of the reward system to receipt of reward, and thus, we focused this analysis on the responses associated with the feedback stimuli that informed participants of their actual gains or losses. We chose components of interest based upon information from our previous research that has examined reward and task-monitoring mechanisms (Morie et al. 2014c). These components, which were also examined in Morie et al. (2014c), are shown in Table 1, which displays the events in this experiment, the components of interest associated with each one, and the analyses employed for each component.
All statistical analyses were performed on the mean amplitudes of the components within the time frames specified in Table 2. To maintain consistency with our previous ERP study in healthy controls (Morie et al. 2014c) and the extant literature reporting modulations of cue- and reward-related ERP components over fronto-central scalp regions, we extracted an activity averaged across electrodes C1, FCz, and C2 for statistical analysis.
Results
Questionnaire data
As reported previously in Morie et al. (2014a), cocaine users scored significantly higher than controls on both physical (t = 5.4 p < .03) and social (t = 10.2 p < .002) trait measures of anhedonia. The groups also differed significantly on the measure of state anhedonia (t = 2.6 p < .01), where once again, cocaine users demonstrated higher levels of anhedonia. The mean score of the cocaine users on the Cocaine Selective Severity Assessment was 26.30. The ASI composite scores were as follows: medical = .27; employment = .71; legal = .09; alcohol = .14; drug = .22; family history = .24; and psychiatric = .16. For the mean scores of both groups on the anhedonia scales, and the details of the correlation between addiction severity and anhedonia, the reader is referred to Morie et al. (2014a).
Task performance data
There were no differences between groups (F 1,44 = 2.2, p > .5) and cue probability conditions (F 1,44 = 1.3, p > .4) and no group × cue probability interaction (F 1,44 = 1.2, p > .3) for task accuracy, as could be expected since task performance was titrated online for each subject to 70 %. Similarly, no main or interactive effects (group: p > .4; cue probability conditions: p > .4; group × cue probability conditions: p > .3) were found for RT.
ERPs associated with reward anticipation and task preparation
Figure 2 displays the electrophysiological responses after the presentation of the cue for each probability condition for both cocaine users and controls. The CRN and the CNV can be seen, as can the offset response of the 300 ms cue. Our chosen analysis windows did not overlap this offset response.

Electrophysiological responses for the conditions in which the participant heard the tone letting them know they responded in time or not, separate for each probability and each group. The small gray rectangles indicate the time window in which statistical analyses were performed
A repeated measure ANOVA with factors of group and probability was performed on the cue-related negativity (CRN). The RM-ANOVA revealed a main effect of group (F 1, 44 = 5.5, p < .01), along with an interaction of probability and group (F 1, 44 = 5.9 p < .01). Cocaine users displayed more negative-going waveforms than controls, and between-group comparisons revealed group differences in all probability conditions (all p < .01). Pairwise comparisons to follow up the significant interaction revealed significant differences in controls between the very high and very low conditions (t 22 = 2.29, p ≤ .04) and between the very high and low conditions (t 22 = 2.1, p ≤ .05). On the other hand, the probability effect in cocaine users was driven entirely by the difference between the very high and very low probability conditions (t 22 = 3.2, p ≤ .02).
For the subsequent response, the contingent negative variation (CNV), which reflects preparatory behavior, we again found a main effect of group (F 1, 44 = 6.0, p < .01) with an interaction of probability and group (F 1, 44 = 3.1, p < .03). Cocaine users displayed a more negative-going CNV than controls, and once again, between-group comparisons on all probabilities revealed group differences in all probability conditions (all p < .01). Pairwise comparisons in both groups to follow up the significant interaction revealed significant differences in only the controls between the very high and very low conditions (t 22 = 2.31, p ≤ .04) and between the high and very low conditions (t 22 = 2.25, p ≤ .04), where the CNV was more negative in the very high and high conditions. Cocaine users, however, showed no significant dissociation of the CNV across probabilities (all p > .4).
ERPs associated with task monitoring
Figure 3 displays the electrophysiological responses for the condition in which the participant heard the tone letting them know whether they had performed the task successfully or not and displays the activity in the success or failure condition for each probability separately. Two separate between-group analyses were performed on the components that arose as a result of this feedback.

Electrophysiological activity over the scalp for each group, for each probability condition, and each valence condition at specific time points after the instance in which the participant heard the tone letting them know they responded in time or not. The small gray rectangles indicate the time window in which statistical analyses were performed
A 2 × 2 × 4 RM-ANOVA on the feedback P2 revealed a main effect of valence (i.e., whether the tone indicated a win or a loss, F 1, 44 = 8.5, p = .006), a main effect of group (F 1, 44 = 7.1, p < .01), and an interaction of valence and group (F 1, 44 = 5.2, p = .027). There was no effect of probability. The P2 was larger in controls than in cocaine users, with an even larger difference between groups in the loss condition, and the interaction was driven by this effect (p < .05). Post hoc between-group analyses revealed this as well, with between-group t tests revealing that loss conditions were significantly different between groups for all probabilities, with larger P2 amplitudes in controls driving this interaction (all p values <.05) while win conditions were marginally different between groups for all probabilities, with larger P2 amplitudes in controls (p < .09).
Analysis of the later positive component, the P300, revealed a main effect of probability (F 1, 44 = 2.8, p < .05), a main effect of group (F 1, 44 = 6.7 p < .01), an interaction of group and probability (F 1, 44 = 3.8, p < .02), and an interaction of valence and probability (F 1, 44 = 3.7, p < .02). There was no three-way interaction. t tests between groups revealed significant between-group differences for all probability conditions in both wins and loss outcomes (all p values <.05) except for the high condition during a win, which was marginally different between groups (p = .053). Controls demonstrated increased amplitudes of the P300 compared to cocaine users. Follow-up analyses, and our work previously, revealed that controls demonstrated different amplitudes of the P300 depending upon probability (high or low) and context (either a loss or a win). Cocaine users, on the other hand, appeared to be insensitive to probability.
ERPs associated with reward receipt
Figure 4 demonstrates the electrophysiological responses for the condition in which the participant received feedback telling them the actual reward outcome.

Electrophysiological responses for the conditions in which the participants received feedback telling them of actual rewards or losses for each group. Magnitude information in the loss and win outcomes is plotted separately, and the information is collapsed across probability. The small gray rectangles indicate the time window in which statistical analyses were performed
A typical FRN was identified in both cocaine users and controls, peaking between 200 and 250 ms. The effects observed from the between-group RM-ANOVA were a main effect of valence (F 1, 44 = 6.5, p < .02), a main effect of magnitude (F 1, 44 = 7.3 p = .002), a main effect of group (F 1, 44 = 6.6, p = .01), an interaction of valence and group (F 1, 44 = 11.3 p = .002), and an interaction of magnitude and group (F 1, 44 = 4.3, p = .04). There was no effect of probability or any interactions with it. Looking between groups, the main group difference appeared to be driven by smaller amplitudes of the FRN in the addicted group in the case of a reward (p < .04) while the interaction came about due to a lack of a group difference in the case of a large or small loss (p > .5). Examining within groups, controls displayed larger amplitudes of high magnitude wins and losses compared to the no-change outcome (p < .02), smaller amplitudes of low magnitude wins and losses compared to high magnitude wins and losses (p < .02), and larger amplitudes of low magnitude wins and losses compared to the no-change outcome. Cocaine users, however, appeared less sensitive than controls to magnitude of reward. The difference in responses to low magnitude wins and losses was marginally different in cocaine users (p < .05) as were the responses to the large win vs the no-change outcome (p < .05).
A second between-group RM-ANOVA with the same factors was performed on the later positive potential that arose at centro-parietal locations. There was a main effect of magnitude (F 1, 44 = 6.4, p < .01), and while there was no main effect of group or valence, there was a group by valence interaction (F 1, 44 = 4.2, p < .04). As before, there was no effect of probability or any interactions with it (all p values >.3). Looking between groups, cocaine users showed a smaller P300 than controls during reward outcomes (p values <.03) and during the large magnitude loss condition (p < .03), underlying the interaction between valence and group. When examining within groups, in controls, pairwise comparisons of the magnitude factor to follow up the significant finding revealed significant differences between the no-change outcome and the large win/loss outcomes (p ≤ .02), but showed no difference between the small and large win/loss outcomes (p = .32). Cocaine users, however, appeared to be insensitive to any effects of magnitude (p > .1).
Correlations between ERPs and anhedonia
As it is possible that preoccupation with reward, driven by anhedonia, would bias cocaine users toward salient rewards at the expense of resources put toward task monitoring, an important aspect of this research was to investigate the relationship between anhedonia and the response to salient reward as well as anhedonia’s relationship to indices of task monitoring and reward anticipation (Fig. 5).

a Scatter plots illustrating correlations between anhedonia and ERP components of interest in the control group. Correlations were found between anhedonia and the CRN as well as CNV amplitudes. b Scatter plots illustrating significant correlations between anhedonia and ERP components of interest in the cocaine using group. Correlations were found between anhedonia and the CRN, between anhedonia and the P2 in the case of task success, and between anhedonia and the FRN in the case of a reward
In controls, only physical anhedonia correlated with the amplitude of the electrophysiological responses to the cue, correlating negatively with both the CRN (r 44 = −.449, p < .04) and the CNV (r 44 = −.444, p < .04). The correlation was negative, as the CRN and CNV are both negative amplitude components—thus, the more robust the components, the more anhedonic controls were. Social anhedonia did not correlate with any ERP measures.
In cocaine users, however, total trait anhedonia correlated with not only the early electrophysiological response to the cue, the CRN (r 44 = −.53, p < .01), but also to the amplitude of the P2 (r 44 = −.47, p < .03) that arose in response to the tone that let participants know they succeeded. Turning to reward feedback, total trait anhedonia correlated with the FRN (r 44 = .42, p < .04) in response to reward when the participant won. In the case of the P2 and FRN, increased anhedonia was associated with less robust amplitude. However, the ASI score did not correlate with any ERP measures, nor did social anhedonia alone correlate with any ERP measures.
For both groups, there were no correlations found between any ERP measures and scores on the state measure of anhedonia, the SHPS, or between scores on the measure of withdrawal, the Cocaine Selective Severity Index (CSSA). There were no correlations between the CSSA and any measure of trait anhedonia.
Discussion
There were two goals for this work. The first was to examine the integrity of the reward processing and task-monitoring systems, and their interaction, in cocaine abusers. The second was to determine whether levels of anhedonia were associated with a deficit in any of these factors in this population. Our central thesis was that increased anhedonia would lead to a desire to alleviate this negative state, resulting in increased reward anticipation and motivation toward reward along with decreased consummatory reward responses, and that preoccupation with reward would bias cocaine users away from adequately monitoring their own behaviors or updating reward predictions.
Reward anticipation and task preparation
It is well established that substance abusers show increased drive toward drug-related cues (Carter and Tiffany 1999; Kuhn and Gallinat 2011), but it is an open question whether this same increased reward anticipation occurs in response to non-drug-related cues. Here, cocaine users showed more robust cue-related negativities (CRNs) and considerably increased amplitudes of the contingent negative variation (CNV) when presented with stimuli that predicted reward, regardless of the probability that reward would in fact be forthcoming. The group difference between users and controls was striking. This enhanced CNV in cocaine abusers is evidence that cocaine abusers do indeed show increased motivation toward reward, even when that reward is not drug-related. The larger amplitude of the CNV suggests more preparatory behavior as they want the reward more. The points they received went toward gift cards that could only be redeemed at local department stores, and thus, their reward was several steps removed from anything that could be used to purchase drugs. As such, we think it extremely unlikely that the goal to purchase drugs was the reason for the increased motivation observed here.
However, despite neurophysiological responses that suggested increased motivation, cocaine users failed to take into account the information about cued probability and reward likelihood at this stage. If one considers the two extreme cases, the lowest probability cue initiated trials where reward was only to be had on 7 % of trials, whereas the highest probability condition resulted in reward on 63 % of trials, a ninefold differential. Controls showed clear sensitivity to both large and modest probability differences, with significant modulations of the CRN evident between very high and very low and very high and low reward contingencies, in line with previous observations in healthy populations (Yu et al. 2011). In contrast, the CRN in cocaine users was only sensitive to differences between very high and very low probability conditions. More dramatically, there were no detectible probability effects on the preparatory sustained potential that preceded the onset of the task stimulus (i.e., the CNV) in cocaine users, in contrast to the robust systematic effects of probability we saw in controls, the latter findings also consistent with prior findings in healthy populations (Goldstein et al. 2006). Despite their increased motivation to perform the task in order to achieve reward, and an expressed understanding of the different contingencies, cocaine users appeared to be considerably less sensitive to the meaning of the cues as they worked toward reward. The implications of this finding, and indeed any findings that involve differences in the control group that were not then found in the cocaine using group, should take into account the possibility that response variability may have been higher in the clinical group. That said, this may indicate, as hypothesized, a preoccupation with reward at the expense of more directed efforts at accurate reward predictions.
Anhedonia may help explain this preoccupation. Trait physical anhedonia was correlated with ERP activity related to reward motivation, specifically with the CRN in both groups and with the CNV in controls. To our knowledge, this is only the third study to explicitly link anhedonia to reward motivation in healthy controls, and the first to find such a relationship in cocaine users. Trait physical anhedonia was associated with volume of the caudate and with pre-frontal activity during processing of reward information (Harvey et al. 2007). In addition, previous work has identified an effect of increased physical anhedonia in healthy controls on approach behaviors and in their ability to sustain reward predictions when those healthy individuals were grouped into high and low anhedonia groups (Padrao et al. 2012). However, amplitude of the CRN in cocaine users was correlated with anhedonia, suggesting that anhedonia may in fact be associated with increased early processing stages of reward motivation.
Task monitoring and reward interactions
The early response to task feedback was represented by the P2 component, a positive-going potential that arises 200–250 ms after participants receive information about whether or not they have successfully responded within the allotted time window. Controls showed a stronger positivity for both successful and unsuccessful responses, with a larger difference seen between users and controls in the case of unsuccessful responses. This finding likely relates to the difficulties with task monitoring that are commonly observed in cocaine users (Goldstein et al. 2009) and is also consistent with the literature on impairment in monitoring and executive functioning in cocaine users (Li et al. 2006; Sokhadze et al. 2008). The difficulty cocaine users encountered was once again found to be related to anhedonia, as the amplitude of the P2 was negatively correlated with physical anhedonia. It is possible that this relationship came about due to preoccupation with reward at the expense of monitoring.
Similarly, controls also showed more robust P300 amplitudes for both successful and unsuccessful responses. There was no correlation with anhedonia for the P300 for either group. The main finding of interest for this component was the lack of any effect of probability on the amplitude of the P300 for cocaine users. It is apparent that cocaine users failed to update predictions based upon task feedback in the way that controls did. Considering that probability information was not taken into account during the preparatory process, either it is possible that this reflects a complete lack of reward prediction in cocaine users or a failure to re-evaluate predictions based upon new information. This is reflective of the body of work on reversal learning in cocaine addiction. Rats (Schoenbaum et al. 2004), monkeys (Jentsch et al. 2002), and humans (Bechara et al. 2001; Fillmore and Rush 2006) who were administered or used substances have all demonstrated an impaired ability to alter their responding based upon changes in the feedback they received. Further, animal models of stimulant use have demonstrated a failure in these animals to modify behavior in the face of reward devaluation when administered amphetamines (Nelson and Killcross 2006). This work, coupled with the findings presented here, suggests that cocaine use is associated with an impaired ability to use new information to modify expected reward outcomes and may help explain why cocaine users continue to perseverate in their drug use despite increasingly negative consequences.
However, it has been demonstrated that task-monitoring deficits outside the context of reward appear to be normalized in abstinent cocaine users (Bell et al. 2014; Morie et al. 2014b). Future work should investigate the interaction of these processes in abstinent populations to see if that normalization remains in the context of reward.
Reward receipt
Upon receiving feedback of successful reward, controls showed more robust FRNs than cocaine users. Both groups demonstrated sensitivity to reward and loss magnitude in the time window of the FRN. The smaller response in cocaine users to reward outcomes is somewhat surprising considering the enhanced motivation that cocaine users displayed in response to reward cues. However, it becomes clearer when considering the body of work that demonstrates reward dysfunction in addiction along with the association that was observed between FRN amplitude and anhedonia. The more anhedonia an individual indicated via their score on the Chapman Physical Anhedonia Scale, the smaller their FRN was in response to reward. This is different from what was observed in Padrao et al. (2012), who observed intact responses to reward feedback in more anhedonic participants. The obvious difference between their work and the present findings is the difference in samples, with their focus on anhedonia in a non-using healthy population versus our investigation of cocaine users. This implies that anhedonia is indeed associated with a blunted response to salient reward in cocaine addiction. However, this finding was not observed in controls and was not observed in the FRN when the cocaine-using participants received feedback telling them they had lost points. It appears that general anhedonia is associated only with response to salient reward feedback in cocaine use, but not to salient losses. This lends evidence to the proposal that an impaired ability to process rewards may lead to a negative anhedonic state.
Controls did demonstrate larger P300 amplitudes than cocaine users across all outcomes and demonstrated a sensitivity to magnitude information that cocaine users did not. This parallels the findings of Goldstein and colleagues, who found that cocaine users were insensitive to magnitude of reward. Our findings, however, isolated this lack of sensitivity to the P300 component, which most likely reflects later processing of reward meaning (Sato et al. 2005). Considering the magnitude effects observed in the FRN in cocaine users, this group clearly processes reward magnitude information at some level but fails to process it to the same extent that controls do. Anhedonia was not associated with the P300 in either group.
Study limitations
An issue raised by one of the reviewers of this manuscript pertained to the possibility that pre-chosen analysis windows, selected based on the prior literature with an eye to measuring two different ERP processes (see e.g., the CRN and CNV windows in Fig. 2), could well end up measuring the same sustained process rather than two independent processes. If one observes the between-group differences at electrode site C1 in Fig. 2, it could certainly be argued that the first window (i.e., the CRN) captures the early phase of a sustained negative-going shift that is then simply re-measured during the CNV window. While this is an important general caveat and should lead to appropriate caution in the interpretation of these two time windows, we do not believe that this is what is occurring here. If one observes the waveforms in the neighboring electrode sites, one sees that there is little or no early negativity (CRN) at FCz, whereas the second late negative phase (CNV) is clearly present. Put another way, the early and late negative phases have different topographic distributions, and therefore, they cannot represent the same process.
Examination of drug-abusing populations always raises the uncertainty that the effects observed are due to acute effects of the drug or due to sudden abstinence from the drug. While participants were asked to refrain from drug use for 24 h, and a goal of this work was to examine the neurocognitive profiles of cocaine users without requiring them to alter their normal usage patterns, it is possible that the effects observed could be due to acute withdrawal, especially in those who did not show cocaine-positive urines. However, it should be noted that the 24-h period of abstinence we asked participants to undergo was not onerous considering the typical “binge” use pattern of cocaine (Gawin 1989; Simon et al. 2002), and the average thrice weekly use pattern of our particular cohort.
Another difficulty that arises when investigating drug use is the tendency of drug users to abuse more than one substance. It is difficult to generalize the findings here only to cocaine, despite this substance being the drug of choice for every participant, as all but three participants also used nicotine. It is especially worthwhile to consider that nicotine use could have an effect on the findings here. However, a strength of this study is that this population more accurately reflects general drug using populations, making our findings very relevant to treatment providers who seek to treat individuals who may report drugs of choice but actually abuse many different substances.
In addition, though groups were the same size, due to the fact that cocaine users are a clinical population, increased variability may explain some of the failure to find patterns in cocaine users that were found in controls, such as the failure to find probability or magnitude differences in later stages of processing. In addition, the limitations that were present in Morie et al. (2014a, b, c) are also present in this work, as the tasks were identical. Finally, while an effort was made to recruit female participants, only seven of our participants were female. This limits the generalizability of our findings.
Conclusions
The major goals of this project were to examine reward and monitoring processes in cocaine users and controls and to determine if there was any association of anhedonia with these processes. Our findings imply that cocaine users show increased motivation toward reward when given reward cues, but fail to make accurate reward predictions or update predictions based on task feedback. Further, cocaine users demonstrate blunted reward responses to rewarding feedback, despite their increased motivation. Anhedonia is indeed associated with anticipatory reward in cocaine users, along with indices of task monitoring and with reward response. This work lends further support to the idea that cocaine use is associated with a dysregulation between wanting rewards and liking rewards, as has been suggested in the incentive sensitization theory of drug use (Robinson and Berridge 2001), and implies that anhedonia may be a factor involved with this dysregulation. Finally, these data point to deficits in the ability to properly monitor actions taken to receive reward or update reward predictions in cocaine addicts, which may well contribute to the difficulty they encounter when trying to stop using. This lends evidence to the idea that treatment in the future should be focused upon improving self-monitoring capabilities and inhibiting craving, as with cognitive behavioral therapy, and also suggests a need for reward supplementation, such as contingency management.
References
Baker TE, Holroyd CB (2011) Dissociated roles of the anterior cingulate cortex in reward and conflict processing as revealed by the feedback error-related negativity and N200. Biol Psychol 87:25–34
Bechara A, Dolan S, Denburg N, Hindes A, Anderson SW, Nathan PE (2001) Decision-making deficits, linked to a dysfunctional ventromedial prefrontal cortex, revealed in alcohol and stimulant abusers. Neuropsychologia 39:376–389
Bechara A, Dolan S, Hindes A (2002) Decision-making and addiction (part II): myopia for the future or hypersensitivity to reward? Neuropsychologia 40:1690–1705
Bell RP, Foxe JJ, Ross LA, Garavan H (2014) Intact inhibitory control processes in abstinent drug abusers (I): a functional neuroimaging study in former cocaine addicts. Neuropharmacology 82:143–150
Benikos N, Johnstone SJ, Roodenrys SJ (2013) Varying task difficulty in the Go/Nogo task: the effects of inhibitory control, arousal, and perceived effort on ERP components. Int J Psychophysiol 87:262–272
Carter BL, Tiffany ST (1999) Meta-analysis of cue-reactivity in addiction research. Addiction 94:327–340
Chapman LJ, Chapman JP, Raulin ML (1976) Scales for physical and social anhedonia. J Abnorm Psychol 85:374–382
Chase HW, Eickhoff SB, Laird AR, Hogarth L (2011) The neural basis of drug stimulus processing and craving: an activation likelihood estimation meta-analysis. Biol Psychiatry 70:785–793
Dorard G, Berthoz S, Phan O, Corcos M, Bungener C (2008) Affect dysregulation in cannabis abusers: a study in adolescents and young adults. Eur Child Adolesc Psychiatry 17:274–282
Erlenmeyer-Kimling L, Cornblatt BA, Rock D, Roberts S, Bell M, West A (1993) The New York High-Risk Project: Anhedonia, Attentional Deviance, and Psychopathology. Schizophr Bull 19
Everitt BJ (2014) Neural and psychological mechanisms underlying compulsive drug seeking habits and drug memories—indications for novel treatments of addiction. Eur J Neurosci 40:2163–2182
Fillmore MT, Rush CR (2006) Polydrug abusers display impaired discrimination-reversal learning in a model of behavioural control. J Psychopharmacol 20:24–32
Franken IH, Zijlstra C, Muris P (2006) Are nonpharmacological induced rewards related to anhedonia? A study among skydivers. Prog Neuropsychopharmacol Biol Psychiatry 30:297–300
Franken IH, Rassin E, Muris P (2007a) The assessment of anhedonia in clinical and non-clinical populations: further validation of the Snaith-Hamilton Pleasure Scale (SHAPS). J Affect Disord 99:83–89
Franken IH, van Strien JW, Franzek EJ, van de Wetering BJ (2007b) Error-processing deficits in patients with cocaine dependence. Biol Psychol 75:45–51
Garavan H, Hester R (2007) The role of cognitive control in cocaine dependence. Neuropsychol Rev 17:337–345
Garavan H, Kaufman JN, Hester R (2008) Acute effects of cocaine on the neurobiology of cognitive control. Philos Trans R Soc Lond Ser B Biol Sci 363:3267–3276
Gawin F (1989) Cocaine dependence. Annu Rev Med 40:149–161
Goldstein RZ, Cottone LA, Jia Z, Maloney T, Volkow ND, Squires NK (2006) The effect of graded monetary reward on cognitive event-related potentials and behavior in young healthy adults. Int J Psychophysiol Off J Int Organ Psychophysiol 62:272–279
Goldstein RZ, Parvaz MA, Maloney T, Alia-Klein N, Woicik PA, Telang F, Wang GJ, Volkow ND (2008) Compromised sensitivity to monetary reward in current cocaine users: an ERP study. Psychophysiology 45:705–713
Goldstein RZ, Alia-Klein N, Tomasi D, Carrillo JH, Maloney T, Woicik PA, Wang R, Telang F, Volkow ND (2009) Anterior cingulate cortex hypoactivations to an emotionally salient task in cocaine addiction. Proc Natl Acad Sci U S A 106:9453–9458
Harvey PO, Pruessner J, Czechowska Y, Lepage M (2007) Individual differences in trait anhedonia: a structural and functional magnetic resonance imaging study in non-clinical subjects. Mol Psychiatry 12(703):767–775
Hewig J, Kretschmer N, Trippe RH, Hecht H, Coles MG, Holroyd CB, Miltner WH (2010) Hypersensitivity to reward in problem gamblers. Biol Psychiatry 67:781–783
Janiri L, Martinotti G, Dario T, Reina D, Paparello F, Pozzi G, Addolorato G, Di Giannantonio M, De Risio S (2005) Anhedonia and substance-related symptoms in detoxified substance-dependent subjects: a correlation study. Neuropsychobiology 52:37–44
Jentsch JD, Olausson P, De La Garza R 2nd, Taylor JR (2002) Impairments of reversal learning and response perseveration after repeated, intermittent cocaine administrations to monkeys. Neuropsychopharmacology Off Publ Am Coll Neuropsychopharmacology 26:183–190
Jia Z, Worhunsky PD, Carroll KM, Rounsaville BJ, Stevens MC, Pearlson GD, Potenza MN (2011) An initial study of neural responses to monetary incentives as related to treatment outcome in cocaine dependence. Biol Psychiatry 70:553–560
Kampman KM, Volpicelli JR, McGinnis DE, Alterman AI, Weinrieb RM, D’Angelo L, Epperson LE (1998) Reliability and validity of the Cocaine Selective Severity Assessment. Addict Behav 23:449–461
Kuhn S, Gallinat J (2011) Common biology of craving across legal and illegal drugs—a quantitative meta-analysis of cue-reactivity brain response. Eur J Neurosci 33:1318–1326
Leynes PA, Allen JD, Marsh RL (1998) Topographic differences in CNV amplitude reflect different preparatory processes. Int J Psychophysiol Off J Int Organ Psychophysiol 31:33–44
Li CS, Milivojevic V, Kemp K, Hong K, Sinha R (2006) Performance monitoring and stop signal inhibition in abstinent patients with cocaine dependence. Drug Alcohol Depend 85:205–212
McLellan AT, Luborsky L, Cacciola J, Griffith J, Evans F, Barr HL, O’Brien CP (1985) New data from the Addiction Severity Index: reliability and validity in three centers. J Nerv Ment Dis 3:412–423
Morie KP, De Sanctis P, Garavan H, Foxe JJ (2014a) Executive Dysfunction and Reward Dysregulation: A High-Density Electrical Mapping Study in Cocaine Abusers. Neuropharmacology 85
Morie KP, Garavan H, Bell RP, De Sanctis P, Krakowski MI, Foxe JJ (2014b) Intact inhibitory control processes in abstinent drug abusers (II): a high-density electrical mapping study in former cocaine and heroin addicts. Neuropharmacology 82:151–160
Morie KP, Sanctis PD, Foxe JJ (2014c) Reward Contingencies and the Recalibration of Task Monitoring and Reward Systems: A high-density electrical mapping study. Neuroscience
Nelson A, Killcross S (2006) Amphetamine exposure enhances habit formation. J Neurosci Off J Soc Neurosci 26:3805–3812
Padrao G, Mallorqui A, Cucurell D, Marco-Pallares J, Rodriguez-Fornells A (2012) Neurophysiological differences in reward processing in anhedonics. Cogn Affect Behav Neurosci
Parvaz MA, Maloney T, Moeller SJ, Woicik PA, Alia-Klein N, Telang F, Wang GJ, Squires NK, Volkow ND, Goldstein RZ (2012) Sensitivity to monetary reward is most severely compromised in recently abstaining cocaine addicted individuals: a cross-sectional ERP study. Psychiatry Res 203:75–82
Polich J, Kok A (1995) Cognitive and biological determinants of P300: an integrative review. Biol Psychol 41:103–146
Robinson TE, Berridge KC (2001) Incentive-sensitization and addiction. Addiction 96:103–114
Sato A, Yasuda A, Ohira H, Miyawaki K, Nishikawa M, Kumano H, Kuboki T (2005) Effects of value and reward magnitude on feedback negativity and P300. Neuroreport 16:407–411
Schoenbaum G, Saddoris MP, Ramus SJ, Shaham Y, Setlow B (2004) Cocaine-experienced rats exhibit learning deficits in a task sensitive to orbitofrontal cortex lesions. Eur J Neurosci 19:1997–2002
Simon SL, Richardson K, Dacey J, Glynn S, Domier CP, Rawson RA, Ling W (2002) A comparison of patterns of methamphetamine and cocaine use. J Addict Dis 21:35–44
Sokhadze E, Stewart C, Hollifield M, Tasman A (2008) Event-related potential study of executive dysfunctions in a speeded reaction task in cocaine addiction. J Neurother 12:185–204
Sturmer B, Nigbur R, Schacht A, Sommer W (2011) Reward and punishment effects on error processing and conflict control. Front Psychol 2:335
Wang J, Chen J, Lei Y, Li P (2014) P300, not feedback error-related negativity, manifests the waiting cost of receiving reward information. Neuroreport 25:1044–1048
Wu Y, Zhou XL (2009) The P300 and reward valence, magnitude, and expectancy in outcome evaluation. Brain Res 1286:114–122
Yeung N, Sanfey AG (2004) Independent coding of reward magnitude and valence in the human brain. J Neurosci Off J Soc Neurosci 24:6258–6264
Yu R, Zhou W, Zhou X (2011) Rapid processing of both reward probability and reward uncertainty in the human anterior cingulate cortex. PLoS One 6:e29633. doi:10.1371/journal.pone.0029633
Acknowledgments
We thank the Albert Einstein Division of Substance Abuse, Dr. Julia Arnsten, Dr. Sarah Church, Juan Martinez, Amy Greengrass, Marsha Dommel, and all of the staff at the Next Steps Addiction Treatment Centers in the Bronx for all of their help in recruitment efforts. The work would simply not have been possible without the dedication of these individuals. We would also like to express our sincere gratitude to the participants for giving their time to this effort. Additionally, we thank Dr. Ryan Bell, Ms. Sarah Ruberman, and Mr. Frantzy Acluche for their help during data collection. Participants in this study were recruited and evaluated at The Human Clinical Phenotyping Core, a facility of the Rose F. Kennedy Intellectual and Developmental Disabilities Research Center (IDDRC) which is funded through a center grant from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD P30 HD071593). Dr. Morie is now at the Department of Psychiatry, Yale University School of Medicine, New Haven, CT, USA.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All participants signed an informed consent document administered by HIPAA-certified staff. All procedures were approved by the Institutional Review Board of the Albert Einstein College of Medicine. The study conformed to the principles outlined in the Declaration of Helsinki.
Conflict of interest
The authors declare that they have no competing interests.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 39 kb)
Rights and permissions
About this article

Cite this article
Morie, K.P., De Sanctis, P., Garavan, H. et al. Regulating task-monitoring systems in response to variable reward contingencies and outcomes in cocaine addicts. Psychopharmacology 233, 1105–1118 (2016). https://doi.org/10.1007/s00213-015-4191-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-015-4191-8