
Abstract
While hedonic and reward-related processes are central to drug use and dependence, this article focuses on the contribution that cognitive processes may make to addiction. In particular, attention is drawn to those processes involved in exercising control over behavior as drug dependence is characterized by risky, impulsive behavior. Functional neuroimaging implicates prefrontal deficits in cocaine dependence with an emerging picture of cocaine users having attentional biases towards drug-related stimuli, poor performance in laboratory tests of inhibitory control, and compromised monitoring and evaluation of their behavior. Combined, these deficits may contribute to the continuation of use in dependent individuals and may qualify as important targets for therapeutic interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The DSM-IV criteria for drug dependence, while stressing physiological reactions to continued drug use such as withdrawal and tolerance, place considerable emphasis on the behavioral aspects of dependence (DSM-IV-TR; American Psychiatric Association 2000). In particular, an inability to reduce use despite knowledge of its detrimental effects points to dysfunctional behavioral control as a key contributor to dependence. Advances in cognitive neuroscience research is showing that the willpower so often called upon to control use, like all cognitive processes, has a neurobiological basis and can be investigated using modern neuroscientific methods. An emerging picture from this research suggests a particularly unfortunate scenario for users of drugs such as cocaine: As well as affecting the brain’s reward and reinforcement circuitry generating pathological desires for the drug, cocaine users would also appear to display neurobiological impairments in those same brain systems that are required to exercise control (willpower) over those desires.
Cognitive Aspects of Drug Use
Drug dependence is commonly characterized as an affective or emotional phenomenon given the central roles of psychological functions such as reward, reinforcement, craving, and stress. An open question, and one that might speak to individual differences in dependence risk, is the contributing role of cognitive processes such as inhibitory and attentional control, behavior monitoring and memory. Although hedonic processes of liking and craving may be the core of the motivation to consume drugs, certain cognitive processes such as memory likely contribute to these drives whereas others, such as impulse control, contribute to the individual’s efforts to resist these drives. In this regard, cognitive functions may be of significant importance in understanding the transition from recreational to dependent use, and the relapse so typical of those attempting abstinence.
Research into the cognitive dimension of dependence can be placed into two groupings. The first is studies on the impact that drugs of abuse may have on cognitive abilities. For example, information on the effects that cannabis use may have on memory (Pope et al. 2001; Solowij et al. 2002), nicotine on attention (Lawrence et al. 2002; Rezvani and Levin 2001), or ecstasy on recognition of facial expressions (Hoshi et al. 2004) help characterize the effects of these drugs. This knowledge may provide insights into the mechanisms of action of a drug and guidance on functions to target for therapeutic interventions. The second grouping of studies focuses on cognitive processes that may contribute directly to the dependence itself, so that their very dysfunction may exacerbate the dependence. Examples would include the mechanisms of drug-related Pavlovian and instrumental reinforcement (Everitt and Robbins 2005); the mechanisms by which stimuli associated with previous drug use are detected and processed, and may initiate drug cravings (Hester et al. 2006; Grant et al. 1996); the role of rewards and reward expectancy in guiding decision-making (Bechara et al. 2002; Goldstein et al. 2007a; Grant et al. 2000; Stout et al. 2005; Wrase et al. 2007); the contribution of learning and memory processes to the development of pathological addictive memories (Hyman 2005); and the cognitive processes involved in monitoring and inhibiting one’s behavior (Forman et al. 2004; Kaufman et al. 2003). An argument may be made that the first group of studies also contributes to the continuance of use (e.g., a self-medication hypothesis might hold that the acute improvements that these drugs may have on these cognitive processes contributes to their reinforcing power). However, the second group of studies may be more directly relevant to dependence and, by their nature, may apply more generally to all drugs of abuse. It is the possible contribution of cognitive control functions to dependence that is the focus of this paper.
Cognitive control functions may be of particular relevance at either end of the addiction life cycle. That is, in the same way that pre-existing levels of D2 receptors in the ventral striatum can mediate the pleasure response to a first administration of methylphenidate (Volkow et al. 1999), impairments in cognitive functions such as impulse control may predispose some individuals either to a first impulsive use of an illicit drug or to the transition from recreational to dependent use. For example, behavioral and cognitive measures of impulsivity in 10–12 year olds predict drug use at age 19 (Tarter et al. 2003). Similarly, specific personality risk factors correlate with specific patterns of drug use and psychiatric co-morbidities, with cocaine use associated with antisocial personality disorder and impulsivity (Conrod et al. 2000). An animal model of impulsivity, which shows elevated levels of cocaine self-administration, has also been shown to have reduced D2 receptor levels in the ventral striatum prior to first use (Dalley et al. 2007). At the other end of the dependence cycle, cognitive control may contribute to risk of relapse for those attempting abstinence. Stroop-like tasks (described below), which can assess an attentional bias for drug-related stimuli, have been shown to predict relapse and to do so better than other standard dependence measures, such as self-reports of dependence or drug use histories (Cox et al. 2002; Waters et al. 2003). Paulus and colleagues have shown that prefrontal, cingulate and temporal lobe activation during a two-choice prediction task performed three to four weeks after ceasing methamphetamine use could predict relapsers approximately a year later (Paulus et al. 2005). In this study, the first to show that functional magnetic resonance imaging (fMRI) could predict relapse, activation specific to uncertain decision making was isolated by comparison with a sensorimotor control task in which participants pushed a button to acknowledge a target’s presence on screen. It would appear that the cognitive and neurobiological processes involved in risky decision-making may be of particular consequence for relapse.
Cocaine and Cognitive Control Dysfunction
Cognitive control processes, also commonly referred to as executive functions, are typically non-routinized, attentionally demanding, volitional processes that are involved in goal-directed behavior. On one level, all goal-directed behavior, however trivial, might be said to require cognitive control: one operational definition of executive functions includes all processes that can be influenced by instructions or incentives (Cowan 2001). Control processes that are most typically investigated in the laboratory include inhibitory control, attention switching, performance monitoring, and decision making. Many studies of cognitive control using a range of methodologies identify this control with the frontal lobes.
Cocaine is a short acting, CNS psychostimulant that produces marked physiological and behavioral alterations in both experimental animals and humans. Acutely, cocaine increases heart rate, blood pressure, stereotypy and locomotion, increases arousal, decreases fatigue and produces a profound euphoria (Johanson and Fischman 1989). Many of these effects are thought to be directly related to the drug’s ability to increase monoamines in the synaptic cleft by inhibiting transmitter uptake (Ritz et al. 1990). The mesocorticolimbic and nigrostriatal dopamine systems are thought to be principally involved in cocaine’s reinforcing and motor activating properties, respectively, with the nucleus accumbens suggested to lie at the limbic-motor interface involved in both the reinforcing and the locomotor effects of cocaine (Kelly and Iversen 1976, Mogenson et al. 1980). Cocaine use has been linked to cerebral atrophy (Pascual-Leone et al. 1991) and hypoperfusion in the frontal, periventricular, and/or temporal–parietal areas (Holman et al. 1991, Strickland et al. 1993). More recent automated techniques that assess tissue concentration or tissues volumes based on high-resolution anatomical magnetic resonance imaging (MRI) have revealed volumetric deficits in multiple frontal areas in cocaine users including anterior cingulate and orbitofrontal cortex as well as insula and temporal cortex (Franklin et al. 2002; Matochik et al. 2003). Tissue deficits relative to controls in these areas are of particular interest given the cognitive deficits in users, discussed below, that are thought to rely on functions subserved by these regions.
There are data to suggest that the frontal lobes may be particularly affected by cocaine. In animal models the frontal lobes are the first areas to show metabolic changes caused by acute cocaine (Porrino et al. 1998). In a seminal fMRI study of cocaine users, lateral prefrontal and cingulate regions were among those that activated in response to an acute IV cocaine administration (Breiter et al. 1997). The time-course of cocaine-induced activity changes in the majority of the activated prefrontal regions corresponded with behavioral measures of a “rush” response, having early but transient signal changes following injection. In addition, cocaine craving, which can be induced in users by viewing videos of cocaine use or by handling cocaine paraphernalia while undergoing functional brain imaging, also typically involves the prefrontal cortex (Garavan et al. 2000; Grant et al. 1996): It is likely that similar prefrontal structures involved in the response to a drug’s effects may subsequently be engaged in the re-imagining or craving of those effects. Measures of resting glucose utilisation (i.e., basal brain activity with no task being performed) in abstinent cocaine users show initial increases (e.g., one week after abstinence) followed by prolonged decreases (three to four months after detoxification) in prefrontal and orbitofrontal metabolism (Volkow et al. 1991, 1992, 1993). The early increases in metabolic activity correlate with craving and may reflect reduced brain dopamine activity (Volkow et al. 1993).
Chronic cocaine users often perform poorly on experimental and neuropsychological tasks that probe working memory function (Berry et al. 1993; Kübler et al. 2005; O’Malley and Gawin 1990). Of note, tasks that load heavily on cognitive control demands (Ardila et al. 1991; Beatty et al. 1995; Hoff et al. 1996; Kübler et al. 2005; Rosselli and Ardila 1996) frequently reveal poorer performance in cocaine users. Many of these compromised cognitive functions require dorsolateral prefrontal and orbitofrontal participation, dopamine rich regions hypothesized to be vulnerable to drug-induced dysregulation (Dackis and O’Brien 2001) and, as noted, regions with central roles in executive functions. The role of the frontal lobes in cognitive control and the evidence of the effects of cocaine on them lead to the hypothesis that cocaine may disrupt volitionally mediated control. If true, this would render the behavior of cocaine users less under internal volitional control (willpower) and perhaps driven instead by automatic, habitual behavioral patterns or environmental contingencies (e.g., drug-related cues). As articulated in a model of addiction (I-RISA: impaired response inhibition and salience attribution, Goldstein and Volkow 2002), reduced prefrontal control renders the heightened salience attributed to drugs and drug-related stimuli unfettered in determining behavior. The I-RISA model proposes neuroanatomical substrates for the key behavioral manifestations of addiction including intoxification, craving, bingeing and withdrawal. Reinforcement and salience attribution are associated with intoxification, expectancy with craving and loss of control with bingeing and relapse. To assess the evidence relevant to the hypothesis of diminished prefrontal control, the following sections will focus on the links between cocaine use and attentional control, inhibitory control and behavioral monitoring.
Attentional Control
Incentive salience theories of addiction hold that stimuli associated with drug use acquire disproportionately high approach value to the user (Robinson and Berridge 2003). One result of the increased salience of such stimuli is that it may result in an attentional bias wherein users are highly attuned to detect and process these stimuli. This processing may initiate cravings, leading eventually to use. These attentional biases can be assessed using “emotional” Stroop tasks in which irrelevant evocative information can interfere with a primary task. Typical task versions present drug-related words in color fonts requiring participants to report the font and ignore the word name or might present drug-related pictures surrounded by a color border requiring participants to report the border color and ignore the drug-related image (Hester et al. 2006). The essential feature of these tasks is that the irrelevant information will prove distracting, slowing responses and reducing accuracy, if that information is evocative for the participant. Consequently, drug users will show performance decrements on trials with irrelevant drug stimuli that are of a similar magnitude to trials in which the distracting information might be inherently evocative such as erotic images or highly valenced words. In contrast, control participants will only show performance decrements for the inherently evocative stimuli which demonstrates the importance of an individual’s personal drug history in generating the interference effects. Stroop-like attentional biases have been observed in alcohol (Cox et al. 2002; Duka and Townshend 2004; Lusher et al. 2004), nicotine (Waters et al. 2003; Wertz and Sayette 2001), heroin (Franken et al. 2000), and cocaine users (Hester et al. 2006). Although these tasks lack the response conflict inherent in the standard Stroop task in which the distracting information (the word name or picture within the colored border) is one of the legitimate responses, they nonetheless have considerable clinical interest in that these attentional biases, as noted earlier, have been shown to predict relapse (Waters et al. 2003).
The neural mechanisms underlying these attentional biases in human cocaine users have not been the subject of much investigation. Goldstein and colleagues report an imaging study of cocaine users performing a verbal Stroop task (Goldstein et al. 2007b). Consistent with typical Stroop tasks in healthy controls (Bush et al. 2000), substantial bilateral activation was observed in the anterior cingulate cortex (ACC), a region frequently implicated in the cognitive dysfunctions of drug users as discussed in more detail below. Activation in response to cocaine-related words relative to neutral words differed in rostral anterior cingulate and medial orbitofrontal cortex. In addition, individual differences in performance correlated with activity in these same areas, implicating them in processing the heightened salience of drug stimuli.
Most attention switching studies have assessed switching between externally presented stimuli (e.g., between sensory modalities or between competing stimuli in one modality; Guzy and Axelrod 1972) or between task sets (e.g., between performing a mathematical operation and a language-based semantic operation; Monsell 2003). However, attentional control to one’s thoughts may be of particular relevance for drug abuse. Perseverative thinking on a topic, be it ruminations on one’s body weight, one’s repeated failures, the feared object of a phobia, or the pleasure to be had from a drug of abuse, are characteristic of many clinical conditions. An inability to switch attention away from thoughts of drug use may contribute to drug-seeking behavior. One operationalisation of attentional control to one’s thoughts is a task in which participants must switch between items held in working memory (Garavan 1998). These items may be counts in verbal working memory or locations within a matrix imagined in visuospatial working memory and in which subjects can be cued visually to attend to one item or another (Kübler et al. 2003). Using a task in which participants were required to switch between counts in working memory, Kuebler and colleagues observed reduced activity in cocaine users in the anterior cingulate cortex and the putamen (Kübler et al. 2005). This finding may provide initial support for a neurobiological basis for a difficulty in disengaging attention from drug-related thoughts (a single-mindedness) that might characterize the drug-seeking behaviors often observed in users.
Inhibitory Control
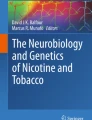
The ability to attend selectively to a subset of a complex environment, activate appropriate meanings during verbal and written language comprehension, and activate appropriate memories at encoding and retrieval may all be critically dependent upon the ability to suppress interfering stimuli, interpretations and memories, respectively (Dagenbach and Carr 1994). Neuroimaging studies have implicated prefrontal regions in these inhibitory functions (Garavan et al. 1999; Konishi et al. 1999; Menon et al. 2001) but activation associated with response inhibition extends beyond prefrontal regions to include the supplementary motor area and pre-supplementary motor area and the occipital and parietal lobes (Liddle et al. 2001, Mostofsky et al. 2003). Studies that have exploited the cognitive specificity afforded by event-related fMRI, in which trial-specific activity can be isolated, have observed a strongly right lateralized network underlying inhibitory control that includes prefrontal, midline (anterior cingulate and pre-supplementary motor area), and parietal regions (Garavan et al. 2006; Rubia et al. 2003; see Fig. 1). In addition, lesion and transcranial magnetic stimulation studies (the latter temporarily disrupt neural functioning with magnetic pulses) point to the right inferior frontal gyrus as a crucial node for motor response inhibition (Aron et al. 2003; Chambers et al. 2006).

Regions activated for successful inhibitions in a go/no-go task. These results are based on a large sample (n = 71) and show robust right hemisphere involvement in inhibiting a prepotent motor behavior (Garavan et al. 2006)
Cocaine users have been shown to have poor inhibitory control. Fillmore and colleagues (Fillmore and Rush 2002) have demonstrated this using one of the most widely used tests of motor inhibition, the stop task (Logan and Cowan 1984), in which a response, prompted by a stimulus, is occasionally and unpredictably required to be withheld following a second stimulus (i.e., the stop signal). Moreover, acute cocaine administrations produce a quadratic dose-response effect on performance on this task in which performance improved but only for lower doses of cocaine (Fillmore et al. 2006). On a go/no-go task which is similar insofar as it also requires frequent motor responses and occasional, unpredictable response withholds, performance improved linearly as a function of dose. The authors explain these effects as evidence of impaired impulse control in users being corrected for a range of intermediate doses (and differences between the tasks explaining the failure to see a curvilinear relationship between performance and dose in the go/no-go task). If we assume that inhibitory control is mediated by dopamine (these mechanisms should also apply to other neuro-trasmitter systems) then this restorative effect may reflect a pharmacological improvement of a basal hypodopaminergic state that may either have preceded or resulted from cocaine use. Higher doses of cocaine push the user away from the peak of an idealized dose-response curve between performance and dopamine levels into a hyperdopaminergic state. Similar effects can be observed in healthy controls in that individuals with low working memory capacities (a behavioral assay of low basal dopamine function) show beneficial effects on performance following a dopamine agonist (Gibbs and D’Esposito 2005).
Neuroimaging studies have shown reduced prefrontal activity during inhibition in users (Hester and Garavan 2004; Kaufman et al. 2003). Hester and colleagues have shown that an impairment in users is best observed when task demands are increased by adding a simultaneous working-memory load. In this task, a serial stream of letters were presented and participants were instructed to respond to all letters except those previously identified as no-go letters from which responding should be withheld. The size of the no-go letter set was varied across trials thereby requiring subjects to maintain a variable amount of information in working memory while performing the response inhibition task. Adding this parametric manipulation yielded insights into the dynamics of functional cortical recruitment in users. For example, healthy control participants revealed increased dorsolateral prefrontal and anterior cingulate activity for inhibitions as a function of increased working memory load (Hester et al. 2004a, b). The cerebellum showed an opposite pattern, reducing in activity as a function of memory load. These results were interpreted to reflect the roles of the prefrontal cortex in flexible, controlled action as distinct from the cerebellum which would be involved in more routinised, predictable, stimulus-response operations (Courchesne and Allen 1997). In stark contrast to this pattern in controls, cocaine users did not show increases in activation in response to the memory load manipulation in dorsolateral prefrontal and anterior cingulate cortices. Instead, they showed increases in cerebellar activity. Similar evidence of functional cerebellar recruitment has been observed in cannabis users (Bolla et al. 2005) and alcoholics (Desmond et al. 2003). One interpretation of these results is that the cognitive control deficits mediated by prefronted regions of users produce a reversion to reliance on sub-optimal cerebellar circuits.
Behavioral Monitoring
The ability to monitor one’s ongoing performance is central to behavioral control. Detecting one’s errors (or the likelihood of committing an error) serves an adaptive function in signaling to an individual that the intervention of other attention or control processes would be advantageous (Botvinick et al. 2001; MacDonald et al. 2000). This type of executive control is necessary for producing coherent and effective behavior in real-world environments, in which task demands fluctuate and dynamic responses to performance feedback is crucial. The inability to detect or appreciate the importance of errors has been found to relate to a wide variety of clinical symptoms, including the particularly debilitating symptoms of loss of insight (Ott et al. 1996), perseverative behavior, and the disorganisation syndrome of schizophrenia (Liddle et al. 1992). These clinical symptoms have also been shown to be strong predictors of poor clinical outcomes, including the inability to maintain independent living skills (DeBettignies et al. 1990), and relapse rates in depression and drug addiction (Peralta and Cuesta 1998; Teasdale et al. 2002).
Much research implicates the anterior cingulate cortex (ACC) in error-related functions (Dehaene et al. 1994) and error-related hypoactivity has been observed in cocaine users (Kaufman et al. 2003). Others have observed a similar ACC hypoactivity in opiate users (Forman et al. 2004; Lee et al. 2005; Yucel and Lubman 2007), on a Stroop task in both cocaine (Bolla et al. 2004) and cannabis users (Eldreth et al. 2004), and following alcohol administration (Ridderinkhof et al. 2002) suggesting that this phenomenon may be a general feature of drug abuse. Anterior cingulate cortex functional hypoactivity is also consistent with other metabolic and anatomical evidence of ACC dysregulation in cocaine users (Franklin et al. 2002; Hammer et al. 1993). The ACC response to errors may be driven by the same mesocorticolimbic dopamine system that involves the nucleus accumbens in cocaine’s reinforcing effects (Holroyd and Coles 2002). Indeed, the nucleus accumben’s prediction-error response to rewards and their absence (Schultz et al. 1997) shares many characteristics with the ACC’s response to errors insofar as an error is a loss of a possible reward. Consequently, the proposed mechanisms by which dopamine affects reinforcement-related processes in the nucleus accumbens may also apply to control-related processes in the ACC.
An ACC functional deficit may be quite consequential for addiction especially in light of recent theories which propose that the ACC monitors the likelihood of errors (and not errors, per se; Brown and Braver 2005; Magno et al. 2006) and, conceptually similar, that the ACC assesses risk and uncertainty in decision making (Paulus and Lawrence 2006). Compromise to these psychological functions may render the cocaine user more likely to make risky decisions concerning use, or not to detect when the likelihood of drug use increases (e.g., monitoring internal risk factors such as stress or craving or external factors such as meeting drug-using acquaintances). To determine those cognitive consequences that might follow from an ACC deficit, cocaine users were tested on two modified go/ no-go tasks thought to rely on intact ACC functioning (Hester et al. 2007; see Fig. 2). The first task measured post-error slowing which is an adaptive response to improve performance following errors while the second task assessed error awareness by requiring subjects to make a separate button press whenever they made an error. Results revealed that although cocaine users were identical to controls in their post-error behavior they detected fewer of their errors. Anterior cingulate cortex hypoactivity and a diminished awareness of errors is complemented by a body of evidence showing a blunted response to losses in drug users on laboratory gambling tasks (Garavan and Stout 2005). In support of the proposition that these neurobiological deficits may also relate to risk-taking behavior, it is notable that the risky behavior of methamphetamine users on a gambling task has been linked to reduced ACC activity (Fishbein et al. 2005). Similar ACC-mediated cognitive risk factors may apply at the other end of the addiction life cycle. A risk-taking personality type is predictive of drug use (Feldstein and Miller 2006) and the risk taking behavior of adolescents has been linked to ACC hypofunction (Bjork et al. 2007).

The Error Awareness Task presents a serial stream of color name words. Subjects are required to make a button-press response to all stimuli except when a stimulus repeats (Repeat no-go) or when a stimulus contains an incongruency between the color name and the color font (Stroop no-go). Subjects make two button-press responses on the trial immediately following an error of commission to communicate their conscious awareness of their errors. Cocaine users had a higher percentage of unaware errors relative to controls (Hester et al. 2007). The Behavior Adaptation Task presents a serial stream of the letters X and Y and requires response inhibitions whenever a letter is the same as the preceding letter (Repeat no-go). It manipulates a requirement for post-error slowing by presenting occasional double-repeats (condition shown on bottom). That is, a repeat no-go is sometimes immediately followed by a second repeat no-go resulting in subjects showing substantially slower responses on trials following all repeat no-gos in this condition. Cocaine users and controls performed identically on all measures of post-error slowing (Hester et al. 2007)
Conclusion
Research into the cognitive abilities of cocaine users present a picture in which there are deficits in the very processes that may be integral to averting dependent use. The emerging results suggest that cocaine users may have an attentional bias to detect drug-related stimuli, poor inhibitory control, and compromised evaluation of their risky behaviors. That said, the exact pattern of neurocognitive deficits and how they may interact with one another in cocaine users is still being elucidated. For example, Li and colleagues provide evidence that the impulse control deficits of users as assayed by the STOP signal task may be secondary to other attentional or monitoring deficits (Li et al. 2006). The challenge to researchers is not only to discover the true profile of cognitive deficits, but to demonstrate that they are consequential, in a causal sense, for addiction. In this regard, the evidence that cognitive abilities can predict the development of drug problems or can predict relapse are highly relevant. Modern neuroimaging techniques are invaluable here in that they enable the neurobiology of the uniquely human dimensions of addiction to be investigated. Whereas dominant theories of addiction, rooted, as they are, primarily in animal models, may explain the drive to consume drugs, there is an important role for human studies to explain the decisions to consume. These decisions can be decomposed into elementary psychological processes that are amenable to investigation. Understanding what might be the core cognitive dysfunctions contributing to dependence may result in an increased emphasis on cognitive control rehabilitation in treatment (Ryan 2006; Yucel and Lubman 2007).
References
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed—text revision). Washington, DC: American Psychiatric Press.
Ardila, A., Rosselli, M., & Strumwasser, S. (1991). Neuropsychological deficits in chronic cocaine abusers. International Journal of Neuroscience, 57(1–2), 73–79.
Aron, A. R., Fletcher, P. C., Bullmore, E. T., Sahakian, B. J., & Robbins, T. W. (2003). Stop-signal inhibition disrupted by damage to right inferior frontal gyrus in humans. Nature Neuroscience, 6, 115–116.
Beatty, W. W., Katzung, V. M., Moreland, V. J., & Nixon S. J. (1995). Neuropsychological performance of recently abstinent alcoholics and cocaine abusers. Drug and Alcohol Dependence, 37, 247–253.
Bechara, A., Dolan, S., & Hindes, A. (2002). Decision-making and addiction (part II): Myopia for the future or hypersensitivity to reward? Neuropsychologia, 40, 1690–1705.
Berry, J., van Gorp, W. G., Herzberg, D. S., Hinkin, C., Boone, K., Steinman, L. et al. (1993). Neuropsychological deficits in abstinent cocaine abusers: preliminary findings after two weeks of abstinence. Drug and Alcohol Dependence, 32(3), 231–237.
Bjork, J. M., Smith, A. R., Danube, C. L., & Hommer, D. W. (2007). Developmental differences in posterior mesofrontal cortex recruitment by risky rewards. The Journal of Neuroscience, 27(18), 4839–4849.
Bolla, K., Ernst, M., Kiehl, K., Mouratidis, M., Eldreth, D., Contoreggi, C. et al. (2004). Prefrontal cortical dysfunction in abstinent cocaine abusers. Journal of Neuropsychiatry and Clinical Neurosciences, 16(4), 456–464.
Bolla, K. I., Eldreth, D. A., Matochik, J. A., & Cadet, J. L. (2005). Neural substrates of faulty decision-making in abstinent marijuana users. NeuroImage, 26, 480–492.
Botvinick, M. W., Carter, C. S., Braver, T. S., Barch, D. M., & Cohen, J. D. (2001). Conflict monitoring and cognitive control. Psychological Review, 108(3), 624–652.
Breiter, H. C., Gollub, R. L., Weisskoff, R. M., Kennedy, D. N., Makris, N., Berke, J. D. et al. (1997). Acute effects of cocaine on human brain activity and emotion. Neuron, 19(3), 591–611.
Brown, J. W., & Braver, T. S. (2005) Learned predictions of error likelihood in the anterior cingulate cortex. Science, 307, 1118–1121.
Bush, G., Luu, P., & Posner, M. I. (2000). Cognitive and emotional influences in anterior cingulate cortex. Trends in Cognitive Sciences, 4, 215–222.
Chambers, C. D., Bellgrove, M. A., Stokes, M. G., Henderson, T. R., Garavan, H., Robertson, I. H. et al. (2006). Executive ‘brake failure’ following deactivation of human frontal lobe. Journal of Cognitive Neuroscience, 18, 444–455.
Conrod, P. J., Pihl, R. O., Stewart, S. H., & Dongier, M. (2000). Validation of a system of classifying female substance abusers on the basis of personality and motivational risk factors for substance abuse. Psychology of Addictive Behaviors, 14(3), 243–256.
Cowan, N. (2001). An embedded-processes model of working memory. In A. Miyake & P. Shah (Eds.), Models of working memory (p. 62–101). Cambridge University Press: Cambridge.
Courchesne, E., & Allen, G. (1997). Prediction and preparation, fundamental functions of the cerebellum. Learning Memory, 4, 1–35.
Cox, W. M., Hogan, L. M., Kristian, M. R., and Race, J. H. (2002). Alcohol attentional bias as a predictor of alcohol abusers’ treatment outcome. Drug and Alcohol Dependence, 68, 237–243.
Dackis, C. A., & O'Brien, C. P. (2001). Cocaine dependence: A disease of the brain’s reward centers. Journal of Substance Abuse Treatment, 21(3), 111–117.
Dagenbach, D. & Carr, T. (1994). Inhibitory processes in attention, memory, and language. New York: Academic.
Dalley, J. W., Fryer, T. D., Brichard, L, Robinson, E. S. J., Theobald, D. E. H., Lääne, K. et al. (2007). Nucleus accumbens D2/3 receptors predict trait impulsivity and cocaine reinforcement. Science, 315, 1267–1270.
DeBettignies, B. H., Mahurin, R. K., & Pirozzolo, F. Z. (1990). Insight for impairment in independent living skills in Alzheimer’s disease and multi-infarct dementia. Journal of Clinical and Experimental Neuropsychology, 12(2), 355–363.
Dehaene, S., Posner, M. I., & Tucker, D. M. (1994). Localization of a neural system for error detection and compensation. Psychological Science, 5, 303–305.
Desmond, J. E., Chen, S. H., DeRosa, E., Pryor, M. R., Pfefferbaum, A., & Sullivan, E. V. (2003). Increased frontocerebellar activation in alcoholics during verbal working memory: an fMRI study. NeuroImage, 19(4), 1510–1520.
Duka, T., & Townshend, J. M. (2004). The priming effect of alcohol pre-load on attentional bias to alcohol-related stimuli. Psychopharmacology (Berl), 176(3–4), 353–361.
Eldreth, D. A., Matochik, J. A., Cadet, J. L., & Bolla, K. I. (2004). Abnormal brain activity in prefrontal brain regions in abstinent marijuana users. NeuroImage, 23(3), 914–920.
Everitt, B. J., & Robbins, T. W. (2005). Neural systems of reinforcement for drug addiction: from actions to habits to compulsion. Nature Neuroscience, 8(11), 1481–1489 [erratum in Nat Neurosci. 2006 Jul;9(7):979].
Feldstein, S. W., & Miller, W. R. (2006). Substance use and risk-taking among adolescents. Journal of Mental Health, 15(6), 633–643.
Fillmore, M. T., & Rush, C. R. (2002). Impaired inhibitory control of behavior in chronic cocaine users. Drug and Alcohol Dependence, 66(3), 265–273.
Fillmore, M. T., Rush, C. R., & Hays, L. (2006). Acute effects of cocaine in two models of inhibitory control: Implications of non-linear dose effects. Addiction, 101(9), 1323–1332.
Fishbein, D. H., Eldreth, D. L., Hyde, C., Matochik, J. A., London, E. D., Contoreggi, C. et al. (2005). Risky decision making and the anterior cingulate cortex in abstinent drug abusers and nonusers. Cognitive Brain Research, 23, 119–136.
Forman, S. D., Dougherty, G. G., Casey, B. J., Siegle, G. J., Braver, T. S., Barch, D. M. et al. (2004). Opiate addicts lack error-dependent activation of rostral anterior cingulate. Biological Psychiatry, 55(5), 531–537.
Franken, I. H., Kroon, L. Y., Wiers, R. W., & Jansen, A. (2000). Selective cognitive processing of drug cues in heroin dependence. Journal of Psychopharmacology (Oxf), 14, 395–400.
Franklin, T. R., Acton, P. D., Maldjian, J. A., Gray, J. D., Croft, J. R., Dackis, C. A. et al. (2002). Decreased gray matter concentration in the insular, orbitofrontal, cingulate, and temporal cortices of cocaine patients. Biological Psychiatry, 51, 134–142.
Garavan, H. (1998). Serial attention within working memory. Memory & Cognition, 26(2), 263–276.
Garavan, H. & Stout, J. C. (2005). Neurocognitive insights into substance abuse. Trends in Cognitive Sciences, 9, 195–201.
Garavan, H., Ross, T. J., & Stein, E. A. (1999). Right hemispheric dominance of inhibitory control: An event-related fMRI study. Proceedings of the National Academy of Sciences, USA, 96(14), 8301–8306.
Garavan, H., Pankiewicz, J., Bloom, A., Cho, J.-K., Sperry, L., Ross, T. J., et al. (2000). Cue-induced cocaine craving: Neuroanatomical specificity for drug users and drug stimuli. American Journal of Psychiatry, 157, 1789–1798.
Garavan, H., Hester, R., Murphy, K., Fassbender, C., & Kelly, C. (2006). Individual differences in the neuroanatomy of inhibitory control. Brain Research, 1105, 130–142.
Gibbs, S. E., & D’Esposito, M. (2005). Individual capacity differences predict working memory performance and prefrontal activity following dopamine receptor stimulation. Cognitive, Affective & Behavioral Neuroscience, 5(2), 212–221.
Goldstein, R. Z., & Volkow, N. D. (2002). Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. American Journal of Psychiatry, 159, 1642–1652.
Goldstein, R. Z., Tomasi, D., Alia-Klein, N., Cottone, L. A., Zhang, L., Telang, F., et al. (2007a). Subjective sensitivity to monetary gradients is associated with frontolimbic activation to reward in cocaine abusers. Drug and Alcohol Dependence, 87(2–3), 233–240.
Goldstein, R. Z., Tomasi, D., Rajaram, S., Cottone, L. A., Zhang, L., Maloney, T., et al. (2007b). Role of the anterior cingulate and medial orbitofrontal cortex in processing drug cues in cocaine addiction. Neuroscience, 144, 1153–1159.
Grant, S., London, E. D., Newlin, D. B., Villemagne, V. L., Liu, X., Contoreggi, C., et al. (1996). Activation of memory circuits during cue-elicited cocaine craving. Proceedings of the National Academy of Sciences of the United States of America, 93, 12040–12045.
Grant, S., Contoreggi, C., & London, E. D. (2000). Drug abusers show impaired performance in a laboratory test of decision making. Neuropsychologia, 38, 1180–1187.
Guzy, L. T., & Axelrod, S. (1972). Interaural attention shifting as response. Journal of Experimental Psychology, 95, 290–294.
Hammer, R. P., Jr., Pires, W. S., Markou, A., & Koob, G. F. (1993). Withdrawal following cocaine self-administration decreases regional cerebral metabolic rate in critical brain reward regions. Synapse, 14(1), 73–80.
Hester, R., & Garavan, H. (2004). Executive dysfunction in cocaine addiction: Evidence for discordant frontal, cingulate and cerebellar activity. The Journal of Neuroscience, 24, 11017–11022.
Hester, R., Fassbender, C. & Garavan, H. (2004a). Individual differences in error processing: A review and meta-analysis of three event-related fMRI studies using the go/no-go task. Cerebral Cortex, 14(9), 966–973.
Hester, R., Murphy, K., & Garavan, H. (2004b). Beyond common resources: the cortical basis for resolving task interference. NeuroImage, 23(1), 202–212.
Hester, R., Dixon, V., & Garavan, H. (2006). The relationship between attentional bias for cocaine-related material and drug-seeking behavior in active cocaine users. Drug & Alcohol Dependence, 81, 251–257.
Hester, R, Simões-Franklin, C., & Garavan, H. (2007). Post-error behavior in active cocaine users: poor awareness of errors in the presence of intact performance adjustments. Neuropsychopharmacology (in press) DOI 10.1038/sj.npp.1301326.
Hoff, A. L., Riordan, H., Morris, L., Cestaro, V., Wieneke, M., Alpert, R. et al. (1996). Effects of crack cocaine on neurocognitive function. Psychiatry Research, 60(2–3), 167–176.
Holman, B. L., Carvalho, P. A,. Mendelson, J., Teoh, S. K., Nardin, R., Hallgring, E. et al. (1991). Brain perfusion is abnormal in cocaine-dependent polydrug users: a study using technetium-99m-HMPAO and ASPECT. Journal of Nuclear Medicine, 32(6), 1206–1210.
Holroyd, C. B., & Coles, M. G. H. (2002) The neural basis of human error processing: reinforcement learning, dopamine, and the error-related negativity. Psychological Review, 109, 679–709.
Hoshi, R., Bisla, J., & Curran, H. V. (2004). The acute and sub-acute effects of ‘ecstasy’ (MDMA) on processing of facial expressions: preliminary findings. Drug and Alcohol Dependence, 76, 297–304.
Hyman, S. E. (2005). Addiction: A disease of learning and memory. American Journal of Psychiatry, 162, 1414–1422.
Johanson, C. E. & Fischman, M. W. (1989). The pharmacology of cocaine related to its abuse. Pharmacology Review, 41(1), 3–52.
Kaufman, J., Ross, T. J., Stein, E. A., & Garavan, H. (2003). Cingulate hypoactivity in cocaine users during a go/no-go task as revealed by event-related fMRI. The Journal of Neuroscience, 23(21), 7839–7843.
Kelly, P. H., & Iversen, S. D. (1976). Selective 6OHDA-induced destruction of mesolimbic dopamine neurons: abolition of psychostimulant-induced locomotor activity in rats. European Journal of Pharmacology, 40(1), 45–56.
Konishi, S., Nakajima, K., Uchida, I., Kikyo, H., Kameyama, M., & Miyashita, Y. (1999). Common inhibitory mechanism in human inferior prefrontal cortex revealed by event-related functional MRI. Brain, 122, 981–991.
Kübler, A., Murphy, K., Kaufman, J., Stein, E. A., & Garavan, H. (2003). Co-ordination within and between verbal and visuospatial working memory: Network modulation and anterior frontal recruitment. NeuroImage, 20, 1298–1308.
Kübler, A., Murphy, K., & Garavan, H. (2005). Cocaine dependence and attention switching within and between verbal and visuospatial working memory. European Journal of Neuroscience, 21, 1984–1992.
Lawrence, N. S., Ross, T. J., & Stein, E. A. (2002). Cognitive mechanisms of nicotine on visual attention. Neuron, 36, 539–548.
Lee, T. M. C., Zhou, W., Luo, X., Yuen, K. S. L., Ruane, X., & Weng, X. (2005). Neural activity associated with cognitive regulation in heroin users: A fMRI study. Neuroscience Letters, 382, 211–216.
Li, C. s. R., Milivojevic, V., Kemp, K., Hong, K., & Sinha, R. (2006). Performance monitoring and stop signal inhibition in abstinent patients with cocaine dependence. Drug and Alcohol Dependence, 85(3), 205–212.
Liddle, P. F., Friston, K. J., Frith, C. D., Hirsch, S. R., Jones, T., & Frackowiak, R. S. (1992). Patterns of cerebral blood flow in schizophrenia. British Journal of Psychiatry, 160, 179–186.
Liddle, P. F., Kiehl, K. A., & Smith, A. M. (2001). Event-related fMRI study of response inhibition. Human Brain Mapping, 12(2), 100–109.
Logan G. D., & Cowan W. B. (1984). On the ability to inhibit thought and action: a theory of an act of control. Psychological Review, 91, 295–327.
Lusher, J., Chandler, C., & Ball, D. (2004). Alcohol dependence and the alcohol Stroop paradigm: Evidence and issues. Drug Alcohol Depend, 75, 225–231.
MacDonald, A. W. III, Cohen, J. D., Stenger, V. A., & Carter, C. S. (2000). Dissociating the role of the dorsolateral prefrontal and anterior cingulate cortex in cognitive control. Science, 288(5472), 1835–1838.
Magno, E., Foxe, J. J., Molholm, S., Robertson, I., & Garavan, H. (2006). The anterior cingulate and error avoidance. The Journal of Neuroscience, 26(18), 4769–4773.
Matochik, J. A., London, E. D., Eldreth, D. A., Cadet, J. L. & Bolla, K.I. (2003). Frontal cortical tissue composition in abstinent cocaine abusers: a magnetic resonance imaging study. Neuroimage, 19, 1095–1102.
Menon, V., Adleman, N. E., White, C. D., Glover, G. H., & Reiss, A. L. (2001). Error-related brain activation during a go/no-go response inhibition task. Human Brain Mapping, 12(3), 131–143.
Mogenson, G. J., Jones, D. L., & Yim, C. Y. (1980). From motivation to action: functional interface between the limbic system and the motor system. Progress in Neurobiology, 14(2–3), 69–97.
Monsell, S. (2003). Task switching. Trends in Cognitive Sciences, 7(3), 134–141.
Mostofsky, S. H., Schafer J. G., Abrams, M. T., Goldberg, M. C., Flower, A. A., Boyce, A., Courtney, S. M., Calhoun, V. D., Kraut, M. A., Denckla, M. B., & Pekar, J. J. (2003). fMRI evidence that the neural basis of response inhibition is task-independent. Cognitive Brain Research, 17, 419–430.
O'Malley, S. S., & Gawin, F. H. (1990). Abstinence symptomatology and neuropsychological impairment in chronic cocaine abusers. NIDA Research Monographs, 101, 179–190.
Ott, B.R., Lafleche, G., Whelihan, W. M., Buongiorno, G. W., Albert, M. S., & Fogel, B. S. (1996). Impaired awareness of deficits in Alzheimer disease. Alzheimer Disease and Associated Disorders, 10(2), 68–76.
Pascual-Leone, A., Dhuna, A., & Anderson, D. C. (1991). Cerebral atrophy in habitual cocaine abusers: A planimetric CT study. Neurology, 41(1), 34–38.
Paulus, M. P., & Lawrence, R. (2006). Anterior cingulate activity modulates nonlinear decision weight function of uncertain prospects. NeuroImage, 30, 668–677.
Paulus, M. P., Tapert, S. F., & Schuckit, M. A. (2005). Neural activation patterns of methamphetamine-dependent subjects during discussion making predict relapse. Archives of General Psychiatry, 62(7), 761–768.
Peralta, V., & Cuesta, M. J., (1998). Lack of insight in mood disorders. Journal of Affective Disorders, 49(1), 55–58.
Pope, H. G, Jr, Gruber, A. J., Hudson, J. I., Huestis, M. A., & Yurgelun-Todd, D. (2001) Neuropsychological performance in long-term cannabis users. Archives of General Psychiatry, 58, 195–909.
Porrino, L. J., Domer, F. R., Crane, A. M., & Sokoloff, L. (1998). Selective alterations in cerebral metabolism within the mesocorticolimbic dopaminergic system produced by acute cocaine administration in rats. Neuropsychopharmacology, 1(2), 109–118.
Rezvani, A. H., & Levin, E. D. (2001). Cognitive effects of nicotine. Biological Psychiatry, 49, 258–267.
Ridderinkhof, K. R., de Vlugt, Y., Bramlage, A., Spaan, M., Elton, M., Snel, J. et al. (2002). Alcohol consumption impairs detection of performance errors in mediofrontal cortex. Science, 298(5601), 2209–2211.
Ritz, M. C., Cone, E. J., & Kuhar, M. J. (1990). Cocaine inhibition of ligand binding at dopamine, norepinephrine and serotonin transporters: A structure-activity study. Life Sciences, 46(9), 635–645.
Robinson, T. E., & Berridge, K. C. (2003). Addiction. Annual Review of Psychology, 54, 25–53.
Rosselli, M. & Ardila, A. (1996). Cognitive effects of cocaine and polydrug abuse. Journal of Clinical and Experimental Neuropsychology, 18(1), 122–135.
Rubia, K., Smith, A. B., Brammer, M. J., & Taylor, E. (2003). Right inferior prefrontal cortex mediates response inhibition while mesial prefrontal cortex is responsible for error detection. NeuroImage, 20(1), 351–358.
Ryan, F. (2006). Appetite lost and found: Cognitive psychology in the addiction clinic. In M. Munafo & I. Albery (Eds.), Cognition and addiction. Oxford University Press: Oxford.
Schultz, W., Dayan, P., & Montague, P. R. (1997). A neural substrate of prediction and reward. Science, 275, 1593–1599.
Solowij, N., Stephens, R., Roffman, R. A., & Babor, T. (2002). Does marijuana use cause long-term cognitive deficits? JAMA, 287(20), 2653–2654.
Stout, J. C., Rock, S. L., Campbell, M. C., Busemeyer, J. R., & Finn, P. R. (2005). Psychological processes underlying risky decisions in drug abusers. Psychology of Addictive Behaviors, 19(2), 148–157.
Strickland, T. L., Mena, I., Villanueva-Meyer, J., Miller, B. L., Cummings, J., Mehringer, C. M. et al. (1993). Cerebral perfusion and neuropsychological consequences of chronic cocaine use. Journal of Neuropsychiatry and Clinical Neurosciences, 5(4), 419–427.
Tarter, R. E., Kirisci, L., Mezzich, A., Cornelius, J. R., Pajer, K., Vanyukov, M. et al. (2003). Neurobehavioral disinhibition in childhood predicts early age at onset of substance use disorder. American Journal of Psychiatry, 160, 1078–1085.
Teasdale, J. D., Moore, R. G., Hayhurst, H., Pope, M., Williams, S., & Segal, Z. V. (2002). Metacognitive awareness and prevention of relapse in depression: empirical evidence. Journal of Consulting and Clinical Psychology, 70(2), 275–287.
Volkow, N. D., Fowler, J. S, Wolf, A. P, Hitzemann, R., Dewey, S., Bendriem, B. et al. (1991). Changes in brain glucose metabolism in cocaine dependence and withdrawal. American Journal of Psychiatry, 148(5), 621–626.
Volkow, N. D., Hitzemann, R., Wang, G. J., Fowler, J. S., Wolf, A. P., Dewey, S. L. et al. (1992). Long-term frontal brain metabolic changes in cocaine abusers. Synapse, 11(3), 184–190.
Volkow, N. D., Fowler, J. S., Wang, G.-J., Hitzemann, R., Logan, J., Schlyer, D. et al. (1993). Decreased dopamine D2 receptor availability is associated with reduced frontal metabolism in cocaine abusers. Synapse, 14, 169–177.
Volkow, N. D., Wang, G.-J., Fowler, J. S., Logan, J., Gatley, S. J., Gifford, A. et al. (1999). Prediction of reinforcing responses to psychostimulants in humans by brain dopamine D2 receptor levels. American Journal of Psychiatry, 156, 1440–1443.
Waters, A. J., Shiffman, S., Sayette, M. A., Paty, J. A., Gwaltney, C. J., & Balabanis, M. H. (2003). Attentional bias predicts outcome in smoking cessation. Health Psychol, 22, 378–387.
Wertz, J. M., & Sayette, M. A. (2001). Effects of smoking opportunity on attentional bias in smokers. Psychology of Addictive Behaviors, 15, 268–271.
Wrase, J. Schlagenhauf, F., Kienast, T., Wustenberg, T., Bermpohl, F., Kahnt, T. et al. (2007). Dysfunction of reward processing correlates with alcohol craving in detoxified alcoholics. NeuroImage, 35(2), 787–794.
Yucel, M., & Lubman, D. I. (2007). Neurocognitive and neuroimaging evidence of behavioral dysregulation in human drug addiction: implications for diagnosis, treatment and prevention. Drug and Alcohol Review, 26, 33–39.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Garavan, H., Hester, R. The Role of Cognitive Control in Cocaine Dependence. Neuropsychol Rev 17, 337–345 (2007). https://doi.org/10.1007/s11065-007-9034-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11065-007-9034-x