
Abstract
Rationale
A growing body of evidence suggests that gambling frequently co-occurs with smoking, yet little is known about the degree to which nicotine and/or tobacco use influences gambling behavior. Nonetheless, an increasing number of studies suggest that acute administration of nicotine may alter other reinforcing behaviors in both animal and human models, raising the possibility that nicotine may also influence gambling behavior and craving.
Objectives
The purpose of this study was to examine the acute effects of nicotine on subjective and behavioral gambling responses.
Methods
Twenty-eight (15 male) regular gamblers who smoke daily completed two double-blind laboratory sessions where their subjective and behavioral responses to video lottery terminal (VLT) gambling were assessed, following the administration of nicotine inhalers (NI; 4 mg deliverable) or placebo inhalers.
Results
NI significantly decreased tobacco-related cravings (p < 0.05) but did not affect gambling-related cravings, VLT betting patterns, or subjective responses (ps > 0.1).
Conclusions
NI were found to acutely suppress tobacco-related cravings without influencing gambling. These results suggest that use of nicotine replacement therapies may be a safe option for gamblers who are attempting to quit smoking.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
An accumulating body of evidence has established the frequent co-occurrence of tobacco use and gambling (McGrath and Barrett 2009). Smoking is especially prevalent among pathological gamblers (PGs), with North American epidemiological investigations suggesting rates of nicotine dependence in the range of 41% (Smart and Ferris 1996) to 60% (Cunningham-Williams et al. 1998). Research also indicates that tobacco-using PGs experience stronger urges to gamble (Grant and Potenza 2005), are more likely to be dependent on other substances (Cunningham-Williams et al. 1998), and are more likely to experience psychosocial problems (Petry and Oncken 2002) than non-smoking PGs. Despite high rates of co-occurrence and associated psychological difficulties, little attention has been directed toward disentangling the relationship between smoking and gambling.
Currently, there is sparse evidence to indicate that nicotine directly effects gambling behavior; however, a number of recent research findings suggest that nicotine may alter processes that are involved in gambling. For instance, Businelle et al. (2009) found that heavy smokers performed more poorly than never smokers on the Gambling Task (GT; Bechara et al. 1994; Bechara et al. 2000), a decision-making task which contains choice, rewards, and negative outcomes. This finding suggests that heavy smokers on average preferred short-term rewards at the expense of sustaining longer-term losses. There is also evidence to indicate that smokers perform more poorly on tasks measuring impulsivity such as delay and probability discounting procedures. For example, a number of recent studies have found that compared to non-smokers, smokers on average tend to discount real and hypothetical rewards at a significantly higher rate (e.g., Bickel et al. 1999; Ohmura et al. 2005; Reynolds 2004). Problem gamblers also display higher rates of delay discounting compared to non-gamblers (Petry and Casarella 1999; Petry 2001), and it has been suggested that other substance use/abuse may additively contribute to rates of delay discounting among problem gamblers (Reynolds 2006). While these studies suggest that smokers and non-smokers differ in their responses, the extent to which these differences are due to nicotine per se is not known. However, there is growing evidence from animal models that nicotine may have direct reinforcement-enhancing effects (Chaudhri et al. 2006). In rats, both contingent and noncontingent nicotine can enhance the reinforcement value of lever pressing to visual stimuli through non-associative mechanisms (e.g., Chaudhri et al. 2007; Donny et al. 2003; Palmatier et al. 2006). Additionally, larger doses of nicotine are associated with higher rates of responding to a stimulus (i.e., light) that was previously paired with nicotine than lower doses (Palmatier et al. 2008). Studies into the effects of nicotine on reinforced behaviors in humans are less conclusive. In a series of experiments, overnight tobacco-abstinent smokers displayed reduced responsiveness to a card-sorting test that was paired with a financial incentive when compared to a non-abstinent condition (Al-Adawi and Powell 1997; Powell et al. 2002). Similarly, smokers in a nicotine lozenge condition exhibited greater responsiveness to a card-sorting test over a placebo (Dawkins et al. 2006). Barr et al. (2008) also reported that non-smokers who wore nicotine patches demonstrated increased responding toward a more rewarding stimulus (e.g., positive cues, monetary reward) than those given placebo. However, in a recent study of non-dependent smokers, nicotine administered via nasal spray or cigarette did not significantly increase the number of responses for money, music, or the removal of an aversive stimulus (Perkins et al. 2009). The aggregate findings from these human experiments are mixed. While most suggest that nicotine may influence processes directly involved in gambling, others do not support this notion.
In the present study, we examined the potential for nicotine to influence video lottery terminal (VLT) gambling. Given the influence of operant conditioning processes in the maintenance of electronic gaming (Delfabbro and Winefield 1999), VLT gambling represents a common and externally valid form of conditioned behavior. Daily smokers who regularly gamble on slot machines/VLTs were recruited for a within-subjects study involving nicotine inhaler (NI) and placebo inhaler (PI) conditions. Based on previous animal and human findings, it was predicted that nicotine would augment VLT gambling over placebo, as indexed by subjective ratings (e.g., gambling craving) and observable gambling behavior.
Methods
Participants
Participants were 28 (15 males) regular VLT gamblers (i.e., VLT gambling at least once per month for past 3 months) who smoked daily and were at least 19 years of age or older (M = 37.5 years; SD = 13.1). The sample reported smoking an average of 13.9 (SD = 5.8) cigarettes per day (ranging from 4 to 25) and had a mean Fagerström Test for Nicotine Dependence (FTND; Heatherton et al. 1991) score of 4.1 (SD = 1.6) with scores ranging from 1–7. The FTND (Heatherton et al. 1991) is designed to measure nicotine dependence with a score of 6 or greater indicating a “high” level of dependence. It has been found to possess strong psychometric properties including good internal consistency (α = 0.72) and high test–retest reliability over a 6-week period (r = 0.91) among regular smokers (see Meneses-Gaya et al. 2009 for a review). Average score on the South Oaks Gambling Screen (SOGS; Lesieur and Blume 1987) in the sample was 5.3 (SD = 4.9) with a range of 0–19. A score of 5 or more indicates a “probable pathological gambler”. The SOGS is a commonly used instrument to assess pathological gambling severity that has good internal consistency (α = 0.97), test–retest reliability over a 4-week period (r = 0.71), and convergent validity with the DSM-III-R (American Psychiatric Association [APA], 1987) pathological gambling criteria (r = 0.94) (Lesieur and Blume 1987). Lastly, all participants were compensated $20 CAD per session plus any amount won while gambling.
Measures
Visual analog scales
Used to measure subjective state, the visual analog scales (VAS) (Bond and Lader 1974) contained seven items: “confident”, “intoxicated”, “bored”, “high”, “unsure”, “crave cigarette”, and “want to play VLT”. Each item was rated from 1 = “not at all” to 10 = “extremely”, with participants asked to rate their current feelings. Similar scales have been used in previous studies of drug impacts on gambling (e.g., Zack and Poulos 2004).
Post-VLT play questionnaire
This short author-compiled multi-item questionnaire was used to assess enjoyment/excitement from gambling and desire to continue gambling. Three items were of interest in this study (e.g., “did you enjoy the game you just played?”), with each measured on a scale from 1 = “not at all” to 7 = “absolutely”.
Apparatus
Inhalers
Nicotine was administered via inhalers (10 mg; 4 mg deliverable, Pharmacia, Mississauga, Ontario, Canada) flavored with menthol spray. Placebo inhalers contained a pharmacologically inert substance sprayed with menthol. In both conditions, inhalers were administered at a rate of one deep inhalation every 10 s for 20 consecutive minutes, totalling 120 puffs. In their review of the nicotine inhaler, Schneider et al. (2001) report that a nicotine inhaler puffed 80 times for 20 min results in an average plasma nicotine concentration of 8.1 μg/L at 30 min following the start of inhaler administration. In the current study, VLT gambling was initiated approximately 30 min after the beginning of inhaler administration. The decision to use inhalers over other forms of nicotine administration was influenced by their tolerability and similarity to cigarettes on sensory-motor qualities and method of administration (Schneider et al. 2005).
VLTs
Gambling occurred on authentic VLTs (i.e., identical to those in the marketplace) provided by the Atlantic Lotto Corporation and the Nova Scotia Gaming Corporation. The VLTs were located in a “bar-lab” decorated to resemble a real-world VLT gambling environment (see Stewart et al. 2000 for a more detailed description). Participants were provided with $60 CAD to gamble. VLT play was limited to one spinning reels game (i.e., Royal Spins) to ensure a similar gambling experience for all participants in both conditions (Ellery et al. 2005). However, in an effort to increase external validity, restrictions on gambling play were minimized wherever possible. Participants could place any size bet per spin (ranging from 5 cents to $2.50) and could play the VLT for as long as they wished for up to 30 min. Single wagers of $2.50 via a single button press constitute a maximum bet. The amount spent per bet and the number of spins was recorded by the experimenter who was seated behind the participant out of view. Printouts provided by the VLT machine recorded the total amount played and the total amount won/lost per session. The average number of bets per minute, total dollars played on the VLT, average bet size, and the average number of maximum bets were examined in this study. Any amount won by participants (or remaining from the initial $60) was paid out at the end of the experimental session.
Heart rate monitor
A heart rate monitor (Polar Electro Canada Inc., Lachine, QC) was used to measure average heart rate (HR). The monitor was strapped to the participant’s chest and the average number of beats was recorded over a 3-min interval for each individual measurement period. HR recordings have been used in previous VLT studies to record physiological changes from baseline following a drug challenge (e.g., Stewart et al. 2005; Stewart et al. 2006).
Procedure
Participants were community recruited from the Halifax Regional Municipality, Nova Scotia. The experiment included two double-blind sessions completed during the morning (M = 5.7, SD = 6.5 days apart), with each participant taking part in counter-balanced NI and PI conditions. For each session, 12-h overnight tobacco abstinence was verbally confirmed at the outset of the session and verified with a breath carbon monoxide (CO) reading of less than 20 ppm (Vitalograph Breath CO, Lenexa, KS). This cutoff was chosen based on recommendations for verifying overnight abstinence outlined by the Society for Research on Nicotine and Tobacco (SRNT) Subcommittee on Biochemical Verification (Benowitz et al. 2002). The CO readings were found to range from 1 to 19 ppm in both the NI (M = 8.9, SD = 4.6) and PI (M = 7.6, SD = 4.4) conditions. Following informed consent (first session), the experiment began. Participants first completed a questionnaire packet of baseline subjective measures (T1) and the first heart rate reading was recorded (average over 3 min). Next, the inhaler (NI or PI) was administered with inhalation occurring every 10 s for 20 consecutive minutes. A second HR reading was taken during the first 3 min of inhaler administration and a second measures package was completed (T2). Upon completion of the measures, participants were brought to the VLT laboratory where they were provided with $60 CAD and permitted to play a VLT for up to 30 min. A third HR reading was taken during the start of VLT play, and another measures package was completed after 15 min of VLT play (T3). The final HR reading was taken after 15 min of VLT play and the last measures package was completed at the end of VLT play (T4). Participants were then debriefed on the nature of the experiment (following the second session) and compensated for their time.
Data analyses
Analyses were conducted using SPSS Version 15 (Chicago, Illinois, USA). Dependent variables were: VAS ratings, average HR, post-VLT ratings, and betting patterns (i.e., average number of bets per minute, total dollars played on the VLT, average bet size, average number of maximum bets). Mixed modeling was used to analyze the data with pharmacology (NI, PI) and time [following inhaler administration (T2), during VLT play (T3), and post-VLT play (T4)] entered as fixed and repeated factors, respectively; sex was entered as a fixed factor, and pre-administration baseline scores (T1) were entered as a time-varying covariate. No analyses involving time were conducted for post-VLT ratings or betting patterns as only a single measurement was taken per testing session. Covariance structures were selected on the basis of model simplicity and the likelihood ratio test (West 2009). For VAS items and HR, interactions of pharmacology with time were the outcomes of interest. For the post-VLT play questionnaire and VLT betting patterns, main effects of pharmacology were the outcomes of interest.
Results
Visual analog scales
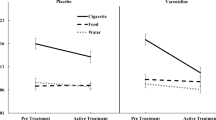
There was a significant interaction of pharmacology × time on ratings of “crave cigarette”, F (3, 22) = 3.85, p = 0.02, indicating lower craving in the NI condition relative to the PI condition at T2 and T3 (following inhaler and during VLT play) and a similar marginal effect (p = 0.06) at T4 (post-VLT play) (see Fig. 1a). There was no significant interaction of pharmacology × time for ratings of “want to play VLT”, F (3, 27) = 1.60, p = 0.21 (see Fig. 1b). Similarly, no interactions of pharmacology × time were found for ratings of “confident” F (3, 25) = 1.62, p = 0.21, “intoxicated” F (3, 28) = 0.74, p = 0.54, “bored” F (3, 28) = 2.18, p = 0.11, “high” F (3, 24) = 0.84, p = 0.49, or “unsure” F (3, 28) = 2.29, p = 0.10. There were no significant interactions involving sex for any of the VAS measures.

Unadjusted mean ratings for VAS item “crave cigarette”, and VAS item “want to play VLT” for nicotine inhaler (NI) and placebo inhaler (PI) conditions at: baseline (T1); following inhaler administration (T2); during VLT play (T3); and post-VLT play (T4). Baseline values were used as time-varying covariates. Bars represent standard errors (SE). NI reduced ratings for “crave cigarette” at T2, T3, and T4 relative to PI. No differences were observed between NI and PI at any time point on ratings for “want to play VLT”
Post-VLT play questionnaire
No significant differences were found between NI (M = 4.94, SE = 0.35) and PI (M = 4.70, SE = 0.35) on ratings of “enjoy the VLT game”, F (1, 55) = 0.22, p = 0.64. Similarly, no differences were found between NI (M = 4.32, SE = 0.35) and PI (M = 4.29, SE = 0.35) on ratings of “the VLT was exciting”, F (1, 55) = 0.01, p = 0.96. Finally, no significant differences between NI (M = 4.21, SE = 0.36) and PI (M = 3.88, SE = 0.37) were found for “the VLT reduced tensions/worries”, F (1, 55) = 0.39, p = 0.54. The interactions of pharmacology × sex were not significant for any of the three post-VLT play questions.
Betting patterns
An examination of the average number of bets per minute suggests that NI (M = 8.78, SE = 0.47) and PI (M = 8.87, SE = 0.47) did not significantly differ, F (1, 56) = 0.18, p = 0.89. For dollars spent gambling, no significant differences were found between NI (M = $105.99, SE = 12.38) and PI (M = $100.28, SE = 12.38), F (1, 56) = 0.11, p = 0.75. Also, there were no significant differences between NI (M = $0.99, SE = 0.24) and PI (M = $0.61, SE = 0.24) on average bet size, F (1, 56) = 1.19, p = 0.28. Lastly, no differences were found for average number of maximum bets between the NI (M = 5.91, SE = 2.70) and PI (M = 4.99, SE = 2.70) conditions, F (1, 56) = 0.06, p = 0.81. No significant main or interaction effects of sex were observed for any of the indices of betting patterns.
Heart rate
There was a significant interaction of pharmacology × time on average HR, F (3, 28) = 8.57, p = 0.01. Average HR in the NI condition was higher than the PI condition at T2 (following inhaler) [M = 74.53 (SE = 0.72) vs. M = 73.07(SE = 0.57), p = 0.03], T3 (following inhaler and during VLT play) [M = 78.93 (SE = 0.74) vs. M = 74.73 (SE = 0.80), p = 0.01], and T4 (post-VLT play) [M = 76.70 (SE = 1.13) vs. M = 72.82 (SE = 0.79), p = 0.01]. Thus, significant effects of inhaler condition were present at all three time points (HR greater in NI than PI) although the effects were somewhat stronger during and following VLT play relative to post-inhalation/pre-VLT play. There were no significant interactions involving sex.
Tests for the presence of order effects
Although our two experimental sessions were counter-balanced, we examined whether a participant’s gambling “strategy” in the second session may have been influenced by the results of their first gambling session. Specifically, we re-examined the VAS item that reached significance, the HR index, and VLT betting patterns by including “session received nicotine” as a between-subjects variable. For “crave cigarette”, the interaction of pharmacology × time remained significant [F (3, 22) = 3.54, p = 0.03], and the interaction of pharmacology × time× session was not significant [F (3, 23) = 1.32, p = 0.29]. Similarly, for average HR, the interaction of pharmacology × time remained significant [F (3, 28) = 9.44, p = 0.01], and the interaction of pharmacology × time × session was not significant [F (3, 29) = 2.43, p = 0.09]. These results indicate that no order effects were present for either variable. In terms of VLT practice effects, no main effects were found for “session received nicotine” on: average number of bets per minute [F (1, 56) = 2.52, p = 0.12], dollars spent gambling [F (1, 56) = 0.15, p = 0.70], average bet size [F (1, 56) = 0.18, p = 0.67], or number of maximum bets [F (1, 56) = 2.99, p = 0.09]. These results suggest that no order effects were present for any of the betting patterns of interest.
Discussion
The present study examined the effect of nicotine on subjective and objective measures of gambling behavior in smokers. No differences were found between the NI and PI conditions on most VAS items including “want to play VLT”. Similarly, NI and PI did not differ on post-VLT ratings: “enjoy the VLT game”, “the VLT was exciting”, or “playing the VLT reduced tensions/worries”. Moreover, no differences between NI and PI were evident for VLT betting patterns including average number of bets per minute, amount spent, average bet size, and number of maximum bets. Thus, contrary to predictions, the aggregate of these results indicate that acute administration of nicotine does not augment craving for gambling or VLT gambling behavior.
Nicotine decreased subjective cigarette cravings to a greater extent than placebo. Participants in the study were required to abstain from tobacco for the duration of both study sessions. Evidence suggests that receiving nicotine replacement therapy (NRT) during tobacco abstinence reduces craving and withdrawal (e.g., Schneider et al. 2008; Shiffman et al. 2006). Our results indicate that NI can reduce cigarette cravings without influencing VLT gambling, suggesting that NRTs may be an efficacious and safe option for gamblers who wish to quit smoking. This potential benefit warrants further consideration.
One possible reason for the lack of effects of nicotine on gambling could be the high incentive value of VLT gambling itself. That is, unlike other reinforced behavior (e.g., card sorting tasks) which could be considered to have low incentive value, the already strong incentive value of gambling (at least among regular gamblers) may not be further enhanced by substances such as nicotine. While conceivable, there is evidence to suggest that nicotine does enhance craving for other addictive behaviors. For instance, Reid et al. (1998) examined the extent to which acute nicotine (vs. placebo) delivered via transdermal patch impacted craving following exposure to cocaine cues in individuals with a history of smoking crack cocaine. While all participants reported an increase in cocaine craving and changes in physiological measures (e.g., skin conductance) following cue exposure, craving was strongly enhanced by nicotine. In addition, previous studies conducted in our lab indicate that VLT gambling may also be sensitive to alcohol manipulations. For example, Stewart et al. (2005) examined heart rate responses to VLT play between an alcohol condition and a control beverage condition. They found that those in the alcohol condition exhibited increased heart rate from predrinking to VLT play relative to controls. Similarly, Ellery et al. (2005) assigned non-pathological and probable pathological gamblers to either an alcohol dose condition or a non-alcoholic control beverage condition and had them play a VLT video poker game. They found that probable pathological gamblers in the alcohol condition spent more time playing the VLT and had a higher rate of power betting (doubling a bet after seeing two cards of the five card poker hand) than those in the control condition. No differences were found for either behaviour among non-pathological gamblers in the alcohol and control conditions. These studies suggest that the VLT behavioral assay is sensitive to pharmacological challenges. Nevertheless, future work looking at nicotine’s impact on gambling would benefit from the inclusion of a neutral (non-gambling) control condition (e.g., Wulfert et al. 2009) to rule out the possibility that the lack of effects of nicotine on gambling in the present study was due to the high incentive value of VLT gambling.
The study has some limitations. First, the degree to which nicotine alters real-world gambling compared to laboratory-based gambling remains unclear. This experiment placed limits on the amount that could be spent and time available to gamble—constraints that do not exist in everyday gambling. However, previous findings suggest that lab-based gambling can serve as a valid analog when real-world cues (e.g., real VLTs) are provided (see review by Stewart and Jefferson 2007). In addition, the gambling frequency inclusion criteria of playing “VLT games” at least once per month for past 3 months may have been too liberal. It is unclear if our results would generalize to heavier VLT use (e.g., daily or weekly use) or to clinical populations of gamblers. Next, the participants included in the study were daily smokers. There is evidence to suggest that nicotine elimination is slow in regular smokers and nicotine can remain in body tissues for up to several days during abstinence (see Matta et al. 2007). While we exceeded the 8 h of overnight tobacco abstinence recommended for in vivo studies (Matta et al. 2007), it is possible that chronic tolerance to nicotine affected subjective craving to gamble in our pharmacological conditions. Additionally, although the sample was comprised of daily smokers, the relatively low average number of cigarettes smoked per day (M = 13.9, SD = 5.8) and relatively low FTND scores (Heatherton et al. 1991) (M = 4.1, SD = 1.6) suggest that most participants were moderately dependent smokers, and it is possible that more robust effects would have been observed in a sample of more heavy/highly dependent smokers. Moreover, due to the slow overnight elimination of CO (Benowitz et al. 2002) and the early morning scheduling of the experimental sessions, the maximum CO cutoff to verify abstinence was set at 20 ppm. While all participants also verbally confirmed abstinence at the start of each session, this CO cutoff is likely inadequate to verify abstinence in light smokers. The current study also relied solely on one method of nicotine delivery—the inhaler. The inhaler was designed to “wean” smokers off of nicotine (Schneider et al. 2001) and produces lower acute blood nicotine levels compared to other methods of nicotine delivery such as lozenges (McEwen et al. 2008). Future work should attempt to replicate our methodology with other forms of NRT that produce more rapid increases in blood nicotine levels. Lastly, nicotine was acutely administered in this study, whereas NRT is typically used over a longer time period. It is uncertain how prolonged NRT use would impact gambling.
In conclusion, acute administration of nicotine via inhaler did not impact gambling cravings or betting behavior. Nicotine did, however, reduce subjective craving for cigarettes and increase heart rate. These findings suggest that use of NRTs may be appropriate for gamblers attempting to quit smoking.
References
Al-Adawi S, Powell J (1997) The influence of smoking on reward responsiveness and cognitive functions: a natural experiment. Addiction 92:1773–1782. doi:10.1046/j.1360-0443.1997.9212177318.x
American Psychiatric Association (1987) Diagnostic and statistical manual of mental Disorders, third edition—revised (DSM-III-R). APA, Washington
Barr RS, Pizzagalli DA, Culhane MA, Goff DC, Evins AE (2008) A single dose of nicotine enhances reward responsiveness in nonsmokers: implications for development of dependence. Biol Psychiatry 63:1061–1065. doi:10.1016/j.biopsych.2007.09.015
Bechara A, Damasio AR, Damasio H, Anderson SW (1994) Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 50:7–15. doi:10.1016/0010-0277(94)90018-3
Bechara A, Tranel D, Damasio H (2000) Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain 123:2189–2202. doi:10.1093/brain/123.11.2189
Benowitz NL, Jacob P III, Ahijevych K, Jarvis MJ, Hall S, LeHouezec J, Velicer W (2002) Biochemical verification of tobacco use and cessation. Nicotine Tob Res 4:149–159. doi:10.1080/14622200210123581
Bickel WK, Odum AL, Madden GJ (1999) Impulsivity and cigarette smoking: delay discounting in current, never, and ex-smokers. Psychopharmacology 146:447–454. doi:10.1007/PL00005490
Bond A, Lader M (1974) The use of analogue scales in rating subjective feelings. Br J Med Psychol 47:211–218
Businelle MS, Kendzor DE, Rash CJ, Patterson SM, Coffey SF, Copeland AL (2009) Heavy smokers perform more poorly than nonsmokers on a simulated task of gambling. Subst Use Misuse 44:905–914. doi:10.1080/10826080802484173
Chaudhri N, Caggiula AR, Donny EC, Palmatier MI, Liu X, Sved AF (2006) Complex interactions between nicotine and nonpharmacological stimuli reveal multiple roles for nicotine in reinforcement. Psychopharmacology 184:353–366. doi:10.1007/s00213-005-0178-1
Chaudhri N, Caggiula AR, Donny EC, Booth S, Gharib M, Craven L, Palmatier MI, Liu X, Sved AF (2007) Self-administered and noncontingent nicotine enhance reinforced operant responding in rats: impact of nicotine dose and reinforcement schedule. Psychopharmacology 190:353–362. doi:10.1007/s00213-006-0454-8
Cunningham-Williams RM, Cottler LB, Compton WM, Spitznagel EL (1998) Taking chances: problem gamblers and mental health disorders: results from the St Louis Epidemiologic Catchment Area study. Am J Public Health 88:1093–1096. doi:10.2105/AJPH.88.7.1093
Dawkins L, Powell JH, West R, Powell J, Pickering A (2006) A double-blind placebo controlled experimental study of nicotine: I—effects on incentive motivation. Psychopharmacology 189:355–367. doi:10.1007/s00213-006-0588-8
Delfabbro PH, Winefield AH (1999) Poker-machine gambling: an analysis of within session characteristics. Br J Psychol 90:425–439. doi:10.1348/000712699161503
Donny EC, Chaudhri N, Caggiula AR, Evans-Martin FF, Booth S, Gharib MA, Clements LA, Sved AF (2003) Operant responding for a visual reinforcer in rats is enhanced by noncontingent nicotine: implications for nicotine self-administration and reinforcement. Psychopharmacology 169:68–76. doi:10.1007/s00213-003-1473-3
Ellery M, Stewart SH, Loba P (2005) Alcohol’s effects on video lottery terminal (VLT) play among probable pathological and non-pathological gamblers. J Gambl Stud 21:299–324. doi:10.1007/s10899-005-3101-0
Grant JE, Potenza MN (2005) Tobacco use and pathological gambling. Ann Clin Psychiatry 17:237–241. doi:10.1080/10401230500295370
Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO (1991) The Fagerström Test for nicotine dependence: a revision of the Fagerström Tolerance Questionnaire. Br J Addict 86:1119–1127. doi:10.1111/j.1360-0443.1991.tb01879.x
Lesieur HR, Blume SB (1987) South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. Am J Psychiatry 144:1184–1188
Matta SG, Balfour DJ, Benowitz NL et al (2007) Guidelines on nicotine dose selection for in vivo research. Psychopharmacology 190:269–319. doi:10.1007/s00213-006-0441-0
McEwen A, West R, Gaiger M (2008) Nicotine absorption from seven current nicotine replacement products and a new wide-bore nicotine delivery device. J Smoking Cess 3:117–123. doi:10.1375/jsc.3.2.117
McGrath DS, Barrett SP (2009) The comorbidity of tobacco smoking and gambling: a review of the literature. Drug Alcohol Rev 28:676–681. doi:10.1111/j.1465-3362.2009.00097.x
Meneses-Gaya IC, Zuardi AW, Loureiro SR, Crippa JA (2009) Psychometric properties of the Fagerström Test for Nicotine Dependence. J Bras Pneumol 35:73–82
Ohmura Y, Takahashi T, Kitamura N (2005) Discounting delayed and probabilistic monetary gains and losses by smokers of cigarettes. Psychopharmacology 182:508–515. doi:10.1007/s00213-005-0110-8
Palmatier MI, Evans-Martin FF, Hoffman A, Caggiula AR, Chaudhri N, Donny EC, Liu X, Booth S, Gharib M, Craven L, Sved AF (2006) Dissociating the primary reinforcing and reinforcement-enhancing effects of nicotine using a rat self-administration paradigm with concurrently available drug and environmental reinforcers. Psychopharmacology 184:391–400. doi:10.1007/s00213-005-0183-4
Palmatier MI, Coddington SB, Liu X, Donny EC, Caggiula AR, Sved AF (2008) The motivation to obtain nicotine-conditioned reinforcers depends on nicotine dose. Neuropharmacology 55:1425–1430. doi:10.1016/j.neuropharm.2008.09.002
Perkins KA, Grottenthaler A, Wilson AS (2009) Lack of reinforcement enhancing effects of nicotine in non-dependent smokers. Psychopharmacology 205:635–645. doi:10.1007/s00213-009-1574-8
Petry NM (2001) Pathological gamblers, with and without substance use disorders, discount delayed rewards at high rates. J Abnorm Psychol 110:482–487. doi:10.1037/0021-843X.110.3.482
Petry NM, Casarella T (1999) Excessive discounting of delayed rewards in substance abusers with gambling problems. Drug Alcohol Depend 56:25–32. doi:10.1016/S0376-8716(99)00010-1
Petry NM, Oncken C (2002) Cigarette smoking is associated with increased severity of gambling problems in treatment-seeking gamblers. Addiction 97:745–753. doi:10.1046/j.1360-0443.2002.00163.x
Powell J, Dawkins L, Davis RE (2002) Smoking, reward responsiveness, and response inhibition: tests of an incentive motivation model. Biol Psychiatry 51:151–163. doi:10.1016/S0006-3223(01)01208-2
Reid M, Mickalian J, Delucchi K, Hall S, Berger S (1998) An acute dose of nicotine enhances cue-induced cocaine craving. Drug Alcohol Depen 49:95–104. doi:10.1016/S0376-8716(97)00144-0
Reynolds B (2004) Do high rates of cigarette consumption increase delay discounting? A cross-sectional comparison of adolescent smokers and young-adult smokers and nonsmokers. Behav Processes 67:545–549. doi:10.1016/j.beproc.2004.08.006
Reynolds B (2006) A review of delay-discounting research with humans: relations to drug use and gambling. Behav Pharmacol 17:651–667. doi:10.1097/FBP.0b013e3280115f99
Schneider NG, Olmstead RE, Franzon MA, Lunell E (2001) The nicotine inhaler: clinical pharmacokinetics and comparison with other nicotine treatments. Clin Pharmacokinet 40:661–684
Schneider NG, Terrace S, Koury MA, Patel S, Vaghaiwalla B, Pendergrass R, Olmstead RE, Cortner C (2005) Comparison of three nicotine treatments: initial reactions and preferences with guided use. Psychopharmacology 182:545–550. doi:10.1007/s00213-005-0123-3
Schneider NG, Cortner C, Gould JL, Koury MA, Olmstead RE (2008) Comparison of craving and withdrawal among four combination nicotine treatments. Hum Psychopharmacol 23:513–517. doi:10.1002/hup.947
Shiffman S, Ferguson SG, Gwaltney CJ, Balabanis MH, Shadel WG (2006) Reduction of abstinence-induced withdrawal and craving using high-dose nicotine replacement therapy. Psychopharmacology 184:637–644. doi:10.1007/s00213-005-0184-3
Smart RG, Ferris J (1996) Alcohol, drugs and gambling in the Ontario adult population, 1994. Can J Psychiatry 41:36–45
Stewart SH, Jefferson S (2007) Experimental methodologies in gambling studies. In: Smith G, Hodgins DC, Williams RJ (eds) Research and measurement issues in gambling studies. Elsevier, New York, pp 87–110
Stewart SH, Blackburn JR, Klein RM (2000) Against the odds: establishment of a video lottery terminal research laboratory in a naturalistic setting. Nova Scotia Psychologist 11:3–6
Stewart SH, Collins P, Blackburn JR, Ellery M, Klein RM (2005) Heart rate increase to alcohol administration and video lottery terminal (VLT) play among regular VLT players. Psychol Addict Behav 19:94–98. doi:10.1037/0893-164X.19.1.94
Stewart SH, Peterson JB, Collins P, Eisner S, Ellery M (2006) Heart rate increase to alcohol administration and video lottery terminal (VLT) play among probable pathological gamblers and non-pathological gamblers. Psychol Addict Behav 20:53–61. doi:10.1037/0893-164X.20.1.53
West BT (2009) Analyzing longitudinal data with the linear mixed models procedure in SPSS. Eval Health Prof 32:207–228. doi:10.1177/0163278709338554
Wulfert E, Maxson J, Jardin B (2009) Cue-specific reactivity in experienced gamblers. Psychol Addict Behav 23:731–735. doi:10.1037/a0017134
Zack M, Poulos CX (2004) Amphetamine primes motivation to gamble and gambling-related semantic networks in problem gamblers. Neuropsychopharmacology 29:195–207. doi:10.1038/sj.npp.1300333
Acknowledgments
The authors would like to acknowledge Lyndsay Bozec’s assistance with participant recruitment and phone screening. This work was supported by student research grants awarded to Daniel McGrath from the Canadian Tobacco Control Research Initiative and Gambling Awareness Nova Scotia. Daniel McGrath was funded by studentships from the Nova Scotia Health Research Foundation and the Ontario Problem Gambling Research Centre during the completion of this research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McGrath, D.S., Barrett, S.P., Stewart, S.H. et al. The effects of acute doses of nicotine on video lottery terminal gambling in daily smokers. Psychopharmacology 220, 155–161 (2012). https://doi.org/10.1007/s00213-011-2465-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-011-2465-3