
Abstract
Rationale
Given the hypothesised association between cannabis use and schizophrenia, and the well documented alterations in pre-pulse inhibition (PPI) that are observed in schizophrenia, it is of interest to examine the effects of cannabis use on PPI.
Objective
The objective of the study was to use novel methodology for the measurement and characterisation of attentional modulation of PPI, in order to examine the nature of PPI in chronic cannabis users.
Methods
PPI was measured in 34 chronic cannabis users (who were otherwise healthy) and 32 healthy controls, across a range of startling stimulus intensities, during two attention set conditions, one in which they were instructed to attend to the auditory stimuli and one in which they were instructed to ignore the auditory stimuli and focus on a visual task. Curves of best fit were fitted to the startle magnitudes, across the stimulus intensities. A number of reflex parameters were extracted from these logistic functions, each of which reflects a different characteristic of the startle response.
Results
Cannabis users failed to show attentional modulation of any of the reflex parameters and showed altered PPI, relative to controls, but only when they were instructed to sustain attention to the auditory stimuli.
Conclusion
Cannabis users showed an attention-dependant alteration in PPI, which appeared to reflect a deficit in sustain attention, and which was different to that which has been observed in schizophrenia using the same methodology.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The possibility of a relationship between cannabis use and schizophrenia has a relatively long and controversial history, and the past 15 years has seen extensive research attention on this topic. Despite the breadth of literature, the exact nature of this relationship is still unclear (e.g. Degenhardt and Hall 2006; Degenhardt et al. 2003), and the topic remains controversial. Given the hypothesised association between cannabis use and schizophrenia, it is of interest to examine whether cannabis use in healthy people produces effects on cognitive and psychophysiological endophenotypes consistent with those observed in schizophrenia (e.g. Solowij and Michie 2007). Altered pre-pulse inhibition (PPI) in schizophrenia is one such proposed endophenotype (Braff and Light 2005; Turetsky et al. 2007). PPI is the decrease in the magnitude of the startle response when a non-startling stimulus (pre-pulse) precedes a startling stimulus (pulse) at certain stimulus onset asynchronies (SOAs; Graham 1975). Early studies using uninstructed PPI paradigms found that, relative to healthy controls, patients with schizophrenia showed reduced PPI (for a review, see Braff et al. 2001), which was hypothesised to reflect a disturbance to pre-attentive processing (Braff and Geyer 1990). A number of more recent studies have shown that, unlike healthy controls, patients with schizophrenia do not show attentional modulation of PPI during PPI tasks with attentional instructions (Dawson et al. 1993, 2000; Hazlett et al. 1998, 2008, 2007; Kedzior and Martin-Iverson 2007; Scholes and Martin-Iverson 2009). That is, where controls show differing levels of PPI depending on whether they are instructed to attend to, or ignore the auditory stimuli, patients do not. Further, decreased PPI in patients, using such tasks, has only been observed under certain attentional instructions, suggesting that disturbed PPI in schizophrenia results from disrupted top-down controlled modulation of PPI (Dawson et al. 1993, 2000; Hazlett et al. 2008, 2007; Kedzior and Martin-Iverson 2007; Scholes and Martin-Iverson 2009).
The reported effects of cannabinoid administration on PPI in animals are inconsistent (Bortolato et al. 2005; Malone and Taylor 2006; Martin-Iverson and Cornelisse 2005; Martin et al. 2003; Nagai et al. 2006; Schneider et al. 2005; Schneider and Koch 2003, 2002; Stanley-Cary et al. 2002; Wegener et al. 2008). In humans, one study found no difference between cannabis users and non-users in an uninstructed PPI task (Quednow et al. 2004), while another study by Kedzior and Martin-Iverson (2007) found that chronic cannabis users failed to show significant attentional modulation of PPI, and had reduced PPI relative to controls, but only when they were instructed to sustain attention to the auditory stimuli, not when they were instructed to ignore the stimuli and focus on a visual task. Interestingly, the findings of the latter study are consistent with the findings that have been reported in patients with schizophrenia using attentional modulation PPI paradigms (e.g. Dawson et al. 1993, 2000; Hazlett et al. 2001, 2008; Kedzior and Martin-Iverson 2007).
The variation in findings regarding the effects of cannabinoids in both animals and humans may be due to an array of factors including differences in strains or species of animals; acute or chronic effects; doses administered, or in the case of humans, amount and strength of cannabis used; as well as duration of use, age of onset of use and frequency of use. The effects of various other substances should also be taken into consideration, given that nicotine, caffeine, alcohol and other illicit substances may affect PPI (e.g. Acri et al. 1994; Kumari and Gray 1999; Schicatano and Blumenthal 1995; Swerdlow et al. 2003, 2000) and attention (e.g. Peeke and Peeke 1984; Schicatano and Blumenthal 1998). Importantly, methodological variation likely also contributes to the variation in findings in human studies particularly. The use of PPI paradigms in which attention is controlled are advantageous over uninstructed paradigms; this is because unconstrained and unmeasured attention varying across trials and between subjects in uninstructed tasks confounds the findings and limits interpretation (Kedzior and Martin-Iverson 2007; Scholes and Martin-Iverson 2009). Additionally, differences in acoustic stimuli and PPI parameters between studies can lead to variation in findings. Attention can modulate startle and PPI differently (i.e. in the opposite direction) depending on the intensity of the startle stimuli (Scholes and Martin-Iverson 2009). Further, there are vast individual differences in sensitivity to startle stimuli (e.g. Hamm et al. 2001; Hince and Martin-Iverson 2005), which can produce sampling biases (Hamm et al. 2001) and can confound calculation of PPI (Csomor et al. 2008).
Examining startle magnitudes to a range of startling stimulus intensities, rather than to just one stimulus intensity as is common practice, has been suggested to help deal with these limitations associated with traditional PPI methods, and can also be more informative (Hince and Martin-Iverson 2005; Martin-Iverson and Stevenson 2005; Scholes and Martin-Iverson 2009; Stoddart et al. 2008; Yee et al. 2005). By doing this, the stimulus intensity-response magnitude (SIRM) relationship can be examined, and the resulting parameters, reflecting different aspects of this relationship, can be determined (Martin-Iverson and Stevenson 2005), similar to the methods in pharmacology used to assess dose-response relationships. These SIRM parameters are reflex capacity (R MAX; the asymptote of the curve, the maximum limit of the reflex), stimulus potency (ES50; the stimulus intensity required to elicit a half-maximal response), stimulus sensitivity (Threshold; the minimum level of stimulation required to elicit a startle response) and reflex efficacy (Hillslope; the slope of the dynamic range at its mid-point). The SIRM methods have been validated in rats (Hince and Martin-Iverson 2005; Martin-Iverson and Stevenson 2005), mice (Stoddart et al. 2008) and humans (Scholes and Martin-Iverson 2009), and provide enhanced detail on the effects of various manipulations on startle and PPI.
These SIRM methods have recently been employed in a study of patients with schizophrenia (Scholes and Martin-Iverson 2009). Consistent with previous studies using traditional methods for the indexation of PPI, patients with schizophrenia failed to show attentional modulation of all SIRM parameters. Further, patients showed significantly reduced PPI of R MAX and significantly increased PPI of Hillslope, relative to controls, but only when they were instructed to ignore the auditory stimuli and focus on a visual stimulus. These findings were suggested to reflect a disruption of controlled modulation of PPI, resulting from, at least in part, an inability to ignore distracting potent stimuli.
Therefore, the present study aimed to use the SIRM methodology to examine the effects of frequent cannabis use on PPI during an attention manipulation task, in healthy humans. It was predicted that cannabis users would show a similar disturbance to that observed in schizophrenia using SIRM methods and an attention manipulation task; that is, a failure to show attentional modulation of all SIRM parameters, and altered PPI of R MAX and Hillslope, but only when instructed to selectively attend to a relevant visual stimulus and ignore the distracting auditory startle and pre-pulse stimuli.
Materials and methods
Participants
The sample comprised healthy volunteers, recruited from the general community, who were divided into two groups, frequent cannabis users (n = 36) and control non-users (n = 35). Participants were recruited via advertisements in local media and from a database of potential willing volunteers at the research centre, and were screened prior to inclusion in the study. There were approximately 150 cannabis users who responded to the advertisements for this study (over a period of 2 years), of these, approximately 80 satisfied the exclusion criteria and were booked appointments in the study. However, of these, only 36 cannabis users completed the testing session (the rest did not show up to their appointment/s despite numerous reminder calls and every effort being made to ensure their attendance). The exclusionary criteria for the study included: self-reported presence of any hearing disorders, any neurological disorders or head injury, loss of consciousness for over 15 min, diagnosis of psychiatric illness or current use of psychiatric medications (such as antidepressants) or a first degree relative with a diagnosis of schizophrenia or schizoaffective disorder, as healthy relatives of patients with schizophrenia may show a reduction in PPI (Cadenhead et al. 2000). Further, controls were not to have used any illicit substance more than once in the past 12 months. After recruitment, all participants were administered the Mini International Neuropsychiatric Interview (MINI; Sheehan et al. 1998) to assess for the presence of Axis I disorders. The MINI has established reliability and validity (Amorim et al. 1998; Sheehan et al. 1997). Two controls were excluded from analysis as they were classified as non-responders; that is, they had a mean Threshold in the pulse alone condition greater than 115 dB, under either the ATTEND or IGNORE condition (they required a startle stimulus intensity of over 115 dB to elicit a startle response). One control participant was excluded, as a urine sample was not provided and absence of illicit drug use could not be confirmed. A further two cannabis users and one control were excluded at random (based on their individual order of PPI attention condition presentation) so the order of presentation of the attention conditions was counterbalanced. Thus, the final sample consisted of 66 participants, 34 cannabis users and 32 controls. There was no intentional matching of controls and cannabis users in the current (we just aimed to recruit as many participants as possible in order to maximise power), but as can be seen in Table 1, there were very few differences in the demographic and substance use (besides cannabis) characteristics between the two groups. This study was approved by the Western Australia North Metropolitan Area Mental Health Service Ethics Committee, and was performed in accordance with the ethical standards laid down in the 1963 Declaration of Helsinki.
Substance use assessment
Recent use of nicotine, alcohol, caffeine, cannabis and other illicit substances was assessed with a self-report questionnaire, as previously described (Scholes and Martin-Iverson 2009). In addition, for cannabis use, participants were required to indicate their average usage in the past 12 months (daily/nearly daily, weekly, monthly or less than monthly), the age at which they first started using cannabis regularly and the total duration of years in which they had been using cannabis regularly. Current (past 12 months) alcohol and substance misuse was assessed with the MINI. Self reports of substance use have been shown to be consistent, valid and reliable among healthy drug users (Brown et al. 1992; Del Boca and Noll 2000; Harrison et al. 1993; Kedzior et al. 2006; Langendam et al. 1999; Martin et al. 1988). Urine samples were also obtained from all participants in order to screen for the presence of illicit drugs and to quantify the levels of cotinine (metabolite of nicotine) and 11-nor-Δ9-tetrahydrocannabinol-9-carboxylic acid (THC-COOH; metabolite of cannabis). Urine samples were analysed using cloned enzyme donor immunoassay (CEDIA) to screen for the presence of illicit drugs, using AS/NZ 4308 2001 cut-off levels. Further, gas chromatography–mass spectrometry (GCMS) was performed to quantify cotinine and THC-COOH levels.
Psychophysiological data collection and processing
The current study’s stimuli, recording and processing were identical to our previous report (Scholes and Martin-Iverson 2009). Briefly, the experiment consisted of two attention set tasks, one in which participants were instructed to attend to the auditory stimuli and identify the number of auditory stimuli presented on each trial (‘ATTEND’ task) and one in which they were instructed to ignore the auditory stimuli and focus on a visual task where they were required to find small smiley faces hidden amongst a neutral visual stimulus (‘IGNORE’ task). The response requirements and the visual stimuli onset and offset (i.e. pictures during the IGNORE task and blank screens during the ATTEND task) were matched across the attention tasks.
Both attention tasks comprised two blocks of 26 trials, which were separated by a random inter-trial interval (10–20 s, M = 15 s), and were presented in a random order. Each block contained eight pulse alone trials (40 ms bursts of white noise, 80–115 dB, in 5-dB increments), eight pre-pulse plus pulse trials with a 60 ms SOA (pre-pulses were 20 ms bursts of 74 dB white noise), eight pre-pulse plus pulse trials with a 100 ms SOA, one pre-pulse only trial and one null trial in which no auditory stimuli were presented. Auditory stimuli were presented binaurally through a pair of stereo headphones, over 60-dB background white noise.
The startle reflex was recorded from two miniature tin-cup surface electrodes using a standard National Instruments data acquisition (DAQ) card (DAQ 6062E; San Diego, CA, USA). The electrodes were filled with conductive paste, and placed approximately 1 cm beneath the right pupil, and a ground electrode was placed on top of the left hand. Recording of the electromyographic signal began 600 ms prior to onset of the startling stimulus and continued for 400 ms after its presentation. Filtering, amplification, rectification, smoothing and signal processing are described in detail elsewhere (Scholes and Martin-Iverson 2009). The peak startle response magnitude was extracted from each trial, according to the procedure described previously (Scholes and Martin-Iverson 2009).
Procedure
Upon arrival at the research centre, all participants provided written informed consent after the study procedures were explained in full. They then completed the substance use questionnaire, were administered the MINI and provided a urine sample. Cannabis users were instructed not to alter their cannabis use on the day of testing, to reduce the likelihood of participants experiencing an abstinence syndrome during testing (e.g. Haney et al. 2004, 1999; Hart et al. 2002; Jones et al. 1976), and smoking of cigarettes was permitted ad libitum prior to the testing session, in order to reduce the likelihood of nicotine withdrawal affecting PPI (Duncan et al. 2001). Acute effects of nicotine (Kumari et al. 2001) were minimised as participants spent approximately 20 min with the researcher performing consent procedures and collecting demographic and substance use information before they were prepared for recording and the startle testing began. Before the start of the two PPI attention tasks, participants completed a ‘pre-pulse detection test’ where auditory stimuli of varying intensity were presented to them, and they were required to indicate after each trial whether they heard a sound. This provided further assurance that all participants could hear all auditory stimuli used in the experiment.
Data analysis
Fitting of logistic functions
Identical to previously described (Scholes and Martin-Iverson 2009), non-linear regression was used to fit curves of best fit to each individual’s mean peak response magnitudes, across the startle stimulus intensities, for the pulse alone and each pre-pulse condition, under each attention condition. The SIRM parameters were determined with a non-linear regression Levenberg–Marquardt algorithm for iterative estimation. For cases where curves could not be fitted under the pre-pulse conditions (i.e. 100% inhibition, Hillslope = 0) the following values were computed for statistical analysis: R MAX = the maximum observed response for the given individual under the given condition; Hillslope = 0; ES50 = 115; Threshold = 115.
Statistical analysis
Between-group differences in demographics and substance use were investigated with independent samples t tests, chi square/fishers exact tests or Mann–Whitney U tests, where relevant. Statistical analyses were performed on the parameters (R MAX, ES50, Threshold and Hillslope) drawn from the SIRM functions. Missing parameter values were replaced by the group series mean (note: There are very few missing values using SIRM procedures, as curves are fitted to the data as long as there are at least five raw data points on which to estimate the curve, and thus missing values only occur if there are less than five raw data points for any one curve. See Table 3). The Hillslope parameters were significantly skewed to the right, and were normalised with the application of common Log transformations. PPI of R MAX was calculated according to the following formula (negative values indicate inhibition):
PPI of ES50, Hillslope and Threshold were calculated as difference scores (pre-pulse plus pulse−pulse alone) given that these parameters were on logarithmic scales. Positive values of PPI of ES50 and Threshold indicate inhibition (increases in these parameters with pre-pulse presentation indicate increases in the intensity of the stimuli required to produce startle; i.e. inhibition of sensitivity/potency), while negative values of PPI of Hillslope indicate inhibition. PPI was calculated for each SOA under each attention condition.
Each parameter, under the pulse alone condition, was analysed with repeated measures analysis of covariance (RM ANCOVA) with one between-subjects factor (group: cannabis users and controls), one within-subjects factor (attention: ATTEND and IGNORE) and one covariate (cotinine level). PPI of each parameter was analysed with RM ANCOVA with one between-subjects factor (group: cannabis users and controls), two within-subjects factors (attention: ATTEND and IGNORE; SOA 60 and 100 ms) and one covariate (cotinine level). Given the insensitivity of ANOVA to ordinal interactions (Strube and Bobko 1989), planned pairwise comparisons with Sidak correction (p < 0.05) were used to examine differences between cannabis users and controls under each attention task and to examine differences between ATTEND and IGNORE tasks (i.e. attentional modulation), regardless of the significance of the relevant interaction terms.
Pearson's bivariate correlations were performed between attentional modulation of PPI (differential PPI = PPI under IGNORE−PPI under ATTEND) and each of the cannabis use variables, controlling for cotinine levels. These were confirmed with Spearman's correlations as some of the cannabis use variables were not normally distributed. Further, behavioural performance under each attention condition was analysed with RM ANCOVAs as per the startle data.
Results
Demographics and substance use
As can be seen in Table 1, there was a significantly greater proportion of cigarette smokers and a greater cotinine concentration in the cannabis users as compared to controls. Therefore cotinine was included as a covariate in the subsequent analyses. Table 2 shows the substance use characteristics of the cannabis users. In addition, 16 cannabis users reported using other drugs in the last month (amphetamine = 12, hallucinogens = 4). Analysis of the urine samples revealed that, of the cannabis users, two screened positive for opiates (reported pain medication taken the day before testing), eight screened positive for amphetamines, and one screened positive for benzodiazepines. The alcohol and substance use modules of the MINI (past 12 months of use) indicated that, of the cannabis users, eight abused cannabis, while 21 were dependant on cannabis. Further, 12 of the cannabis users screened positive for abuse or dependence of other substances in the past 12 months (alcohol abuse = 9, dependence = 7; amphetamine abuse = 7, dependence = 7; hallucinogen abuse = 7; tranquilliser abuse = 1, dependence = 2; cocaine abuse = 1, dependence = 2).
SIRM function fits
The fits for the logistic functions that were fitted to the raw data are presented in Table 3. The mean SIRM curves, as a function of group, attention condition and stimulus condition, are presented in Fig. 1.

The mean acoustic startle response magnitude for a controls and b cannabis users, as a function of stimulus intensity (SIRM function), under each stimulus condition and each attention condition, for cases with Hillslope greater than zero and with at least five data points on which to estimate the curve. The lines represent the mean predicted response (±SEM) obtained from the logistic regression; the symbols represent the observed means
Startle
R MAX
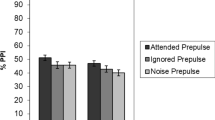
RM ANCOVA revealed a main effect of attention (F(1,63) = 5.06, p = 0.028, partial η 2 = 0.07) but no main effect of group (F(1,63) = 0.27, p = 0.608, observed power = 0.08) and no attention by group interaction (F(1,63) = 0.40, p = 0.531, observed power = 0.10). Pairwise comparisons with Sidak correction indicated that controls showed attentional modulation of startle R MAX (greater R MAX under IGNORE than ATTEND; F(1,63) = 5.52, p = 0.022, partial η 2 = 0.08) but cannabis users did not (F(1,63) = 2.18, p = 0.145, observed power = 0.31). See Fig. 2a.

Mean (±SEM) SIRM parameters under pulse alone condition, for cannabis users and controls, under both the ATTEND and IGNORE conditions. Significant difference at *p < 0.05, ** p < 0.01
ES50
There was a significant main effect of attention (F(1,63) = 5.50, p = 0.022, partial η 2 = 0.08) but no main effect of group (F(1,63) = 1.03, p = 0.313, observed power = 0.17) and no group by attention interaction (F(1,63) = 0.18, p = 0.677, observed power = 0.07). Pairwise comparisons with Sidak correction revealed that controls exhibited attentional modulation of startle ES50 (greater ES50 under IGNORE than ATTEND; Sidak correction; F(1,62) = 4.43, p = 0.039, partial η 2 = 0.07) but cannabis users did not (F(1,63) = 2.38, p = 0.128, observed power = 0.33). See Fig. 2b.
Threshold
There were no significant main effects of attention (F(1,63) = 0.31, p = 0.580, observed power = 0.09) or group (F(1,63) = 0.91, p = 0.345, observed power = 0.16) and no attention by group interaction (F(1,63) = 3.76, p = 0.057, observed power = 0.48). The difference between Threshold under ATTEND and IGNORE (i.e. attentional modulation) was close to significance for controls with pairwise comparisons (F(1,63) = 3.78, p = 0.056, observed power = 0.48) and was not significant for cannabis users (F(1,63) = 0.87, p = 0.358, observed power = 0.15). See Fig. 2c.
Hillslope
There was a significant main effect of attention (F(1,63) = 16.07, p < 0.0005, partial η 2 = 0.20) indicating that both controls and cannabis users showed greater Hillslope under ATTEND than IGNORE (this was main effect was supported in the follow-up pairwise comparisons), but no main effect of group (F(1,63) = 0.77, p = 0.384, observed power = 0.14) and no group by attention interaction (F(1,63) = 1.64, p = 0.205, observed power = 0.24). See Fig. 2d.
PPI
R MAX
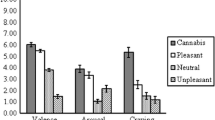
RM ANCOVA revealed a significant main effect of attention (F(1,63) = 8.98, p = 0.004, partial η 2 = 0.13) and SOA (F(1,63) = 8.32, p = 0.005, partial η 2 = 0.12) but no main effect of group (F(1,63) = 3.44, p = 0.068, observed power = 0.45) and no attention by group (F(1,63) = 0.21, p = 0.647, observed power = 0.07), SOA by group (F(1,63) = 0.20, p = 0.653, observed power = 0.07), attention by SOA (F(1,63) = 0.57, p = 0.452, observed power = 0.12) or attention by group by SOA interactions (F(1,63) = 2.17, p = 0.145, observed power = 0.31). Pairwise comparisons with Sidak correction indicated that under the ATTEND condition, cannabis users exhibited more PPI of R MAX at the 100 ms SOA, as compared to controls (F(1,63) = 5.40, p = 0.023, partial η 2 = 0.08), but this group difference was not evident at the 60 ms SOA (F(1,63) = 0.13, p = 0.717, observed power = 0.07). There were no group differences under the IGNORE condition at both the 60 ms (F(1,63) = 1.00, p = 0.321, observed power = 0.17) and 100 ms (F(1,63) = 0.30, p = 0.584, observed power = 0.08) SOAs. Further, controls exhibited attentional modulation of PPI at the 100 ms SOA (F(1,63) = 11.14, p = 0.001, partial η 2 = 0.15) but not the 60 ms SOA (F(1,63) = 1.43, p = 0.236, observed power = 0.22), whereas cannabis users did not exhibit attentional modulation of PPI at either SOA (60 ms (F(1,63) = 3.19, p = 0.079, observed power = 0.42), 100 ms (F(1,63) = 0.81, p = 0.371, observed power = 0.14)). See Figs. 3a and 4a.

Mean (±SEM) PPI of SIRM parameters for cannabis users and controls under both the ATTEND and IGNORE conditions, at the 60 ms SOA

Mean (±SEM) PPI of SIRM parameters for cannabis users and controls under both the ATTEND and IGNORE conditions, at the 100 ms SOA. Significant difference at *p < 0.05, **p < 0.01
ES50
There were no main effects of attention (F(1,63) = 3.10, p = 0.083, observed power = 0.41), SOA (F(1,63) = 1.34, p = 0.252, observed power = 0.21) or group (F(1,63) = 1.95, p = 0.168, observed power = 0.28) and no attention by group (F(1,63) = 0.37, p = 0.955, observed power = 0.09), SOA by group (F(1,63) = 1.16, p = 0.285, observed power = 0.19), attention by SOA (F(1,63) = 0.08, p = 0.773, observed power = 0.06) or attention by group by SOA interactions (F(1,63) = 2.24, p = 0.140, observed power = 0.31). Pairwise comparisons with Sidak correction indicated that under the ATTEND condition, cannabis users showed reduced PPI at the 100 ms SOA, relative to controls (F(1,63) = 6.19, p = 0.016, partial η 2 = 0.09) but not at the 60 ms SOA (F(1,63) = 0.48, p = 0.490, observed power = 0.11). There were no group differences under the IGNORE condition at both the 60 ms (F(1,63) = 0.59, p = 0.444, observed power = 0.12) and 100 ms (F(1,63) = 0.36, p = 0.551, observed power = 0.09) SOAs. Further, controls showed attentional modulation of PPI at the 100 ms SOA (F(1,63) = 5.06, p = 0.028, partial η 2 = 0.07) but not the 60 ms SOA (F(1,63) = 0.88, p = 0.351, observed power = 0.15), whereas cannabis users did not show attentional modulation of PPI at either SOA (60 ms (F(1,63) = 1.60, p = 0.210, observed power = 0.24), 100 ms (F(1,63) = 0.17, p = 0.685, observed power = 0.07)). See Figs. 3b and 4b.
Threshold
RM ANCOVA revealed a significant group by attention interaction (F(1,63) = 4.43, p = 0.039, partial η 2 = 0.07) and a significant SOA by group interaction (F(1,36) = 4.62, p = 0.036, partial η 2 = 0.07), but no attention by SOA (F(1,36) = 0.95, p = 0.334, observed power = 0.16) or attention by group by SOA interactions (F(1,36) = 1.65, p = 0.204, observed power = 0.24). Pairwise comparisons with Sidak correction indicated that under the ATTEND condition, cannabis users had reduced PPI at the 100 ms SOA as compared to controls (F(1,36) = 9.29, p = 0.003, partial η 2 = 0.13) but not at the 60 ms SOA (F(1,36) = 0.18, p = 0.676, observed power = 0.07). There were no group differences under the IGNORE condition for the both 60 ms (F(1,36) = 0.96, p = 0.332, observed power = 0.16) and 100 ms (F(1,36) = 0.07, p = 0.787, observed power = 0.06) SOAs. Further, for controls, the difference between PPI under ATTEND and IGNORE (i.e. attentional modulation) was just off significance for both the 60 ms (F(1,63) = 3.86, p = 0.054, observed power = 0.49) and 100 ms (F(1,36) = 3.71, p = 0.058, observed power = 0.48) SOAs. There were no significant differences between PPI under ATTEND and IGNORE for the cannabis users (60 ms SOA (F(1,36) = 0.02, p = 0.898, observed power = 0.05); 100 ms SOA (F(1,36) = 2.61, p = 0.111, observed power = 0.36)). See Figs. 3c and 4c.
Hillslope
There was a significant main effect of attention (F(1,36) = 14.44, p < 0.0005, partial η 2 = 0.19) but no main effects of group (F(1,36) = 0.60, p = 0.440, observed power = 0.12) or SOA (F(1,36) = 0.50, p = 0.483, observed power = 0.11), and no attention by group (F(1,36) = 0.81, p = 0.371, observed power = 0.14), SOA by group (F(1,36) = 0.31, p = 0.580, observed power = 0.09), attention by SOA (F(1,36) = 1.09, p = 0.300, observed power = 0.18) or attention by group by SOA (F(1,36) = 1.57, p = 0.214, observed power = 0.24) interactions. Pairwise comparisons with Sidak correction revealed that controls showed attentional modulation of PPI at the 100 ms SOA (F(1,36) = 11.33, p = 0.001, partial η 2 = 0.15) but not the 60 ms SOA (F(1,36) = 3.52, p = 0.065, observed power = 0.46). Cannabis users did not show attentional modulation of PPI at either SOA (60 ms (F(1,36) = 3.30, p = 0.074, observed power = 0.43); 100 ms (F(1,36) = 1.56, p = 0.216, observed power = 0.23)). See Figs. 3d and 4d.
These PPI analyses were repeated using only certain sub-groups of the cannabis users; these analyses included: only daily users of cannabis (n = 21, all between-group differences remained significant); less than daily users of cannabis (n = 13, only Threshold between-group difference was significant, others were not close to significance (p > 0.2), and no significant correlations between PPI and cannabis use were observed); only those with positive toxicology screen for cannabis metabolites (n = 30, all between-group differences significant); only those who were dependant on cannabis, according to the MINI screening (n = 21, all between-group differences were significant except R MAX, which was close to significance (p = 0.2)); only daily users of cannabis who did not use any other illicit substance in the past 30 days (n = 10; all between-group differences were significant); only those who did not screen positive for any other substances on the toxicology screen (n = 24, between-group differences in ES50 and Threshold were close to significance (p < 0.18), correlations between cannabis use measures and PPI were consistent with those observed from the whole group analyses, see below); only those that did not screen positive for abuse/dependence of any other substance in the past 12 months, according to the MINI (n = 22, between-group difference for ES50 just off significance (p < 0.1), between-group differences in R MAX, Threshold and Hillslope were significant). Further, median splits were performed on the cannabis use variables ‘hours since last use’ and ‘number of days of use in the past 30’, and analyses were repeated separately on each of the split groups (i.e. n = 17 for each analysis). For hours since last use, those with the most recent cannabis use showed significant between-group differences on all measures, and those with the longest time since last use only showed a significant between-group difference in Threshold (though the rest were just off significance, p < 0.1). Similarly, for number of days of cannabis use in the past 30, those with the most days of use showed significant between-group differences on all PPI measures, those with the least days of use in the past 30 only showed a significant between-group difference in Threshold (though again, the rest of the PPI measures were just off significance, p < 0.1). In all analyses, cannabis users failed to show significant attentional modulation of PPI.
Correlations
As can be seen in Table 4, there were significant positive correlations between number of days of cannabis use in the last 30 days and differential PPI of ES50 at the 100 ms SOA (Fig. 5a), as well as differential PPI of R MAX at the 100 ms SOA (Fig. 5b), when controlling for cotinine levels. These correlations suggest that the more use of cannabis in the past month, the less attentional modulation of PPI (modulation in the same direction as controls). Further, there was a significant negative correlation between differential PPI of ES50 at the 100 ms SOA and total duration of cannabis use. However, this correlation was no longer significant when controlling for both age and cotinine levels (r = −0.127, p = 0.519). The correlations between the various cannabis use measures can be found in Table 5.

Correlations between cannabis use in the past 30 days and a differential PPI of ES50 at the 100 ms SOA (p = 0.034) and b differential PPI of R MAX at the 100 ms SOA (p = 0.008), controlling for cotinine levels
Task performance
There were no significant differences in performance measures between cannabis users and controls, for both the ATTEND and IGNORE tasks (Tables 6 and 7).
Discussion
The current study used novel methodology to examine the effects of frequent cannabis use on PPI during an attention set task, in otherwise healthy participants. It was predicted that cannabis users would fail to show attentional modulation of PPI, resulting specifically from an alteration in PPI of R MAX and Hillslope under the IGNORE condition only, as we have observed in schizophrenia (Scholes and Martin-Iverson 2009). Indeed, chronic cannabis users failed to show significant attentional modulation of PPI of all SIRM parameters. However, unlike patients with schizophrenia (Scholes and Martin-Iverson 2009), cannabis users showed altered PPI the SIRM parameters under the ATTEND condition only, when task instructions required them to maintain sustained attention to the auditory stimuli.
The current study suggests, as observed in schizophrenia, that cannabis users do not show normal modulation of PPI by attention; however, the basis for this lack of attentional modulation appears to be different between the two groups. Schizophrenia patients appear to have difficulty in the correct allocation of attentional resources, and in particular, the ignoring of distracting potent stimuli (Scholes and Martin-Iverson 2009). Unlike patients (Scholes and Martin-Iverson 2009), cannabis users showed no differences in PPI under the IGNORE condition, suggesting they were effectively able to ‘ignore’ the auditory stimuli when required. Consistent with a previous report (Kedzior and Martin-Iverson 2007), cannabis users appeared to simply fail to sustain attention to the auditory stimuli when required, resulting in altered PPI levels under the ATTEND condition, with PPI of each SIRM parameter being equivalent to that observed when they were ignoring the auditory stimuli. A number of studies have found deficits in sustained attention or vigilance in cannabis users (Bahri and Amir 1994; Croft et al. 2001; Ehrenreich et al. 1999; Ilan et al. 2004; Moskowitz and McGlothlin 1974; Pope and Yurgelun-Todd 1996). Alternatively, or as a possible moderator of sustained attention deficits, it may be that a disturbance in motivational processes in cannabis users (e.g. Kouri et al. 1995) results in a lack of motivation to maintain attention to the ATTEND task, although there were no intentional intrinsic motivational differences between the two attention tasks. It should also be considered that the two PPI attention tasks required attention to different modalities, and it is possible that cannabis affects modality specific attentional processes (i.e. auditory attention, as PPI disturbances were only observed under the ATTEND condition when attention to the auditory stimuli was required).
These effects (lack of attentional modulation and between-group differences) were only evident at the 100 ms SOA. The effects of attention on PPI are well characterised, and attentional effects are most prominent at SOAs of approximately 120 ms (e.g. Dawson et al. 1993), though they can be evident at shorter SOAs (e.g. Elden and Flaten 2002). Thus, this provides further support to the notion that group differences were due to differences in attention, as they were only evident at the longer SOA where attentional effects are strongest. Given that cannabis users show altered PPI only when they were required to sustain attention to the auditory stimuli, and not when they were ignoring them, it is most likely that these alterations are secondary to attentional set/sustained attention dysfunction and a resultant deficit in the modulation of PPI, rather than due to a principal deficit in PPI or sensorimotor gating itself. If the altered PPI in cannabis users was due to underlying pre-attentive inhibitory or sensorimotor gating deficits, the alterations should be observed under both attention manipulations. Such a contention could explain the lack of significant differences between controls and cannabis users in the study by Quednow et al. (2004) which used an uninstructed PPI task. A number of recent studies have shown that sensory gating of the P50 response (a psychophysiological measure that has been likened to PPI) is disrupted by administration of cannabinoids in humans (Rentzch et al. 2007) and in rats (Hajos et al. 2008; Zachariou et al. 2008), suggesting that cannabinoids disrupt early information processing or gating. However, drug conditions may have differing effects on PPI and P50 gating (e.g. Mann et al. 2007; Oranje et al. 2006), and thus P50 gating effects may not be directly comparable to PPI effects. Further, in the current study, differences between cannabis users and controls were confined to a single attentional condition, suggesting that these differences were contingent upon the attentional conditions, and are thus a result of a top-down attentional deficit.
In the current study, the lack of attentional modulation in cannabis users was associated with more days of cannabis use in the past month. This suggests that recent frequent use of cannabis is associated with less attentional modulation of PPI. Use of cannabis in the last 30 days was highly correlated with other measures of recent use (urine THC-COOH level, hours since last cannabis use and number of uses in the past 24 h), and thus the correlation observed here between PPI and cannabis use in the past 30 days likely reflects the effects of recent use of cannabis on the brain. Maximal plasma levels of THC are observed approximately 2 h after cannabis use (Curran et al. 2002), while the median number of hours since last cannabis use in the current study was 8.5 h. Thus, given that PPI correlations were observed between use in the last 30 days (as opposed to urine THC-COOH level and hours since last use or numbers of uses in the past 24 h) and that the median number of hours since last use was well above the time of peak plasma THC levels, the effects observed in the current study are not likely to be due to acute cannabis intoxication but are likely to be primarily due to sub-acute effects of cannabinoids present in the brain. It should be noted that the issue of sub-acute effects of cannabis on cognition is contentious, and deficits observed after short periods of abstinence may alternatively reflect withdrawal effects (e.g. Haney et al. 1999; Pope and Yurgelun-Todd 1996). While we contend that the PPI alterations observed here likely reflect the effects of recent chronic cannabis use (given the correlations observed between recent use, but not acute use), this study employed no defined abstinence period, and some cannabis users had used cannabis with the previous few hours before the testing session; it is possible that these PPI effects observed here may be due to acute intoxication, although none of the participants appeared intoxicated at time of testing.
Despite the differences in attentional modulation of PPI, no significant differences in errors of commission or omission were observed between cannabis users and controls on either of the attention set tasks. There was very little variability in the data, and thus, these measures of performance may not have been sensitive enough to reflect attention deficits. Some studies suggest that the cognitive deficits in cannabis users are quite subtle and may only be evident in complex or taxing tasks, or may be more apparent with psychophysiological measures, rather than more crude cognitive performance measures (Solowij 1995; Solowij et al. 1995). Further, as noted above, and consistent with Kedzior and Martin-Iverson (2007), cannabis users showed PPI equivalent to controls under the IGNORE condition. This suggests that they were able to effectively ignore the irrelevant auditory stimuli when completing the visual task. While some cognitive studies have found that cannabis users show deficits in attentional control (Skosnik et al. 2001; Solowij 1995; Solowij et al. 1995), others have only found differences in sub-groups of users, such as only in males (Pope and Yurgelun-Todd 1996) or those with low cognitive reserves (Bolla et al. 2002), and still others have found no effects of cannabis use on attentional control (Eldreth et al. 2004; Gruber and Yurgelun-Todd 2005; Pope et al. 2001; Solowij et al. 2002). It would be of interest to examine PPI and cognitive performance together in cannabis users, in order to gain better understanding of the attention disturbances that may contribute to the altered PPI observed here.
The between-group differences and associated correlations appeared not to be related to dependence on cannabis, recent use of other illicit drugs or abuse/dependence of other drugs in the past 12 months. However, the analysis on the sub-group of users who used cannabis less than daily was not entirely consistent with the findings observed with the cannabis-using group as a whole. This may be a power issue, as this analysis only contained 13 cannabis users. However, median split analyses showed that the PPI alterations in the cannabis users were also weaker (i.e. fewer between-group differences) in those who had the longest time since last use and those with the least use of cannabis in the past 30 days. Thus, it is likely that the attention-dependant disturbances in PPI are particularly associated with recent frequent use, which is likely related to the sub-acute effects of THC in the body. Our sample consisted of only four cannabis users who had no detectable THC-COOH metabolites in their urine at time of testing, and thus we could not examine whether these disturbances in PPI remain when THC residues are no longer detectable. Given that significant group differences and correlations were not observed in infrequent users, four of which had no detectable THC in their urine, and were weaker in those with the longest time since last use and the least use in the past month, it may be that, consistent with a number of studies (Fried et al. 2002; Pope et al. 2001, 1995; Skosnik et al. 2001), after an extended period of abstinence, these attention-dependant disturbances would no longer be evident.
In conclusion, cannabis users showed an attention-dependant alteration in PPI, which appeared to reflect a deficit in the ability to sustain attention to the auditory stimuli when required. This disturbance was correlated with the amount of use of cannabis in the past 30 days, suggesting that these findings reflect sub-acute effects of cannabinoids present in the brain. While these findings in cannabis users are similar to those reported in patients with schizophrenia, in so far as both groups fail to show significant attentional modulation of PPI, the current study suggests that slightly different attentional disturbances underlie PPI alterations in cannabis users and patients with schizophrenia, a finding made possible with the SIRM methodology for startle characterization.
References
Acri J, Morse D, Popke E, Grunberg N (1994) Nicotine increases sensory gating measured as inhibition of the acoustic startle reflex in rats. Psychopharmacology (Berlin) 114:369–374
Amorim P, Lecrubier Y, Weiller E, Hergueta T, Sheehan BD (1998) DSM-III-R psychotic disorders: procedural validity of the Mini International Neuropsychiatric Interview (MINI). Concordance and causes for discordance with the CIDI. Eur Psychiatry 13:26–34
Bahri T, Amir T (1994) Effect of hashish on vigilance performance. Percept Mot Skills 78:11–16
Bolla KI, Brown K, Eldreth D, Tate K, Cadet JL (2002) Dose-related neurocognitive effects of marijuana use. Neurology 59:1337–1343
Bortolato M, Aru GN, Frau R, Orru M, Luckey GC, Boi G, Gessa GL (2005) The CB receptor agonist WIN 55, 212-2 fails to elicit disruption of prepulse inhibition of the startle in Sprague–Dawley rats. Psychopharmacology (Berlin) 177:264–271
Braff D, Geyer M (1990) Sensorimotor gating and schizophrenia: human and animal model studies. Arch Gen Psychiatry 47:181–188
Braff DL, Light G (2005) The use of neurophysiological endophenotypes to understand the genetic basis of schizophrenia. Dialogues Clin Neurosci 7:125–135
Braff D, Geyer M, Light G, Sprock J, Perry W, Cadenhead K, Swerdlow N (2001) Impact of prepulse characteristics on the detection of sensorimotor gating deficits in schizophrenia. Schizophr Res 49:171–178
Brown JS, Dranzler HR, Del Boca FK (1992) Self-reports by alcohol and drug abuse inpatients: factors affecting reliability and validity. Br J Addict 87:1013–1024
Cadenhead KS, Swerdlow NR, Shafer KM, Diaz M, Braff DL (2000) Modulation of the startle response and startle laterality in relatives of schizophrenia patients and schizotypal personality disordered subjects: evidence of inhibitory deficits. Am J Psychiatry 157:1660–1668
Croft RJ, Mackay AJ, Mills ATD, Gruzelier JGH (2001) The relative contributions of ecstacy and cannabis to cognitive impairment. Psychopharmacology (Berlin) 153:373–379
Csomor PA, Yee BK, Vollenweider FX, Feldon J, Nicolet T, Quednow BB (2008) On the influence of baseline startle reactivity on the indexation of prepulse inhibition. Behav Neurosci 122:885–900
Curran HV, Brignell C, Fletcher S, Middleton P, Henry J (2002) Cognitive and subjective dose-response effects of acute oral Δ9-tetrahydrocannabinol (THC) in infrequent cannabis users. Psychopharmacology (Berlin) 164:61–70
Dawson M, Hazlett E, Filion D, Nuechterlein K, Schell A (1993) Attention and schizophrenia: impaired modulation of the startle reflex. J Abnorm Psychol 102:633–641
Dawson M, Schell A, Hazlett E, Nuechterlein K, Filion D (2000) On the clinical and cognitive meaning of impaired sensorimotor gating in schizophrenia. Psychiatry Res 96:187–197
Degenhardt L, Hall W (2006) Is cannabis use a contributory cause of psychosis. Can J Psychiatry 51:556–565
Degenhardt L, Hall W, Lynskey M (2003) Testing hypotheses about the relationship between cannabis use and psychosis. Drug Alcohol Depend 71:37–48
Del Boca FK, Noll JA (2000) Truth or consequences: the validity of self-report data in health services research on addictions. Addiction 95:S347–S360
Duncan E, Madonick S, Charkravorty S, Parwani A, Szilagyi S, Efferen T, Gonzenbach S, Angrist B, Rotrosen J (2001) Effects of smoking on acoustic startle and prepulse inhibition in humans. Psychopharmacology (Berlin) 156:266–272
Ehrenreich H, Rinn T, Kunert HJ, Moeller MR, Poser W, Schilling L, Gigerenzer G, Hoehe MR (1999) Specific attentional dysfunction in adults following early start of cannabis use. Psychopharmacology (Berlin) 142:295–301
Elden A, Flaten MA (2002) The relationship of automatic and controlled processing to prepulse inhibition. J Psychophys 16:46–55
Eldreth D, Matochik JA, Cadet JL, Bolla KI (2004) Abnormal brain activity in prefrontal brain regions in abstinent marijuana users. Neuroimage 23:914–920
Fried P, Watkinson B, James D, Gray Y (2002) Current and former marijuana use: preliminary findings of a longitudinal study of effects on IQ in young adults. Can Med Assoc J 166:887–891
Graham F (1975) The more or less startling effects of weak prestimulation. Psychophysiology 12:238–248
Gruber SA, Yurgelun-Todd D (2005) Neuroimaging of marijuana smokers during inhibitory processing: a pilot investigation. Brain Res Cogn Brain Res 23:107–118
Hajos M, Hoffman WE, Kocsis B (2008) Activation of cannabinoid-1 receptors disrupts sensory gating and neuronal oscillation: Relevance to schizophrenia. Biol Psychiatry 63:1075–1083
Hamm A, Weike A, Schupp H (2001) The effect of neuroleptic medication on prepulse inhibition in schizophrenia patients: Current status and future issues. Psychopharmacology (Berlin) 156:259–265
Haney M, Ward AS, Comer SD, Foltin RW, Fischman MW (1999) Abstinence symptoms following smoked marijuana in humans. Psychopharmacology (Berlin) 141:395–404
Haney M, Hart CL, Vosburg SK, Nasser J, Bennett A, Zubaran C, Foltin RW (2004) Marijuana withdrawal in humans: effects of oral THC or divalproex. Neuropsychopharmacology 29:158–170
Harrison ER, Haaga J, Richards T (1993) Self-reported drug use data: what do they reveal? Am J Drug Alcohol Abuse 19:423–441
Hart CL, Ward AS, Haney M, Comer SD, Foltin RW, Fischman MW (2002) Comparison of smoked marijuana and oral delta (9)-tetrahydrocannabinol in humans. Psychopharmacology (Berlin) 164:407–415
Hazlett E, Buchsbaum MS, Haznedar MM, Singer MB, Germans MK, Schnur DB, Jimenez EA, Buchsbaum BR, Troyer BT (1998) Prefrontal cortex glucose metabolism and startle eyeblink modification abnormalities in unmedicated schizophrenia patients. Psychophysiology 35:186–198
Hazlett EA, Dawson ME, Schell AM, Nuechterlein KH (2001) Attentional stages of information processing during a continuous performance test: a startle modification analysis. Psychophysiology 38:669–677
Hazlett EA, Romero MJ, Haznedar MM, New AS, Goldstein KE, Newmark RE, Siever LJ, Buchsbaum MS (2007) Deficient attentional modulation of startle eyeblink is associated with symptom severity in the schizophrenia spectrum. Schizophr Res 93:288–295
Hazlett EA, Dawson ME, Schell AM, Nuechterlein KH (2008) Probing attentional dysfunctions in schizophrenia: startle modification during a continuous performance test. Psychophysiology 45:632–642
Hince D, Martin-Iverson M (2005) Differences in prepulse inhibition (PPI) between Wistar and Sprague-Dawley rats clarified by a new method of PPI standardization. Behav Neurosci 119:66–77
Ilan AB, Smith ME, Gevins A (2004) Effects of marijuana on neurophysiological signals of working and episodic memory. Psychopharmacology (Berlin) 176:214–222
Jones RT, Benowitz N, Bachman J (1976) Clinical studies of cannabis tolerance and dependence. Ann N Y Acad Sci 282:221–239
Kedzior KK, Martin-Iverson M (2007) Attention-dependent reduction in prepulse inhibition of the startle reflex in cannabis users and schizophrenia patients—a pilot study. Eur J Pharmacol 560:176–182
Kedzior KK, Badcock JC, Martin-Iverson MT (2006) Validity and consistency of self-reports regarding substance use in general research volunteers, including regular cannabis users and schizophrenia patients. Subst Use Misuse 41:743–750
Kouri E, Pope JHG, Yurgelun-Todd D, Gruber S (1995) Attributes of heavy vs. occasional marijuana smokers in a college population. Biol Psychiatry 38:475–481
Kumari V, Gray J (1999) Smoking withdrawal, nicotine dependence and prepulse inhibition of the acoustic startle reflex. Psychopharmacology (Berlin) 141:11–15
Kumari V, Soni W, Sharma T (2001) Influence of cigarette smoking on prepulse inhibition of the acoustic startle response in schizophrenia. Hum Psychopharmacol 16:321–326
Langendam MW, van Haastrecht HJA, van Ameijden EJC (1999) The validity of drug users' self-reports in a non-treatment setting: prevalence and predictors of incorrect reporting methadone treatment modalities. Int J Epidemiol 28:514–520
Malone DT, Taylor DA (2006) The effect of Delta9-tetrahydrocannabinol on sensorimotor gating in socially isolated rats. Behav Brain Res 166:101–109
Mann C, Croft RJ, Scholes KE, Dunne A, O'Neill BV, Leung S, Copolov D, Phan KL, Nathan PJ (2007) Differential effects of acute serotonin and dopamine depletion on prepulse inhibition and P50 suppression measures of sensorimotor and sensory gating in humans. Neuropsychopharmacology 33:1653–1666
Martin GW, Wilkinson DA, Kapur BM (1988) Validation of self-reported cannabis use by urine analysis. Addict Behav 13:147–150
Martin RS, Secchi RL, Sung E, Lemaire M, Bonhaus DW, Hedley LR, Lowe DA (2003) Effects of cannabinoid receptor ligands on psychosis-relevant behavior models in the rat. Psychopharmacology (Berlin) 165:128–135
Martin-Iverson M, Cornelisse V (2005) Cannabinoid agonist effects on the startle reflex and its prepulse inhibition depend upon corticosteroid levels. Program No. 936.4 Society of Neuroscience, Nov 12–16
Martin-Iverson M, Stevenson K (2005) Apomorphine effects on emotional modulation of the startle reflex in rats. Psychopharmacology (Berlin) 181:60–70
Moskowitz H, McGlothlin W (1974) Effects of marihuana on auditory signal detection. Psychopharmacology (Berlin) 40:137–145
Nagai H, Egashira N, Sano K, Ogata A, Mizuki A, Mishima K, Iwasaki K, Shoyama Y, Nishimura R, Fujiwara M (2006) Antipsychotics improve [Delta]9-tetrahydrocannabinol-induced impairment of the prepulse inhibition of the startle reflex in mice. Pharmacol Biochem Behav 84:330–336
Oranje B, Geyer MA, Bocker KBE, Kenemans JL, Verbaten MN (2006) Prepulse inhibition and P50 suppression: commonalities and dissociations. Psychiatry Res 143:147–158
Peeke SC, Peeke HVS (1984) Attention, memory, and cigarette smoking. Psychopharmacology (Berlin) 84:205–216
Pope HG, Gruber AJ, Yurgelun-Todd D (1995) The residual neuropsychological effects of cannabis: the current status of research. Drug Alcohol Depend 38:25–34
Pope HG, Yurgelun-Todd D (1996) The residual cognitive effects of heavy marijuana use in college students. JAMA 275:521–527
Pope HG, Gruber AJ, Hudson JI, Huestis MA, Yurgelun-Todd D (2001) Neuropsychological performance in longterm cannabis users. Arch Gen Psychiatry 58:909–915
Quednow BB, Kuhn K-U, Hoenig K, Maier W, Wagner M (2004) Prepulse inhibition and habituation of acoustic startle response in male MDMA (‘ecstasy’) users, cannabis users, and healthy controls. Neuropsychopharmacology 29:982–990
Rentzch J, Penzhorn A, Kernbichler K, Plockl D, Gomez-Carrillo de Castro AG, Gallinat J, Jockres-Scherubl MC (2007) Differential impact of heavy cannabis use on sensory gating in schizophrenic patients and otherwise healthy controls. Exp Neurol 205:241–249
Schicatano EJ, Blumenthal TD (1995) The effects of different doses of caffeine on habituation of the human acoustic startle reflex. Pharmacol Biochem Behav 52:231–236
Schicatano EJ, Blumenthal TD (1998) The effects of caffeine and directed attention on acoustic startle habituation. Pharmacol Biochem Behav 59:145–150
Schneider M, Koch M (2002) The cannabinoid agonist WIN 55, 212–2 reduces sensorimotor gating and recognition memory in rats. Behav Pharmacol 13:29–37
Schneider JK, Koch M (2003) Chronic pubertal, but not adult chronic cannabinoid treatment impairs sensorimotor gating, recognition memory, and the performance in a progressive ratio task in adult rats. Neuropsychopharmacology 28:1760–1769
Schneider JK, Drews E, Koch M (2005) Behavioral effects in adult rats of chronic prepubertal treatment with the cannabinoid receptor agonist WIN 55, 212–2. Behav Pharmacol 16:447–454
Scholes KE, Martin-Iverson MT (2009) Disturbed prepulse inhibition in patients with schizophrenia is consequential to dysfunction of selective attention. Psychophysiology (in press)
Sheehan DV, Lecrubier Y, Sheehan KH, Janavs J, Weiller E, Keskiner A, Schinka J, Knapp E, Sheehan MF, Dunbar GC (1997) The validity of the Mini International Neuropsychiatric Interview (MINI) according to the SCID-P and its reliability. Eur Psychiatry 12:232–241
Sheehan DV, Lecrubier Y, Sheehan H, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC (1998) The Mini-International Neuropsychiatric Interview (M.I.N.I): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 59(Supplement 20):22–57
Skosnik PD, Spatz-Glenn L, Park S (2001) Cannabis use is associated with schizotypy and attentional disinhibition. Schizophr Res 48:83–92
Solowij N (1995) Do cognitive impairments recover following cessation of cannabis use. Life Sci 56:2119–2126
Solowij N, Michie PT (2007) Cannabis and cognitive dysfunction: parallels with endophenotypes of schizophrenia. J Psychiatry Neurosci 32:30–52
Solowij N, Michie PT, Fox AM (1995) Differential impairments of selective attention due to frequency and duration of cannabis use. Biol Psychiatry 37:731–739
Solowij N, Stephens RS, Roffman RA, Babor T, Kadden R, Miller M, Christiansen K, McRee B, Vendetti J (2002) Cognitive functioning of long-term heavy cannabis users seeking treatment. JAMA 287:1123–1131
Stanley-Cary CC, Harris C, Martin-Iverson M (2002) Differing effects of the cannabinoid agonist, CP 55, 940, in an alcohol or Tween 80 solvent, on prepulse inhibition of the acoustic startle reflex in the rat. Behav Pharmacol 12:1–15
Stoddart CW, Noonan J, Martin-Iverson MT (2008) Stimulus quality affects expression of the acoustic startle response and prepulse inhibition in mice. Behav Neurosci 122:516–526
Strube MJ, Bobko P (1989) Testing hypotheses about ordinal interactions: simulations and further comments. J Appl Psychol 74:247–252
Swerdlow NR, Eastvold A, Gerbranda T, Uyan KM, Hartman P, Doan Q, Auerbach P (2000) Effects of caffeine on sensorimotor gating of the startle reflex in normal control subjects: impact of caffeine intake and withdrawal. Psychopharmacology (Berlin) 151:368–378
Swerdlow N, Stephany N, Wasserman LC, Talledo J, Shoemaker J, Auerbach PP (2003) Amphetamine effects on prepulse inhibition across-species: replication and parametric extension. Neuropsychopharmacology 28:640–650
Turetsky BI, Calkins ME, Light GA, Olincy A, Radant AD, Swerdlow NR (2007) Neurophysiological endophenotypes of schizophrenia: the viability of selected candidate measures. Schizophr Bull 33:69–94
Wegener N, Kuhnert S, Thuns A, Roese R, Koch M (2008) Effects of acute systemic and intra-cerebral stimulation of cannabinoid receptors on sensorimotor gating, locomotion and spatial memory in rats. Psychopharmacology (Berlin) 198:375–385
Yee B, Chang T, Pietropaolo S, Feldon J (2005) The expression of prepulse inhibition of the acoustic startle reflex as a function of three pulse stimulus intensities, three prepulse stimulus intensities, and three levels of startle responsiveness in C57BL6/J mice. Behav Brain Res 163:265–267
Zachariou M, Dissanayake DWN, Coombes S, Owen MJ, Mason R (2008) Sensory gating and its modulation by cannabinoids: electrophysiological, computational and mathematical analysis. Cognitive Neurodynamics 2:159–170
Acknowledgements
We gratefully acknowledge Peter Hackett and Rose Kwa for GCMS and CEDIA toxicology analyses.
Ethical standards
The experiment detailed in the current manuscript complied with the current laws in Australia.
Conflict of interest
Both KES and MTM-I declare no actual or potential conflicts of interest. Both authors have full control over all the data presented here, and agree to allow the journal to review the data if requested.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Scholes, K.E., Martin-Iverson, M.T. Alterations to pre-pulse inhibition (PPI) in chronic cannabis users are secondary to sustained attention deficits. Psychopharmacology 207, 469–484 (2009). https://doi.org/10.1007/s00213-009-1679-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-009-1679-0