
Abstract
Metabolic syndrome is defined by a constellation of complex coexisting cardiometabolic risk factors such as hyperglycemia, dyslipidemia, inflammation, abdominal obesity, coagulopathies, and hypertension that raise the risk of diabetes mellitus and cardiovascular disease. Recently, there has been an increasing interest in the use of herbs and natural compounds in prevention and treatment of diseases and a large number of published articles have focused on this issue. Rosmarinus officinalis L. or rosemary (Lamiaceae) is a rich source of phenolic phytochemicals having significant anti-oxidant, anti-inflammatory, hypoglycemic, hypolipidemic, hypotensive, anti-atherosclerotic, anti-thrombotic, hepatoprotective, and hypocholesterolemic effects. The purpose of this review is to highlight the interesting pharmacological effects of rosemary, and its active compounds, and the related mechanisms in the management of metabolic syndrome that are documented in in vitro and in vivo studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Metabolic syndrome (syndrome X) is defined as a complex metabolic disorder with disturbance of glucose metabolism (insulin resistance, high blood glucose, and impaired glucose tolerance), central obesity and being overweight, abnormalities in serum lipid levels, hypertension, and atherosclerosis (Alberti et al. 2006; Miranda et al. 2005). It is considered as a major public health problem and the cause of morbidity and mortality due to high risks for developing cardiovascular diseases (Isomaa et al. 2001) and diabetes mellitus (Haffner et al. 1992). According to the National Cholesterol Education Program (NCEP) criteria, diagnosis of the metabolic syndrome is confirmed in person who meets at least three of the following: abdominal obesity: waist circumference >102 cm in men and >89 cm in women (in case of body mass index (BMI) >30 kg/m2, central obesity can be assumed instead of measuring waist circumference), raised plasma triacylglycerol (TG) ≥150 mg/dL, reduced high-density lipoprotein cholesterol (HDL-C) <40 mg/dL in men or <50 mg/dL in women, raised blood pressure ≥130/85 mm Hg, and fasting plasma glucose of 110 to 125 mg/dL (Alberti et al. 2005; Miranda et al. 2005).
Medicinal plants have been in the center of attention for the following: their potential effect in improving and maintaining human health, low side effects, and low costs for thousands of years. They are commonly used to treat various disorders such as dyslipidemia and hypertension and to restore metabolic balance (Huang et al. 2005; Ramadan et al. 2013). So, identifying herbs and their active compounds with these effects can be a good choice in the treatment of metabolic syndrome (Hosseini and Hosseinzadeh 2015; Hosseinzadeh and Nassiri-Asl 2014; Razavi and Hosseinzadeh 2014; Sahebkar 2013). Rosmarinus officinalis Linn. (rosemary) belonging to the family Lamiaceae is an evergreen aromatic plant with 1-m height, upright stems, whitish-blue flowers, and dark green leaves distributed in the Mediterranean region. Rosemary extract, especially the leave extract, was shown to be one of the most popular herbal products that has been consumed as a flavoring and anti-oxidant agent in food conservation and cosmetics (Cui et al. 2012; Perez-Fons et al. 2010). In many countries, rosemary is frequently used as a medicinal plant in the traditional and modern medicines to treat diabetes complications and hypertension (Amel 2013; Javanmardi et al. 2003; Martynyuk et al. 2014). In folk medicine, it is widely used as a remedy for several purposes like reducing pain, anti-spasmodic in renal colic and dysmenorrhea, anti-rheumatic, carminative, cholagogue, diuretic, expectorant, anti-convulsant, stimulating hair growth (hair tonics, hair lotion), and many other effects (al-Sereiti MR et al. 1999). Hypoglycemic (Ramadan et al. 2013), anti-atherogenic (Ullevig et al. 2011), anti-hypertensive (Kwon et al. 2006), hypocholesterolemic (Afonso et al. 2013), anti-oxidant and anti-inflammatory (Rocha et al. 2015), hepatoprotective (Fahim et al. 1999), anti-depressant (Sasaki et al. 2013), anti-proliferative (Tai et al. 2012), and anti-bacterial (Wang et al. 2012b) activities; diminishing morphine withdrawal syndrome (Hosseinzadeh and Nourbakhsh 2003; Hosseinzadeh et al. 2006); healing diabetic wounds (Abu-Al-Basal 2010; Umasankar et al. 2012); and the treatment of cognitive disorder (Hosseinzadeh et al. 2004) are approved as diverse pharmacological activities for rosemary in modern scientific research projects. It has also been reported that the bioactive compounds of rosemary have either direct or indirect epigenetic targets in cancer chemoprevention and chemotherapy and hold great potential in the prevention and the therapy of a wide variety of diseases by altering various epigenetic modifications (Meeran et al. 2010). Analysis of chemical composition of different rosemary extracts shows that the most important pharmacologically active constituents are phenolic diterpenes, triterpenes, and phenolic acids such as carnosic acid (CA), carnosol, rosmanol, ursolic acid, betulinic acid, and rosmarinic acid (RA) (al-Sereiti MR et al. 1999; Borras-Linares et al. 2014; Okamura et al. 1994; Tu et al. 2013). The chemical structures of these compounds of rosemary are presented in Fig. 1. Among the isolated phenolic compounds, CA and RA have been shown to possess predominant pharmacological effects of rosemary including anti-oxidant, anti-inflammatory, anti-viral, and anti-bacterial actions and to interact with multiple molecular targets that are involved in the pathogenesis of metabolic syndrome (Birtic et al. 2015; Jayanthy and Subramanian 2014; Lipina and Hundal 2014; Sedighi et al. 2015). The aims of the present review are to summarize the potential efficacy of rosemary and its active compounds in metabolic syndrome and to identify the underlying mechanisms of action.

Chemical structures of rosemary constituents
Effects on diabetes and on the lipid profile
Suppression of gluconeogenesis
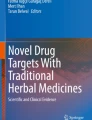
High blood glucose concentration in type II diabetes is the final result of imbalance among intestinal absorption, gluconeogenesis in the liver, glucose consumption, and uptake by the peripheral tissues. There are several enzymes that control gluconeogenesis in the liver including cytosolic phosphoenolpyruvate carboxykinase (PEPCK-C) and glucose-6-phosphatase (G6Pase). Cyclic adenosine monophosphate (CAMP) response element binding protein (CREB: a transcription factor) which is activated via the adenylate cyclase/cAMP/protein kinase A (AC/cAMP/PKA) signaling pathway binds to the promoters of the PEPCK-C, G6Pase, and peroxisome proliferator-activated receptor (PPAR)-γ coactivator-1α (PGC1α) genes (a transcription coactivator which induces PEPCK-C and G6Pase) and enhances their transcription (Herzig et al. 2001). So, suppression of these enzymes or related genes results in the reduction of fasting blood glucose and are important goals for managing type II diabetes. According to these facts, results of Yun et al. (2013) study showed that 100 μg/mL methanolic extract of rosemary especially 7-O-methylrosmanol and royleanonic acid constituents in HepG2 cells suppressed the cAMP responsiveness of gluconeogenic genes, PEPCK-C and G6Pase promoters. Carnosol showed suppressive activity toward cAMP/CREB-induced gene expression under the G6Pase promoter control. So, inhibition of the cAMP/PKA/CREB pathway may involve in the mechanism of action of rosemary-induced reduction of fasting blood glucose (Yun et al. 2013). In a model of type 2 diabetes, RA (100 mg/kg) decreased blood glucose, urine sugar, and glycosylated hemoglobin (HbA1C), which is an important predictor of diabetic complications and long-term glycemic control. These effects were exhibited through the modulation of carbohydrate-metabolizing enzymes such as hexokinase, pyruvate kinase (glycolytic enzymes), and G6Pase and fructose 1,6-bisphosphatase (gluconeogenic enzymes) and glycogen metabolism (Jayanthy and Subramanian 2014). Hormone-sensitive lipase (HSL) is a kind of neutral lipase which catalyzes the hydrolysis of triglycerides leading to a flux of free fatty acids (FFAs) from the adipocytes. Since the activity of this enzyme is normally inhibited by insulin, in type 2 diabetes (insulin resistance) suppression of the HSL activity is diminished resulting in excessive FFAs levels in plasma. Plasma FFA levels are involved in the modulation of carbohydrate metabolism in several tissues, including liver and muscle (Voshol et al. 2003). Elevated FFA levels stimulate overproduction of glucose in the liver and contribute to the inhibition of glucose uptake and utilization by muscles (Bergman and Ader 2000). Bustanji et al. (2010) undertook an investigation to identify how rosemary could ameliorate the blood glucose and lipid profile simultaneously. In in vitro assay, they revealed that methanol rosemary extract dose dependently (with the component gallic acid: IC50 14.5 μg/mL) inhibited the activity of this enzyme (Bustanji et al. 2010) (Fig. 2).

Rosemary and related compounds improve lipid and glucose metabolism through multiple mechanisms: A suppressing the cAMP responsiveness of gluconeogenic genes, PEPCK-C, and G6Pase; B up-regulation of LDLR; C activation of the AMPK and PPAR signaling pathways, up-regulation of sirtuin 1, and PGC1α; D increasing insulin secretion; and E modulation of carbohydrate-metabolizing enzymes and glycogen metabolisms. There is no information about the receptors involved in these effects. AC adenylate cyclase, AMPK AMP-activated protein kinase, CREB cAMP response element binding protein, FP fructose 1,6-bisphosphatase, G6Pase glucose-6-phosphatase, GP glycogen phosphorylase, GS glycogen synthase, HK hexokinase (glycolysis), LDLR low-density lipoprotein receptor, PEPCK-C cytosolic phosphoenol pyruvate carboxykinase, PGC PPAR-γ coactivator, PK pyruvate kinase (glycolysis), PKA protein kinase A, SIRT1 sirtuin 1, PPAR peroxisome proliferator-activated receptor
Inhibition of the breakdown of carbohydrates
An important carbohydrate in daily dietary is starch which is converted to monosaccharides by α-glucosidase (AGc) and α-amylase in the small intestines. Oral administration of rosemary-distilled extract to normal and diabetic mice was effective in reduction of plasma glucose levels. The anti-diabetic effect of rosemary observed in this study was deduced from the activity of the active compounds in inhibiting the action of AGc (maltase and sucrase) in the diabetic group (Koga et al. 2006). In biochemical tests, the aqueous and methanol extracts of rosemary inhibited AGc and α-amylase activities (Cazzola et al. 2011). In another survey, α-amylase inhibitory effects of RA were also seen on porcine pancreatic amylase (McCue and Shetty 2004). The aqueous extract of clonal herbs of Lamiaceae species especially rosemary and the active phenolic compounds including caffeic acid and RA (water extracts contained more phenolic compound than ethanol extracts) had also a great AGc inhibitory activity (68 %), but they did not have inhibitory effects on α-amylase activity (Kwon et al. 2006).
Regulation of PPAR-γ
PPAR-γ, which is a nuclear receptor protein, controls the glucose transport and metabolism and the transcription of the proteins and enzymes responsible for glucose and fatty acid cellular uptake (Scazzocchio et al. 2011). PPAR-γ agonists like thiazolidinediones (glitazones), a class of hypoglycemics, have shown to increase glucose catabolism and decrease hepatic glucose output. In skeletal muscle, PPAR-γ increases glucose uptake to lower blood glucose levels, and in the liver, G-protein downregulation may mediate PPAR-γ-elicited insulin sensitization (Jay and Ren 2007). In Rau et al. (2006) research, 80 % using a reporter gene assay aqueous ethanol extract of rosemary was effective in PPAR-γ activation. The analysis of active constituents revealed that both phenolic diterpene compounds carnosol and CA were responsible for these effects, and as a result, it can be a part of the mechanism of anti-hyperglycemic effects of rosemary like glitazone, a type of glucose-lowering drugs (Rau et al. 2006). Based on the anti-oxidant and ameliorating effects of dichloromethane-methanol rosemary extract on complications associated with type-2 diabetes mellitus and obesity, Tu et al. 2013, described the mechanism of metabolic regulation of the extract in HepG2 cells. The rosemary extract showed hypoglycemic and hypolipidemic effects by activation of signaling pathways including AMP-activated protein kinase (AMPK) (which induce glycolysis) and PPAR-γ and up-regulation of low-density lipoprotein cholesterol (LDL-C) receptor (responsible for endocytosis of LDL-C from circulation to liver hepatocytes), sirtuin 1 (increases fatty acid oxidation), and PGC1α (activates PPAR-γ) (Tu et al. 2013) (Fig. 2). Findings of another survey implied that CA in 3T3-L1 adipocytes increased the PPAR-γ messenger RNA (mRNA) expression, suppressed activation of nuclear factor-κB (NF-κB) (which is activated by tumor necrosis factor-α (TNF-α) and inhibits the activity of PPAR-γ in adipocytes), and improved glucose uptake through promotion of glucose transporter type 4 (GLUT4) translocation in adipocytes (Tsai et al. 2014).
Reduction of inflammatory cytokines
Low-grade chronic inflammation in adipose tissue is associated with obesity and insulin resistance. Inflammatory cytokines, such as TNF-α, interleukin 6 (IL-6), and monocyte chemotactic protein-1 (MCP-1), secreted by adipose tissue, inhibit the expression of GLUT4, mediating glucose uptake in adipocytes, and cause insulin resistance (Tsai et al. 2014; Xie et al. 2010). The results of the study done by Tsai et al. (2014) indicated that CA reduced the TNF-α-mediated inflammation and improved insulin resistance in 3T3-L1 adipocytes. The mechanism has been suggested to be inhibition of mRNA expression of the inflammatory genes (IL-6 and MCP-1) and protein levels of multiple agents of mitogen-activated protein kinase (MAPK) signaling pathway (extracellular signal-regulated kinase [ERK] and c-Jun NH2-terminal kinase [JNK]), mammalian target of rapamycin (mTOR), and forkhead transcription factor 1(FOXO1 binds to PPAR-γ and inhibits its function) (Tsai et al. 2014). Ursolic acid (UA), b-hydroxy-12-urs-12-en-28-oic acid, a pentacyclic triterpenoid carboxylic acid with anti-oxidant, anti-inflammatory, anti-tumor, anti-atherosclerotic, and anti-hypertensive activities, is another bioactive compound of rosemary. The inhibition of T cell and B cell proliferation, ERK, JNK, MAPK kinase, and c-raf phosphorylation, which control T cell survival; suppression of regulators of antigen-induced immune response including NF-κB, nuclear factor of activated T cell (NF-AT), and activator protein-1(AT-1); and reduction of the IL-1b, TNF-α, and IL-6 secretion are responsible for anti-inflammatory actions of UA (Checker et al. 2012).
Anti-oxidative stress
Hyperglycemia induces oxidative stress through generation of free radicals that results in development of diabetic complications such as atherosclerosis, hyperlipidemia, hypertension, and tissue and cell (like pancreatic β-cells) damages (Bakirel et al. 2008). As expression of anti-oxidant enzymes is low in pancreatic β-cells, they are particularly susceptible to the deleterious effects of reactive oxygen species (ROS) which induce apoptosis and suppress insulin biosynthesis (El-Alfy et al. 2005; Vijayakumar et al. 2006). So, the anti-oxidant agents can protect the functional β-cells from further deterioration or they can induce the regeneration of β-cells by alleviating the oxidative damage. Oral administration of high doses of ethanol rosemary extract (especially 200 mg/kg) reduced blood glucose, in normoglycemic and glucose-hyperglycemic rabbits. Evaluation of in vivo anti-oxidant activity revealed that the rosemary extract reduced serum malondialdehyde (MDA) (as a marker of lipid peroxidation) and elevated activities of serum superoxide dismutase (SOD) and catalase (CAT) (an anti-oxidant enzymes) (Bakirel et al. 2008). Ameliorating effect of endurance exercise with aqueous rosemary extract on blood anti-oxidant enzyme activities and lipid peroxidation was also demonstrated in Nazem et al. (2015) research. Anti-hyperlipidemic and anti-oxidant effects of two kinds of rosemary extracts including aqueous (major compound: RA) and nonesterified phenolic fraction (NEPF) (major compound: CA) were evaluated in hypercholesterolemic rats. Both kinds of extracts increased anti-oxidant enzymes activity in liver and kidney. The NEPF showed no significant effect on the hyperlipidemia, but the aqueous rosemary extract improved the lipid profile (70 mg/kg) (Afonso et al. 2013).
Anti-hyperlipidemic effects
Hyperlipidemia is known to be a cause of lipid peroxidation and atherosclerosis. The lipid-lowering and anti-oxidant activities of aqueous rosemary extract (RA was the most important active constituent), essential oil, and crude plant powder (mixture of hydrophilic and lipophilic compounds are similar to the aqueous extract and essential oils, respectively) were studied in high-fat-diet-fed SD rats (hyperlipidemia rat model). The effects of these three forms were different on hyperlipidemic rats. While essential oil in all doses resulted in higher cholesterol levels, the aqueous extract and the plant powder with greater extent decreased the serum cholesterol levels. The lowering effect on TG levels was obvious with the essential oil and more significant with the powder. The aqueous extract, essential oil, and crude plant powder reduced MDA levels, increased serum HDL-C levels and SOD activity, and improved anti-oxidant capacity (Wu et al. 2011). In another attempt, Al Sheyab et al. (2012) found that administration of 100 mg/kg aqueous rosemary extract to the mice on a high fat diet reduced the plasma levels of total cholesterol, TG, and LDL-C and increased the HDL-C levels.
Improvement of insulin action and secretion
Type 2 diabetes mellitus is characterized by high blood glucose and insulin resistance. Lipina and Hundal 2014 reported that CA at 20-μM concentration like insulin stimulated glucose clearance by rat skeletal L6 myotube through protein phosphatase methylesterase-1/ protein phosphatase 2A/ protein kinase B or Akt (PME-1/PP2A/PKB) signaling axis. It also increased the translocation of the GLUT4 to plasma membrane. Mechanistically, CA increased demethylation (inactivation) of the PP2A catalytic subunit through PME-1, so reduced the suppressive effects of PP2A on PKB which mediates insulin-induced glucose uptake in skeletal muscle independent of AMPK. Moreover, this study indicated that the effect of CA on glucose uptake was not mediated by PPAR-γ signaling pathway and anti-oxidant activities in L6 myotube (Lipina and Hundal 2014). Naimi et al. (2015) showed that methanol rosemary extract stimulated L6 myotube glucose uptake through increasing AMPK and acetyl-CoA carboxylase (ACC) phosphorylation but did not affect GLUT4 or GLUT1 translocation or insulin receptor substrate 1/phosphoinositide 3-kinase (PI3K)/Akt signaling cascade which is involved in the insulin-stimulated glucose uptake (Naimi et al. 2015). In another study, the effects of greenhouse-grown or commercially purchased herbs on dipeptidyl peptidase IV and protein tyrosine phosphatase 1B were evaluated. Inhibition of these two enzymes results in the improvement of insulin secretion and insulin signaling cascade, respectively. Among all of the herbs, rosemary extract was one of the most potent inhibitors of the mentioned enzymes (Bower et al. 2014). Β-Hydroxy-lup-20(29)-en-28-oic acid (betulinic acid (BA)) is a pentacyclic triterpenoid found in hydroalcoholic extract of aerial parts of rosemary. Different doses of BA (especially 10 mg/kg) in male Wistar rats mimicked insulin action and increased insulin secretion, glucose uptake, and glycogen content in muscle via PI3K and MAPK pathway which stimulates GLUT4 synthesis and translocation (Castro et al. 2014).
Obesity
Modulation of lipid synthesis and lipolysis and inhibition of adipocyte differentiation
Obesity is a major public health problem which is characterized by disequilibrium between lipogenic and lipolytic processes which cause storage of excessive fat in the form of TG in white adipose tissue and predispose person to diabetes, coronary heart disease, and hypertension (Langin 2006). Diacylglycerol acyltransferase (DGAT2 and DGAT1), proved to be one of the drug targets in pharmacological studies, is a major enzyme responsible for TG synthesis. Abietane-type diterpenes and, especially carnosol (40 μm), which is one of the main compounds of the methanol rosemary extract, could suppress DGAT1 activity moderately in in vitro assay and exhibited inhibitory effects on intracellular TG synthesis in human hepatocyte HepG2 cells (Cui et al. 2012). In male obese leptin-deficient C57BL/6J-ob/ob mice model, CA showed anti-obesity activity and reduced hepatic lipid accumulation, food intake, and body weight gain. These metabolic effects were related to decreasing hepatic lipogenesis gene expression (liver fatty acid-binding protein, stearoyl-CoA desaturase 1 (SCD1), fatty acid synthase), regulator of calcineurin 2–3 mRNA expression, which regulates food intake and weight gain, and increasing fatty acid oxidation molecules (carnitine palmitoyltransferase 1, uncoupling protein 2) (Park and Sung 2015a). Treatment with 500 mg/kg of a standard aqueous rosemary extract containing 20 % CA in C57BL/6J mice on a high-fat diet significantly reduced weight gain and cholesterol levels through increasing fecal fat and energy excretion, the inhibition of the pancreatic lipase activity, and the activation of PPAR-γ (30 μg/mL) but did not affect the food or energy intake. The pharmacological dose of the extract used in this study was based on the normal dietary exposure of CA estimated in adults and preschool children (0 · 04 and 0 · 11 mg/kg, respectively) by the European Food Safety Authority Panel on Food Additives (Ibarra et al. 2011). Consumption of a diet containing rosemary ethanol extract rich in CA (40 %) modulated serum lipids, increased fecal weight, and reduced weight gain in obese female Zucker rats. These effects were accompanied with the inhibition of lipase activity in the stomach and reduction of fat absorption, modification of microbiota composition, and decrease in β-glucosidase activity in the cecum of both groups as shown by Romo Vaquero et al. (2012). In intestinal microbiota, β-glucosidase contributes to the fermentation of non-digested polysaccharides to short-chain fatty acids (Romo-Vaquero et al. 2014b; Romo Vaquero et al. 2012). So, the inhibition of the activity of this enzyme reduces dietary energy extraction from short-chain fatty acids which turns into host carbohydrates and lipids. The differentiation of the adipocytes and increase in their size are other causes of obesity and considered as therapeutic targets for the treatment of obesity. Acetone rosemary extract and CA in murine 3T3-L1 cells inhibited preadipocyte differentiation, exerted anti-adipogenic effects, and blocked mitotic clonal expansion and expression of PPAR-γ and CCAAT/enhancer-binding protein α (C/EBPα), which are critical for acquiring the adipocyte phenotype (Gaya et al. 2013). In Park and Sung 2015b study, CA in 3T3-L1 adipocytes suppressed adipogenesis and lipid accumulation. Downregulation of adipogenesis-related genes (PPAR-γ, C/EBPα, SCD1, and SREBP1) and decreasing glycerol 3-phosphate dehydrogenase activity, a key enzyme involved in TG synthesis, are the reported mechanisms for anti-adipogenic effects of CA (Park and Sung 2015b). The endogenous activators of all members of the PPAR family are a variety of fatty acids, which suggests that the PPARs are highly involved in lipid metabolism. Moreover, it has been shown that ligands for this receptor (like thiazolidinediones) have emerged as potent insulin sensitizers used in the treatment of type 2 diabetes. Increased levels of circulating FFAs and lipid accumulation in non-adipose tissue have been implicated in the development of insulin resistance. This situation is improved by PPAR-γ ligands, which promote fatty acid storage in fat depots and regulate the expression of adipocyte-secreted hormones that impact on glucose homeostasis. Although the result is the improvement of insulin sensitivity, undesired side effects such as weight gain through the increased adipogenesis and fat storage limit the utility of this therapy (Larsen et al. 2003; Rangwala and Lazar 2004). So, more studies need to be done on rosemary to dissociate the anti-diabetic and the adverse effects. It may be possible through finding or synthesizing new derivatives that selectively target the PPAR-γ in the desired tissue. The regulatory effects of a commercial rosemary extract on specific genes and also microRNAs that play a role in adipogenesis and the pathogenesis of obesity were evaluated in Stefanon et al. (2015) research. The induction of phase 2 enzymes related to glutathione metabolism and increased levels of total reduced glutathione (GSH) through activation of transcription factor Nrf2 (nuclear factor (erythroid-derived 2)-like 2 is a regulator of phase2 enzyme expression) are other mechanisms for inhibition of 3T3-L1 adipocyte differentiation by CA and carnosol (Takahashi et al. 2009).
Anti-inflammatory effects
Obesity is associated with the activation of the innate immune system that alters metabolic homeostasis over time. Analysis of gene expression networks in adipose tissue identified a signature gene expression pattern enriched for macrophage activation gene that predicted risk for the features of metabolic syndrome. In addition, elevated production of inflammatory cytokines, decreased protective factors (e.g., adiponectin), and communication between inflammatory and metabolic cells appear to contribute to the link between inflammation and metabolic dysfunction (Lumeng CN and Saltiel 2011). In obese individuals, production of many inflammatory cytokines including TNF-α, IL-1β, and leptin is increased by adipocytes (adipokines). In contrast, the levels of anti-inflammatory adipokines (adiponectin) are reduced. These imbalances induce inflammatory processes and signaling pathways (AMPK, PPARs) and negatively affect different organs (liver, brain, adipose tissue, and muscle) (Romo-Vaquero et al. 2014a). Reduced serum inflammatory cytokine levels, MCP-1, TNF-α, and IL-6, which contribute to insulin resistance and diabetes, are another observed mechanism for anti-inflammatory effects of CA in obesity (Park and Sung 2015a). Consuming a diet containing rosemary extract enriched in CA (40 %) in lean and obese female Zucker rats resulted in increased adiponectin levels (has anti-inflammatory effects, improves insulin resistance, reduces serum TG levels and weight) and induction of PGC1α gene expression (improves fatty acid oxidation and insulin-stimulated glucose transport) (lean rats). Modulation of the transcript levels of phase I and II metabolizing enzyme gene expression such as cytochromes P450 and glutathione transferases (in both groups) and decrease in adipokines (lean group) and adenosine monophosphate activated protein kinase (pAMPK) (obese group) levels are other mechanisms underlying the anti-inflammatory effects of CA (Romo-Vaquero et al. 2014a). The activation of Toll-like receptors (TLRs), which results in increased IL-6 and MCP-1 levels via ERK signaling pathway and NF-κB (which is activated through myeloid differentiation factor 88: MyD88 and TNF receptor-associated factor 6: TRAF6) in adipocytes, is recognized in chronic inflammation induced by obesity. CA dose dependently decreased inflammatory cytokines (TNF-α, IL-6, and MCP-1); TLR4 mRNA expression; and MyD88, TRAF6, p-ERK, and NF-κB (10 and 20 μM) protein levels in lipopolysaccharide-induced inflammation in 3T3-L1 adipocyte (Park and Mun 2014). In other experience in ob/ob mice, Wang et al. 2011 demonstrated that CA (0.05 % w/w) induced weight loss in 3 weeks and reduced serum lipids, as well as liver TG content, and size of visceral fat regions. According to Wang et al. 2012a, these effects were mediated by reduced inflammatory cytokine levels such as IL-1β, IL-12, IL-17, interferon (IFN)-γ, macrophage inflammatory protein-1β, MCP-1, and hepatic levels of PPAR-γ (which is a regulator of TG homeostasis and contributes to hepatic steatosis). Moreover, CA activated signaling molecules such as AMPK, ACC, and MAPK (ERK 1/2) and upstream regulators epithelium growth factor receptor which inhibit preadipocyte proliferation and differentiation (Wang et al. 2012a). It has also been demonstrated that obese adipose tissue is characterized by the enhanced infiltration of macrophages that produce various inflammatory cytokines such as TNF-α, IL-1β, and IL-6 and thereby contribute to inflammation. Rosemary-derived CA and carnosol strongly suppressed Gaussia luciferase secretion induced by macrophages and up-regulated adiponectin secretion and the nitric oxide production and inducible nitric oxide synthase (iNOS) gene expression by inhibiting NF-κB activation (Lo, et al. 2002; Nagasaki et al. 2012). The various anti-obesity mechanisms of rosemary and the active compounds are presented in Fig. 3.

Different anti-obesity mechanisms of rosemary and related compounds. CPT1 carnitine palmitoyltransferase 1, DGAT1 diacylglycerol acyltransferase 1, FAS fatty acid synthase, IL interleukin, INF-γ interferon-γ, L-FABP liver fatty acid-binding protein, MyD88 myeloid differentiation factor 88, PPAR peroxisome proliferator-activated receptor γ, Rcan2–3 regulator of calcineurin 2–3, SCD1 stearoyl-CoA desaturase 1, TG triglyceride, TLR4 Toll-like receptors 4, TNF-α tumor necrosis factor-α, TRAF6 TNF receptor-associated factor 6, UCP2: uncoupling protein 2
Cardiovascular effects
Anti-hypertensive and cardioprotective effects
Angiotensin I-converting enzyme (ACE-I) is a key enzyme in controlling blood pressure by producing vasoconstrictor agents, which increase the blood pressure. According to the results of in vitro studies, rosemary (25 %) in combination with cranberry (75 %) (Apostolidis et al. 2006) and the aqueous extracts of rosemary LA (one of clonal lines of rosemary) among other clonal herbs of Lamiaceae (Kwon et al. 2006) inhibited ACE-I activity. Based on the beneficial effects of omega-3 fatty acids in reducing plasma lipids, atherogenic LDL-C, and hypertension, researchers investigated the effects of a diet containing Omega-3 plus lecithin, curcumin, and rosemary extracts on the lipid disturbance, high blood pressure, and hyperinsulinemia associated with cardiovascular disease (CVD). After dietary supplementation in a double-blind placebo-controlled trial in CVD patients, a significant decrease was observed in blood pressure especially the systolic blood pressure without producing significant changes in blood glucose (Yam et al. 2002). It was also demonstrated that rosemary extract decreased the levels of blood glucose and enzyme activities related to cardiac injury and corrected the lipid profile (Alnahdi 2012). Rosmarinic acid (10 mg/kg) supplementation in fructose-fed hypertensive rats (model of insulin resistance) also reduced blood pressure and prevented cardiac injury and hypertrophy. Decrease in endothelin-1 (a vasoconstrictor) level and ACE-I activity, downregulation of the expression of NADPH oxidase p22phox subunit, increase in NO (which has vasorelaxant effect) levels, and improvement of cardiac anti-oxidant defense were the observed mechanisms for cardioprotective effects of RA (Karthik et al. 2011).
Anti-atherogenic effects
Inhibition of
Advanced glycation end products (AGEs), which trigger cytokine secretion and oxidation reactions, are produced through non-enzymatic glycation of proteins by sugar and cause vessel damage. The glycation of LDL-C, one of the pro-atherogenic factors, which enhances its oxidation and accumulation in vessel walls; polymerization of collagen that inhibits the proteolytic attacking enzyme and results in atrophy of vascular basal membranes; and the induction of thrombosis by the glycation of anti-thrombin III and plasminogen are the mechanisms by which AGEs induce platelet and endothelial cell dysfunction and vascular damage (Gugliucci 2000; Gugliucci and Menini 2002). The anti-glycation-related features of the aqueous and acetone extract of rosemary have been evaluated in biochemical tests. Both extracts of rosemary were capable of inhibiting LDL-C glycation and AGE formation in collagen. The active ingredients RA, carnosol, CA, 12-methoxycarnosic acid, and methyl carnosate also showed radical scavenging effects and potentiated the activity of the anti-thrombin III which can inhibit coagulation by lysing thrombin and other blood coagulation factors (Hsieh et al. 2007). In another study, rosemary extract (50 mg/kg) rich in high levels of phenolic compound indicated significant anti-diabetic effects and the decrease in the percentage of glycated hemoglobin (Silva et al. 2011).
Anti-chemotaxic action
Another early event in the development of atherosclerotic plaque is the recruitment and persistent accumulation of monocyte-derived macrophages in the subendothelial layer of the vessel. The release of chemokine (MCP-1) from vessels and adhesion molecules (vascular cell adhesion molecule-1 and intracellular adhesion molecule-1) and matrix metalloproteinase (MMP) expression by endothelial cells trigger these events. Then, the cells transform into lipid-laden foam cells and are characterized as early lesions of atherosclerosis (Chae et al. 2012; Ullevig et al. 2011). Ullevig et al. 2011 evaluated the potential anti-atherogenic effect of UA in high-fat-diet-fed LDL receptor-deficient mice, which develop accelerated atherosclerosis, and in in vitro model of human THP-1 monocytic cells. The result showed that dietary supplementation with UA decreased the mortality of diabetic mice (90 %), blood glucose, and the formation of atherosclerotic lesions in aortic arch. These anti-atherogenic effects of UA were attributed to reduced macrophage infiltration into the lesions and possibly anti-oxidative stress activity. In this study, 24 mg/kg/day = 1.7 g/day for a 70-kg person was estimated as the approximate efficient dose of UA for anti-atherosclerotic activity (Ullevig et al. 2011).
Inhibition of lipid oxidation
Glycation and oxidation of LDL-C and HDL-C are important in pathophysiology of atherosclerosis in diabetes. Results of Jin and Cho (2011) study revealed that aqueous extract of rosemary (less than cinnamon and clove) inhibited glycation of apolipoprotein A-I (major protein constituent of HDL-C) and LDL-C oxidation and had anti-oxidant and good radical scavenging activities (Jin and Cho 2011). Similar to the previous study, the aqueous rosemary extract rich in phenolic compounds (carnosol, RA, genkwanin, rosmadial, CA) and the methanol extract had high anti-oxidant, radical scavenging, anti-glycant, and anti-lipid peroxidation effects in biochemical tests (Cazzola et al. 2011). The inhibitory activities of CA, carnosol, RA, rosmanol, carnosol, and epirosmanol on LDL-C oxidation were also observed in human aortic endothelial cells and biochemical tests (Pearson et al. 1997; Zeng et al. 2001). So, rosemary can be a good choice for the prevention and treatment of diabetes, CVDs, and their complications.
Inhibition of vascular smooth muscle cells’ migration
Arterial endothelial dysfunction is a key marker in the pathogenesis and complication of atherosclerosis. In a clinical research done in healthy young volunteers, rosemary extract rich in carnosol, CA, and RA increased flow-mediated dilatation of the brachial artery and decreased endothelial dysfunction and plasminogen activator inhibitor-1 level (Sinkovic et al. 2011). Another key event that contributes to the progression of atherosclerosis is the proliferation and migration of vascular smooth muscle cells (VSMCs) from the tunica media into the intima and is facilitated through NF-κB-induced expression of MMP in VSMCs. Yu et al. (2008) reported that CA inhibited the TNF-α-induced migration of human aortic smooth muscle cells, MMP-9 activity, and expression through downregulation of NF-κB (Yu et al. 2008). In another investigation, CA, methanol extract (CA content 9.4 %), and n-hexane fraction (CA content 8.4 %) of rosemary reduced MMP-9 and MCP-1 activities and suppressed TNF-α-induced rat VSMC migration (Chae et al. 2012). Schematic of anti-atherogenic effects of rosemary and active compounds is presented in Fig. 4.

Inhibitory effects of rosemary on atherosclerosis plaque progression. Rosemary or the active compounds inhibit LDL-C glycation and oxidation and AGE formation in collagen, have radical scavenging activities, reduce MMP-9, MCP-1, and NF-κB activities and macrophage infiltration into the lesion, and suppress VSMC migration. AGE advanced glycation end products, AM adhesion molecules (vascular cell adhesion molecule-1 and intracellular adhesion molecule-1), LDL-C low-density lipoprotein cholesterol, MCP-1 monocyte chemotactic protein-1, MMP-9 matrix metallopeptidase 9
Some predictable adverse effect reactions
Although many studies have confirmed the positive health effects of rosemary, little research has been done to evaluate the possible risk to human health. Rosemary volatile oil at dose of 25 mg/kg administered to hyperglycemic normal and diabetic rabbits increased the plasma glucose and decreased insulin levels (al-Hader et al. 1994). In another research, the volatile oil was able to increase blood pressure in patients diagnosed with primary hypotension (Fernandez et al. 2014). Therefore, this product of rosemary should be used with caution in patients with hypertension and diabetes. In the study of Lee et al. (2007), CA showed anti-platelet activity through inhibition of cytosolic calcium mobilization in experimental model of rabbit platelet aggregation induced by arachidonic acid, U46619, collagen, and thrombin. Despite the anti-platelet activity of CA, two other active compounds of rosemary, UA and oleanolic acid, were able to potentiate platelet aggregation induced by thrombin or adenosine diphosphate (Kim et al. 2014). The hepatotoxicity and inhibitory effects of CA on cytochrome P450 (CYP) activities were indicated in primary human hepatocytes and microsomes. The hepatic toxic effects were increased in a dose-dependent manner (EC50 value of 94.8 ± 36.7 μM). The activity of important hepatic CYP like 2C9 and 3A4 was not inhibited. But, the CYP2B6 and CYP3A4 mRNA and enzyme activity were induced (Dickmann et al. 2012). So, the toxicity and drug interactions of rosemary and the pharmacologically active compounds should be considered in their therapeutic use.
Unifying data and conclusion
Metabolic syndrome is the combination of disturbances of glucose and insulin metabolism, central obesity, mild dyslipidemia, and hypertension that directly increase the risk of CVD and type 2 diabetes mellitus. Reports have established that rosemary extracts and the major phenolic constituents exert beneficial effects against diabetes, obesity, CVD, and metabolic syndrome as a whole syndrome through improvement of insulin secretion and response; inhibition of AGE production; suppression of gluconeogenesis; carbohydrate digestion; lipid synthesis; induction of lipolysis; anti-oxidant and anti-inflammatory activities; and anti-hyperlipidemic, hypotensive, and anti-atherosclerotic effects. These glorious effects are consistently related to modulation of enzymes, different critical signal transduction pathways, transcription factors, and key gene expressions. In spite of much evidence from animal and in vitro assays, more clinical studies are needed to confirm the effectiveness and safety of the phenolic compounds of rosemary in humans. Tables 1 and 2 present the most relevant in vivo and in vitro studies relating to the effects and proposed underlying the mechanisms of rosemary and its constituents in many metabolic responses.
References
Abu-Al-Basal MA (2010) Healing potential of Rosmarinus officinalis L. on full-thickness excision cutaneous wounds in alloxan-induced-diabetic BALB/c mice. J Ethnopharmacol 131:443–450. doi:10.1016/j.jep.2010.07.007
Afonso MS, De O Silva AM, Carvalho EB et al (2013) Phenolic compounds from Rosemary (Rosmarinus officinalis L.) attenuate oxidative stress and reduce blood cholesterol concentrations in diet-induced hypercholesterolemic rats. Nutr Metab 10:19. doi:10.1186/1743-7075-10-19
al-Hader AA, Hasan ZA, Aqel MB (1994) Hyperglycemic and insulin release inhibitory effects of Rosmarinus officinalis. J Ethnopharmacol 43:217–221. doi:10.1016/0378-8741(94)90046-9
al-Sereiti MR, Abu-Amer KM, Sen P (1999) Pharmacology of rosemary (Rosmarinus officinalis Linn.) and its therapeutic potentials. Indian J Exp Biol 37:124–130
Al Sheyab FM, Abuharfeil N, Salloum L, Hani RB, Awad DS (2012) The effect of rosemary (Rosmarinus officinalis. L) plant extracts on the Immune response and lipid profile in mice. J Biol Life Sci 3:31–58. doi:10.5296/jbls.v3i1.906
Alberti KG, Zimmet P, Shaw J (2005) The metabolic syndrome—a new worldwide definition. Lancet 366:1059–1062. doi:10.1016/s0140-6736(05)67402-8
Alberti KGMM, Zimmet P, Shaw J (2006) Metabolic syndrome—a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med 23:469–480. doi:10.1111/j.1464-5491.2006.01858.x
Alnahdi HS (2012) Effect of Rosmarinus officinalis extract on some cardiac enzymes of streptozotocin-induced diabetic rats. J Health Sci 2:33–37. doi:10.5923/j.health.20120204.03
Amel B (2013) Traditional treatment of high blood pressure and diabetes in Souk Ahras District. J Pharmacogn Phytother 5:12–20. doi:10.5897/JPP11.065
Apostolidis E, Kwon YI, Shetty K (2006) Potential of cranberry-based herbal synergies for diabetes and hypertension management. Asia Pac J Clin Nutr 15:433–441
Ayaz NO (2012) Antidiabetic and renoprotective effects of water extract of Rosmarinus officinalis in streptozotocin-induced diabetic rat. Afr J Pharm Pharmacol 6:2664–2669. doi:10.5897/AJPP12.319
Bakirel T, Bakirel U, Keles OU, Ulgen SG, Yardibi H (2008) In vivo assessment of antidiabetic and antioxidant activities of rosemary (Rosmarinus officinalis) in alloxan-diabetic rabbits. J Ethnopharmacol 116:64–73. doi:10.1016/j.jep.2007.10.039
Bergman RN, Ader M (2000) Free fatty acids and pathogenesis of type 2 diabetes mellitus. Trends Endocrinol Metab 11:351–356. doi:10.1016/S1043-2760(00)00323-4
Birtic S, Dussort P, Pierre FX, Bily AC, Roller M (2015) Carnosic acid. Phytochemistry 115:9–19. doi:10.1016/j.phytochem.2014.12.026
Borras-Linares I, Stojanovic Z, Quirantes-Pine R, Arraez-Roman D, Svarc-Gajic J, Fernandez-Gutierrez A, Segura-Carretero A (2014) Rosmarinus officinalis leaves as a natural source of bioactive compounds. Int J Mol Sci 15:20585–20606. doi:10.3390/ijms151120585
Bower AM, Real Hernandez LM, Berhow MA, de Mejia EG (2014) Bioactive compounds from culinary herbs inhibit a molecular target for type 2 diabetes management, dipeptidyl peptidase IV. J Agric Food Chem 62:6147–6158. doi:10.1021/jf500639f
Bustanji Y, Issa A, Mohammad M et al (2010) Inhibition of hormone sensitive lipase and pancreatic lipase by Rosmarinus officinalis extract and selected phenolic constituents. J Med Plants Res 4:2235–2242. doi:10.5897/JMPR10.399
Castro AJ, Frederico MJ, Cazarolli LH et al (2014) Betulinic acid and 1,25(OH)(2) vitamin D(3) share intracellular signal transduction in glucose homeostasis in soleus muscle. Int J Biochem Cell Biol 48:18–27. doi:10.1016/j.biocel.2013.11.020
Cazzola R, Camerotto C, Cestaro B (2011) Anti-oxidant, anti-glycant, and inhibitory activity against alpha-amylase and alpha-glucosidase of selected spices and culinary herbs. Int J Food Sci Nutr 62:175–184. doi:10.3109/09637486.2010.529068
Chae IG, Yu MH, Im NK, Jung YT, Lee J, Chun KS, Lee IS (2012) Effect of Rosemarinus officinalis L. on MMP-9, MCP-1 levels, and cell migration in RAW 264.7 and smooth muscle cells. J Med Food 15:879–886. doi:10.1089/jmf.2012.2162
Checker R et al (2012) Potent anti-inflammatory activity of ursolic acid, a triterpenoid antioxidant, is mediated through suppression of NF-kappaB, AP-1 and NF-AT. PloS one 7:e31318. doi:10.1371/journal.pone.0031318
Cui L et al (2012) Abietane diterpenoids of Rosmarinus officinalis and their diacylglycerol acyltransferase-inhibitory activity. Food Chem 132:1775–1780
Dickmann LJ, Vandenbrink BM, Lin YS (2012) In vitro hepatotoxicity and cytochrome P450 induction and inhibition characteristics of carnosic acid, a dietary supplement with antiadipogenic properties. Drug Metab Dispos 40:1263–1267. doi:10.1124/dmd.112.044909
El-Alfy AT, Ahmed AA, Fatani AJ (2005) Protective effect of red grape seeds proanthocyanidins against induction of diabetes by alloxan in rats. Pharmacol Res 52:264–270. doi:10.1016/j.phrs.2005.04.003
Emam MA (2012) Comparative evaluation of antidiabetic activity of Rosmarinus officinalis L. and Chamomile recutita in streptozotocin induced diabetic rats. Agric Biol J N Am 3:247–252. doi:10.5251/abjna.2012.3.6.247.252
Fahim FA, Esmat AY, Fadel HM, Hassan KF (1999) Allied studies on the effect of Rosmarinus officinalis L. on experimental hepatotoxicity and mutagenesis. J Food Sci Nutr 50:413–427. doi:10.1080/096374899100987
Fernandez LF, Palomino OM, Frutos G (2014) Effectiveness of Rosmarinus officinalis essential oil as antihypotensive agent in primary hypotensive patients and its influence on health-related quality of life. J Ethnopharmacol 151:509–516. doi:10.1016/j.jep.2013.11.006
Gaya M, Repetto V, Toneatto J, Anesini C, Piwien-Pilipuk G, Moreno S (2013) Antiadipogenic effect of carnosic acid, a natural compound present in Rosmarinus officinalis, is exerted through the C/EBPs and PPARgamma pathways at the onset of the differentiation program. Biochim Biophys Acta 1830:3796–3806. doi:10.1016/j.bbagen.2013.03.021
Gugliucci A (2000) Glycation as the glucose link to diabetic complications. J Am Osteopath Assoc 100:621–634
Gugliucci A, Menini T (2002) The botanical extracts of Achyrocline satureoides and Ilex paraguariensis prevent methylglyoxal-induced inhibition of plasminogen and antithrombin III. Life Sci 72:279–292. doi:10.1016/S0024-3205(02)02242-7
Haffner SM, Valdez RA, Hazuda HP, Mitchell BD, Morales PA, Stern MP (1992) Prospective analysis of the insulin-resistance syndrome (syndrome X). Diabetes 41:715–722. doi:10.2337/diabetes.41.6.715
Herzig S, Long F, Jhala US et al (2001) CREB regulates hepatic gluconeogenesis through the coactivator PGC-1. Nature 413:179–183. doi:10.1038/35093131
Hosseini A, Hosseinzadeh H (2015) A review on the effects of Allium sativum (Garlic) in metabolic syndrome. J Endocrinol Invest 38:1147–57. doi:10.1007/s40618-015-0313-8
Hosseinzadeh H, Karimi G, Noubakht M (2004) Effects of Rosmarinus officinalis L. aerial parts essential oil on intact memory and scopolamine-induced learning deficits in rats performing the Morris water maze task. J Med Plants 3:68–68
Hosseinzadeh H, Nassiri-Asl M (2014) Review of the protective effects of rutin on the metabolic function as an important dietary flavonoid. J Endocrinol Invest 37:783–788. doi:10.1007/s40618-014-0096-3
Hosseinzadeh H, Nourbakhsh M (2003) Effect of Rosmarinus officinalis L. aerial parts extract on morphine withdrawal syndrome in mice. Phytother Res 17:938–941. doi:10.1002/ptr.1311
Hosseinzadeh H, Ramezani M, Shahsavand S (2006) (2006) Effect of Rosmarinus officinalis L. aerial parts extract and fractions on morphine withdrawal syndrome in mice. J Med Plants 5:27–35
Hsieh CL, Peng CH, Chyau CC, Lin YC, Wang HE, Peng RY (2007) Low-density lipoprotein, collagen, and thrombin models reveal that Rosemarinus officinalis L. exhibits potent antiglycative effects. J Agric Food Chem 55:2884–2891. doi:10.1021/jf0631833
Huang TH-W, Kota BP, Razmovski V, Roufogalis BD (2005) Herbal or natural medicines as modulators of peroxisome proliferator-activated receptors and related nuclear receptors for therapy of metabolic syndrome. Basic Clin Pharmacol Toxicol 96:3–14. doi:10.1111/j.1742-7843.2005.pto960102.x
Ibarra A, Cases J, Roller M, Chiralt-Boix A, Coussaert A, Ripoll C (2011) Carnosic acid-rich rosemary (Rosmarinus officinalis L.) leaf extract limits weight gain and improves cholesterol levels and glycaemia in mice on a high-fat diet. Br J Nutr 106:1182–1189. doi:10.1017/s0007114511001620
Isomaa B, Almgren P, Tuomi T et al (2001) Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabet Care 24:683–689. doi:10.2337/diacare.24.4.683
Javanmardi J, Stushnoff C, Locke E, Vivanco J (2003) Antioxidant activity and total phenolic content of Iranian Ocimum accessions. Food Chem 83:547–550
Jayanthy G, Subramanian S (2014) Rosmarinic acid, a polyphenol, ameliorates hyperglycemia by regulating the key enzymes of carbohydrate metabolism in high fat diet—STZ induced experimental diabetes mellitus. Biomed Prev Nutr 4:431–437. doi:10.1016/j.bionut.2014.03.006
Jay MA, Ren J (2007) Peroxisome proliferator-activated receptor (PPAR) in metabolic syndrome and type 2 diabetes mellitus. Curr Diabet Rev 3:33–39. doi:10.2174/157339907779802067
Jin S, Cho KH (2011) Water extracts of cinnamon and clove exhibits potent inhibition of protein glycation and anti-atherosclerotic activity in vitro and in vivo hypolipidemic activity in zebrafish. Food Chem Toxicol 49:1521–1529. doi:10.1016/j.fct.2011.03.043
Karthik D, Viswanathan P, Anuradha CV (2011) Administration of rosmarinic acid reduces cardiopathology and blood pressure through inhibition of p22phox NADPH oxidase in fructose-fed hypertensive rats. J Cardiovasc Pharmacol 58:514–521. doi:10.1097/FJC.0b013e31822c265d
Kim M, Han CH, Lee MY (2014) Enhancement of platelet aggregation by ursolic acid and oleanolic acid. Biomol Ther 22:254–259. doi:10.4062/biomolther.2014.008
Koga K, Shibata H, Yoshino K, Nomoto K (2006) Effects of 50% ethanol extract from rosemary (Rosmarinus officinalis) on α-glucosidase inhibitory activity and the elevation of plasma glucose level in rats, and its active compound. J Food Sci 71:S507–S512. doi:10.1111/j.1750-3841.2006.00125.x
Kwon YI, Vattem DA, Shetty K (2006) Evaluation of clonal herbs of Lamiaceae species for management of diabetes and hypertension. Asia Pac J Clin Nutr 15:107–118
Langin D (2006) Adipose tissue lipolysis as a metabolic pathway to define pharmacological strategies against obesity and the metabolic syndrome. Pharmacol Res 53:482–491. doi:10.1016/j.phrs.2006.03.009
Larsen TM, Toubro S, Astrup A (2003) PPARgamma agonists in the treatment of type II diabetes: is increased fatness commensurate with long-term efficacy? Int J Obes Relat Metab Disord 27:147–161. doi:10.1038/sj.ijo.802223
Lee JJ et al (2007) Antiplatelet activity of carnosic acid, a phenolic diterpene from Rosmarinus officinalis. Planta Med 73:121–127. doi:10.1055/s-2006-957066
Lipina C, Hundal HS (2014) Carnosic acid stimulates glucose uptake in skeletal muscle cells via a PME-1/PP2A/PKB signalling axis. Cell Signal 26:2343–2349. doi:10.1016/j.cellsig.2014.07.022
Lo AH, Liang YC, Lin-Shiau SY, Ho CT, Lin JK (2002) Carnosol, an antioxidant in rosemary, suppresses inducible nitric oxide synthase through down-regulating nuclear factor-kappaB in mouse macrophages. Carcinogenesis 23:983–91. doi:10.1093/carcin/23.6.983
Lumeng CN, Saltiel AR (2011) Inflammatory links between obesity and metabolic disease. J Clin Invest 121:2111–2117. doi:10.1172/JCI57132
Martynyuk L, Martynyuk L, Ruzhitska O, Martynyuk O (2014) Effect of the herbal combination Canephron N on diabetic nephropathy in patients with diabetes mellitus: results of a comparative cohort study. J Altern Complement Med 20:472–478. doi:10.1089/acm.2013.0400
McCue PP, Shetty K (2004) Inhibitory effects of rosmarinic acid extracts on porcine pancreatic amylase in vitro. Asia Pac J Clin Nutr 13:101–106
Meeran SM, Ahmed A, Tollefsbol TO (2010) Epigenetic targets of bioactive dietary components for cancer prevention and therapy. Clin Epigenet 1:101–116. doi:10.1007/s13148-010-0011-5
Miranda PJ, DeFronzo RA, Califf RM, Guyton JR (2005) Metabolic syndrome: definition, pathophysiology, and mechanisms. Am Heart J 149:33–45. doi:10.1016/j.ahj.2004.07.013
Nagasaki H, Yoshimura T, Aoki N (2012) Real-time monitoring of inflammation status in 3T3-L1 adipocytes possessing a secretory Gaussia luciferase gene under the control of nuclear factor-kappa B response element. Biochem Biophys Res Commun 420:623–627. doi:10.1016/j.bbrc.2012.03.049
Naimi M, Tsakiridis T, Stamatatos TC, Alexandropoulos DI, Tsiani E (2015) Increased skeletal muscle glucose uptake by rosemary extract through AMPK activation. Appl Physiol Nutr Metab 40:407–413. doi:10.1139/apnm-2014-0430
Nazem F, Farhangi N, Neshat-Gharamaleki M (2015) Beneficial effects of endurance exercise with Rosmarinus officinalis labiatae leaves extract on blood antioxidant enzyme activities and lipid peroxidation in streptozotocin-induced diabetic rats. Can J Diabetes 39:229–234. doi:10.1016/j.jcjd.2014.11.003
Okamura N, Fujimoto Y, Kuwabara S, Yagi A (1994) High-performance liquid chromatographic determination of carnosic acid and carnosol in Rosmarinus officinalis and Salvia officinalis. J Chromatograph A 679:381–386. doi:10.1016/0021-9673(94)80582-2
Park MY, Mun ST (2014) Carnosic acid inhibits TLR4-MyD88 signaling pathway in LPS-stimulated 3T3-L1 adipocytes. Nutr Res Pract 8:516–520. doi:10.4162/nrp.2014.8.5.516
Park MY, Sung MK (2015a) Carnosic acid attenuates obesity-induced glucose intolerance and hepatic fat accumulation by modulating genes of lipid metabolism in C57BL/6J-ob/ob mice. J Sci Food Agric 95:828–835. doi:10.1002/jsfa.6973
Park MY, Sung MK (2015b) Carnosic acid inhibits lipid accumulation in 3T3-L1 adipocytes through attenuation of fatty acid desaturation. J Cancer Prev 20:41–49. doi:10.15430/jcp.2015.20.1.41
Pearson DA, Frankel EN, Aeschbach R, German JB (1997) Inhibition of endothelial cell-mediated oxidation of low-density lipoprotein by rosemary and plant phenolics. J Agric Food Chem 45:578–582
Perez-Fons L, Garzon MT, Micol V (2010) Relationship between the antioxidant capacity and effect of rosemary (Rosmarinus officinalis L.) polyphenols on membrane phospholipid order. J Agric Food Chem 58:161–171. doi:10.1021/jf9026487
Ramadan KS, Khalil OA, Danial EN, Alnahdi HS, Ayaz NO (2013) Hypoglycemic and hepatoprotective activity of Rosmarinus officinalis extract in diabetic rats. J Physiol Biochem 69:779–783. doi:10.1007/s13105-013-0253-8
Rangwala SM, Lazar MA (2004) Peroxisome proliferator-activated receptor γ in diabetes and metabolism. Trends Pharmacol Sci 25:331–336. doi:10.1016/j.tips.2004.03.012
Rau O, Wurglics M, Paulke A et al (2006) Carnosic acid and carnosol, phenolic diterpene compounds of the labiate herbs rosemary and sage, are activators of the human peroxisome proliferator-activated receptor gamma. Planta Med 72:881–887. doi:10.1055/s-2006-946680
Razavi BM, Hosseinzadeh H (2014) A review of the effects of Nigella sativa L. and its constituent, thymoquinone, in metabolic syndrome. J Endocrinol Invest 37:1031–1040. doi:10.1007/s40618-014-0150-1
Rocha J, Eduardo-Figueira M, Barateiro A et al (2015) Anti-inflammatory effect of rosmarinic acid and an extract of Rosmarinus officinalis in rat models of local and systemic inflammation. Basic Clin Pharmacol Toxicol 116:398–413. doi:10.1111/bcpt.12335
Romo-Vaquero M, Larrosa M, Yanez-Gascon MJ et al (2014a) A rosemary extract enriched in carnosic acid improves circulating adipocytokines and modulates key metabolic sensors in lean Zucker rats: critical and contrasting differences in the obese genotype. Mol Nutr Food Res 58:942–953. doi:10.1002/mnfr.201300524
Romo-Vaquero M, Selma MV, Larrosa M et al (2014b) A rosemary extract rich in carnosic acid selectively modulates caecum microbiota and inhibits β-glucosidase activity. Altering fiber and short chain fatty acids fecal excretion in lean and obese female rats. PloS one 9:e94687. doi:10.1371/journal.pone.0094687
Romo Vaquero M, Yanez-Gascon MJ, Garcia Villalba R et al (2012) Inhibition of gastric lipase as a mechanism for body weight and plasma lipids reduction in Zucker rats fed a rosemary extract rich in carnosic acid. PLoS One 7:e39773. doi:10.1371/journal.pone.0039773
Sahebkar A (2013) Why it is necessary to translate curcumin into clinical practice for the prevention and treatment of metabolic syndrome? Biofactors 39:197–208. doi:10.1002/biof.1062
Sasaki K, El Omri A, Kondo S, Han J, Isoda H (2013) Rosmarinus officinalis polyphenols produce anti-depressant like effect through monoaminergic and cholinergic functions modulation. Behav Brain Res 238:86–94. doi:10.1016/j.bbr.2012.10.010
Scazzocchio B, Vari R, Filesi C et al (2011) Cyanidin-3-O-beta-glucoside and protocatechuic acid exert insulin-like effects by upregulating PPARgamma activity in human omental adipocytes. Diabetes 60:2234–2244. doi:10.2337/db10-1461
Sedighi R, Zhao Y, Yerke A, Sang S (2015) Preventive and protective properties of rosemary (Rosmarinus officinalis L.) in obesity and diabetes mellitus of metabolic disorders: a brief review. Curr Opin Food Sci 2:58–70. doi:10.1016/j.cofs.2015.02.002
Silva A, Andrade-Wartha E, Carvalho E, Lima A, Novoa AV, Mancini-Filho J (2011) Effect of aqueous rosemary extract (Rosmarinus officinalis L.) on the oxidative stress of diabetic rats. Revista de Nutrição 24:121–130. doi:10.1590/S1415-52732011000100012
Sinkovic A, Suran D, Lokar L, Fliser E, Skerget M, Novak Z, Knez Z (2011) Rosemary extracts improve flow-mediated dilatation of the brachial artery and plasma PAI-1 activity in healthy young volunteers. Phytother Res 25:402–407. doi:10.1002/ptr.3276
Stefanon B, Pomari E, Colitti M (2015) Effects of Rosmarinus officinalis extract on human primary omental preadipocytes and adipocytes. Exp Biol Med 240:884–95. doi:10.1177/1535370214562341
Tai J, Cheung S, Wu M, Hasman D (2012) Antiproliferation effect of Rosemary (Rosmarinus officinalis) on human ovarian cancer cells in vitro. Phytomedicine 19:436–443. doi:10.1016/j.phymed.2011.12.012
Takahashi T, Tabuchi T, Tamaki Y, Kosaka K, Takikawa Y, Satoh T (2009) Carnosic acid and carnosol inhibit adipocyte differentiation in mouse 3T3-L1 cells through induction of phase2 enzymes and activation of glutathione metabolism Biochemical and biophysical. Res Commun 382:549–554. doi:10.1016/j.bbrc.2009.03.059
Tsai CW, Liu KL, Lin YR, Kuo WC (2014) The mechanisms of carnosic acid attenuates tumor necrosis factor-alpha-mediated inflammation and insulin resistance in 3T3-L1 adipocytes. Mol Nutr Food Res 58:654–664. doi:10.1002/mnfr.201300356
Tu Z, Moss-Pierce T, Ford P, Jiang TA (2013) Rosemary (Rosmarinus officinalis L.) extract regulates glucose and lipid metabolism by activating AMPK and PPAR pathways in HepG2 cells. J Agric Food Chem 61:2803–2810. doi:10.1021/jf400298c
Ullevig SL, Zhao Q, Zamora D, Asmis R (2011) Ursolic acid protects diabetic mice against monocyte dysfunction and accelerated atherosclerosis. Atherosclerosis 219:409–416. doi:10.1016/j.atherosclerosis.2011.06.013
Umasankar K, Nambikkairaj B, Manley Backyavathy D (2012) Effect of topical treatment of Rosmarinus officinalis essential oil on wound healing in streptozotocin induced diabetic rats. Nat Environ Pollut Technol 11:607–611
Vijayakumar M, Govindarajan R, Rao GM et al (2006) Action of Hygrophila auriculata against streptozotocin-induced oxidative stress. J Ethnopharmacol 104:356–361. doi:10.1016/j.jep.2005.09.030
Voshol PJ, Haemmerle G, Ouwens DM et al (2003) Increased hepatic insulin sensitivity together with decreased hepatic triglyceride stores in hormone-sensitive lipase-deficient mice. Endocrinology 144:3456–3462. doi:10.1210/en.2002-0036
Wang T, Takikawa Y, Satoh T et al (2011) Carnosic acid prevents obesity and hepatic steatosis in ob/ob mice. Hepatol Res 41:87–92. doi:10.1111/j.1872-034X.2010.00747.x
Wang T, Takikawa Y, Tabuchi T, Satoh T, Kosaka K, Suzuki K (2012a) Carnosic acid (CA) prevents lipid accumulation in hepatocytes through the EGFR/MAPK pathway. J Gastroenterol 47:805–813. doi:10.1007/s00535-012-0546-7
Wang W, Li N, Luo M, Zu Y, Efferth T (2012b) Antibacterial activity and anticancer activity of Rosmarinus officinalis L. essential oil compared to that of its main components. Molecules 17:2704–2713. doi:10.3390/molecules17032704
Wu YN, Huang J, Zuo AL, Yao L (2011) Research on the effects of rosemary (Rosmarinus officinalis L.) on the blood lipids and anti-lipid peroxidation in rats. J Essential Oil Res 23:26–34. doi:10.1080/10412905.2011.9700465
Xie L, Ortega MT, Mora S, Chapes SK (2010) Interactive changes between macrophages and adipocytes. Clin Vaccine Immunol 17:651–659. doi:10.1128/CVI.00494-09
Yam D, Friedman J, Bott-Kanner G, Genin I, Shinitzky M, Klainman E (2002) Omega-3 fatty acids reduce hyperlipidaemia, hyperinsulinaemia and hypertension in cardiovascular patients. J Clin Basic Cardiol 5:229–231
Yu YM, Lin HC, Chang WC (2008) Carnosic acid prevents the migration of human aortic smooth muscle cells by inhibiting the activation and expression of matrix metalloproteinase-9. Br J Nutr 100:731–738. doi:10.1017/s0007114508923710
Yun YS, Noda S, Shigemori G et al (2013) Phenolic diterpenes from rosemary suppress cAMP responsiveness of gluconeogenic gene promoters. Phytother Res 27:906–910. doi:10.1002/ptr.4794
Zeng HH, Tu PF, Zhou K, Wang H, Wang BH, Lu JF (2001) Antioxidant properties of phenolic diterpenes from Rosmarinus officinalis. Acta Pharmacol Sin 22:1094–1098
Zhao Y, Sedighi R, Wang P, Chen H, Zhu Y, Sang S (2015) Carnosic acid as a major bioactive component in rosemary extract ameliorates high-fat-diet-induced obesity and metabolic syndrome in mice. J Agric Food Chem 63:4843–4852. doi:10.1021/acs.jafc.5b01246
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hassani, F.V., Shirani, K. & Hosseinzadeh, H. Rosemary (Rosmarinus officinalis) as a potential therapeutic plant in metabolic syndrome: a review. Naunyn-Schmiedeberg's Arch Pharmacol 389, 931–949 (2016). https://doi.org/10.1007/s00210-016-1256-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00210-016-1256-0