
Abstract
Per- and polyfluoroalkyl substances (PFAS) have been widely used and represent a class of environmental persistent chemicals. An association of a reduction of vaccination efficacy with PFAS serum levels in humans was used by the European Food Safety Authority as a key effect for PFAS risk assessment. The data support for using this association is reviewed by a critical analysis of the respective human epidemiology and the available animal studies on the immunomodulation of PFAS. Based on an analysis of the available human epidemiology, the overall level of evidence regarding associations between PFAS serum levels and reduced antibody response remains weak. Absence of an association between an increase in clinical infections and PFAS serum levels and the limited understanding of the importance of antibody levels as an isolated data point further support this conclusion. Animal toxicity studies with PFAS focusing on immunomodulation also provide only limited support for immunomodulation as an important endpoint in PFAS toxicity. While immunomodulation is observed after PFAS administration, generally at blood concentrations several orders of magnitude above those seen in environmentally exposed humans, the relevance of these observation is hampered by the high doses required to influence immune endpoints, the limited number of endpoints assessed, and inconsistent results. The limitations of the current database on associations of human PFAS exposures outlined here indicate that more evidence is required to select immunomodulation as a critical endpoint for human PFAS risk assessment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In per- and polyfluoroalkyl substances (PFAS), multiple hydrogen atoms in an aliphatic carbon chain are replaced by fluorine and a hydrophilic functional group is present at the end of the carbon chain, typical chain lengths range from four to 16. Perfluorinated acids such as perfluorooctanoic acid (PFOA) and perfluorinated alkylsulfonates such as perfluorooctane sulfonic acid (PFOS) are the major PFAS of concern, but a large number of other PFAS with different functional groups have been developed for commercial applications or are formed by degradation of other PFAS in the environment.
PFAS have varying physicochemical properties depending on the number of carbon atoms and the presence of functional groups (Buck et al. 2011; OECD 2018). Due to the stability of the carbon–fluorine bond to chemical degradation, many PFAS are stable in the environment and may accumulate in the food chain to result in ubiquitous human exposure.
For the majority of the many PFAS with past and present uses, few or no data on chemical properties and potential health effects are available (Cousins et al. 2020). The available data include associations of PFAS concentrations in blood with birth weight, reduced vaccination responses, increases in blood cholesterol, and changes in enzymes indicative of liver dysfunction in humans (overview in EFSA-CONTAM Panel et al. 2020). In experimental animals, the toxicological database is also limited even for well-studied PFAS such PFOA and PFOS as many endpoints considered relevant for a human health risk assessment have not been addressed by adequate toxicity testing (ATSDR 2021; EFSA-CONTAM Panel et al. 2020). Hepatotoxicity may represent the most sensitive toxicity endpoint in rodents for both PFOS and PFOA (ATSDR 2021; EFSA-CONTAM Panel et al. 2020; Fragki et al. 2021). Limited developmental toxicity studies with PFAS in rodents showed high offspring mortality early after birth, reduced fetal weight, litter sizes and post-natal growth, increased liver weight, and indications for immunomodulation at doses at or below those inducing maternal toxicity (ATSDR 2021; EFSA-CONTAM Panel et al. 2020). Liver effects of PFAS may be due to an interaction with the peroxisome proliferator-activate receptor α (PPARα) but modes of action for the many other effects of PFAS have not been defined (EFSA-CONTAM Panel et al. 2020).
Major species differences in toxicokinetics complicate the human health risk assessment of PFAS (Pizzurro et al. 2019). For PFOS and PFOA, rapid absorption from the gastrointestinal (GI) tract is evident in rodents and, likely, in humans. In rodents, absorbed PFOS and PFOA mainly distribute to the liver and serum. PFAS also reach the fetus by placental transfer and PFAS are distributed into maternal milk resulting in human exposure by lactation. Neither PFOS nor PFOA is subjected to biotransformation and is excreted as parent compound in both urine and feces. Kinetics of elimination show significant sex differences in rats and elimination half-lives range from several weeks in rodents to up to 10 years in humans (Pizzurro et al. 2019). Due to these differences in elimination kinetics, blood concentrations at the points of departure are considered as much more relevant than doses applied for human risk characterization.
The presence of PFAS in environmental media and in human blood has resulted in a number of health risk assessments by regulatory agencies and advisory groups using different endpoints as points of departure and different approaches to risk characterization. Several of the assessments relied on the limited animal toxicity information for PFOA and PFOS. Others used associations of a reduced antibody response in children with PFAS exposures were also applied as endpoints to derive a tolerable exposures to PFAS, but such associations may not be suitable for human risk characterization due to inconsistencies in the database (ATSDR 2021; Health-Canada 2018; UBA-HBM-Kommission 2020; US-EPA 2016a, 2016b).
In this review, the data support for the use of reduced antibody responses indicative of immunomodulatory effects (defined as change in the immune system caused by agents that activate or suppress its function) of PFAS in humans is assessed applying general weight of evidence criteria to both the animal database and the human epidemiological studies that investigated associations between human PFAS exposures and antibody response to vaccination and incidences of clinical infections. The evaluation used the database from the most recent EFSA evaluation to critically analyze support for EFSAs conclusions. Additional literature searches were performed to identify potential information published after the deadline of the search performed for the EFSA opinion (EFSA-CONTAM Panel et al. 2020). Details of these searches are reported in the epidemiology and animal toxicity sections.
Human studies reporting associations between PFAS and biomarkers of susceptibility to infections and with clinical infections
Methods
This study conforms to the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRSMA) guidelines” (Page et al. 2021). The existing studies related to PFAS and human health published from database inception through 1 November 2021 were identified via Medline/Pubmed using the following search string: "perfluoro* [tiab] OR pfas [tiab] OR perfluorinated*[tiab] AND human health” without language or other restrictions. Key search terms were required to appear in the article title or abstract. Title and abstract of the retrieved reports were independently screened by two reviewers as well as the full texts screening for eligibility. To be included in our analysis, studies had to have an epidemiological study design and must have performed a (logistic) regression analyses of gestational or childhood exposure to PFAS against either (1) antibody levels for pediatric vaccines or (2) the occurrence of child’s infectious diseases. Studies were excluded if they presented non-human data, asthma or allergies, non-vaccine-related antibodies, and were reviews or letters. Of the 2161 screened studies, 2115 were considered irrelevant based on title and abstract. Of the remaining 46 articles that were assessed in full text, 22 studies were excluded because they reported on outcomes not relevant to this study, were reviews/letters, or reported secondary data analyses. Two articles were retrospectively identified during the review process of this manuscript. Finally, 26 articles were identified as relevant and included in the review.
Vaccine response
The relationship between PFAS exposures and biomarkers of immunomodulation such as vaccine responses in humans has been investigated in 13 studies. These include six birth cohort studies conducted in Norway (Granum et al. 2013), the Faroe islands (Grandjean et al. 2012, 2017a, b; Shih et al. 2021), Germany (Abraham et al. 2020), and China (Zeng et al. 2019); one longitudinal analysis of adult residents in the US state of West Virginia with higher PFOA levels in drinking water (Looker et al. 2014); three cross-sectional studies based on data from the US National Health and Nutrition Examination Survey (NHANES) (Stein et al. 2016a, b), a study using adult volunteers from a hospital in Denmark (Kielsen et al. 2016), one study using cross-sectional data from the cohort Isomer of C8 Health Project in China (Zeng et al. 2020) and a prospective study based on a subset of data from a randomized controlled trial conducted in West Africa (Timmermann et al. 2020).
Seven studies (Abraham et al. 2020; Grandjean et al. 2012, 2017a, b; Granum et al. 2013; Kielsen et al. 2016; Shih et al. 2021) examined tetanus antibody concentrations. Diphtheria antibody concentrations were examined in five studies (Abraham et al. 2020; Grandjean et al. 2012, 2017a; Kielsen et al. 2016; Shih et al. 2021). Three studies examined measles antibody concentrations (Granum et al. 2013; Stein et al. 2016b; Timmermann et al. 2020) and one study (Stein et al. 2016a) investigated antibody concentrations of mumps. Rubella antibody concentrations were investigated in one study (Granum et al. 2013). Haemophilus influenza type b (Hib), A/H1N1 and A/H3N2 antibody concentrations were investigated by Looker et al. (2014). Antibody concentrations of FluMist were investigated by Stein et al. (2016a) and hepatitis B surface (HBsAB) antibody concentrations were investigated by Zeng et al. (2020) and Shih et al. (2021). Serum antibodies were investigated by Zeng et al. (2019). One study (Shih et al. 2021) investigated hepatitis type A serum antibody concentrations.
An overview of the design and observations of the human studies on PFAS exposure and antibody response is given in Table 1.
Prospective studies
The first prospective study of PFAS and immune-related health effects that evaluated vaccine responses in children exposed to PFAS in utero was published in 2012 (Grandjean et al. 2012). Further studies in this cohort followed. The study was conducted in the Faroe Islands, where high dietary intake of seafood may be associated with increased exposures to PFAS. The 1st analysis reported that maternal PFOS serum concentrations collected during the last trimester of pregnancy were negatively associated with anti-diphtheria antibody concentrations in 5-year-old children (n = 532). A more recent retrospective analysis (Grandjean et al. 2017b) extended on the existing Faroe Islands birth cohort (Grandjean et al. 2012) by analyzing serum samples (n = 349) for PFAS at the ages of 18 months and 5 years in children and in maternal serum during infancy. PFOS was the dominant PFAS with a mean concentration of 27.3 ng/mL in maternal and 16.7 ng/mL in serum collected from children when these were at age five. Again, inverse associations between serum PFAS concentrations and antibody concentrations were observed in most analyses. The strongest inverse associations were found for tetanus, most pronounced with pre-natal PFAS exposures. For all three sets of serum analyses, PFOA showed the strongest associations with lower tetanus antibody concentrations at age five. Cross-sectional comparisons in the joint analysis at age 5 also showed inverse associations for PFNA and PFDA, though with regards to diphtheria only.
Later, serum concentrations of PFAS and of antibodies against diphtheria and tetanus were measured in the same cohort when the children were at age 13 (n = 516) and results were compared with data from the previous examination at 7 years (Grandjean et al. 2017a). Serum concentrations of PFAS and antibodies generally declined with age from 7 to 13 years. However, 68 subjects had visited the emergency room and had likely received a vaccination booster, and a total of 202 children showed higher vaccine antibody concentrations at 13 years than at 7 years. Therefore, separate analyses were conducted after exclusion of these two subgroups. Diphtheria antibody concentrations decreased at elevated PFAS concentrations at age 7 and 13 years; the associations were statistically significant for perfluorodecanoic acid (PFDA) at age 7 and for PFOA at age 13, both suggesting a decrease by ∼25% for each doubling of exposure. Structural equation models showed that a doubling in PFAS exposure at age 7 was associated with losses in diphtheria antibody concentrations at 13 years of 10–30% for the four PFAS. Few associations were observed for anti-tetanus concentrations.
In the most recent study of the Faroese birth cohort (Shih et al. 2021), concentrations of PFAS were collected in samples of the umbilical cord blood and serum at ages 7, 14, 22 and 28 years. Median concentrations for PFOS, PFOA, PFHxS, PFNA and PFDA were 6.1, 1.1, 0.2 and 0.1 at birth; 32.9, 5.1, 0.9 and 0.2 at 7 years; 31.3, 5.0, 0.6, 0.7 and 0.3 at 14 years; 12.5, 3.0, 0.5, 0.9 and 0.4 at 22 years and 7.0, 1.3, 0.4, 1.0 and 0.3 at 28 years. Serum antibody concentrations against hepatitis type A and B, diphtheria and tetanus were analyzed at age 28 years. Inverse trends (although non-significant) were observed between PFOA at ages 14 and 28 years and hepatitis type A concentrations per doubling of exposure. Inverse trends were also observed between serum PFOA at ages 22 and 28 years and hepatitis type B antibody concentration per doubling of exposure. Some sex-specific associations observed with hepatitis A were also observed for cord blood PFAS and concentrations art 7 and 14 years. No inverse associations between PFAS exposures were observed for tetanus or diphtheria.
In a Norwegian Mother and Child Cohort Study, which is considered representative of the general population in Norway, Granum et al. (2013) observed that concentrations of PFOA, PFOS, perfluorohexanoic acid sulfonate (PFHxS), and perfluorononanoic acid (PFNA) in maternal blood (median concentrations were 1.1, 5.5, 0.3, and 0.3 ng/mL, respectively) collected at the time of delivery, were all inversely associated with the level of anti-rubella antibodies measured in the children at age three (n = 56). Maternal serum levels of PFOA and PFNA were positively associated with the number of episodes of common colds in the group of children, and PFOA and PFHxS were positively correlated with the number of episodes of gastroenteritis.
A prospective study (known as the “C8 Health Project”) of 403 adults who were exposed to PFOA and PFOS via water contaminated from a nearby PFAS manufacturing facility, was conducted in the Ohio/West Virginia area (Looker et al. 2014). Sera were tested for influenza-specific antibodies for A/H3N2, A/H1N1 and influenza B. Samples were analyzed for PFOA and PFOS concentrations (median concentrations of 31.5 and 9.2 ng/mL, respectively). Elevated PFOA serum levels were associated with reduced antibody titer rise, particularly to A/H3N2 influenza vaccine and an increased risk of not attaining the antibody threshold considered to offer long-term protection. No association between self-reported colds or influenza and PFOA or PFOS serum concentrations was reported.
More recently, the association between plasma concentrations of PFHxS, PFOS, PFOA and PFNA and antibodies to diphtheria, tetanus and haemophilus influenza type b (Hib) was examined in a comparably small cross-sectional study in a cohort of 101 infants from Germany (Abraham et al. 2020). This study was used by EFSA as key study to derive a PoD for human health risk assessment of PFAS. Mothers and their children were recruited in 1997–1999 when the infants were between 341 and 369 days old. Of these, 21 were formula-fed (≤2 weeks of breastfeeding) and 80 were breastfed for >4 months. When combining exclusive and partial breastfeeding into ‘equivalent to exclusive breastfeeding’, the median duration of breastfeeding was 7.4 months. Mean levels of PFASs in plasma from, respectively, non-breastfed and breastfed infants were 3.8 and 16.8 ng/mL for PFOA, 6.8 and 15.2 ng/mL for PFOS, 1.7 and 2.1 ng/mL for PFHxS, and 0.2 and 0.6 ng/mL for PFNA. For the mothers, the mean concentrations in plasma among those who did not breastfeed (n = 21) and those who breastfed (n = 80) were 4.9 and 3.2 ng/mL for PFOA, 17.2 and 14.1 ng/mL for PFOS, 1.8 and 1.0 ng/mL for PFHxS, and 0.4 and 0.3 ng/mL for PFNA. The results showed significant correlations between adjusted antibody levels and PFOA levels for Hib (r = −0.23) tetanus (r = −0.25) and diphtheria (r = −0.23). No significant correlations were observed for PFOS and of the vaccines. Moreover, effect sizes (means for PFOA quintiles Q1 vs. Q5) were estimated to be lower by 86% for Hib, 54% for tetanus and 53% for diphtheria.
The higher concentrations of PFAS in plasma among breastfed infants and lower concentrations of PFAS among mothers who breastfed were explained by lactational transfer of PFASs from the mother to the baby. This transfer into breast milk is more effective for PFOA compared to PFOS, which also explains the differences in PFOS/PFOA ratio between mothers and infants.
A prospective cohort study, which included a randomized controlled trial based on a subset of data from West Africa (Timmermann et al. 2020) included measurements of 237 children. PFAS were quantified in infant serum at the time of inclusion (mean age of 5.6 months) and measles antibody concentrations were measured at least once after receiving a measles vaccination. Low concentrations (compared to other reports) of PFHxS, PFOS, PFOA PFNA PFDA and PFUnDA (median concentrations of 0.10, 0.77, 0.68, 0.21, 0.19 and 0.12 ng/mL, respectively) were detected in all but one child. A doubling in PFOS and PFDA was associated with 21 and 25% lower measles concentrations at the 9-month visit.
Cross-sectional studies
In a large cross-sectional analysis of data (n = 1191) from 12- to 19-year-old children based on data from NHANES in the US, associations between mean concentrations of PFHxS, PFOS, PFOA and PFNA (mean concentrations of 1.1, 5.22, 2.28 and 0.77 ng/mL, respectively) and serum antibody concentrations to measles, mumps and rubella were investigated (Stein et al. 2016b). The study reported that decreases in mumps antibodies were associated with increases in serum concentrations of PFOA and PFOS and anti-rubella antibodies were associated with increases in serum concentrations of PFOA, PFOS, and PFHxS. PFOS and PFOA showed slightly weaker but significant inverse associations with antibody concentrations to mumps (~ 6–7% decrease per ng/mL increase). Non-significant, but inverse associations were observed for PFHxS and non-significant associations were observed for measles for all four compounds.
In a representative sample of individuals > 12 years from NHANES for years 1999–2000 and 2003–2004 (Pilkerton et al. 2018), associations between rubella titers, PFOA (mean concentrations of 4.8 ng/mL in youth, 4.3 ng/mL in women and 6 ng/mL in men) and PFOS (mean concentrations of 25.1 ng/mL in youth, 22.1 ng/mL in women and 28.1 ng/mL in men) were investigated in two samples, in youth (12–18 years) and in adult men and women. No significant associations with rubella titers for either PFOA or PFOS were reported for the youth. In adults, there was a significant association between both PFOA and PFOS quartiles and rubella titers, but when stratifying the analysis by sex, the associations remained significant for PFOA and anti-rubella titers in men only.
In a very small cross-sectional study of 12 adult volunteers selected from the general human population in Denmark, Kielsen et al. (2016) reported a negative association between serum concentrations of PFOS, PFNA, PFDA, perfluoroundecanoic acid (PFUnDA) and perfluorododecanoic acid (PFDoDA) (median concentrations of 9.52, 0.66, 0.30, 0.21 and 0.039 ng/mL, respectively), and anti-tetanus and diphtheria antibodies were reported.
Associations between several PFASs measured in cord blood and antibodies to hand, foot and mouth disease (CA16 and EV71) were examined in 201 Chinese mother–child pairs both in cord blood and at three months of age (Zeng et al. 2019). Except for PFHxS and PFDoDA, all PFASs quantified (including the sum) were inversely associated with antibodies to hand, foot, and mouth disease in cord blood (mean concentrations of 0.12 ng/mL for PFDA, of 3.96 ng/mL for PFHxS, of 0.16 ng/mL for PFNA, of 0.13 ng/mL for PFUnDA, of 1.22 ng/mL for PFOA and 3.17 ng/mL for PFOS). Similar inverse associations were observed at 3 months, but statistical significance was not reached for any compound. Cord blood concentrations of individual PFASs (including the sum) were, however, associated with increased odds of having serum antibodies below protective levels in both cord blood and in offspring serum drawn at 3 months. The only exception from this pattern was PFHxS.
Finally, in a cross-sectional study conducted with adults based on data from the Isomer C8 Health Project in China, associations between serum PFOS and PFOA and hepatitis B surface antibody (HBsAb) were examined (Zeng et al. 2020). Median PFOS concentrations were reported as 10.1 ng/mL for HBsAb seropositive and 14.1 ng/mL for seronegative HBsAb participants, respectively. PFOA concentrations were 5.10 ng/mL for HBsAb seropositive and 5.54 ng/mL for seronegative HBsAb participants respectively. Statistically significant inverse associations were observed between PFOS and HBsAb, but no associations were observed between PFOA exposure concentrations and HBsAb antibody response.
Summary of human studies reporting associations of blood/serum PFAS with vaccination responses
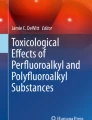
Figure 1 summarizes the number of studies in which the association of PFOA and PFOS and reduced antibody was found significantly (p < 0.05) negative, meaning a reduced antibody response per vaccine tested, significantly positive or no association was found. Results are presented only for PFOA and PFOS as these two compounds have the highest prevalence in the blood samples and their concentrations are most frequently assessed in the studies as compared to the other PFAS. That groups studies by the antigen/vaccine assessed and includes effect sizes and exposure measures (NTP 2016).

Frequency of studies with a reduced antibody response (red) and no association (green) of the antigen tested with PFOA and PFOS exposure in humans
No studies were found with a significant positive association. Most studies reported a negative association between PFOA exposure and antibody concentrations against diphtheria (n = 3) and tetanus (n = 3), predominantly in children. Two studies conducted with children also reported negative associations between PFOA and PFOS exposure and antibody concentrations against rubella and one retrospective study reported a negative association only between PFOA and antibody concentrations against Haemophilus influenza type b (Hib) in children, while a second cross-sectional study reported no significant association. A study conducted in youth and adults reported negative associations between rubella and adults only. Two studies in children reported no association between PFOA or PFOS and antibody concentrations against measles. Meanwhile, a study reported an inverse association between PFOS exposure and measles in children. In one study, both PFOA and PFOS exposures were negatively associated with antibody concentrations against mumps, and PFOS exposure was inversely associated with hepatitis B surface antibody (HBsAb) in a single study conducted with adults. In a study conducted with adults, PFOA was associated with lower A/H3N2 antibody titers. In a retrospective study of adults, PFOA and PFOS were negatively associated with hepatitis A, and PFOA only was negatively associated with PFOA.
None of the studies reported an association between either PFOA or PFOS exposure and antibody concentrations against A/H1N1, influenza type b, influenza and antibody seronegativity.
Associations between PFAS in serum/blood and susceptibility to infectious diseases
Ten prospective cohort studies (Abraham et al. 2020; Dalsager et al. 2016; Fei et al. 2010; Goudarzi et al. 2017; Granum et al. 2013; Impinen et al. 2019, 2018; Okada et al. 2012; Timmermann et al. 2020) and one cross-sectional study (Looker et al. 2014) in adult residents exposed to higher PFOA concentrations in drinking water (part of the C8 studies) evaluated the association between exposure to PFAS (usually PFOA and PFOS) and infectious diseases (see Table 2).
Across the studies, there is mixed evidence on the association between PFAS exposure and incidences of infectious diseases. Fei et al. (2010) found that children who were prenatally exposed to higher levels of PFOA had lower risks of hospitalization due to infections, but the incidence rate was statistically significant only for the second quartile of exposure compared to the first. No associations were observed for PFOS. However, in a stratified analysis, a slightly higher risk of hospitalization for infections among girls associated with higher maternal exposure PFOS or PFOA levels in the higher three quartiles compared with the lowest. Incidence rates were all below 1.0 among boys whose mothers were exposed to higher levels of PFOA or PFOS compared to the lowest. Granum et al. (2013) reported a significant positive association between the total number of reported episodes of common cold for both the children’s third years of life and all three years merged and maternal concentrations of PFOA. Concentrations of PFOA were positively associated with the number of episodes of gastroenteritis for all three years merged. Higher concentrations of PFOS and PFOA tended to increase the number of episodes of fever during the 1-year period study (Dalsager et al. 2016). No associations were reported for the other compounds. PFOS exposure in the high tertile compared to the low tertile was associated with an increased proportion of days with fever and increased odds of experiencing days with fever above the median. The latter tendency was also apparent for PFOA (Dalsager et al. 2016). Similarly, more days with fever among children with higher pre-natal exposure to PFOS and PFOA were reported in a recent study (Dalsager et al. 2021). In this study, the risk for any infection increased at elevated PFOS concentrations, whereas the specific risk of lower respiratory tract infections increased with higher concentration of both PFOS and PFOA.
Timmermann et al. (2020) examined the associations between PFAS and coughing, fever and diarrhea and found that the effects were generally more pronounced at the 9-month visit (mean age of child: 9.9 months), while the strongest results were seen for PFOA in relation to coughing. Positive trends between PFAS and diarrhea were also observed, generally in boys, but they did not reach statistical significance. Positive associations were reported between cord blood concentrations of PFOS and PFOA and the number of episodes of respiratory tract infection until 10 years of age (Impinen et al. 2018). Maternal PFOS levels (in the highest quartile) were associated with a greater risk of total infectious diseases in all children. No associations were observed for the other compounds. Positive associations were reported between cord blood concentrations of PFOS and PFOA and the number of episodes of respiratory tract infection until 10 years of age. Maternal PFOS levels (in the highest quartile) were associated with a greater risk of total infectious diseases in all children. No associations were observed for the other compounds. Among 7-year-old children, exposure to PFOS was inversely associated with rhino-conjunctivitis (RSV), while exposure to PFOA was associated with an increased risk of pneumonia (Ait Bamai et al. 2020).
Positive associations were reported between cord blood concentrations of PFOS and PFOA and the number of episodes of respiratory tract infection until 10 years of age (Impinen et al. 2018). Maternal PFOS levels (in the highest quartile) were associated with a greater risk of total infectious diseases in all children. No associations were observed for the other compounds.
In summary, there are relatively few human studies available that investigated the association between PFAS exposure and subsequent immunomodulation. While PFOA and PFOS have been investigated in relation to the antibody response against mainly diphtheria and tetanus in children, the results remain mixed and not conclusive for the association between PFAS and infectious diseases.
Data on immunomodulation by PFAS in experimental animals
The associations of PFAS blood/serum concentrations with reduced vaccination efficacy in the human studies indicates a potential for immunomodulation of PFAS in humans. As defined in the Bradford–Hill criteria, causality of reported associations in epidemiology studies can be supported by concordance with experimental results in animals. In the case of PFAS, a number of animal studies have addressed immunomodulation as an endpoint after PFAS administration and report blood concentrations where effects indicative of immunomodulation occur. While immunotoxicity has been observed after PFAS administration in animals in a number of studies with widely differing designs, assessing extent of support for causality of the associations reported in the human studies requires a detailed analysis of the animal data, the relevance of the endpoints assessed, and their strengths and weaknesses. Moreover, it needs to be assessed if effects of PFAS on the immune system in animals are sufficiently solid to serve as a point of departure (PoD) for human risk characterization.
Key studies on PFAS-induced immunomodulation in animals were identified from EFSA-CONTAM Panel et al. (2020) which covered studies through to August 2019. In addition, a literature search was performed in November 2021 to identify additional relevant peer-reviewed papers published after August 2019. PubMed/Toxline was identified as relevant database, and the following search terms were employed: (PFAS OR perfluoroalkyl* OR polyfluoroalkyl*) AND (immunotox* OR Immunosuppr* OR immunomodul* OR TDAR) AND ("in vivo" OR mice OR mouse OR animal OR rat OR rats). This literature search for publications published from August 01, 2019 to November 30, 2021, yielded 23 results. Based on a review of the titles and abstracts, 22 of these papers were excluded since they did not contain primary data, did not evaluate internal exposure (serum levels), and assessed endpoints or species not relevant for the present analysis. Only one publication assessed effects of poly-fluorinated aliphatics, but focused on compounds that were outside the scope of this review (short chain perfluoroethers; Woodlief et al. 2021).
General remarks on the available immunotoxicity studies with PFAS in experimental animals
While a large number of studies has been addressing immune effects of PFAS (EFSA-CONTAM Panel et al. 2020; NTP 2016), this review restricts the evaluation to animal studies on immunotoxicity-related findings by PFAS that report plasma or serum levels at the time of effects assessment (app. 50% of the studies available). Information on internal exposures to PFAS (i.e., plasma or serum concentrations) is required for an extrapolation of the effects seen in animals and their relevance to humans due to significant interspecies differences in toxicokinetics of PFAS (Pizzurro et al. 2019). Results of studies giving applied doses (in mg/kg/day) as only dose metric cannot be readily extrapolated to humans (Chou and Lin 2019, 2020) and thus do not permit a comparison of NOAELs/LOAELs with present human exposures (ATSDR 2021; Gomis et al. 2018). When internal exposures are considered, a comparison of NOAECs/LOAECs in animals with human blood levels is possible.
In addition, the endpoints selected in animals require consideration regarding relevance for conclusions on effects levels and applicability to humans. Across available human studies, effects indicate that immunosuppression by PFAS (i.e., the reduced ability of the immune system to respond to a challenge from a level considered normal, regardless of whether clinical disease is present) is of greatest concern (DeWitt et al. 2019). Immunosuppression can be assessed in experimental animals using different study designs and endpoints. The endpoints can be separated into screening (tier 1) studies i.e., using effects covered in standard animal toxicity testing (i.e., histopathology of immune organs) and results from functional immunotoxicity assays (like NK cell activity, lipopolysaccharide (LPS) response, IgM antibody PFC response), and more comprehensive (tier 2) studies usually assessing chemical-related effects on sensitivity to infections with model organisms. Observations of immunomodulation in tier 1 studies only indicate a concern for immunotoxicity and a need to perform tier 2 studies. Therefore, tier 1 studies should not be used to define points of departure for human risk characterization (ICH 2005; Luster et al. 1988, 1992; US-EPA 1996a, b). Among the many tier 1 studies, the T cell-dependent antibody response (TDAR) or plaque-forming cell (PFC) assay (Ladics 2018) is considered as “gold standard” (DeWitt et al. 2019) and the most sensitive functional assay for immunosuppression (FDA 2002; Luster et al. 1992). In this assay, rodents are exposed to the chemical of interest for a minimum of four weeks. Four to five days before the end of the experiment, a T cell-dependent antigen (typically sheep red blood cells, SRBC) is injected, resulting in IgM antibodies binding to epitopes on the surface of the sheep erythrocyte. After lysis of the erythrocyte by the classical complement pathway, hemoglobin diffuses into the agar matrix resulting in a clear area on the red lawn of sRBCs.
Overview of the available studies on immunomodulation by PFAS
Most of the studies on immunomodulation by PFAS studied PFOA and PFOS and used mice as model organism. The studies used endpoints like disease resistance, antibody response, NK cell activity, delayed-type hypersensitivity response, or monocyte phagocytosis. Additionally, some studies investigated effects of PFAS on secondary outcomes like lymphoid organ weights, lymphocyte counts or subpopulations, lymphocyte proliferation, cytokine levels, serum antibody levels, or histological alterations in immune organs. Overviews of the study design, effects and effective plasma levels are presented in Tables 3 (PFOS) and 4 (PFOA).
Qazi et al. (2009b) studied changes in the cellular compositions of the thymus and spleen in mice after a short-term exposure to PFOS or PFOA. Groups of male mice received diets containing different concentrations of PFOS or 0.02% PFOA. At the end of the 10-day treatment, blood was taken and thymus, spleen, liver and epididymal fat were isolated, weighed and submitted to histopathological evaluation. Serum levels of PFOS and PFOA, thymic and splenic cellularity and cell viability were determined, and immunophenotyping of thymocytes and splenocytes was performed. While mean daily intakes of PFAS were not presented, daily intake was calculated as 2, 10, 40, 100, 200, 500, or 1000 mg/kg PFOS or 40 mg/kg PFOA based on EFSA default values for food intake in mice (EC-EFSA 2012). Due to general toxicity, animals treated with ≥100 mg/kg/day had to be withdrawn. Serum levels achieved at 2, 10, and 40 mg/kg/day PFOS were 50, 100, or 340 µg/mL; serum level at 40 mg/kg/day PFOA was 150 µg/mL.
Mice treated with 40 mg/kg/day PFOS or PFOA had a decreased food consumption and subsequent reduced body weight gain. Liver weights were increased at >2 mg/kg/day PFOS and by PFOA. Thymus, spleen, and fat weights were negatively affected only at 40 mg/kg/day PFOS. Regarding cellularity and cell surface-phenotypes of thymocytes and splenocytes, only 40 mg/kg/day PFOS or 40 mg/kg/day PFOA led to a marked decrease in the total number of thymocytes and splenocytes. PFOA induced more pronounced effects as compared to PFOS. Moreover, all of the individual subpopulations of thymocytes and splenocytes examined were also significantly reduced in size. Histopathology showed that the thymic cortex of animals exposed to 40 mg/kg/day PFOS or the same dose of PFOA was smaller and virtually devoid of cells, and the cortical/medullary junction was not distinguishable. Regarding the spleen, with the exception of a moderate reduction in the size of the lymphoid nodules, atrophy was not associated with other structural changes.
In a second study (Qazi et al. 2009a), the same author assessed the effects of high-dose, short-term exposure of mice to PFOS or PFOA on the innate immune system. Groups of male mice received chow containing 0.001 or 0.02% PFOS or PFOA for 10 days. In a second experiment, groups of mice were treated as before and, thereafter, on day 10, each of the three groups was divided randomly into two subgroups, one of which was injected with saline containing 300 µg LPS to induce acute inflammation. Either directly following the exposure (in the first series of studies) or two hours after administration of LPS (in the second series), blood samples were obtained and liver, spleen, thymus, and epididymal fat were collected. Total and differential white blood cell counts (WBC) as well as levels of TNF-alpha and IL-6 were determined, and immunofluorescent staining and flow cytometric analysis of peritoneal, bone marrow and spleen macrophages were performed.
Since mean daily intakes for all dietary levels were not presented, daily intake was calculated to be 2 or 40 mg/kg PFOS or PFOA. Serum concentrations were 50 and 340 µg/mL for PFOS and 152 µg/mL for the high dose of PFOA (data for low-dose group not available). No effect was observed at low dose. Following 0.02% PFOS or PFOA administration, food consumption and body weight gain were reduced. Liver weight was increased while body weight, thymus, spleen and epididymal fat weights were reduced. Both compounds reduced the total numbers of WBC and lymphocytes, whereas the number of neutrophils was decreased only by PFOA. PFOS or PFOA elevated the proportion, but not the total number of macrophages (CD11b+) among the cells isolated from the peritoneal cavity. They also reduced both the proportion and total number of these cells in the bone marrow. Effects on the size of the splenic population of macrophages were not seen, despite the fact that the overall cellularity of the spleen was strikingly reduced. In vitro stimulation with LPS of cells isolated from the peritoneal cavity and bone marrow increased the production of both TNF alpha and IL-6 in animals treated with PFOS; a similar pattern was observed following treatment with PFOA. PFOA also significantly enhanced the ex vivo production of TNF-alpha and IL-6 by splenic cells in response to in vitro stimulation with LPS. When mice were challenged in vivo with an intravenous injection of LPS, pretreatment with PFOS or PFOA prior to the challenge with LPS further potentiated production of these cytokines by both peritoneal and bone marrow cells, while attenuating the ex vivo responses of splenocytes to LPS-induced inflammation. Circulating levels of TNF-α and IL-6, however, were increased only in animals treated with PFOA.
Peden-Adams et al. (2008) investigated the suppression of humoral immunity in mice following exposure to PFOS. Mice were administered 0.166, 1.66, 3.31, 16.6, 33.1, or 166 µg PFOS/kg bw for 28 consecutive days. At termination, blood samples were obtained and spleen, thymus, liver, kidney, uterus, and testis were collected. Lymphocyte proliferation, serum lysozyme and natural killer cell activity, T cell-dependent IgM production, as well as splenic and thymic CD4/CD8 subpopulations were determined. In a separate experiment conducted to assess T cell-independent antibody production, female mice were administered 334 µg/kg/day PFOS or vehicle for 21 days (10 mice/treatment group). Seven days prior to euthanization, these mice were injected with trinitrophenyl conjugated to LPS (TNP–LPS) and serum anti-trinitrophenyl IgM levels were measured.
Body weight gain, organ weights, and lymphocytic proliferation were not affected by PFOS. Overall, the effects on immune parameters differed in males and females despite similar blood concentrations of PFOS and dose–response was inconsistent. Lysozyme activity increased significantly in females, but not males, at 33 and 166 µg PFOS/kg/day; however, the response was not dose-related. NK cell activity was increased significantly in males at ≥16.6 µg PFOS/kg /day, but was not affected in females. Splenic CD4/CD8 subpopulations were only slightly affected by PFOS in females, but were significantly altered in males treated at ≥3.3 µg/kg/day. Male thymic T cell subpopulations were not affected with PFOS treatment and in females were increased only at the two highest dose groups.
T cell-dependent IgM production in response to sheep red blood cells (SRBC) was suppressed in both sexes, but males were more sensitive. Suppression of the plaque-forming cell (PFC) response was seen without dose–response in males from 1.66 µg/kg/day and with dose–response in females from 16.6 µg/kg/day. The authors calculated ED50 values for this effect of 0.69 µg/kg/day (0.05 µg PFOS/mL serum) in males and 21 µg/kg/day (0.78 µg PFOS/mL serum) in females. When studying the T cell-independent antibody production in response to TNP–LPS, serum levels of TNP-specific IgM were significantly suppressed (62% decrease) in animals treated with 334 µg/kg/day.
Qazi et al. (2010) attempted to confirm observations by Peden-Adams et al. (2008), but used dietary administration instead of gavage dosing and applied only one high-dose level of PFOS. Groups of five male mice received mean daily PFOS doses of 250 µg/kg/day. At the termination, blood samples, spleen and thymus were collected. T cell-dependent IgM production in response to SRBC was determined both in the plaque-forming assay and by measuring circulating IgM and IgG serum levels; T cell-independent IgM production was measured in response to TNP. Splenic and thymic phenotyping was performed. PFOS serum concentration at the end of dosing was 12 µg/mL. While food consumption was unaffected by PFOS, body weight gain was lower in exposed animals. Relative liver weight was increased while thymus and spleen weights were unchanged. Dietary exposure had no effect on the total numbers of circulating leukocytes or of cells in the thymus and spleen of males. Dietary exposure of mice to 250 µg/kg/day did not alter the relative numbers of the phenotypically distinct types of cells present in the thymus or spleen. Likewise, no effect of PFOS exposure on T cell-dependent or independent antibody response was observed in this study.
Zheng et al. (2009) studied the humoral immune response in mice orally exposed to PFOS. Groups of male mice were dosed by gavage with 5, 20, or 40 mg PFOS/kg/day for seven days. At termination of the study, spleen, thymus, liver, and kidneys were collected and weighed, and the spleen and thymus were processed into suspensions to look at NK cell activity, lymphocyte proliferation and the plaque-forming cell (PFC) response.
PFOS serum concentrations were 110, 280, and 340 µg/mL for the 5, 20, and 40 mg/kg/day dose groups, respectively. Food intake and body weight gain were significantly reduced at the two higher dose groups. Relative spleen and thymus weights were reduced at 20 and 40 mg/kg/day and relative liver weight was significantly increased at all dose levels. Splenic and thymic cellularity were significantly decreased at 20 and 40 mg/kg/day. To determine population changes in functional cell types of spleen and thymic lymphocytes, CD4/CD8 marker analysis was performed. Significant decreases in CD4+ and CD8+ cells were observed in both the spleen and thymus in the mice administered ≥20 mg/kg/day PFOS. Likewise, splenic NK cell activity was reduced in the two top dose groups. The SRBC-specific IgM plaque-forming cell response was reduced in a dose-related manner from the lowest tested dose of 5 mg/kg/day.
To observe chronic effects of immunotoxicity, groups of male mice were administered five different dose levels of PFOS daily by gavage for 60 days (Dong et al. 2009). Parameters similar to those described above (Zheng et al. 2009) were measured. Food intake and body weight gain were significantly reduced at ≥0.417 mg/kg/day and relative spleen and thymus weights were reduced; relative liver weight was significantly increased at ≥0.083 mg/kg/day. Splenic and thymic cellularity were significantly decreased from 0.417 mg/kg/day. To determine population changes in functional cell types of spleen and thymic lymphocytes, CD4/CD8 marker analysis was performed. Significant decreases in CD4+ and CD8+ cells were observed in both the spleen and thymus in the mice administered 0.417 mg/kg/day PFOS or greater. Splenic NK cell activity was reduced in the two top dose groups. The SRBC-specific IgM plaque-forming cell response was reduced in a dose-related manner from 0.083 mg/kg/day.
Only one study on immunosuppression of PFOS in rats is available (Lefebvre et al. 2008). Rats received diets delivering mean daily intakes of 0.15, 1.4, 3.5, or 7 mg PFOS/kg for 28 days. Plasma levels of PFOS were 0.95 and 1.5 µg/mL in males and females at 0.15 mg PFOS/kg, 13.5 and 15 µg/mL at 1.4 mg PFOS/kg, 20 and 32 µg/mL at 3.5 mg PFOS/kg, and 30 and 43 µg/mL at 7 mg PFOS/kg. At the end of the exposure period, blood samples were obtained, and spleen, thymus, mesenteric lymph nodes, and small and large intestines were collected, weighed, and submitted to histopathological evaluation. Serum immunoglobulins were determined, and lymphocyte phenotyping and splenocyte proliferation analysis were performed. T cell-dependent antibody response was assessed after immunization with keyhole limpet hemocyanin (KLH). Body weight gain was lower in the two top dose groups; relative liver weight was increased from 1.4 mg/kg/day. Relative spleen and thymus weights were unaffected. Histopathology revealed increased apoptosis of thymic lymphocytes in the thymic cortex and medulla of male rats treated with 3.5 or 7 mg/kg/day and in the cortex of female high-dose rats. No significant differences in lymphocyte subsets were observed; likewise, there was no effect on splenocyte proliferation. Regarding circulating immunoglobulin levels, in males, serum IgG1 was significantly reduced in the two lower dose groups and reverted to baseline at higher doses, while trend analyses indicated that there was a significant elevation in serum total IgG, IgG2a, and IgG2c levels with increasing PFOS dose; IgM was not affected. In females, there was a significant increase in serum total IgM and IgG2c with increasing PFOS exposure. After challenge with the T-dependent antigen KLH, in male rats there was a significant trend toward elevated KLH-specific IgG levels with increasing PFOS dose, while there were no significant changes in KLH-specific IgG titers in PFOS-treated female rats. Overall, the significant reduction of IgG1 observed in males at the lowest tested dose was considered of questionable relevance by the authors as (1) no similar effect was observed in female animals, (2) the effect was not evident at higher doses, and (3) was not associated with functional changes in response to challenge with KLH antigen.
Effects of PFAS administration on immune responses in animal infection models
Only two studies in animal infection models report plasma levels of PFAS, both applied PFOS. Guruge et al. (2009) studied host resistance to infections with influenza A virus (H1N1) in female mice exposed by gavage to 5 or 25 µg/kg/day PFOS for 21 days. At the end of the exposure, three animals per dose group were sacrificed to collect plasma for PFOS analysis; liver, kidney, lung, thymus and spleen were collected and weighed. The remaining animals were exposed intranasally to influenza A virus and observed for 20 days past inoculation using mortality as endpoint. PFOS levels in spleen, thymus, and lung also showed a dose-dependent increase. Body and organ weights were not affected. While there was no significant difference in mean survival time, there was a significant trend for a dose-related decrease in survival rate of mice on day 20 after virus infection, the eventual survival rate, however, was significantly lower than in controls only in high-dose mice.
Dewitt et al. (2008) studied the effects of PFOA in drinking water on humoral and cellular immunity using standard assays for assessing immune function. Groups of female mice received PFOA at daily doses of 0.94, 1.88, 3.75, 7.5, 15, or 30 mg/kg for 15 consecutive days. Plasma levels at the lowest dose were not reported, plasma levels at the other doses in ascending order were 35, 75, 87, 128 and 163 µg PFOA/mL. Mice were immunized with sheep red blood cells or sensitized to bovine serum albumin in Freund’s complete adjuvant (CFA) on day 10 of exposure; immune responses and PFOA serum levels were determined 1 day post exposure. A subgroup of animals were given a booster immunization of SRBCs two weeks after primary immunization, these were sacrificed 5 days later. Circulating IgG and IgM levels were determined in animals immunized with SRBC; footpad thickness was determined in animals immunized with CFA as a measure of delayed-type hypersensitivity response. Lymphoid organ weights were measured in animals sacrificed for IgM (1 day after exposure ended) and IgG (15 days after exposure ended) antibody determinations. Body weight gain was reduced in the two top doses. Relative liver weight was increased in animals of all dose groups, while relative spleen and thymus weights were reduced at >3.75 mg/kg/day. SRBC-specific IgM antibody titers (measured on day 1 after end of exposure) were reduced as compared to controls at doses of ≥3.75 mg/kg/day in a dose-related manner; no suppression of SRBC-specific IgG antibody titers (measured on day 15 after end of exposure) was observed.
Discussion
Human studies reporting associations of PFAS in blood/serum with immune parameters
In the studies evaluated, a decrease in antibody response was associated with PFOA and PFOS exposure for some of the vaccines examined, which is intriguing. The methodology used by most studies to measure antibody response seems to be reliable and valid. While the observed differences across vaccines with regards to the antibody level and length of time that an effective antibody response is maintained are expected, most evidence is based on studies with children. Effects within these studies vary with regards to the timing of the exposure. Therefore, we cannot be certain about the “best” age or time to study this association.
While Granum et al. (2013) and Grandjean et al. (2012) report that maternal concentrations of PFOA and PFOS are associated with decreased antibody levels in children; these studies cannot exclude the potential impact of post-natal exposure. There is no a priori reason or a biological hypothesis to suggest a specific window of susceptibility for PFOA and PFOS exposure to affect the antibody response (i.e., developmental, childhood, or adult). The only study that tested both developmental and childhood exposures (Grandjean et al. 2012) reported that both exposure windows were associated with lower antibody levels to diphtheria vaccinations and the most consistent results were for the association with childhood exposure measures.
Only two (both conducted with the Faroese birth cohorts) of the thirteen studies showed associations with antibody titers falling below protective levels (Grandjean et al. 2012, 2017b). It is therefore difficult to assess the clinical relevance of reduced antibody responses in the other studies, as it is unknown whether small to moderate reductions in antibody levels influence an immune response. It is known that the antibody response to rubella and mumps are typically robust and last for decades, whereas diphtheria and tetanus require booster vaccinations to maintain higher antibody levels that provide effective immunity. In the studies above, the antibody response to diphtheria showed the most consistent response and was suppressed in relation to maternal, childhood and adult PFOA and PFOS concentrations (Abraham et al. 2020; Grandjean et al. 2012, 2017b; Kielsen et al. 2016). Higher PFOA and PFOS concentrations were also associated with lower antibody response for tetanus; but the antibody response was only associated with maternal PFOA and PFOS in one study (Grandjean et al. 2017b). The antibody response to measles was not associated with PFOA or PFOS in two (Granum et al. 2013; Stein et al. 2016b) of the three (Timmermann et al. 2020) studies in which it was measured while the antibody response to mumps was only significant in one study (Stein et al. 2016b). It is possible that heterogeneity in the association between PFOA and PFOS exposure and reduced antibody levels for different vaccines is a result of differences in the strength of the response (i.e., higher antibody levels/clinical relevance) or the rates at which antibody titers change over time (NTP 2016).
The effects of PFAS fetal, infant and childhood exposures on the development of childhood response to vaccines, infectious diseases, allergic reactions, atopic dermatitis, asthma, and lung function were recently reviewed by von Holst et al. (2021). Compared to that review, we decided to only focus our review on studies examining the association between PFAS exposure and immunosuppression and infectious diseases in children but also in adults. Our aim was to provide more targeted evidence and inform regulatory agencies in their decision whether immunomodulation is a critical endpoint for human PFAS assessment. Thus, we combined the existing evidence from studies on animal toxicity and human toxicity, an important compilation of the evidence missing from von Holst.
With regard to the results, the von Holst review authors concluded that there was a strong indication of immunosuppression, demonstrated as diminished childhood antibody response to vaccination, particularly with the three PFOA, PFOS and PFHxS exposures. Some indication of increased risks of childhood infectious diseases/infections particularly from PFOS exposure was suggested by the authors, while limited indication of an effect of PFAS exposure on allergic reactions, atopic dermatitis, asthma, and lung function was suggested.
In our review, however, we suggested that there is not consistent evidence to support a strong association between PFAS and diminished response to vaccination. Nonetheless, we suggest that there is some consistency in the findings of the association between PFOA exposure and specifically tetanus and diphtheria predominantly in children, but not in adults.
With regard to infectious diseases, aligned with von Holst, we support the mixed evidence on the association between PFAS exposure and infectious diseases.
In summary, although some epidemiological studies suggest an inverse association between antibody response and PFAS exposure, the evidence remains weak due to a small number of studies, especially per vaccine type or per PFAS exposure; relatively high heterogeneity of study methodologies; and small effect sizes. In addition, results on reduction of antibody levels are not consistent with an increase in infectious diseases as consequence of PFAS exposures.
Therefore, the epidemiological human evidence is at best “suggestive” of an association but is considered too weak to draw a solid conclusion.
The extrapolation of the epidemiological data is further hampered by the fact that many of the associations were seen with high PFAS exposures in cohorts examined between 1997 and 2009 with PFAS exposures which are not observed anymore in contemporary populations. Although the releases of these compounds and especially PFOS, PFHxS and PFOA have been considerably reduced since 2000, it should be noted that in certain populations average increases of PFAS concentrations have been observed (Lin et al. 2021). Moreover, residual confounding that may occur in the relationship between PFAS and health outcomes due to co-exposure to other compounds, such as methylmercury and polychlorinated biphenyls (PCBs), cannot be safely ruled out. Furthermore, it has been shown that mainly Arctic populations, included in PFAS studies, due to their diet and lifestyle are more likely to have elevated levels of methylmercury and PCBs concentrations (Bjerregaard et al. 2001; Johansen et al. 2000). Irrespective of the outcome on the relationship between PFAS and health effects, even when these confounding exposures are controlled in a statistical analysis, we cannot eliminate the a priori correlation between PFAS and PCBs or other human toxicant exposures and their combined effect on the outcome.
This field needs large-scale, prospective studies with real-world exposure data on PFAS, methylmercury and PCBs and antibody responses on a variety of vaccinations. Moreover, studies on effects of various human toxicant exposures on vaccine responses and effectiveness have been proposed as a means to demonstrate that tests on immunotoxicity performed mainly with animals showing immune suppression can predict human responses (Hessel et al. 2015; Luster et al. 2005; Selgrade 2007). However, whether these immunotoxic agents, and especially PFAS in this case, work in a transient fashion to suppress the developing immune system, or, alter developmental events that can have profound permanent effects remains to be confirmed in humans. These effects should become clearer with well-designed human epidemiologic studies including tests of immunophenotyping and serum immunoglobulin levels at various time points. Such tests have been already validated in humans, although difficult to implement in experimental settings (Luster et al. 2005).
Furthermore, studies investigating the association between PFAS exposure and vaccine response in regions, which have received less attention by researchers, such as Veneto (Italy) and Ronneby (Sweden), where high levels of water contamination and their associations with, among other diseases, high mortality rates and thyroid hormone levels respectively, have been observed (Panieri et al. 2022) are warranted.
Animal studies on immunotoxicity of PFAS
While all reviewed studies report effects on immune parameters of PFAS in animals under the conditions of the experiment, their reliability is limited due to design deviations from guidance documents on immunotoxicity testing and widely varying effect levels in the same species and in different species despite close similarities of study designs, PFAS serum levels, and endpoints assessed (FDA 2002; Ladics 2018; US-EPA 1996a).
Regarding issues with study design, many studies included less than the recommended minimum number of 10 animals per dose group and none of the studies included a positive control to assess the sensitivity of methods applied. In addition, host resistance assays, which allow the assessment of effects on the innate immune system, should focus on non-lethal resistance models like those quantifying viral titers or bacterial counts in target tissues, as those models provide greater sensitivity than mortality as they are deemed to be a better reflection of protective immunity in the organism (WHO/IPCS 2012).
Regarding effect levels, a comparison of no-observed-adverse-effect-levels/serum concentrations and lowest-observed-adverse-effect-levels/serum concentrations of the most conclusive assays to characterize immunotoxicity of PFAS in animals in Table 5 summarizes the significant differences in PFAS plasma/serum levels required to induce effects in studies (Dong et al. 2009; Lefebvre et al. 2008; Peden-Adams et al. 2008; Qazi et al. 2010) that used a minimum exposure of 28 days and of the only one host resistance assay available. In general, the serum/plasma concentrations of PFAS in animals at the NOAELs varied widely. While the wide range of NOAECs/LOAECs may be due to differences in routes of exposure, species, strain and sex, inconsistencies in results (ATSDR 2021; Health-Canada 2018; US-EPA 2016a, 2016b) remain even when closely corresponding study designs were applied (Peden-Adams et al. 2008; Qazi et al. 2010). The lowest effect levels in the reviewed studies with PFAS were reported in male mice for IgM response (Peden-Adams et al. 2008). However, the IgM response only showed dose–response in female mice and no explanation for the absence of dose–response in males was provided; a difference in PFOS serum levels can be discarded as a contributing factor to this inconsistency. In contrast, effects of PFOS were not seen at the effect levels of (Peden-Adams et al. 2008) in study using a longer exposure period (Dong et al. 2009). However, that study observed dose–response for PFAS-induced effects in both male and female mice, but at higher doses. In addition, an attempt to replicate the results (Qazi et al. 2010) of Peden-Adams et al. (2008) using dietary administration did not observe effects on IgM production at even higher serum levels. The serum levels (Qazi et al. 2010) were also higher than the serum levels in Dong et al. (2009) for the lowest effect level for suppression of IgM production suggesting that the low-dose effects observed in males (Peden-Adams et al. 2008) are questionable. These inconsistencies were pointed out in several PFAS assessments (ATSDR 2021; Health-Canada 2018; US-EPA 2016a, b) and a review concluded that the very low NOAEL/NOAEC in (Peden-Adams et al. 2008) “may be an outlier of the PFC response dataset in terms of its dose–response” (Pachkowski et al. 2019).
While host resistance models are more conclusive as compared to the tier 1 studies described above (WHO/IPCS 2012), the only host resistance to the influenza A virus with PFAS (Guruge et al. 2009) included only two dose groups and mortality as the only endpoint used. The observations therefore do not permit conclusions since “the biological relevance of death as an endpoint is questionable when most or all of the immunocompetent controls do not survive, because the virulence or number of the challenge agents simply overwhelms the initial response to infection, killing the host before a protective response can be mounted” (WHO/IPCS 2012).
Other issues that induce difficulties in an assessment of the human relevance of the results of the animal studies are widely differing blood levels regarding effects on immune parameters in animals and human blood levels of PFAS that were seen in populations with a possible immunomodulation by PFAS as most NOAECs from the animal studies were several orders of magnitude above the human blood levels for PFAS where associations with vaccination efficacy and PFAS concentrations were reported.
While a mode of action for the immunotoxicity seen in animal models after exposure to PFOS and PFOA has not been established (ATSDR 2021; EFSA-CONTAM Panel et al. 2020), additional uncertainty regarding utility of the animal data on immunotoxicity for human risk assessment is introduced by the major species difference in potency of PFAS between mice and rats and the observation that immunomodulation by PFAS in mice was partially dependent on an interaction of PFAS with PPARα (Qazi et al. 2009b). This may question the use of the mouse as animal model to predict potential immunomodulatory effects in humans as PPARα activation shows marked species differences in responses to PFAS (Takacs and Abbott 2007; Wolf et al. 2012, 2008) and major species differences have been demonstrated for many other compounds interacting with PPARα (Ashby et al. 1994; Bentley et al. 1993; Cattley et al. 1998).
In conclusion, while there is some support for an association of decreased antibody levels in humans with PFAS exposures, the absence of an increased incidence of diphtheria, tetanus, measles, mumps in children exposed to PFAS questions the clinical relevance of the ‘surrogate’ endpoint antibody levels (Edwards 2001; Plotkin 2010, 2013). In addition, the much higher PFAS serum/plasma levels at the NOAELs in animals study also argue against a clinical relevance of the “surrogate” endpoints. A dedicated large-scale study would be required to conclusively establish a reduced vaccination efficacy as an endpoint of PFAS in humans.
References
Abraham K, Mielke H, Fromme H, Volkel W, Menzel J, Peiser M, Zepp F, Willich SN, Weikert C (2020) Internal exposure to perfluoroalkyl substances (PFASs) and biological markers in 101 healthy 1-year-old children: associations between levels of perfluorooctanoic acid (PFOA) and vaccine response. Arch Toxicol 94:2131–2147. https://doi.org/10.1007/s00204-020-02715-4
Ait Bamai Y, Goudarzi H, Araki A, Okada E, Kashino I, Miyashita C, Kishi R (2020) Effect of prenatal exposure to per- and polyfluoroalkyl substances on childhood allergies and common infectious diseases in children up to age 7 years: The Hokkaido study on environment and children’s health. Environ Int 143:105979. https://doi.org/10.1016/j.envint.2020.105979
Ashby J, Brady A, Elcombe CR, Elliott BM, Ishmael J, Odum J, Tugwood JD, Kettle S, Purchase IF (1994) Mechanistically-based human hazard assessment of peroxisome proliferator-induced hepatocarcinogenesis. Hum Exp Toxicol 13(Suppl 2):S1-117. https://doi.org/10.1177/096032719401300201
ATSDR (2021) Agency for Toxic Substances and Disease Registry. Toxicological profile for perfluoroalkyls. U.S. Department of Health and Human Services, Public Health Service, Atlanta, GA. https://wwwn.cdc.gov/TSP/ToxProfiles/ToxProfiles.aspx?id=1117&tid=237. doi:https://doi.org/10.15620/cdc:59198
Bentley P, Calder I, Elcombe C, Grasso P, Stringer D, Wiegand HJ (1993) Hepatic peroxisome proliferation in rodents and its significance for humans. Food Chem Toxicol 31:857–907. https://doi.org/10.1016/0278-6915(93)90225-n
Bjerregaard P, Dewailly E, Ayotte P, Pars T, Ferron L, Mulvad G (2001) Exposure of Inuit in Greenland to organochlorines through the marine diet. J Toxicol Environ Health A 62:69–81. https://doi.org/10.1080/009841001455490
Buck RC, Franklin J, Berger U, Conder JM, Cousins IT, de Voogt P, Jensen AA, Kannan K, Mabury SA, van Leeuwen SP (2011) Perfluoroalkyl and polyfluoroalkyl substances in the environment: terminology, classification, and origins. Integr Environ Assess Manag 7:513–541. https://doi.org/10.1002/ieam.258
Cattley RC, DeLuca J, Elcombe C, Fenner-Crisp P, Lake BG, Marsman DS, Pastoor TA, Popp JA, Robinson DE, Schwetz B, Tugwood J, Wahli W (1998) Do peroxisome proliferating compounds pose a hepatocarcinogenic hazard to humans? Regul Toxicol Pharmacol 27:47–60. https://doi.org/10.1006/rtph.1997.1163
Chou WC, Lin Z (2019) Bayesian evaluation of a physiologically based pharmacokinetic (PBPK) model for perfluorooctane sulfonate (PFOS) to characterize the interspecies uncertainty between mice, rats, monkeys, and humans: Development and performance verification. Environ Int 129:408–422. https://doi.org/10.1016/j.envint.2019.03.058
Chou WC, Lin Z (2020) Probabilistic human health risk assessment of perfluorooctane sulfonate (PFOS) by integrating in vitro, in vivo toxicity, and human epidemiological studies using a Bayesian-based dose-response assessment coupled with physiologically based pharmacokinetic (PBPK) modeling approach. Environ Int 137:105581. https://doi.org/10.1016/j.envint.2020.105581
Cousins IT, DeWitt JC, Gluge J, Goldenman G, Herzke D, Lohmann R, Miller M, Ng CA, Scheringer M, Vierke L, Wang Z (2020) Strategies for grouping per- and polyfluoroalkyl substances (PFAS) to protect human and environmental health. Environ Sci Process Impacts 22:1444–1460. https://doi.org/10.1039/d0em00147c
Dalsager L, Christensen N, Husby S, Kyhl H, Nielsen F, Host A, Grandjean P, Jensen TK (2016) Association between prenatal exposure to perfluorinated compounds and symptoms of infections at age 1–4years among 359 children in the Odense Child Cohort. Environ Int 96:58–64. https://doi.org/10.1016/j.envint.2016.08.026
Dalsager L, Christensen N, Halekoh U, Timmermann CAG, Nielsen F, Kyhl HB, Husby S, Grandjean P, Jensen TK, Andersen HR (2021) Exposure to perfluoroalkyl substances during fetal life and hospitalization for infectious disease in childhood: A study among 1,503 children from the Odense Child Cohort. Environ Int 149:106395. https://doi.org/10.1016/j.envint.2021.106395
Dewitt JC, Copeland CB, Strynar MJ, Luebke RW (2008) Perfluorooctanoic acid-induced immunomodulation in adult C57BL/6J or C57BL/6N female mice. Environ Health Perspect 116:644–650. https://doi.org/10.1289/ehp.10896
DeWitt JC, Blossom SJ, Schaider LA (2019) Exposure to per-fluoroalkyl and polyfluoroalkyl substances leads to immunotoxicity: epidemiological and toxicological evidence. J Expo Sci Environ Epidemiol 29:148–156. https://doi.org/10.1038/s41370-018-0097-y
Dong GH, Zhang YH, Zheng L, Liu W, Jin YH, He QC (2009) Chronic effects of perfluorooctanesulfonate exposure on immunotoxicity in adult male C57BL/6 mice. Arch Toxicol 83:805–815. https://doi.org/10.1007/s00204-009-0424-0
Dong GH, Liu MM, Wang D, Zheng L, Liang ZF, Jin YH (2011) Sub-chronic effect of perfluorooctanesulfonate (PFOS) on the balance of type 1 and type 2 cytokine in adult C57BL6 mice. Arch Toxicol 85:1235–1244. https://doi.org/10.1007/s00204-011-0661-x
Dong GH, Zhang YH, Zheng L, Liang ZF, Jin YH, He QC (2012) Subchronic effects of perfluorooctanesulfonate exposure on inflammation in adult male C57BL/6 mice. Environ Toxicol 27:285–296. https://doi.org/10.1002/tox.20642
EC-EFSA (2012) Guidance on selected default values to be used by the EFSA Scientific Committee, Scientific Panels and Units in the absence of actual measured data. EFSA J 10:2579. https://doi.org/10.2903/j.efsa.2020.6223
Edwards KM (2001) Development, acceptance, and use of immunologic correlates of protection in monitoring the effectiveness of combination vaccines. Clin Infect Dis 33(Suppl 4):S274–S277. https://doi.org/10.1086/322562
EFSA-CONTAM Panel, Schrenk D, Bignami M, Bodin L, Chipman JK, del Mazo J, Grasl-Kraupp B, Hogstrand C, Hoogenboom LR, Leblanc J-C, Nebbia CS, Nielsen E, Ntzani E, Petersen A, Sand S, Vleminckx C, Wallace H, Barregard L, Ceccatelli S, Cravedi J-P, Halldorsson TI, Haug LS, Johansson N, Knutsen HK, Rose M, Roudot A-C, VanLoveren H, Vollmer G, Mackay K, Riol F, Schwerdtle T (2020) Panel on Contaminants in the Food Chain: Scientific Opinion on the risk to human health related to the presence of perfluoroalkyl substances in food. EFSA J 18:391. doi:https://doi.org/10.2903/j.efsa.2020.6223
FDA U (2002) Immunotoxicology evaluation of investigational new drugs. https://www.fda.gov/media/72228/download
Fei C, McLaughlin JK, Lipworth L, Olsen J (2010) Prenatal exposure to PFOA and PFOS and risk of hospitalization for infectious diseases in early childhood. Environ Res 110:773–777. https://doi.org/10.1016/j.envres.2010.08.004
Fragki S, Dirven H, Fletcher T, Grasl-Kraupp B, Bjerve Gutzkow K, Hoogenboom R, Kersten S, Lindeman B, Louisse J, Peijnenburg A, Piersma AH, Princen HMG, Uhl M, Westerhout J, Zeilmaker MJ, Luijten M (2021) Systemic PFOS and PFOA exposure and disturbed lipid homeostasis in humans: what do we know and what not? Crit Rev Toxicol 51:141–164. https://doi.org/10.1080/10408444.2021.1888073
Gomis MI, Vestergren R, Borg D, Cousins IT (2018) Comparing the toxic potency in vivo of long-chain perfluoroalkyl acids and fluorinated alternatives. Environ Int 113:1–9. https://doi.org/10.1016/j.envint.2018.01.011
Goudarzi H, Miyashita C, Okada E, Kashino I, Chen CJ, Ito S, Araki A, Kobayashi S, Matsuura H, Kishi R (2017) Prenatal exposure to perfluoroalkyl acids and prevalence of infectious diseases up to 4years of age. Environ Int 104:132–138. https://doi.org/10.1016/j.envint.2017.01.024
Grandjean P, Andersen EW, Budtz-Jorgensen E, Nielsen F, Molbak K, Weihe P, Heilmann C (2012) Serum vaccine antibody concentrations in children exposed to perfluorinated compounds. JAMA 307:391–397. https://doi.org/10.1001/jama.2011.2034
Grandjean P, Heilmann C, Weihe P, Nielsen F, Mogensen UB, Budtz-Jorgensen E (2017a) Serum vaccine antibody concentrations in adolescents exposed to perfluorinated compounds. Environ Health Perspect 125:077018. https://doi.org/10.1289/EHP275
Grandjean P, Heilmann C, Weihe P, Nielsen F, Mogensen UB, Timmermann A, Budtz-Jorgensen E (2017b) Estimated exposures to perfluorinated compounds in infancy predict attenuated vaccine antibody concentrations at age 5-years. J Immunotoxicol 14:188–195. https://doi.org/10.1080/1547691X.2017.1360968
Granum B, Haug LS, Namork E, Stolevik SB, Thomsen C, Aaberge IS, van Loveren H, Lovik M, Nygaard UC (2013) Pre-natal exposure to perfluoroalkyl substances may be associated with altered vaccine antibody levels and immune-related health outcomes in early childhood. J Immunotoxicol 10:373–379. https://doi.org/10.3109/1547691X.2012.755580
Guruge KS, Hikono H, Shimada N, Murakami K, Hasegawa J, Yeung LW, Yamanaka N, Yamashita N (2009) Effect of perfluorooctane sulfonate (PFOS) on influenza A virus-induced mortality in female B6C3F1 mice. J Toxicol Sci 34:687–691. https://doi.org/10.2131/jts.34.687
Health-Canada (2018) Science Policy Note SPN2018-02, Cumulative Health Risk Assessment Framework. https://www.canada.ca/en/health-canada/services/consumer-product-safety/reports-publications/pesticides-pest-management/policies-guidelines/science-policy-notes/2018/cumulative-health-risk-assessment-framework-spn2018-02.html
Hessel EV, Tonk EC, Bos PM, van Loveren H, Piersma AH (2015) Developmental immunotoxicity of chemicals in rodents and its possible regulatory impact. Crit Rev Toxicol 45:68–82. https://doi.org/10.3109/10408444.2014.959163
ICH (2005) International Conference on Harmonization of Technical Requirements for Registratio of Pharmaceuticals for Human Use. S8 - Immunotoxicity studies for human pharmaceuticals. https://www.ich.org/page/safety-guidelines
Impinen A, Nygaard UC, Lodrup Carlsen KC, Mowinckel P, Carlsen KH, Haug LS, Granum B (2018) Prenatal exposure to perfluoralkyl substances (PFASs) associated with respiratory tract infections but not allergy- and asthma-related health outcomes in childhood. Environ Res 160:518–523. https://doi.org/10.1016/j.envres.2017.10.012
Impinen A, Longnecker MP, Nygaard UC, London SJ, Ferguson KK, Haug LS, Granum B (2019) Maternal levels of perfluoroalkyl substances (PFASs) during pregnancy and childhood allergy and asthma related outcomes and infections in the Norwegian Mother and Child (MoBa) cohort. Environ Int 124:462–472. https://doi.org/10.1016/j.envint.2018.12.041
Johansen P, Pars T, Bjerregaard P (2000) Lead, cadmium, mercury and selenium intake by Greenlanders from local marine food. Sci Total Environ 245:187–194. https://doi.org/10.1016/s0048-9697(99)00443-x
Kielsen K, Shamim Z, Ryder LP, Nielsen F, Grandjean P, Budtz-Jorgensen E, Heilmann C (2016) Antibody response to booster vaccination with tetanus and diphtheria in adults exposed to perfluorinated alkylates. J Immunotoxicol 13:270–273. https://doi.org/10.3109/1547691X.2015.1067259
Ladics GS (2018) The sheep erythrocyte T-dependent antibody response (TDAR). Methods Mol Biol 1803:83–94. https://doi.org/10.1007/978-1-4939-8549-4_6
Lefebvre DE, Curran I, Armstrong C, Coady L, Parenteau M, Liston V, Barker M, Aziz S, Rutherford K, Bellon-Gagnon P, Shenton J, Mehta R, Bondy G (2008) Immunomodulatory effects of dietary potassium perfluorooctane sulfonate (PFOS) exposure in adult Sprague-Dawley rats. J Toxicol Environ Health A 71:1516–1525. https://doi.org/10.1080/15287390802391943
Lin PD, Cardenas A, Hauser R, Gold DR, Kleinman KP, Hivert MF, Calafat AM, Webster TF, Horton ES, Oken E (2021) Temporal trends of concentrations of per- and polyfluoroalkyl substances among adults with overweight and obesity in the United States: Results from the Diabetes Prevention Program and NHANES. Environ Int 157:106789. https://doi.org/10.1016/j.envint.2021.106789
Looker C, Luster MI, Calafat AM, Johnson VJ, Burleson GR, Burleson FG, Fletcher T (2014) Influenza vaccine response in adults exposed to perfluorooctanoate and perfluorooctanesulfonate. Toxicol Sci 138:76–88. https://doi.org/10.1093/toxsci/kft269
Luster MI, Munson AE, Thomas PT, Holsapple MP, Fenters JD, White KL Jr, Lauer LD, Germolec DR, Rosenthal GJ, Dean JH (1988) Development of a testing battery to assess chemical-induced immunotoxicity: National Toxicology Program’s guidelines for immunotoxicity evaluation in mice. Fundam Appl Toxicol 10:2–19. https://doi.org/10.1016/0272-0590(88)90247-3
Luster MI, Portier C, Pait DG, White KL Jr, Gennings C, Munson AE, Rosenthal GJ (1992) Risk assessment in immunotoxicology. I. Sensitivity and predictability of immune tests. Fundam Appl Toxicol 18:200–210. https://doi.org/10.1016/0272-0590(92)90047-l
Luster AD, Alon R, von Andrian UH (2005) Immune cell migration in inflammation: present and future therapeutic targets. Nat Immunol 6:1182–1190. https://doi.org/10.1038/ni1275
NTP (2016) National Toxicology Program. Monograph on immunotoxicity associated with exposure to perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS). National Toxicology Program. Research Triangle Park, NC. https://ntp.niehs.nih.gov/ntp/ohat/pfoa_pfos/pfoa_pfosmonograph_508.pdf
OECD (2018) Organisation for Economic Cooperation and Development. Toward a new comprehensive global database of per- and polyfluoroalkyl substances (PFASs): Summary report on updating the OECD 2007 list of per- and polyfluoroalkyl substances (PFASs)
Okada E, Sasaki S, Saijo Y, Washino N, Miyashita C, Kobayashi S, Konishi K, Ito YM, Ito R, Nakata A, Iwasaki Y, Saito K, Nakazawa H, Kishi R (2012) Prenatal exposure to perfluorinated chemicals and relationship with allergies and infectious diseases in infants. Environ Res 112:118–125. https://doi.org/10.1016/j.envres.2011.10.003
Pachkowski B, Post GB, Stern AH (2019) The derivation of a Reference Dose (RfD) for perfluorooctane sulfonate (PFOS) based on immune suppression. Environ Res 171:452–469. https://doi.org/10.1016/j.envres.2018.08.004
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hrobjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int J Surg 88:105906. https://doi.org/10.1016/j.ijsu.2021.105906
Panieri E, Baralic K, Djukic-Cosic D, Buha Djordjevic A, Saso L (2022) PFAS molecules: a major concern for the human health and the environment. Toxics 10:44
Peden-Adams MM, Keller JM, Eudaly JG, Berger J, Gilkeson GS, Keil DE (2008) Suppression of humoral immunity in mice following exposure to perfluorooctane sulfonate. Toxicol Sci 104:144–154. https://doi.org/10.1093/toxsci/kfn059
Pilkerton CS, Hobbs GR, Lilly C, Knox SS (2018) Rubella immunity and serum perfluoroalkyl substances: sex and analytic strategy. PLoS ONE 13:e0203330. https://doi.org/10.1371/journal.pone.0203330
Pizzurro DM, Seeley M, Kerper LE, Beck BD (2019) Interspecies differences in perfluoroalkyl substances (PFAS) toxicokinetics and application to health-based criteria. Regul Toxicol Pharmacol 106:239–250. https://doi.org/10.1016/j.yrtph.2019.05.008
Plotkin SA (2010) Correlates of protection induced by vaccination. Clin Vaccine Immunol 17:1055–1065. https://doi.org/10.1128/CVI.00131-10
Plotkin SA (2013) Complex correlates of protection after vaccination. Clin Infect Dis 56:1458–1465. https://doi.org/10.1093/cid/cit048
Qazi MR, Bogdanska J, Butenhoff JL, Nelson BD, DePierre JW, Abedi-Valugerdi M (2009a) High-dose, short-term exposure of mice to perfluorooctanesulfonate (PFOS) or perfluorooctanoate (PFOA) affects the number of circulating neutrophils differently, but enhances the inflammatory responses of macrophages to lipopolysaccharide (LPS) in a similar fashion. Toxicology 262:207–214. https://doi.org/10.1016/j.tox.2009.06.010
Qazi MR, Xia Z, Bogdanska J, Chang SC, Ehresman DJ, Butenhoff JL, Nelson BD, DePierre JW, Abedi-Valugerdi M (2009b) The atrophy and changes in the cellular compositions of the thymus and spleen observed in mice subjected to short-term exposure to perfluorooctanesulfonate are high-dose phenomena mediated in part by peroxisome proliferator-activated receptor-alpha (PPARalpha). Toxicology 260:68–76. https://doi.org/10.1016/j.tox.2009.03.009
Qazi MR, Nelson BD, Depierre JW, Abedi-Valugerdi M (2010) 28-Day dietary exposure of mice to a low total dose (7 mg/kg) of perfluorooctanesulfonate (PFOS) alters neither the cellular compositions of the thymus and spleen nor humoral immune responses: does the route of administration play a pivotal role in PFOS-induced immunotoxicity? Toxicology 267:132–139. https://doi.org/10.1016/j.tox.2009.10.035
Selgrade MK (2007) Immunotoxicity: the risk is real. Toxicol Sci 100:328–332. https://doi.org/10.1093/toxsci/kfm244
Shih YH, Blomberg AJ, Bind MA, Holm D, Nielsen F, Heilmann C, Weihe P, Grandjean P (2021) Serum vaccine antibody concentrations in adults exposed to per- and polyfluoroalkyl substances: A birth cohort in the Faroe Islands. J Immunotoxicol 18:85–92. https://doi.org/10.1080/1547691X.2021.1922957
Stein CR, Ge Y, Wolff MS, Ye X, Calafat AM, Kraus T, Moran TM (2016a) Perfluoroalkyl substance serum concentrations and immune response to FluMist vaccination among healthy adults. Environ Res 149:171–178. https://doi.org/10.1016/j.envres.2016.05.020
Stein CR, McGovern KJ, Pajak AM, Maglione PJ, Wolff MS (2016b) Perfluoroalkyl and polyfluoroalkyl substances and indicators of immune function in children aged 12–19 y: National Health and Nutrition Examination Survey. Pediatr Res 79:348–357. https://doi.org/10.1038/pr.2015.213
Takacs ML, Abbott BD (2007) Activation of mouse and human peroxisome proliferator-activated receptors (alpha, beta/delta, gamma) by perfluorooctanoic acid and perfluorooctane sulfonate. Toxicol Sci 95:108–117. https://doi.org/10.1093/toxsci/kfl135
Timmermann CAG, Jensen KJ, Nielsen F, Budtz-Jorgensen E, van der Klis F, Benn CS, Grandjean P, Fisker AB (2020) Serum perfluoroalkyl substances, vaccine responses, and morbidity in a cohort of Guinea-Bissau children. Environ Health Perspect 128:87002. https://doi.org/10.1289/EHP6517
UBA-HBM-Kommission (2020) Bekanntmachung des Umweltbundesamtes. HBM-II-Werte für Perfluoroctansäure (PFOA) und Perfluoroctansulfonsäure (PFOS) in Blutplasma – Stellungnahme der Kommission Human Biomonitoring des Umweltbundesamts. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 63:356–360
US-EPA (2016) Environmental Protection Agency Health Effects Support Document for Perfluorooctane Sulfonate (PFOS). Health and Ecological Criteria Division, Office of Water, U.S. Environmental Protection Agency, Washington, DC
US-EPA (2016) Environmental Protection Agency Health Effects Support Document for Perfluorooctanoic Acid (PFOA). Health and Ecological Criteria Division, Office of Water, US Environmental Protection Agency, Washington, DC
US-EPA (1996a) Environmental Protection Agency. Biochemicals Test Guidelines: OPPTS 880.3550 Immunotoxicity. EPA/712/C-96/280. Washington, DC: Office of Prevention Pesticides and Toxic Substances. 1–14. https://downloads.regulations.gov/EPA-HQ-OPPT-2009-0158-0005/content.pdf
US-EPA (1996b) Environmental Protection Agency. Biochemicals Test Guidelines: OPPTS 880.3800 Immune Response. EPA/712/C-96/281. Washington, DC: Office of Prevention Pesticides and Toxic Substances. US Environmental Protection Agency: 1–8. https://downloads.regulations.gov/EPA-HQ-OPPT-2009-0158-0006/content.pdf
von Holst H, Nayak P, Dembek Z, Buehler S, Echeverria D, Fallacara D, John L (2021) Perfluoroalkyl substances exposure and immunity, allergic response, infection, and asthma in children: review of epidemiologic studies. Heliyon 7:e08160. https://doi.org/10.1016/j.heliyon.2021.e08160
WHO/IPCS (2012) International Programme on Chemical Safety, World Health Organization. Guidance for immunotoxicity risk assessment for chemicals. IPCS Harmonization Project No. 10. http://www.inchem.org/documents/harmproj/harmproj/harmproj10.pdf, Geneva
Wolf CJ, Takacs ML, Schmid JE, Lau C, Abbott BD (2008) Activation of mouse and human peroxisome proliferator-activated receptor alpha by perfluoroalkyl acids of different functional groups and chain lengths. Toxicol Sci 106:162–171. https://doi.org/10.1093/toxsci/kfn166
Wolf CJ, Schmid JE, Lau C, Abbott BD (2012) Activation of mouse and human peroxisome proliferator-activated receptor-alpha (PPARalpha) by perfluoroalkyl acids (PFAAs): further investigation of C4–C12 compounds. Reprod Toxicol 33:546–551. https://doi.org/10.1016/j.reprotox.2011.09.009
Woodlief T, Vance S, Hu Q, DeWitt J (2021) Immunotoxicity of per- and polyfluoroalkyl substances: insights into Short-chain PFAS exposure. Toxics. https://doi.org/10.3390/toxics9050100
Zeng XW, Bloom MS, Dharmage SC, Lodge CJ, Chen D, Li S, Guo Y, Roponen M, Jalava P, Hirvonen MR, Ma H, Hao YT, Chen W, Yang M, Chu C, Li QQ, Hu LW, Liu KK, Yang BY, Liu S, Fu C, Dong GH (2019) Prenatal exposure to perfluoroalkyl substances is associated with lower hand, foot and mouth disease viruses antibody response in infancy: Findings from the Guangzhou Birth Cohort Study. Sci Total Environ 663:60–67. https://doi.org/10.1016/j.scitotenv.2019.01.325
Zeng XW, Li QQ, Chu C, Ye WL, Yu S, Ma H, Zeng XY, Zhou Y, Yu HY, Hu LW, Yang BY, Dong GH (2020) Alternatives of perfluoroalkyl acids and hepatitis B virus surface antibody in adults: Isomers of C8 Health Project in China. Environ Pollut 259:113857. https://doi.org/10.1016/j.envpol.2019.113857
Zheng L, Dong GH, Jin YH, He QC (2009) Immunotoxic changes associated with a 7-day oral exposure to perfluorooctanesulfonate (PFOS) in adult male C57BL/6 mice. Arch Toxicol 83:679–689. https://doi.org/10.1007/s00204-008-0361-3
Zheng L, Dong GH, Zhang YH, Liang ZF, Jin YH, He QC (2011) Type 1 and Type 2 cytokines imbalance in adult male C57BL/6 mice following a 7-day oral exposure to perfluorooctanesulfonate (PFOS). J Immunotoxicol 8:30–38. https://doi.org/10.3109/1547691X.2010.537287
Acknowledgements
3M, the company that funded portions of this research, previously manufactured products containing perfluorooctanoyl chemistries, including PFOA and PFOS. The 3M support was to Prof. Dr. Wolfgang Dekant, a retired professor of toxicology at the Department of Pharmacology and Toxicology of the University of Würzburg and today an independent consultant to several REACH consortia, trade organization and individual companies.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Each author certifies that their freedom to design, conduct, interpret, and publish research was not compromised by the sponsor. No competing interests. The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Antoniou, E., Colnot, T., Zeegers, M. et al. Immunomodulation and exposure to per- and polyfluoroalkyl substances: an overview of the current evidence from animal and human studies. Arch Toxicol 96, 2261–2285 (2022). https://doi.org/10.1007/s00204-022-03303-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00204-022-03303-4