
Abstract
The aim of this study was to determine the percutaneous absorption flux of BaP (20 μg/cm2 in ethanol) and the usefulness of urinary 3-OHBaP as a bio-indicator of dermal exposure to BaP. The percutaneous absorbed dose and absorption flux were estimated by comparison with intravenous administration of BaP (0.01 and 0.05 mg/kg in Cremophor®) as reference way. A percutaneous absorption flux of 0.37 μg/cm²/h was determined by killing groups of rats, following exposure time of 4.5 and 24 h. [14C] skin content was 3.1 μg/cm2, after 24 h exposure to BaP. Total urinary 3-OHBaP accounted for 0.4% of the real absorbed dose, which was fourfold higher than the percentage of an intravenous dose excreted as 3-OHBaP. This finding reveals that percutaneous absorption of BaP, based on the ratio of urinary excretion of 3-OHBaP following percutaneous exposure compared to percutaneous absorption following intravenous administration of BaP, is overestimated in the rat. In vitro, BaP was intensively metabolised by rat skin. Unchanged BaP and 3-OHBaP in receptor fluid accounted for 50 and 30% of the total radioactivity. This percutaneous first past effect of BaP in rats could, in part, explain the higher urinary excretion ratio of 3-OHBaP compared to the value based on intravenous administration of BaP. Conversely, BaP was largely lower metabolised as 3-OHBaP during percutaneous absorption by humans, so BaP absorption flux should be overestimated to a lesser extent in humans than in rats.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Polycyclic aromatic hydrocarbons (PAHs) are a group of numerous compounds, some of which [i.e. Benzo(a)pyrene (BaP)] are known to be carcinogenic (IARC 1983). PAHs are ubiquitously present in the environment and a population may be exposed to them by inhalation of air, traffic exhaust, tobacco smoke or dietary ingestion, particularly of grilled or smoked food. PAHs are also present in petroleum products, especially in coal tar and its derivatives, and are produced during incomplete combustion of organic compounds.
Occupational exposures are associated with cancer of lung, skin and bladder. In the workplace, PAHs are absorbed by inhalation and skin contamination, which may be an important path of uptake (Jongeneelen et al. 1988b; Van Rooij et al. 1992). Based on estimates of dermal and respiratory pyrene uptake, an average 75% of total absorbed pyrene enters the body of coke oven workers through the skin (Van Rooij et al. 1993). These authors consider that monitoring of ambient air alone may drastically underestimate worker’s total exposure. On the other hand, some studies give lower values based on other estimating methods. Dermal absorption of coke over workers has been evaluated at about 20% of the total absorbed dose (Brzeznicki et al. 1997). Inhalatory and cutaneous route proportions have been shown to be roughly equal in two different workplaces (cathode relining, artificial target manufacturing) (Lafontaine et al. 2000, 2002). Despite divergences in the quantitative distribution between these two penetration routes, nobody nevertheless contests the significance of percutaneous intake.
Extensive efforts have been made to validate biological indicators of PAH exposure such as urinary 1-hydroxypyrene (Jongeneelen et al. 1988a; Clonfero et al. 1989; Buckley and Lioy 1992; Boogaard and van Sittert 1994; Quinlan et al. 1995; Lafontaine et al. 2000) or hydroxyphenanthrene (Angerer et al. 1997; Bentsen-Farmen et al. 1999; Heudorf and Angerer 2001a; Heudorf and Angerer 2001b; Becker et al. 2003). These two metabolites appear to provide effective parameters for evaluating internal exposure. On the other hand, they are insufficient as markers for assessing carcinogenic risk. Neither pyrene nor phenanthrene, the respective parent compound, possesses noteworthy carcinogenic potential. In contrast, BaP has a high carcinogenic potency and its concentration in air has been used as a marker for accessing external PAH exposure. Urinary excretion of 3-OHBaP has been proposed as a biomarker for BaP, which takes into account the concomitant inhalation and skin contamination exposure. However, hygienists have only occasionally applied this approach (Ariese et al. 1994; Gundel et al. 2000). The main reason for this has been the lack of sensitivity of current methods. Urinary excretion levels of 3-OHBaP are 1,000–10,000 times lower than those of 1-OHPy. The advantages of 3-OH-BaP as an exposure biomarker have only been examined with recent sufficiency of sensitive analytical methods (Gundel and Angerer 2000; Simon et al. 2000; Fan et al. 2006).
The most appropriate sampling time for urinary 3-OHBaP has been determined in two studies (Gendre et al. 2002, 2004). One of the aims of a subsequent study (Lafontaine et al. 2004) was to assess a urinary limit value based on the relation between atmospheric BaP and maximum urinary 3-OHBaP concentration. Only people with predominantly respiratory exposure were chosen to avoid artefacts resulting from dermal exposure. A very close relationship between the above two variables (n = 21, r = 0.95, P < 0.0001) was observed for 21 workers in different workplaces.
More recently, 3-OHBaP has been measured in the urine of workers exposed to BaP, again in different workplaces (Forster et al. 2008). Poor correlation of 3-OHBaP in urine and BaP in air was attributed to uptake routes other than via inhalation, such as dermal uptake.
These limited studies would seem to show that 3-OHBaP is a specific, sensitive biomarker for diagnosis purposes. However, urinary levels of a biomarker should be proportional to the real absorbed dose if they are to be truly relevant, irrespective of the exposure route. Control experiments are required for determining the proportionality coefficient between urinary 3-OHBaP excretion and BaP internal dose. Until recently, ethics and analytical limits have curbed control experiments on volunteers and thus the real absorbed dose is generally unknown.
The present study was conducted in animals to determine the suitability of 3-OHBaP as a biomarker for dermal exposure. Batches of rats were killed following different [14C] BaP dermal exposure times up to 24 h. The real absorbed dose and absorption flux were determined from radioactivity in excreta and carcasses. BaP percutaneous absorption flux was estimated from the 3-OHBaP excretion rate in urine of the rat batch, which had been exposed for 24 h. Cutaneous first-past effect was estimated from urinary 3-OHBaP excretion, after topical exposure and IV administration of [14C] BaP (reference way). Moreover, in vitro experiments were conducted to compare the BaP percutaneous metabolism in human and rat skin.
Materials and methods
Chemicals
Radiolabelled benzo(a)pyrene ([7,10-14C]benzo(a)pyrene, batch CFA471) with a specific radioactivity of 2.3 GBq/mmol (61 mCi/mmol) and 37 MBq per glass vial was purchased from Amersham Pharmacia Biotech (Buckinghamshire, England). Its radiochemical purity, determined by the supplier, was 98.7% by HPLC or 98.3% by TLC. A radiochemical check was performed on each stock solution by HPLC, after diluting in unlabelled benzo(a)pyrene or in a vehicle (ethanol for dermal exposure or Cremophore and saline solution for intravenous administration). Administration solutions were prepared 1 day before the experiments by weighing labelled [14C]BaP, unlabelled benzo(a)pyrene and the vehicle. Radiochemical concentration was determined on three aliquots. Unlabelled benzo(a)pyrene was supplied by Sigma-Aldrich (Saint Louis, USA). Identification and chemical purity checking was performed by HPLC on receipt of the product. Its purity was 98.6%. All other chemicals were of the highest purity available.
Animals
Male Sprague–Dawley hairy rats (Charles River, Saint Germain sur l’Arbresle, France) weighing 250–350 g were used. The animals were acclimatised to laboratory conditions for at least 4 days prior to initiating the studies in rooms with a 12 h light/dark cycle designed to maintain relative humidity at 50 ± 5% and temperature at 22 ± 1°C. Commercial food pellets (UAR Alimentation-Villemoison, Epinay sur Orge, France) and tap water were available ad libitum.
Mass balance and urinary 3-OHBaP excretion after intravenous administration (reference way)
Two doses of labelled [14C] benzo(a)pyrene (0.05 mg/kg, n = 6 and 0.01 mg /kg, n = 6) were injected intravenously in a Cremophor® solution (1 mL/kg) into the dorsal vein of the penis of the male hairy rats, lightly anaesthetised under isoflurane. The individual dose was determined by weighing the syringe before and after each administration. The radiocarbon dose was about 3.7 MBq/kg (100 μCi/kg).
Immediately after the dose administration, the rats were placed in individual metabolic cages for collection of urine and faeces at 4°C. Urine was collected at 4.5, 24, 30, 48, 54 and 72 h, whilst faeces were collected each day. At the end of the experiment (72 h), animals were killed by bleeding the abdominal aorta under isoflurane anaesthesia. The radioactivity content of excreta and carcasses and the 3-OHBaP urinary content was analysed by HPLC.
In vivo percutaneous penetration and absorption of [14C]benzo(a)pyrene in ethanol determined by killing
Preparation of animals
One day before the dose was administered, the middle of the back of male hairy rats was clipped with electric clippers. A circular ring (3.5 cm2) was glued with DELO-CA® cyanocrylate (DELO GmbH & Co., Landsberg, Germany) one hour before the application of the toxicant.
Topical dosing of [14C] benzo(a)pyrene in ethanol under occlusion
Experiments were performed with [14C]BaP in ethanol (0.4 μg BaP/μL, 50 μL/cm2, 20 μg BaP/cm2, 3.5 cm2). After topical application of [14C]BaP, the ring was covered by a Tedlar® membrane cap to ensure occlusion. Immediately after the dose was applied, rats were placed in individual metabolic cages for collection of urine and faeces. Batches of rats were killed at different dermal exposure times (0.5–24 h).
Unabsorbed dose washing
At the end of the exposure time, 500 μL of ethanol was introduced through the Tedlar® membrane. The Tedlar® membrane was then cut with a scalpel and the [14C]BaP remaining at the application site was removed using a pipette followed by application of three dry cotton swabs. The skin around the application site was washed with a cotton swab humidified with ethanol to detect any leakage of the tested compound outside the ring. Each step of the removal was separately analysed.
Determination of BaP percutaneous absorption flux by killing
Different batches of rats were killed after BaP dermal exposure time of 0.5–24 h. For each exposure time, the real absorbed dose was determined from radioactivity in the carcass and excreta. Absorption flux was determined from the absorbed dose curve versus exposure time.
Estimation of BaP percutaneous absorption flux based on urinary [14C] and 3-OH BaP urinary excretion rate from catheterised rats
A catheter was introduced into the bladder of six rats 1 week before the dermal exposure experiment. After topical application of [14C] BaP, urinary excretion was induced by injecting 2 mL of a saline solution containing 1% of bovine serum albumin into the catheter at different times for 72 h (corresponding to the end of the experiment). The exposed skin area was washed at 24 h post dosing to eliminate the unabsorbed BaP dose. Animals were killed 48 h after the end of the exposure.
In vitro percutaneous absorption and metabolism of [14C] BaP
In vitro percutaneous absorption was assessed with static diffusion cells using fresh dermatomed skin of male rats (0.37 ± 0.02 mm, n = 3) and skin from women (0.39 ± 0.06 mm, n = 3). The rats were killed with Pentobarbital® and the whole dorsal region was collected. The human skin specimens were obtained from the hospital after plastic abdominal reduction surgery. The skin tissue was transferred into a container with ice. To minimise the loss of viability of the skin tissue, experiments were initiated within 4 h of surgery.
The skin samples were shaved and the excess of subcutaneous tissue was carefully removed and dermatomed (Zimmer Electric Dermatome, Ohio, USA). The skin was cut into circular sections (1 per rat and 2 per human skin) and placed, stratum corneum side up, in diffusion cells. The diffusion cells were kept at a temperature of 36°C with a circulating water bath, which created a skin surface temperature of 32 ± 1°C. The dermis side was kept in contact with the RPMI receptor fluid (Life Technologies, Paisley, Scotland) containing 2% bovine albumin and 1% penicillin–streptomycin. The fluid receptor was previously filtered through a sterile Millex® (Millipore, Bedford, USA) 0.22 μm pore size filter and degassed with a vacuum pump. Preliminary experiments had shown that absorption flux was not significantly different when the receptor fluid was NaCl 0.9%. The integrity of the skin samples was assessed by determining the trans-epidermal water loss (Tewameter®, TM210, Courage + Khazaka) after an equilibrium time of 1 h.
[14C] BaP in ethanol (0.4 μg BaP/μL, 50 μL/cm2, 20 μgBaP/cm2) was applied to a skin surface area of 1.76 cm2. The cells were occluded. Receptor fluid (5.15 ml) was collected and replaced with fresh liquid at 24, 48, 72 and 96 h. At the end of the experiment, the unabsorbed dose of [14C] BaP was removed with dichloroethane (1 × 500 μL) and cotton swabs. The skin was digested in KOH (25%; W/V). The radioactivity contained in the receptor fluid samples, the washing water, and the skin homogenates was measured by adding 10 ml of liquid scintillation solution (Pico Fluor 30, Packard, St Louis, USA). Aliquot of receptor fluid was analysed by HPLC before (unchanged BaP and free 3-OHBAP) and after hydrolysis (unchanged BaP and total 3-OHBaP) by Helix pomatia βglucuronidase and arylsulfatase.
HPLC analysis of urinary 3-OHBaP by fluorescence
The method used was adapted from human urine analysis (Simon et al. 2000). Urine samples (0.5 mL) were diluted twofold with acetate buffer (5 × 10−2 M, pH 5), then vortex-mixed and incubated for 1 h at 37°C with β-glucuronidase and arylsulfatase from Helix pomatia (Merck, Darmstadt, Germany).
Preparation and determination of total radioactivity in biological samples
Radioactivity was determined by direct liquid scintillation counting for urine, plasma, washing cage and in a homogenate of skin and carcass after digestion in 80% ethanol solution of KOH 1.5 M, 1 W/4 V.
Expression of data and statistical analysis
Values were expressed as mean ± SEM. Statistic analysis was performed with Statgraphics software (Sigma Plus, Statical Graphics Corp.). Time-related variation of [14C] and 3-OHBaP urinary excretion rates after intravenous administration was analysed using the Sigma-minus method (Ritschel 1980) with Kinetica software (InnaPhase, Philadelphia, PA). The time-related cumulative urinary excretion of [14C] or 3 OHBaP curve was fitted using a non-linear regression method (see Eqs. 4a, b) with Prism 4 (GraphPad software, INC, San Diego, USA).
For all batches of rats, the percentage of absorbed dose was calculated from:
The percentage of penetrated dose was calculated from:
For experiment by killing, penetration and absorption flux were determined from the slope of the time-related absorbed dose curve.
in which Q(t) = the absorbed dose at time (t), A = absorption flux and A = intecept of the curve when Q(t) = 0.
For catheterised rat experiment, toxicokinetic parameters of [14C] and 3-OHBaP urinary excretion were determined from the time-related cumulative urinary excretion curve based on Eqs. 4a and 4b. For (t) < Tau,
For t > Tau,
in which Tau = the calculated exposure time; KE = the apparent urinary excretion rate of [14C] or 3-OHBaP; A = R/Fu corresponds to the percutaneous absorption flux (R) divided by the fraction of the intravenous dose excreted in urine as [14C] or 3-OHBaP (Fu). A lag time of 7 h was applied to the 3-OHBaP to take into account its excretion delay.
The absorbed dose was estimated from Eq. 5.
Absorption flux was determined from urinary excretion rate of [14C] and 3-OHBaP over the 22–24 h period, based on Eq. 6.
Results
Mass balance and urinary 3-OHBaP excretion after intravenous administration
Table 1 compares the mass balance of [14C] radioactivity after administering intravenously 0.01 and 0.05 mg/kg doses of [14C] BaP to male Sprague Dawley hairy rats. The [14C] was mainly excreted in the faeces: 87 and 96% of the above lower and higher doses, respectively (Table 1).
For the above two doses, [14C] urinary excretion rates were highest during the first collection period (0–4.5 h) and then decreased with time according to a simple exponential function (results not shown). In contrast, urinary excretion rate of 3-OHBaP was highest during the 4.5–24 h period. After 24 h, the urinary excretion rate of this metabolite decreased according to a single exponential function (Fig. 1). Apparent urinary excretion half-life (T 1/2) of 3-OHBaP was significantly highest for the higher dose (9.2 h) than for the lower dose (7.7 h). The total 3-OHBaP excreted in urine was 0.12% of the administered dose in each case.

Urinary excretion rate of [14C] and 3-OHBaP after a single intravenous administration of [14C] BaP in male Sprague Dawley rats. Values are expressed as mean ± SEM (n = 6). Background level of 3-OHBaP determined one day before the administration was 0.003 ± 0.000 ng/h. Urinary excretion rate of 3-OHBaP after intravenous administration of [14C]BaP at 0.01 mg/kg (open circle) and 0.05 mg/kg (filled square). Apparent urinary half-life was 7.7 ± 0.2 h and 9.2 ± 0.3 h for the lowest and highest dose, respectively
In vivo percutaneous absorption flux of [14C]BaP by killing
[14C] BaP was applied in ethanol (50 μL/cm2, 20 μg/cm2, 3.5 cm2) under occlusion. Groups of animals were killed after different exposure times (maximum 24 h). [14C] skin content increased linearly with time up to 4.5 h (Table 2). During this period, the percutaneous absorption flux was 0.12 μg Equivalent/cm2/h (Fig. 2). For exposure time of 4.5–24 h, [14C] skin content did not significantly increase with the exposure time and was 3.4 (± 0.1) μg Equivalent/cm2). In contrast, for exposure time of 4.5–24 h, the absorbed dose increased linearly with exposure time. The absorption flux, calculated over this period, was 0.37 ± 0.02 μg/cm2/h, and the calculated lag time was 3.5 h. At the end of the experiment (24 h), 7.7 μg Equivalent/cm2 of BaP have been absorbed.

In vivo cumulative percutaneous penetration and absorption curves versus time of [14C]benzo(a)pyrene in male Sprague Dawley rats. Batches of male Sprague Dawley rats were killed at different times after a topical application of [14C]benzo(a)pyrene in ethanol and under occlusion (0.4 μg benzo(a)pyrene/μL, 50 μL of the solution/cm2, 20 μg benzo(a)pyrene/cm2, 3.5 cm2, maximal exposure time 24 h). Values are expressed as mean ± SEM. Time course of cumulative penetration (filled circles) and absorption (open circles) curves. Absorption flux for the 4.5–24 h period was F1 (μg/cm2/h) = 0.37 (± 0.02) − 1.24 (± 0.23), T lag = 3.3 h. Penetration flux for the 0–24 h period was F2 (μg/cm2/h) = 0.45 (± 0.02) +1.14 (± 0.28)
Absorbed dose and absorption flux estimated from [14C] and 3-OH BaP urinary excretion by catheterism
[14C] and 3-OHBaP were analysed in urine of rats topically exposed for 24 h and killed at 72 h. The real absorbed dose, determined from the mass balance of [14C], was 52% of the applied dose (Table 3). Total [14C] and 3-OHBaP excreted in urine accounted for 12 and 0.44% of the real absorbed dose. At the end of the experiment, the skin [14C] content accounted for 0.8 μg Equivalent/g.
The cumulative urinary excretion curve of [14C] and 3-OHBaP were closely fitted using a perfusion experiment algorithm (Figure 3). The apparent urinary elimination half-life of [14C] did not differ significantly from that of 3-OHBaP (9.1 h) (Table 4). The estimated exposure time was 25 h, which agrees with the real exposure time.

In vivo cumulative urinary excretion of [14C] and 3-OHBaP curves versus time after dermal exposure to [14C]BaP. Values are expressed as mean ± SEM (n = 6). Male Sprague Dawley rats were topically exposed for 24 h to [14C]benzo(a)pyrene in ethanol and under occlusion (0.4 μg/μL, 50 μL of the solution/cm2, 20 μg benzo(a)pyrene/cm2, 3.5 cm2) and killed 48 h after the end of the exposure. Toxicokinetics parameters for urinary excretion of [14C] (filled circles) and 3-OHBaP (open circles) are reported in Table 3
The absorbed dose estimated from total [14C] urinary excretion (57% of the dose) was very similar to the real absorbed dose determined from the radioactivity mass balance (Table 4). On the other hand, the absorbed dose estimated from total urinary excretion of 3-OHBaP (212% of the dose) was fourfold higher than the real absorbed dose. Similarly, the absorption flux estimated from the time-related cumulative urinary excretion curve for 3-OHBaP or from the urinary excretion rate of 3-OHBaP over the 22–24 h period were approximately sevenfold higher than the absorption flux determined by killing rat batches after different exposure times.
In vitro percutaneous absorption and metabolism of [14C] BaP
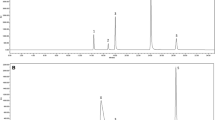
After 24 h of exposure, liquid receptor [14C] content was approximately threefold higher for rat skin (2253 μgEq/cm2) than for human skin (719 μg/cm2) (Fig 4). High inter-skin variation was observed (%CV = 68%) for human skin and more than 85% of the [14C] content were BaP metabolites for the latter skin, whilst total 3-OHBaP accounted for less than 10% of the [14C] content. In contrast, unchanged BaP and total 3-OHBaP (mainly as 3-OHBaPgluc) accounted for 53% and 23% of liquid receptor [14C] content, respectively, after rat skin exposure.

In vitro percutaneous absorption of [14C]BaP in dermatomed skin rats and human. Values are expressed as mean ± SEM. Dermatomed fresh rat (bars with horizontal lines) or human (bars with vertical lines) skins were topically exposed for 24 h under occlusion (0.4 μg/μL, 50 μL of the solution/cm2, 20 μg benzo(a)pyrene/cm2, 3.5 cm2). Total [14C] content in liquid receptor was 2253 ± 374 pmol/cm2/24 h for rat skins and 719 ± 243 pmol/cm2/h for human skins
Discussion
The aim of this study was to determine the percutaneous absorption flux of BaP and the usefulness of urinary 3-OHBaP as a bio-indicator of a dermal exposure to BaP. Percutaneous absorbed dose and absorption flux were estimated in relation to intravenous administration of BaP as a reference method.
The penetrated dose of [14C] BaP, determined from batches of rats killed after various times, increased linearly for exposure times between 0.5 and 24 h; penetration flux was 0.45 μg Equivalent/cm2/h. Between 0.5 and 4.5 exposure hours, skin [14C] content increased steadily with time, indicating higher penetration than absorption flux. On the other hand, between exposures of 4.5 h and 24 h, skin [14C] content (3.1 μg Equivalent/cm2) did not differ significantly, showing that absorption flux and penetration flux were in steady state. The absorption flux was 0.37 μg/cm2/h during the latter exposure periods. For a 24 h exposure, 40% (7.7 μg Equivalent/cm2) and 57% (10.9 μg/cm2) of the applied dose were absorbed and penetrated the skin, respectively. The latter penetration value agreed with the percentages of applied dose recovered in urine, excreta and carcasses of rats (6.1 μ/cm2) or of guinea pigs (9.1 μg/cm2) exposed for 24 h; these figures representing 69% and 68% of the applied dose, respectively.
Similar results were obtained in rats exposed for 24 h and killed 48 h after the end of exposure. Total absorbed and penetrated doses were 52 and 57% of the applied dose, respectively. Comparing skin content for the two experiments revealed that part of the [14C] skin content at 24 h was absorbed during the 24–48 h period. The skin reservoir represented approximately 30% of the total absorbed dose. The skin reservoir contribution to body burden was lower than that for brief exposure to pyrene (Payan et al. 2008). This reduced skin reservoir effect was confirmed by the half-life urinary excretion of 3-OHBaP. Urinary elimination half-lives of 3-OHBaP following dermal exposure (8.9 h) were in fact similar to those following intravenous administration (7.6 and 9.2 h). In contrast, the urinary elimination half-life of 1-OHpyrene was twofold higher after dermal exposure than after intravenous administration (Payan et al. 2008). It should be noted that the urinary excretion half-life of 3-OHBaP obtained in this study was similar to the half-life determined in rats following intravenous administration of BaP (8.1 h) or 3-OHBaP (7.6 h) (Bouchard and Viau 1996). Moreover, it was similar to the half-life determined for workers with mainly respiratory exposure to BaP (8.8 h, n = 21) (Lafontaine et al. 2004) and for those exposed through inhalation and/or skin contamination (8.6 h, n = 60) (Lafontaine, personal report).
Total [14C] urinary excretion after topical exposure corresponded to 12% of the real absorbed dose determined from radioactivity in excreta and carcass. This percentage was similar to the value obtained after intravenous administration of [14C] BaP. BaP percutaneous absorption was therefore accurately estimated from total urinary excretion of [14C]. On the other hand, total urinary excretion of 3-OHBaP after dermal exposure accounted for 0.44% of the real absorbed dose. This percentage was fourfold higher than that following intravenous administration of BaP in the present study (0.1% of 0.01 and 0.05 mg/kg BaP doses) or than that reported by Bouchard and Viau 1996(0.1% of a 10 mg BaP/kg dose). This result leads to an overestimating of both the percutaneous absorbed dose and the BaP absorption flux, when toxicokinetic parameters provided by the intravenous reference method were used. For rat 3-OHBaP urinary excretion compared with absorbed dose, the difference between the two exposure routes (intravenous and percutaneous) may be partly due to a percutaneous first past effect. BaP intensive percutaneous metabolism has been previously reported in mouse, rat, guinea pig and human metabolic viable skin (Kao et al. 1985; Ng et al. 1992; Moody et al. 1995). Approximately, 50% of the absorbed dose represented BaP metabolites, based on in vitro experiments on rat skin conducted under identical exposure conditions to those applied to in vivo experiments. Total 3-OHBaP alone accounted for 23% of the absorbed dose and it has previously been reported that the fraction of administered dose excreted in urine as 3-OHBaP is sevenfold higher following 3-OH BaP administration than that following parent administration (Bouchard and Viau 1996). If we consider 2.2 ± 0.7% (n = 3) of an intravenous dose of 3-OHBaP glucuronoconjugate (96 μg/kg) (result not shown), the percentage of percutaneous absorbed dose excreted as 3-OHBaP should be 0.55% (50% unchanged BaPX0.001 + 23% 3-OHBaP glucuronoconjugate × 0.022), which is close to the value of 0.44% obtained in this study.
If the rat absorption fluxes, based on the absorbed dose and on urinary excretion of 3-OHBaP, are both overestimated, this should also be the outcome, albeit to a lesser degree, in humans. The in vitro experiments revealed that, although BaP was more intensively metabolised by human skin than by rat skin, 3-OHBaP in fact represented only 8% of the total absorbed dose compared with 23% for rat skin. A calculation similar to the one above indicates that 0.2% of a percutaneous absorbed dose should be excreted in human urine (14% unchanged BaP × 0.001 + 8% × 0.022). This is effectively noticeable for workers mainly exposed by inhalation to HAP: 3-0HBaP excreted in urine accounted for 0.07% (n = 21) of a calculated inhaled BaP dose % with a pulmonary retention of 100% (M. Lafontaine, personal report).
Unlike the [14C] urinary excretion rate, which was maximum over the initial sample collection period after an intravenous administration of [14C] BaP, the 3-OHBaP urinary excretion rate was maximum over the 4–24 h collection period. Similar results were obtained following intravenous administration of BaP or a mixture of four BaP metabolites containing 3-OHBaP itself (Bouchard and Viau 1996). The 3-OHBaP maximum excretion rate occurred 10 h after dosing. In workers assumed to be exposed by the HAP inhalation route, the 3-OHBaP maximum urinary excretion rate occurred 3–24 h after the 1-OHPyrene maximum excretion rate (mean lag = 15 h) (Gendre et al. 2004). This delay in reaching the 3-OHBaP maximum urinary excretion rate leads these authors to recommend collecting urine from workers the following pre-shift day following exposure to HAP. Further studies are required to explain the reason of the delay in 3-OHBaP urinary excretion rate compared with other BaP metabolites.
In conclusion, urinary excretion of 3-OHBaP is closely proportional to the administered dose following BaP intravenous administration. However, percutaneous absorption of BaP based on the ratio of 3-OHBaP urinary excretion after percutaneous exposure and compared with intravenous administration is overestimated in relation to time. This finding may be in part explained by the BaP metabolising to 3-OHBaP in the skin. In humans, BaP is metabolised far less as 3-OHBaP during its percutaneous absorption, so the overestimation of the BaP absorption flux should occur to a lesser extent in humans than in rats.
Abbreviations
- BaP:
-
Benzo(a)pyrene
- 3-OHBaP:
-
3-Hydroxybenzo(a)pyrene
- BSA:
-
Bovine serum albumin
- PAH:
-
Polycyclic aromatic hydrocarbons
- i.v.:
-
Intravenous
- HPLC:
-
High performance liquid chromatography
References
Angerer J, Mannschreck C, Gundel J (1997) Occupational exposure to polycyclic aromatic hydrocarbons in a graphite-electrode producing plant: biological monitoring of 1-hydroxypyrene and monohydroxylated metabolites of phenanthrene. Int Arch Occup Environ Health 69:323–331
Ariese F, Verkaik M, Hoornweg GP, van de Nesse RJ, Jukema-Leenstra SR, Hofstraat JW, Gooijer C, Velthorst NH (1994) Trace analysis of 3-hydroxy benzo[a]pyrene in urine for the biomonitoring of human exposure to polycyclic aromatic hydrocarbons. J Anal Toxicol 18:195–204
Becker K, Schulz C, Kaus S, Seivert B (2003) German Environmental Survey 1998 (GerEs III): environmental pollutants in urineof the German population. Int J Hyg Environ Health 206:15–24
Bentsen-Farmen RK, Botnen IV, Noto H, Jacob J, Ovrebo S (1999) Detection of polycyclic aromatic hydrocarbon metabolites by high-pressure liquid chromatography after purification on immunoaffinity columns in urine from occupationally exposed workers. Int Arch Occup Environ Health 72:161–168
Boogaard PJ, van Sittert NJ (1994) Exposure to polycyclic aromatic hydrocarbons in petrochemical industries by measurement of urinary 1-hydroxypyrene. Occup Environ Med 51:250–258
Bouchard M, Viau C (1996) Urinary excretion kinetics of pyrene and benzo(a)pyrene metabolites following intravenous administration of the parent compounds or the metabolites. Toxicol Appl Pharmacol 139:301–309
Brzeznicki S, Jakubowski M, Czerski B (1997) Elimination of 1-hydroxypyrene after human volunteer exposure to polycyclic aromatic hydrocarbons. Int Arch Occup Environ Health 70:257–260
Buckley TJ, Lioy PJ (1992) An examination of the time course from human dietary exposure to polycyclic aromatic hydrocarbons to urinary elimination of 1-hydroxypyrene. Br J Ind Med 49:113–124
Clonfero E, Zordan M, Venier P, Paleologo M, Levis AG, Cottica D, Pozzoli L, Jongeneelen FJ, Bos RP, Anzion RB (1989) Biological monitoring of human exposure to coal tar. Urinary excretion of total polycyclic aromatic hydrocarbons, 1-hydroxypyrene and mutagens in psoriatic patients. Int Arch Occup Environ Health 61:363–368
Fan R, Dong Y, Zhang W, Wang Y, Yu Z, Sheng G, Fu J (2006) Fast simultaneous determination of urinary 1-hydroxypyrene and 3-hydroxybenzo[a]pyrene by liquid chromatography-tandem mass spectrometry. J Chromatogr B Analyt Technol Biomed Life Sci 836:92–97
Forster K, Preuss R, Rossbach B, Bruning T, Angerer J, Simon P (2008) 3-Hydroxybenzo[a]pyrene in the urine of workers with occupational exposure to polycyclic aromatic hydrocarbons in different industries. Occup Environ Med 65:224–229
Gendre C, Lafontaine M, Morele Y, Payan JP, Simon P (2002) Relationship between urinary levels of 1-hydroxypyrene and 3-hydroxypyrene for workers exposed to polyclyc aromatic hydrocarbons. Polycycl Aromat Compd 22:761–769
Gendre C, Lafontaine M, Delsaut P et al (2004) Exposure to polycyclic aromatic hydrocarbons and excretion of urinary 3-hydroxybenzo[a]pyrene: assessment of an appropriate sampling time. Polycycl Aromat Compd 24:433–439
Gundel J, Angerer J (2000) High-performance liquid chromatographic method with fluorescence detection for the determination of 3-hydroxybenzo[a]pyrene and 3-hydroxybenz[a]anthracene in the urine of polycyclic aromatic hydrocarbon-exposed workers. J Chromatogr B Biomed Sci Appl 738:47–55
Gundel J, Schaller KH, Angerer J (2000) Occupational exposure to polycyclic aromatic hydrocarbons in a fireproof stone producing plant: biological monitoring of 1-hydroxypyrene, 1-, 2-, 3- and 4-hydroxyphenanthrene, 3-hydroxybenz(a)anthracene and 3-hydroxybenzo(a)pyrene. Int Arch Occup Environ Health 73:270–274
Heudorf U, Angerer J (2001a) Internal exposure to PAHs of children and adults living in homes with parquet flooring containing high levels of PAHs in the parquet glue. Int Arch Occup Environ Health 74:91–101
Heudorf U, Angerer J (2001b) Urinary monohydroxylated phenanthrenes and hydroxypyrene—the effects of smoking habits and changes induced by smoking on monooxygenase-mediated metabolism. Int Arch Occup Environ Health 74:177–183
IARC (International Agency for Research on Cancer) (1983) Benzo[a]pyrenr. In: IARC monographs on the evaluation of carcinogenic risk of chemicals to humans. Polycyclic aromatic compounds, part 1, chemical, environmental and experimental data, vol 32. Lyon
Jongeneelen FJ, Anzion RB, Scheepers PT, Bos RP, Henderson PT, Nijenhuis EH, Veenstra SJ, Brouns RM, Winkes A (1988a) 1-Hydroxypyrene in urine as a biological indicator of exposure to polycyclic aromatic hydrocarbons in several work environments. Ann Occup Hyg 32:35–43
Jongeneelen FJ, Scheepers PT, Groenendijk A, Van Aerts LA, Anzion RB, Bos RP, Veenstra SJ (1988b) Airborne concentrations, skin contamination, and urinary metabolite excretion of polycyclic aromatic hydrocarbons among paving workers exposed to coal tar derived road tars. Am Ind Hyg Assoc J 49:600–607
Kao J, Patterson FK, Hall J (1985) Skin penetration and metabolism of topically applied chemicals in six mammalian species, including man: an in vitro study with benzo[a]pyrene and testosterone. Toxicol Appl Pharmacol 81:502–516
Lafontaine M, Payan JP, Delsaut P, Morele Y (2000) Polycyclic aromatic hydrocarbon exposure in an artificial shooting target factory: assessment of 1-hydroxypyrene urinary excretion as a biological indicator of exposure. Ann Occup Hyg 44:89–100
Lafontaine M, Gendre C, Morele Y, Laffitte-Rigaud G (2002) Excretion of urinary 1-hydroxypyrene in relation to the penetration routes of polycyclic aromatic hydrocarbons. Polycycl Aromat Compd 22:579–588
Lafontaine M, Gendre C, Delsaut P et al (2004) Urinary 3-hydroxybenzo[a]pyrene as a biomarker of exposure to polycyclic aromatic hydrocarbons: an approach for determining a biological limit value. Polycycl Aromat Compd 24:441–450
Moody RP, Nadeau B, Chu I (1995) In vivo and in vitro dermal absorption of benzo[a]pyrene in rat, guinea pig, human and tissue-cultured skin. J Dermatol Sci 9:48–58
Ng KM, Chu I, Bronaugh RL, Franklin CA, Somers DA (1992) Percutaneous absorption and metabolism of pyrene, benzo[a]pyrene, and di (2-ethylhexyl) phthalate: comparison of in vitro and in vivo results in the hairless guinea pig. Toxicol Appl Pharmacol 115:216–223
Payan JP, Lafontaine M, Simon P, Marquet F, Gendre C, Beydon D, Ferrari E (2008) In vivo and in vitro percutaneous absorption of [(14)C]pyrene in Sprague Dawley male rats: skin reservoir effect and consequence on urinary 1-OH pyrene excretion. Arch Toxicol 82:739–747
Quinlan R, Kowalczyk G, Gardiner K, Calvert IA, Hale K, Walton ST (1995) Polycyclic aromatic hydrocarbon exposure in coal liquefaction workers: the value of urinary 1-hydroxypyrene excretion in the development of occupational hygiene control strategies. Ann Occup Hyg 39:329–346
Ritschel WA (1980) Handbook of basic Pharmacokinetics. Hamilton, IL
Simon P, Lafontaine M, Delsaut P, Morele Y, Nicot T (2000) Trace determination of urinary 3-hydroxybenzo[a]pyrene by automated column-switching high-performance liquid chromatography. J Chromatogr B Biomed Sci Appl 748:337–348
Van Rooij JG, Bodelier-Bade MM, De Looff AJ, Dijkmans AP, Jongeneelen FJ (1992) Dermal exposure to polycyclic aromatic hydrocarbons among primary aluminium workers. Med Lav 83:519–529
Van Rooij JG, Bodelier-Bade MM, Jongeneelen FJ (1993) Estimation of individual dermal and respiratory uptake of polycyclic aromatic hydrocarbons in 12 coke oven workers. Br J Ind Med 50:623–632
Acknowledgments
We would like to thank P. Maxant and P. Sibille for their help in conducting this study and M. C. Grandclaude for her technical assistance. This study was part of the “Evaluation and prediction of dermal absorption of toxic chemicals” project (QLRT-2000-00196), supported by the 5th Framework Program of the European Commission.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Payan, JP., Lafontaine, M., Simon, P. et al. 3-Hydroxybenzo(a)pyrene as a biomarker of dermal exposure to benzo(a)pyrene. Arch Toxicol 83, 873–883 (2009). https://doi.org/10.1007/s00204-009-0440-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00204-009-0440-0