
Abstract
Summary
Osteoporotic hip fracture, mostly induced in falls among the elderly, is a major health burden over the world. The impact force applied to the hip is an important factor in determining the risk of hip fracture. However, biomechanical researches have yielded conflicting conclusions about whether the fall-induced impact force can be accurately predicted by the available models. It also has been debated whether or not the effect of impact force has been considered appropriately in hip fracture risk assessment tools. This study aimed to provide a state-of-the-art review of the available methods for predicting the impact force, investigate their strengths/limitations, and suggest further improvements in modeling of human body falling.
Methods
We divided the effective parameters on impact force to two categories: (1) the parameters that can be determined subject-specifically and (2) the parameters that may significantly vary from fall to fall for an individual and cannot be considered subject-specifically.
Results
The parameters in the first category can be investigated in human body fall experiments. Video capture of real-life falls was reported as a valuable method to investigate the parameters in the second category that significantly affect the impact force and cannot be determined in human body fall experiments.
Conclusions
The analysis of the gathered data revealed that there is a need to develop modified biomechanical models for more accurate prediction of the impact force and appropriately adopt them in hip fracture risk assessment tools in order to achieve a better precision in identifying high-risk patients.

Impact force to the hip induced in sideways falls is affected by many parameters and may remarkably vary from subject to subject
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Most injuries (87% of fractures) to older adults result from falls [1, 2]. Hip fracture is one of the most common consequences of falls [3, 4], as the applied force to the femur can easily exceed the bone strength. Hip fracture has become a major health problem over the world [5] as it is associated with significant morbidity, disability, reduced quality of life, and mortality [6]. It is also a substantial source of long-term institutionalization [7] and health care expenditure [8]. Statistical studies showed that falls from sideways are the main cause of hip fractures (63–69% in fall-related fractures) [5, 9]. Therefore, prediction of sideways fall-induced impact force to the femur has received much attention in the last two decades. There are two main approaches to predict the impact force for hip fracture risk assessment purposes: (a) mathematical modeling of human body falling and (b) empirical functions. In mathematical modeling, human body dynamic models are proposed to predict the kinematics of body falling, determine the impact velocity, and simulate the interaction between the body and the ground during the impact. Experimentally derived empirical functions are also proposed to predict the impact force based on the body parameters, mostly body weight, body height, and trochanteric soft tissue thickness (STT). Although remarkable efforts have been conducted to propose models for predicting the impact force, their accuracy is still questionable. The limited accuracy is due to inadequate consideration of joint reactions during the fall, ignoring the pre-impact movements of body segments, insufficient consideration of the effect of subject-specific fall type, fall direction (forward, backward, and sideways), and contact site on the magnitude of the impact force, and neglecting how the cause of fall (slip, trip, or uneven floor) and the initial conditions (fall from standing height, low stools, stairs, etc.) affect the kinematics of body segments during the fall. A considerable number of simplifications and assumptions have also been used in modeling, including limited number of links for analysis of the human body falling and insufficient number of degrees of freedom for simulating the impact phase by vibrational models.
Not only the available methods have limitations in predicting the impact force, impact force itself is not properly considered as a risk factor in hip fracture risk assessment tools. For example, the effect of impact force is completely ignored in areal bone mineral density (BMD) estimation from dual X-ray absorptiometry (DXA), volumetric BMD from quantitative computed tomography (QCT), and hip structural analysis (HSA). FRAX® (fracture risk assessment tool) considers the body weight and body height as rough representatives of the impact force. Nevertheless, the impact force is not explicitly calculated in FRAX. Only in 2D and 3D finite element analyses (FEA) of femur, the impact force is directly taken into account for assessment of hip fracture risk, although with a limited accuracy. This inadequate consideration may be due to the limitations of the available models for predicting impact force and insufficient understanding of the effect of real-life fall-induced impact force on hip fracture risk. Therefore, in spite of the importance of the impact force, it seems it has not received enough attention. This study aims to provide a review on researches invested on predicting the fall-induced impact force to (1) reveal major challenges and limitations in modeling of human body falling and characterization of the interaction between the body and the ground during the impact, (2) shed lights to resolve the current issues and clarify the missing parameters in the available models, and (3) provide suggestions for future research studies. To this end, the section “Effect of impact force on hip fracture risk” investigates the range of the fall-induced impact force and the range of the force that can cause a hip fracture. It also presents the potential reasons why impact force has not been appropriately considered as a risk factor in hip fracture risk assessment tools. The section “How much impact force differs from subject to subject” surveys the parameters that affect the impact force and evaluates the necessity for subject-specific prediction of impact force. The section “Available models to predict the impact force” provides a review on available models for predicting the impact force and addresses their strengths/limitations. The section “Missing/neglected variables in available models for predicting fall-induced impact force” investigates the missing parameters in the available models and provides recommendations for future research studies.
Effect of impact force on hip fracture risk
From the biomechanical point of view, the fracture risk depends on the bone strength and the applied force. The fracture risk is measured by load to strength ratio (LSR) [10, 11] as the following:
where the bone strength is the maximum force that the bone can withstand without fracture and the applied load is the fall-induced impact force to the hip. If the applied load is greater than the bone strength (LSR>1), the bone will fracture. In this criterion, the applied impact force to the femur is one of the two main determinants of fracture risk [12], and thus, many researches have been conducted to determine the range of the fall-induced impact force as well as the range of the force that can cause a hip fracture. These two parameters are investigated in the following sections.
Range of the fall-induced impact force to the hip
Fall experiments and dynamic models are the two main approaches that have been used to determine the range of the fall-induced impact force. Experimental studies have implemented three methods: (1) voluntary natural fall from standing height by young adults, (2) pelvis-release experiments to measure the damping properties of hip soft tissues and predict the impact force, and (3) fall from a kneeling position to measure the impact force in a low-severity fall. Apart from the experiments, dynamic models have been developed to determine the fall-induced impact force. First, the kinematics of body segments during the fall are simulated by the dynamic models to determine the hip impact velocity. The velocity is then used in an impact model to simulate the interaction between the body and the ground and determine the applied force to the hip. Table 1 provides a review on the studies conducted to determine the range of hip impact velocity and force in a fall.
Based on the benchmark works, conducted by Robinovitch and his colleagues, the average pelvis impact velocity in an unexpected sideways fall from standing height is 3.0 m/s with a standard deviation of 1.0 m/s [23], although it can be higher for some persons, even up to approximately 5 m/s [16]. There is a positive correlation between the impact velocity and impact force during lateral pelvic impact [13]. The peak impact force in a fall from standing height is ranged from 4050 to 6420 N [15]. It may be increased up to 8600 N for an average individual in a fall from a pelvis height of 0.7 m [13]. However, in a low-severity fall, the impact velocity is approximately 1.0 m/s and the impact force can vary from 1 to 2.5 kN [24]. Generally, impact velocity of 3.0 m/s (SD = 1) [23] and femoral force of 5200 N [13] are the mean values in an unexpected fall from sideways for an average individual.
There are many uncertainties in an unexpected real fall that can significantly affect the magnitude of the impact force, including fall direction (forward, backward, or sideways), initial conditions of fall, impact site (anterior/posterior side of the femur or greater trochanter), body stiffness, stiffness of the floor (hard wood or carpeted), and pre-impact movements to arrest the fall [21,22,23, 28]. Therefore, the range of the impact velocity and impact force may vary from subject to subject and even for one subject from fall to fall. For example, any attempt to recover balance, which is common among young adults, may remarkably affect the impact force. Feldman et al. [23] showed that even unsuccessful attempts to recover balance by stepping may affect the magnitude of the hip impact force. Even holding an object [29] may affect the fall kinematics and reduce the applied force to the hip. Since people may experience falls in different environments, they may react differently and thus the impact force will be different. Therefore, if not impossible, it is very difficult to integrate all aspects of an unexpected real fall in modeling or even experiments. Hence, the listed results in Table 1 provide a fair estimation of the force that a subject may experience in a fall from standing height.
Range of the force that can cause a fracture in a femur
Apart from the studies conducted to find the range of the fall-induced impact force, tremendous efforts have been devoted to determine the strength of the femur and evaluate whether or not the fall-induced impact force is sufficient to cause a hip fracture. Experimental tests and finite element analysis are the most common approaches in determining the femoral strength. Table 2 provides a review on the studies conducted to determine the femur strength and the range of the force that can cause a fracture in a femur.
The reviewed studies generally investigated the femoral strength in single-limb stance and fall loading configurations. It has been illustrated that the strength of femur is generally lower under fall loading conditions. From the biomechanical point of view, the potential reason is that a higher moment is applied to the femoral neck in the fall loading configuration, and thus, the fracture occurs under a lower force [37]. Across the listed studies that investigated the single-limb stance loading configuration, the median femoral strength was 7214 N. The average femoral strength under fall loading configuration was 3462 N with a standard deviation of 1520 N (ranged from 573 to 15,034 N) [66]. The structural capacity of the proximal femur is even sensitive to a slight variation in lateral versus posterolateral loading angle in a sideways fall, i.e., when the subject rolls forward/backward. Slightly rolling forward can increase the load required to fracture the femur [40]. Not only the loading configuration affects the femoral fracture force but sex is also an effective parameter on the bone strength. The femoral strength was reported to be lower in women than in men. For the studies that male and female data were separated, the strength of femur was 4027 ± 1464 N for men and 2771 ± 1136 N for women. Age is also an effective parameter in determining the strength of femur due to its direct correlation with BMD. For studies that reported age-specific values, the femoral strength was approximately 40% lower in older adults (2888 N for subjects with the mean age of 80.9 years vs. 4766 N for subjects with the mean age of 63.9 years). Loading rate is another effective parameter on the femur strength. Although there is still an ongoing discussion on how the femur strength is affected by the load rate [62], fracture force is generally reported to be greater at a higher load rate [38, 67, 68].
Figure 1 provides a summary of Tables 1 and 2 and compares the range of fall-induced impact force to the hip with the average femur strength. Concluded from Fig. 1, the median value of the femoral force in an unexpected fall from sideways for an average individual (5200 N) is well within or even beyond the range of the fracture force measured in experimental studies (3500 N). Therefore, an unexpected lateral fall to the hip has the potential of fracturing the femur, especially in the elderly. Accurate prediction of fall-induced impact force is thus of great significance in developing hip fracture risk assessment tools. However, most of the currently available tools in clinics ignore the effect of impact force or do not appropriately consider it. The following section investigates how the impact force is considered in clinical hip fracture risk assessment tools.

Box plot showing median, quartiles, and range of lateral fall-induced impact force to the hip in comparison with the median femur strength
Consideration of/neglecting the impact force in hip fracture risk assessment tools
Among the four dominant biomechanical variables affecting fracture risk, i.e., risk of fall, impact force, bone quality, and bone geometry [12], the first two variables are the difficult ones to be accommodated in assessment of fracture risk.
There are four fracture risk assessment tools currently used in clinical studies, i.e., BMD (T-score) determined from DXA, hip structural analysis (HSA), FRAX (fracture risk assessment tool), and finite element analysis. Bone densitometry based on hip DXA is now a well-established method in clinical centers for monitoring osteoporosis. It is referred to as the “gold standard” by WHO. However, bone quality is the only effective parameter in assessing hip fracture risk by T-score. It means if the bone quality is the same for two subjects who may experience different impact forces in falls from standing height because of the differences in their physical attributes, T-score predicts the same fracture risk for both. Therefore, this method does not take the effect of impact force into consideration for assessing the risk of hip fracture.
The HSA is constructed based on the principle that a line of pixel values across the bone is summed up in the projected DXA image [69]. Bone quality and bone geometry are the only effective parameters in HSA. Similar to the T-score estimation, HSA does not consider the effect of impact force in assessment of hip fracture risk.
FRAX integrates 12 clinical risk factors to assess the fracture risk for an individual, including age, sex, weight, height, previous fracture, parental hip fracture history, current smoking, glucocorticoids, rheumatoid arthritis, secondary osteoporosis, alcohol consumption, and femoral neck BMD [12, 70]. Although body weight and body height are two of the determinants of impact force and they are indeed included in FRAX, other effective parameters are neglected.
In the FE analysis, introduced to orthopedic biomechanics in 1970s [71], load/constraint conditions are applied to the model, constructed from DXA/QCT image, to calculate the strain and stress distribution in the proximal femur and assess the fracture risk. Compared to other clinical assessment tools, FE analysis considers the effect of impact force more appropriately and this is one of the potential reasons why its accuracy is more convincing [12]. However, many effective parameters are still neglected or not appropriately considered in calculating the impact force, including body segment anthropometric parameters, kinematics of body segments during the fall, nature and direction of the fall, initial conditions of the fall, body configuration before the impact, action of joints, energy absorption during the impact, etc.
It has been demonstrated [12] that in most of the clinical fracture risk assessment tools, bone quality and bone geometry have received much more attention than the impact force. Potential reasons are threefold: (1) difficulties in predicting the subject-specific fall scenario, (2) limitations of the available methods in predicting the impact force, and (3) insufficient investigation of the direct effect of real-life fall-induced impact force on hip fracture risk. In order to facilitate the appropriate consideration of impact force in hip fracture risk assessment tools, there is a need to modify the available impact force predictors. Before that, it should be well-understood what parameters affect the impact force and how much they differ from subject to subject. The following section evaluates the necessity for developing a subject-specific impact force predictor.
How much impact force differs from subject to subject
Robinovitch et al. [13] illustrated that the peak force in a lateral pelvis impact is a function of (1) impact velocity, (2) effective pelvis mass (i.e., the mass of the pelvis and connecting structures which contribute to the impact loads), and (3) effective pelvis stiffness (i.e., the in-series stiffness of the soft tissue–femur–pelvis complex). All these parameters are interestingly dependent on a complex combination of body parameters [27]. Changes in any of these three factors may significantly affect the magnitude of the applied force to the femur.
Impact velocity
Impact velocity has a positive correlation with body weight and body height. It indicates that heavier and taller subjects experience a higher impact velocity in a fall from standing height. Greater weight and height increases the initial potential energy, which is converted to the kinetic energy at the impact instant and increases the impact velocity and subsequently the impact force. The effects of weight and height on the impact force are even different between men and women. As a result of a biomechanical statistic [27], body weight has a greater effect on the impact force in men than in women. One of the potential reasons for this phenomenon is that the stiffness/damping properties of the body during the impact are differently associated with the STT in men and women. Heavy and tall men not only have thinner hip soft tissues than women, they generally have stiffer tissues [25]. It may be due to the difference in muscle/fat content between men and women (higher muscle content in men compared to women) [13, 72, 73]. Therefore, body anthropometric parameters may significantly affect the impact velocity and impact force.
Cause of fall, that is significantly different in individuals with different age and life style, can also remarkably affect the impact velocity and thus the magnitude of the force applied to the femur. Incorrect weight shifting is the most important cause of fall among the elderly [74] while the cause of fall may be different in younger adults. Differences in the cause of fall affect the initial conditions, i.e., trunk angle and gate velocity (e.g., falls from standing or during walking), and subsequently change the impact velocity. The cause of fall may also affect the duration of the fall that can limit the time for the individual to effectively break the fall with hands or knees. Even if two subjects experience a fall from the same initial conditions, they may react differently to decrease the severity of the fall, based on their physical abilities, age, and knowledge of effective pre-impact movement strategies. Therefore, impact velocity, as one of the most effective factors on the impact force, can significantly vary from subject to subject.
Effective mass during the impact
Apart from the impact velocity, effective mass, i.e., the mass of that part of the body that moves downwards and contributes to the impact load [13, 14], also changes the magnitude of the force applied to the femur. It is the summation of the effective masses of all body segments at the impact moment [14]. Greater effective mass increases the impact force. In determining the effective mass, the position and orientation of all body segments before the impact are considered in a mathematical model to correlate the vertical position of the hip with its vertical acceleration [75]. Body configuration at the impact instant can thus significantly affect the effective mass. For example, less vertical orientation of the trunk [76] and smaller flexion-extension knee angle (i.e., the angle between the shank and the thigh) [77] can decrease the effective mass and subsequently the impact force. Body segment anthropometric parameters, such as mass, mass center, and mass moment of inertia, are other determinants of the effective mass. Heavier and longer body segments, i.e., shank, thigh, and trunk, have more contribution to the total effective mass [78]. The overall body configuration is another effective factor. Generally, individuals with upside-down pear-shaped body configuration have a greater effective mass during the impact compared to individuals with pear-shaped body configuration [78]. Therefore, the effective mass may also remarkably vary from individual to individual.
Effective pelvis stiffness
The interaction between the body and the ground in the impact stage of a fall is a combination of hyperelastic behavior of the hip soft tissues, fat, skin, muscle, cartilage, and ligaments [79, 80] and visco-elasto-plastic response of the bone [67, 81]. This complex interaction has been mostly simulated by damped vibrational systems, composed of springs and dampers [13]. The spring-damper combination represents the stiffness and damping properties of the soft tissue–femur–pelvis complex that has a significant influence on the amount of absorbed energy during the impact. Table 3 provides a review on the studies that investigated the variation of body stiffness and absorbed energy among different individuals.
As shown in Table 3, body stiffness and damping coefficient remarkably varies among different individuals since it is affected by trochanteric soft tissue thickness (STT), BMI, body configuration at the impact instant, landing surface, condition of muscles (relaxed/contracted), etc. Among all parameters, body mass index, trochanteric soft tissue thickness, and muscle conditions are the most effective factors on the body stiffness during the impact. It has to be pointed out that the effective pelvis stiffness not only depends on the body parameters but also on the force-deflection and force-velocity properties of the pelvis and the ligaments connecting the pelvis to the trunk and thigh [13, 18]. Age [90] and sex [27] also affect the pelvis stiffness and subsequently the hip fracture risk (Fig. 2). For example, if a man and a woman in similar range of age with the same trochanteric soft tissue thickness and effective mass experience a lateral fall with the same impact velocity, the impact force for the male subject is generally higher than that for the female subject [25, 27]. It indicates that the amount of absorbed energy during the impact is affected by sex due in part to the differences in the muscle/fat content in the hip region. In addition to the mentioned parameters, floor surface may also change the magnitude of the impact force [89]. The floor can be hard wood or carpeted that affects the amount of absorbed energy during the impact, and thus, people with different life styles may experience different impact forces in falls on the hip.

Femoral fracture risk at various levels of BMI (kg/m2) for 50 men and 80 women (reproduced from [27] with permission). Fracture risk increases with decreased BMI (but with different trends in men and women) due to the lower capacity of hip soft tissues to absorb impact energy
Since the body stiffness is one of the most dominant parameters affecting the pelvis stiffness and subsequently the hip fracture risk, many studies have devoted to wearable protective pads [66, 91,92,93]. Hip protectors significantly contribute in attenuating the impact energy and may reduce the axial compressive force induced to the femur by 20% [94] and the peak pressure by 70% [95], especially for low BMI subjects who generally do not have thick trochanteric soft tissues. Research studies have thus shown that these pads can remarkably reduce the risk of fall-induced hip fracture.
In general, impact velocity, effective mass, and effective stiffness as determinants of the hip impact force are influenced by age, sex, body anthropometric parameters, body configuration at the impact instant, pre-impact movements, hip soft tissue thickness, and muscle conditions, and thus, the impact force significantly varies from subject to subjects. Since the impact force may remarkably affect the risk of hip fracture, accurate subject-specific prediction of impact force can be considered as of great significance in improving hip fracture risk assessment tools.
Available models to predict the impact force
The available models in the literature to simulate the body falling are generally composed of two parts: (a) a dynamic model to simulate the kinematics of body segments during the fall and (b) an impact model to simulate the interaction between the body and the ground. In this section, a review is provided on the available dynamic and impact models for simulating the body falling and their strength/weaknesses are investigated.
Human body dynamic models for simulating the fall
The purpose of dynamic models, presented in the literature, is to predict the hip impact velocity in a fall. The simplest yet effective biodynamic models for simulating the lateral fall are point-mass (Fig. 3a) and one-link single-degree of freedom (DoF) (Fig. 3b) models based on energy conservation [14]. The hip impact velocity is calculated by equating the available potential energy at the onset of the fall to the potential and kinetic energy at the impact moment. Assuming the location of the hip at the middle of the body, the hip impact velocity by the point-mass and the one-link model are respectively represented by Eqs. (2) and (3), where h cg is the height of the centre of gravity of the body.

a Point-mass, b single-link, c vertical trunk, and d 45° trunk model for simulating the body falling from standing height [14]. e Projection of three-link human body dynamic model on sagittal and coronal plane (reproduced from [77] with permission). f Right posterolateral view showing the 11-link dynamic model to simulate sideways body falling (reproduced from [99] with permission)
Both models have a single DOF and the only difference is that in the point-mass model the mass falls vertically while the one-link model includes the effect of rotational energy. Equations (2) and (3) show that by a slight change in the assumptions, the resulted velocities are considerably different.
A two-link model has also been proposed to represent lower extremity (leg segment) and upper extremity (trunk), interconnected by a hinge at the hip joint [14]. The trunk orientation may vary prior to impact, and thus, two different configurations are considered for the trunk angle, i.e., vertical (Fig. 3c) and 45° (Fig. 3d). The hip impact velocity in vertical and 45° configuration of the trunk is respectively represented by Eqs. (4) and (5), where h is the total body height.
Inspired by a pioneering work performed by Kroonenberg et al. [14], a three-link model is also proposed [77, 78, 96] to simulate the motion of shank, thigh, and trunk in a fall from sideways (Fig. 3e). In this model, the body is represented as an open chain of three links connected by frictionless hinges [14]. This model has two rotational degrees of freedom for the hip, i.e., flexion/extension and abduction/adduction, one flexion/extension degree of freedom for the knee, and an abduction/adduction degree of freedom for the ankle. Rotational springs are incorporated in the hinges to account for muscle forces acting on the joints. Required body segment anthropometric parameters, including length, mass, mass center, and mass moment of inertia, are derived from the whole-body DXA image of the subject [77, 97] and are assigned to the corresponding links. Inverse-dynamic approach was used to take the effect of hip and knee joint torques into account [98]. Subject-specific consideration of body segment anthropometric parameters and joint torques improved the accuracy of the model in predicting the hip impact velocity [77, 78].
More complex models have also been introduced to simulate the fall from sideways and determine the impact velocity. Lo and Ashton-Miller [99] proposed an 11-link model, including shanks, thighs, pelvis, trunk, head, upper arms, and forearms, to simulate the lateral fall from standing height (Fig. 3f). The rigid segments were connected by frictionless hinges (knees, neck, and elbows), universal (waist and shoulder), and ball-and-socket joints (hips). The rotational joint torques were simulated by a pair of agonist and antagonist joint muscle torque actuators. Table 4 shows the range of error for available models in predicting the hip impact velocity in a fall from sideways.
Comparison between the error of different models in Table 4 shows that increasing the complexity of the model does not necessarily result in improved predictions. For example, the accuracy of the two-link model (with the 45° jackknife configuration) in predicting the impact velocity is greater than that of the three-link model (A) [14]. Therefore, increasing the number of links without a proper consideration of the joint torques may even increase the uncertainties of the model and thus reduces the accuracy of predictions. The error of the three-link model (C) (3–10%) [78] is lower than that of three-link model (A) and (B) that indicates the significance of subject-specific consideration of effective parameters in modeling. However, the three-link model (C) is validated by only three subjects due to the difficult nature of the performed fall experiments. Further validations for this model can improve its application in clinical studies. The error of the 11-link model that simulates the kinematics of all body segments [99] is 2–27% in predicting the hip impact velocity, which seems to be the most accurate model among the available ones. Therefore, the number of links and consideration of joint torques and subject-specific body segment anthropometric parameters are the factors that together can effectively improve the ability of the model in predicting the hip impact velocity in a fall. Although increasing the number of links with proper consideration of joint torques improves the accuracy of predictions, it also increases the complexity of the model and subsequently the computational time and storage. Since the models are being used in clinical applications, a combination of model complexity, model accuracy, computational efficiency, and ease of adopting in clinics should be considered to select an appropriate dynamic model for hip fracture risk assessment tools.
Models to simulate the impact stage of a fall and determine the impact force
A benchmark work by Robinovitch et al. [13] simulated the interaction between the body and the ground by a single-degree of freedom damped vibrational system as shown in Fig. 4a. m is the effective mass and K and b are, respectively, body stiffness and damping properties, that are determined from force-deflection and force-velocity properties of the trochanteric soft tissues, muscles of the pelvis, abdomen, lower legs, and the skeletal components [13]. This is the simplest effective model capable of simulating the oscillatory response of the body during the impact stage of a fall.

a Mass-spring model, b Voigt support model, c Maxwell support model, and d standard linear solid support model for simulating the impact stage of a fall. e Trunk-straight and trunk-flexed configuration in pelvis-release experiments (reproduced from [18] with permission)
Robinovitch and colleagues also proposed three nonlinear single-degree of freedom (DOF) shock-absorbing systems for simulating the impact stage of a fall [19], i.e., Voigt support model (Fig. 4b), Maxwell support model (Fig. 4c), and standard linear solid support model (Fig. 4d). Results showed that the Maxwell and standard linear solid support models are better predictors of the peak impact force. Trunk-straight and trunk-flexed configurations of the hip during the impact were also simulated by a two DOF model (Fig. 4e) in order to determine the distribution of contact force to the hip [18]. This model considered both compressive and flexural motion of the body during the impact where both compressive stiffness and damping coefficients were significantly greater than flexural ones. Results showed that with the flexed trunk, the stiffness and the applied force to the hip are significantly increased. The increase in the stiffness is due to the changes in the geometrical relations between femur, pelvis, and supporting ligaments [18]. Also, in the trunk-upright configuration, a larger trunk mass is located closer to the hip that remarkably increases the effective mass during the fall [18]. Although the implemented damper in the vibrational models is to take the effect of damped energy into account, experimental studies showed that the proximal femur region absorbs the vast majority of the impact energy, and only 15% of the total impact force is applied to structures surrounding the hip [18].
Force-deflection properties of the pelvis are also measured in vivo by Robinovitch et al. [13, 18] and Laing et al. [24] to evaluate whether characterization of nonlinearities in stiffness affects the accuracy of a mass-spring model in predicting the peak impact force. Results demonstrated that the force-deflection is slightly nonlinear (limited to force below 300 N), characterized by increasing stiffness as deflection increases. However, for loads beyond 300 N stiffness remained constant.
The characteristics of the introduced impact models are determined from pelvis-release experiments with living humans [13, 17, 18, 24, 25, 28, 89, 90, 94, 95], cadaver-based studies [15], or surrogate human pelvis-pendulum-foam soft tissue [19, 66]. Each approach has its own advantages and limitations. The chief strength of the cadaver-based studies is that the cadaver can be subjected to the impact force occurring in real-life falls without any limitation or simplification in performing the experiments. However, the response of the cadaver may considerably differ from that of the living human, due to the post-mortem changes in the skin and fat in the hip region, lack of active/passive joint muscle actions, and lack of cognition to avoid the fall by real-life pre-impact movements. Furthermore, kinematic constraints are required in order to mimic a real-life fall by a cadaver that will affect the dynamic response [18]. The main weakness of using living humans is that the experiments can only be performed at safe loading levels, which is approximately 250 N [18]. The potential issue is that trochanteric soft tissues show nonlinear force-deflection and force-velocity properties only at low force region (0–300 N) [24] while the response of body at the low force regime is not the representative of that occurring in an actual fall [18]. Furthermore, experiments are only conducted on young adults and the results may not be interpretable for the elderly. For experiments on foam as a surrogate of human soft tissues, again results may significantly differ from what is happening in real-life falls, due to the remarkable differences between the structure of foam and human soft tissues. The other limitation for pendulum experiments with femur covered by foam is that it only simulates the effect of trochanteric soft tissues in attenuating the impact energy, while in a real-life fall, energy absorption during the impact is a complicated mechanism where other structures also contribute, including pelvis, muscle and ligaments that connect the pelvis to the trunk and lower limbs, and femur [18].
In addition to the aforementioned models, Lo and Ashton-Miller proposed formulas (Eqs. (6) and (7)) to separately calculate the stiffness and damping of soft tissues and boney parts for body segments that could potentially impact the ground, such as heels, knees, greater trochanters, pelvis, shoulders, thorax, elbows, wrists, and head [99, 100].
Although specific determination of the stiffness and damping properties of each body part during the impact can remarkably increase the accuracy of predictions, these properties are not the same for all subjects. As an instance, the stiffness and damping of the anterior and posterior surfaces of the pelvis, thorax, and shoulders can considerably differ between overweight and underweight subjects and also between men and women [27], while Eqs. (6) and (7) consider the same stiffness and damping for all individuals.
Apart from the introduced vibrational models to simulate the impact stage of a fall, two empirical equations are also proposed to predict the peak impact force in a lateral fall. Equation (8) is proposed by Kroonenberg et al. [14], where \( n= V\frac{\sqrt{\left(\frac{71000}{\mathrm{EM}}\right)}}{9.81} \), \( V=2.72\sqrt{h} \), ω = π − tan−1 n, m e is the effective mass (0.35 of body weight), and V is the impact velocity.
Equation (9) is obtained by Robinovitch et al. [13] and extrapolated by Yoshikawa et al. [101], where h is body height in centimeters and W is body weight in Newton.
The effective parameters in both empirical equations are body weight and body height. Ignoring other effective parameters, such as trochanteric soft tissue thickness, influences the accuracy of the equations in predicting the peak impact force [77].
A method is also proposed by Robinovitch et al. [15] to consider the effect of hip soft tissues in attenuating the force applied to the greater trochanter. They suggested that for each millimeter increase in tissue thickness, peak force at the greater trochanter level decreases by 71 N. In most FE analyses of the proximal femur, a combination of Kroonenberg and Robinovitch method is implemented to predict the force applied to the femur in a sideways fall as follows:
Although it is a simplification to combine Eq. 8 with Robinovitch method, as in study of Robinovitch et al. [15], the difference between the forces at soft tissue surface and at the greater trochanter was not reported to be 71 N/mm; however, Eq. 10 is the most common method for determining the fall-induced impact force in hip fracture risk assessment tools. Results of hip fracture studies, particularly FE analyses, proved the effectiveness of this formula in estimating the fall-induced impact force to the hip.
Furthermore, a subject-specific damped vibrational model has been proposed [77] to simulate the interaction between the body and the ground. The stiffness and damping properties of the impact model are derived subject-specifically considering the gender of the individual, as well as the thickness of trochanteric soft tissues [27]. However, several simplifications are still used in modeling, including the limited number of degrees of freedom and neglecting the risk of fall and pre-impact movement strategies. Whole-body DXA image is also needed by this model that may affect its applicability in clinics.
Missing/neglected variables in available models for predicting fall-induced impact force
A fall has three phases: (1) the instability phase, (2) the descent phase, and (3) the impact phase [17, 102]. There are many variables in each of these phases that may significantly change the kinematics of the fall and subsequently the impact force. In this section, missing parameters in currently available models for predicting the impact force are investigated and suggestions for future studies are provided.
Instability phase
Instability phase is directly affected by the cause of fall. Most of the models are focused on determining the mechanics of fall without considering how and why the fall occurs. The common causes of falls among the elderly are incorrect weight shifting (41%), trip or stumble (21%), hit or bump (11%), loss of support (11%), collapse (11%), and slipping (3%) [74].
Elderly people mostly initiate the fall because of incorrect transfer or shifting of body weight. As an instance, elderly with walkers who are standing and want to initiate a turn by rotating the walker are likely to lose their balance as the center of gravity is moved outside the base of support [74]. Trip and stumble are mostly attributed to foot catching on the ground and difficulty in raising the foot [74]. Collisions with environmental objects and being pushed or pulled by another person are the most common causes of falls by hit or bump [74]. The cause of fall affects the initial conditions of the faller, the direction of the fall, i.e., sideways, forward, and backward, the kinematics of body segments during descent phase, possibility of using pre-impact movement strategies, and thus the magnitude of the impact force. As an instance, the possibility of stepping, squatting, forward walking, sitting down, and use of knees to break the fall is different in falls from different directions. Also, a fall due to trip, stumble, or slipping may cause a greater impact force compared to a fall due to incorrect weight shifting as the initial velocity at the moment of loss of balance is greater and the time to effectively arrest the fall is shorter. Common activities at the time of fall initiation, i.e., walking forward, standing quietly, sitting down, and initiation of walking [74], and gate speed also affect the instability phase. It has been demonstrated that slips and faints lead to forward falls at fast gate speed. However, at lower gate speed, slips and faints result in sideways falls with impact on the hip, suggesting a greater risk for hip fracture [103]. Not only the cause of fall varies among different subjects due to the differences in the life style and thus environmental hazards but also one individual may experience falls with different initial conditions. Therefore, if not impossible, it is very difficult to consider the subject-specific cause of fall for hip fracture risk assessment purposes. That is the potential reason why the cause of fall is totally neglected in hip fracture risk assessment tools. Determining the age-based most frequent initial conditions using database of video-captured falls [74] may be implementable for the dynamic models to predict the impact force for a subject with a specific age. Another reasonable way is to consider the most common cause of fall among the elderly (incorrect weight shifting [74]) and extract the corresponding initial conditions to be used for prediction of the impact force in hip fracture risk assessment tools. Also, an investigation can be conducted to find the most dangerous and sever cause of fall among the elderly to be adopted in impact force predictions. So far, results of typical falls of young adults on a thick foam mattress have been used for determining the initial conditions of a fall from sideways [14, 16, 23]. However, findings of video capture of the circumstances of falls in the elderly people [74] can be more useful in extracting the initial conditions of a real-life fall. Improving estimation of the initial conditions based on the most frequent cause of fall may increase the accuracy of predicted impact force and hip fracture risk.
Descent phase
Descent phase is between the instant of instability and the impact moment. The most important parameters in this phase that change the magnitude of the impact force are the action of joints and the use of body segments to arrest the fall, i.e., pre-impact movement strategies. Rotational springs [14] and time-dependent functions [78, 98] have been proposed to be accounted for the action of hip and knee during descent. However, one of the criticisms of the currently available methods is that the action of joints is not considered subject-specifically while joint actions may significantly vary from subject to subject. Sedentary individuals may less properly use their joints to decrease the severity of the fall compared to athletes. The joints action during the descent phase may also be culture-dependent. In many Asian countries, people frequently adopt floor sitting in their daily living activities [104, 105], and thus, they may be more experienced in effectively using their body segments to control their balance by applying appropriate torques in their joints. This experience may help them to more appropriately react during the descent phase. The age is another effective parameter, i.e., younger subjects may be able to more properly use their joints to decrease the severity of the fall [23].
Pre-impact movements can also remarkably influence the hip impact force. Although any fall from standing height can potentially lead to a hip fracture, only less than 2% of falls in older adults result in hip fracture [106], suggesting that protective responses can effectively reduce the severity of the fall and facilitate safe landing. Breaking the fall using outstretched hands and stepping are the most common strategies to reduce the impact force in young adults [23, 107]. These strategies can be more effectively implemented in sideways and forward falls [21, 100, 108, 109]. Impacting with knees [23], forward/backward rotation [21], squatting [22], eccentric contraction of lower extremity muscles [20], and knee extension during the final stage of descent [20] are other strategies to reduce the severity of the fall. It has been demonstrated that the hip impact force can be reduced by 56% if the subject uses the knee, hip, and spine rotations to arrest a lateral fall [99]. The reasons for this force reduction include distribution of the impact over a large body area and allowing more time for dissipation of the impact energy [99]. Experimental studies showed that martial arts, such as changing the fall into a rolling movement, can also reduce the hip impact force by 27 – 30% [76]. Holding an object to break the fall is another common activity that may significantly change the kinematics of fall [29] and subsequently reduce the applied force to the hip. Not only the nature of the protective responses affects the magnitude of the impact force but reaction time also influences their effectiveness. Increase in reaction time among the elderly may explain why many hip fractures occur among the older adults but few occur among younger people [107]. Table 5 provides a review on how pre-impact movements can change the magnitude of the impact force.
Although using body segments to break the fall is quite common as an inherent activity, pre-impact movement strategies have not been appropriately considered in available models for predicting the impact force. Concluded from Table 5, the action of an individual to arrest the fall may significantly differ from fall to fall based on many parameters, including the cause and initial conditions of fall that affect the duration of the descent phase, environmental parameters such as the darkness of the room that affects the implementation of the pre-impact movement strategies, subject’s physical ability, subject’s knowledge of pre-impact movement strategies, and the level of cognition of the faller during the descent phase. Therefore, it is impossible to consider the subject-specific pre-impact movements in dynamic models for determining the impact force. Again, the applicable method is to determine the most frequent reaction of the elderly during the descent phase to be considered in modeling. As initiated by Choi, Wakeling, and Robinovitch [116], the valuable recorded videos of real-life falls [74] can be used to identify common pre-impact movements to arrest the fall. Then, mathematical modeling of the pre-impact movements can be added to the impact force predictors for more reliable hip fracture risk assessment. Although hip fracture risk assessment tools are being used in clinics for individuals with varying range of age, the elderly are mostly prone to hip fracture due to the higher risk of fall, lower chance to effectively break the fall, and lower BMD. It may help explain why this study recommends using the elderly database for improving the impact force predictors.
From Table 5, not only martial art fall techniques can substantially reduce the impact force but also learning them may reduce the fear of falling that can result in prevention of falls. Surprisingly, learning martial art fall techniques is achievable in a very short time [113], even for the elderly people [114]. It has been demonstrated that older individuals can learn the basics of protective fall techniques within five weekly training sessions [114]. Nevertheless, instructing/learning fall techniques has not received much attention since its importance has not been emphasized. Future studies can invest on introducing new martial art fall techniques and propose guidelines for vastly implementing them among the elderly.
Impact phase
The last phase in a human body falling is when the hip impacts the ground. Fall direction that affects the boundary conditions of the proximal femur in the impact phase is an important parameter in simulating the proximal femur under fall-induced impact force. As an instance, in an impact with the lateral aspect of the hip, the force is applied to the greater trochanter while in a forward/backward fall the force is applied to the anterior/posterior aspect of the femur. Evidence showed that the impact during the fall to the sides, as opposed to the anterior/posterior aspect of the pelvis, substantially increases the risk for hip fracture [21]. Surprisingly, more than 60% of hip fractures are caused by sideways falls [5, 9], although the number of forward falls is three times that of lateral falls [1, 117]. The magnitude of the impact force is also influenced by the impact site. Potential reasons are the difference in the thickness of soft tissues overlying the hip in lateral, anterior, and posterior aspects of the hip and the difference in boundary conditions of the femur during the impact. Other effective parameters in the impact phase are the condition of muscles (relaxed/contracted), the portion of muscles and ligaments that contribute to the impact which is depended on the landing surface, abdominal and thoracic viscera, flexural deformation of the spine, and muscular connections between the trunk and the thigh [18]. The hardness of floor is also an effective parameter in the impact stage. Falling on a hard floor and a carpet does not lead to a same impact force. Again, it is not applicable to consider the impact site, muscle conditions, and floor hardness, subject-specifically, as these parameters are not constant for an individual. Therefore, lateral fall on a hard floor as the most sever scenario can be considered in impact force predictors. Also, the structure of muscles and ligaments peripheral to the hip and the joint torques that the individual applies during the impact is very complex to be taken subject-specifically into account for determining the impact force. There is a controversy between the effect of muscle conditions and pre-impact movements to reduce the severity of the fall. Although results of fall experiments have shown that impact with relaxed muscle will cause a safer landing [13, 17], any reaction in the lower extremity to arrest the fall may contract the muscles peripheral to the hip. Therefore, a comprehensive research is in need to determine how the muscle conditions and pre-impact movements should compromise to reduce the impact force.
One of the criticisms of the available models in predicting the impact force is that only the thickness of hip soft tissues has been considered for determining the attenuated impact energy. Studies on impact stage of human body falling have shown that a complex combination of interdependent body parameters can also influence the attenuated energy, including the fat and muscle content, age- and sex-related properties of soft tissues, flexural deformation of the spine, connection between trunk and lower limb, muscle conditions (relaxed/contracted), and landing surface [13, 15, 18, 24, 27, 78, 80, 90]. Therefore, future studies are still in need to determine the subject-specific stiffness/damping properties of the body for accurate prediction of fall-induced impact force.
Furthermore, research studies have mostly been focused on determining the peak impact force applied to the femur in a sideways fall. Since our understanding of the visco-elasto-plastic properties of the bone has recently been improved [38, 67, 68, 81, 118,119,120], prediction of the impact force time history may significantly improve the accuracy of future FE models in hip fracture risk assessment. Although considerable amount of studies have devoted to determine the strain-dependent properties of bone, these properties have not been adequately implemented in hip fracture risk assessment tools. Predicting the time history of impact force is much more helpful when the strain-dependent bone failure material properties are well investigated.
Conclusions
Sideways fall-induced impact force is one of the important determinants of hip fracture risk. Nevertheless, the available methods have limitations in predicting the impact force. These limitations are mostly due to the great number of uncertainties in simulating an unexpected real fall, including fall direction (forward, backward, or sideways), initial conditions of fall, impact site (anterior/posterior side of the femur or greater trochanter), body stiffness, stiffness of the floor (hard wood or carpeted), and pre-impact movements to arrest the fall. Not only the available models have limitations in considering all these parameters for simulating the fall and predicting the impact force, impact force itself is not appropriately considered as a risk factor in hip fracture risk assessment tools. This study reviewed the researches that investigated the range of impact force in a sideways fall and the range of femoral fracture force. Our review showed that the median value of the femoral force in an unexpected fall from sideways for an average individual (5200 N) is well within or even beyond the range of the femoral fracture force measured in experimental studies (3500 N). Therefore, accurate prediction of fall-induced impact force is of great significance in developing hip fracture risk assessment tools, although it has not received as much attention as the bone strength did.
The mostly used formulas for predicting the impact force only consider body weight, body height, and hip soft tissues. However, there are many parameters that can be considered in modeling of human body falling to improve prediction of the impact force. This review divided these parameters to two categories: (1) the parameters that can be determined subject-specifically and (2) the parameters that may significantly differ from fall to fall for an individual and cannot be considered subject-specifically.
Body segment anthropometric parameters and body stiffness/damping properties are the effective factors that can be taken into account subject-specifically. Researches have been conducted to determine the anthropometric parameters from clinical images with an appropriate accuracy. Also, many studies have been devoted to investigate body stiffness/damping properties from experimentations. However, we conclude that accurate subject-specific determination of stiffness/damping properties is complex since they are affected by many parameters, including fall direction, condition of muscles (relaxed/contracted), landing surface and the portion of muscles and ligaments that contribute to the impact, abdominal and thoracic viscera, and flexural deformation of the spine. So far, trochanteric soft tissue thickness has been considered as a determinant of the attenuated impact force while other factors can also remarkably affect the impact scenario. This review concludes that more research is required on this topic. Future studies are in need to investigate how sex affects the attenuated force per each millimeter of hip soft tissues, how the portion of fat/muscle content affects the attenuated force, how to take the flexural deformation of spine into account, and how the landing surface and the portion of muscles that contribute to the impact can be considered in determining the impact force.
Pre-impact movements to arrest the fall as well as cause and initial conditions of fall are the parameters that cannot be considered subject-specifically as they may vary from fall to fall for an individual. These parameters significantly affect the kinematics of fall and subsequently the magnitude of the impact force. The lack of information about the complicated effect of cause/initial conditions of fall and pre-impact movements on the magnitude of the impact force is due, in part, to the limitations in performing real-life fall experiments because of the ethical and safety reasons. Therefore, this study suggested using collected database of real-life falls to extract these parameters. As initiated by Robinovitch et al. [74], video-captured falls, experienced by the elderly at long-term care facilities, can be used to determine the most frequent causes of falls. Recorded videos can also be analyzed to extract the common initial conditions of falls and the frequent pre-impact movements to arrest the fall. Results of analyses can then be implemented in human body modeling to more realistically simulate the human body falling and determine the impact force. This review also concludes that determination of joint torques is quite complicated and more research is required on this topic.
Not only there is a need for developing an accurate model for predicting the fall-induced impact force, impact force itself should be more appropriately considered in hip fracture risk assessment tools. FE models are the only tools that explicitly take the impact force into consideration. An improved model for determining the impact force can be a step forward to more appropriately consider the impact force in hip fracture risk assessment.
Due to the worldwide increasing rate of hip fractures, developing an accurate model for predicting the impact force and adopting the model in hip fracture risk assessment tools can be considered as a crucial priority for biomechanical researches. It could improve the accuracy of identifying patients at high risk of fracture who may benefit from in-time treatment.
References
DeGoede KM, Ashton-Miller JA, Schultz AB (2003) Fall-related upper body injuries in the older adult: a review of the biomechanical issues. J Biomech 36:1043–1053
Rivara FP, Grossman DC, Cummings P (1997) Injury prevention. N Engl J Med 337:543–548
Green C, Molony D, Fitzpatrick C, ORourke K (2010) Age-specific incidence of hip fracture in the elderly: a healthy decline. Surgeon 8:310–313
Gullberg B, Johnell O, Kanis JA (1997) World-wide projections for hip fracture. Osteoporos Int 7:407–413
Kannus P, Leiponen P, Parkkari J, Palvanen M, Jarvinen M (2006) A sideways fall and hip fracture. Bone 39:383–384
Boonen S, Autier P, Barette M, Vanderschueren D, Lips P, Haentjens P (2004) Functional outcome and quality of life following hip fracture in elderly women: a prospective controlled study. Osteoporos Int 15:87–94
Phillips S, Fox N, Jacobs J, Wright WE (1988) The direct medical costs of osteoporosis for American women aged 45 and older. Bone 9:271–279
Huddleston JM, Whitford KJ (2001) Medical care of elderly patients with hip fractures. Mayo Clin Proc 76:295–298
Greenspan SL, Myers ER, Kiel DP, Parker RA, Hayes WC, Resnick NM (1998) Fall direction, bone mineral density, and function: risk factors for hip fracture in frail nursing home elderly. Am J Med 104:539–545
Hayes WC, Piazza SJ, Zysset PK (1991) Biomechanics of fracture risk prediction of the hip and spine by quantitative computed tomography. Radiol Clin N Am 29:1–18
Myers ER, Wilson SE (1997) Biomechanics of osteoporosis and vertebral fracture. Spine 22:25S–31S
Luo Y (2015) A biomechanical sorting of clinical risk factors affecting osteoporotic hip fracture. Osteoporosis International 1-17
Robinovitch SN, Hayes WC, McMahon TA (1991) Prediction of femoral impact forces in falls on the hip. ASME J Biomech Eng 113:366–374
Kroonenberg AJ, Hayes WC, McMahon TA (1995) Dynamic models for sideways falls from standing height. J Biomech Eng 117:309–318
Robinovitch SN, McMahon TA, Hayes WC (1995) Force attenuation in trochanteric soft tissues during impact from a fall. J Orthop Res 13:956–962
Van den Kroonenberg AJ, Hayes WC, McMahon TA (1996) Hip impact velocities and body configurations for voluntary falls from standing height. J Biomech 29:807–811
Hayes WC, Myers ER, Robinovitch SN, Van Den Kroonenberg A, Courtney AC, McMahon TA (1996) Etiology and prevention of age-related hip fractures. Bone 18:S77–S86
Robinovitch SN, Hayes WC, McMahon TA (1997) Distribution of contact force during impact to the hip. Ann Biomed Eng 25:499–508
Robinovitch SN, Hayes WC, McMahon TA (1997) Predicting the impact response of a nonlinear single-degree-of-freedom shock-absorbing system from the measured step response. J Biomech Eng 119:221–227
Sandler R, Robinovitch S (2001) An analysis of the effect of lower extremity strength on impact severity during a backward fall. J Biomech Eng 123:590–598
Robinovitch SN, Inkster L, Maurer J, Warnick B (2003) Strategies for avoiding hip impact during sideways falls. J Bone Miner Res 18:1267–1273
Robinovitch SN, Brumer R, Maurer J (2004) Effect of the squat protective response on impact velocity during backward falls. J Biomech 37:1329–1337
Feldman F, Robinovitch SN (2007) Reducing hip fracture risk during sideways falls: evidence in young adults of the protective effects of impact to the hands and stepping. J Biomech 40:2612–2618
Laing AC, Robinovitch SN (2010) Characterizing the effective stiffness of the pelvis during sideways falls on the hip. J Biomech 43:1898–1904
Levine IC, Bhan S, Laing AC (2013) The effects of body mass index and sex on impact force and effective pelvic stiffness during simulated lateral falls. Clin Biomech 28:1026–1033
Choi WJ, Cripton PA, Robinovitch SN (2015) Effects of hip abductor muscle forces and knee boundary conditions on femoral neck stresses during simulated falls. Osteoporos Int 26:291–301
Nasiri M, Luo Y (2016) Study of sex differences in the association between hip fracture risk and body parameters by DXA-based biomechanical modeling. Bone 90:90–98
Laing AC, Tootoonchi I, Hulme PA, Robinovitch SN (2006) Effect of compliant flooring on impact force during falls on the hip. J Orthop Res 24:1405–1411
Bateni H, Zecevic A, McIlroy W, Maki B (2004) Resolving conflicts in task demands during balance recovery: does holding an object inhibit compensatory grasping? Exp Brain Res 157:49–58
Smith LD (1953) Hip fractures: the role of muscle contraction or intrinsic forces in the causation of fractures of the femoral neck. J Bone Joint Surg 35:367–383
Phillips J, Williams J, Melick R (1975) Prediction of the strength of the neck of femur from its radiological appearance. Biomed Eng 10:367–372
Dalen N, Hellstrom L, Jacobson B (1976) Bone mineral content and mechanical strength of the femoral neck. Acta Orthop Scand 47:503–508
Leichter I, Margulies JY, Weinreb A, Mizrahi J, Robin GC, Conforty B, Makin M, Bloch B (1982) The relationship between bone density, mineral content, and mechanical strength in the femoral neck. Clin Orthop Relat Res 163:272–281
Mizrahi J, Margulies JY, Leichter I, Deutsch D (1984) Fracture of the human femoral neck: effect of density of the cancellous core. J Biomed Eng 6:56–62
Alho A, Husby T, Hoiseth A (1988) Bone mineral content and mechanical strength an ex vivo study on human femora at autopsy. Clin Orthop Relat Res 227:292–297
Esses S, Lotz J, Hayes W (1989) Biomechanical properties of the proximal femur determined in vitro by single-energy quantitative computed tomography. J Bone Miner Res 4:715–722
Lotz JC, Hayes WC (1990) The use of quantitative computed tomography to estimate risk of fracture of the hip from falls. J Bone Joint Surg 72:689–700
Courtney AC, Wachtel EF, Myers ER, Hayes WC (1994) Effects of loading rate on strength of the proximal femur. Calcif Tissue Int 55:53–58
Bouxsein ML, Courtney AC, Hayes WC (1995) Ultrasound and densitometry of the calcaneus correlate with the failure loads of cadaveric femurs. Calcif Tissue Int 56:99–103
Pinilla T, Boardman K, Bouxsein M, Myers E, Hayes W (1996) Impact direction from a fall influences the failure load of the proximal femur as much as age-related bone loss. Calcif Tissue Int 58:231–235
Cheng XG, Lowet G, Boonen S, Nicholson PHF, Brys P, Nijs J, Dequeker J (1997) Assessment of the strength of proximal femur in vitro: relationship to femoral bone mineral density and femoral geometry. Bone 20:213–218
Cheng XG, Lowet G, Boonen S, Nicholson PHF, Van Der Perre G, Dequeker J (1998) Prediction of vertebral and femoral strength in vitro by bone mineral density measured at different skeletal sites. J Bone Miner Res 13:1439–1443
Lang TF, Keyak JH, Heitz MW, Augat P, Lu Y, Mathur A, Genant HK (1997) Volumetric quantitative computed tomography of the proximal femur: precision and relation to bone strength. Bone 21:101–108
Keyak JH, Rossi SA, Jones KA, Skinner HB (1998) Prediction of femoral fracture load using automated finite element modeling. J Biomech 31:125–133
Bouxsein ML, Coan BS, Lee SC (1999) Prediction of the strength of the elderly proximal femur by bone mineral density and quantitative ultrasound measurements of the heel and tibia. Bone 25:49–54
Keyak JH (2000) Relationships between femoral fracture loads for two load configurations. J Biomech 33:499–502
Lochmuller EM, Groll O, Kuhn V, Eckstein F (2002) Mechanical strength of the proximal femur as predicted from geometric and densitometric bone properties at the lower limb versus the distal radius. Bone 30:207–216
Eckstein F, Wunderer C, Boehm H, Kuhn V, Priemel M, Link TM, Lochmüller E-M (2004) Reproducibility and side differences of mechanical tests for determining the structural strength of the proximal femur. J Bone Miner Res 19:379–385
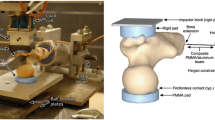
Heini PF, Franz T, Fankhauser C, Gasser B, Ganz R (2004) Femoroplasty-augmentation of mechanical properties in the osteoporotic proximal femur: a biomechanical investigation of PMMA reinforcement in cadaver bones. Clin Biomech 19:506–512
Manske SL, Liu-Ambrose T, de Bakker PM, Liu D, Kontulainen S, Guy P, Oxland TR, McKay HA (2006) Femoral neck cortical geometry measured with magnetic resonance imaging is associated with proximal femur strength. Osteoporos Int 17:1539–1545
Pulkkinen P, Eckstein F, Lochmüller E-M, Kuhn V, Jämsä T (2006) Association of geometric factors and failure load level with the distribution of cervical vs. trochanteric hip fractures. J Bone Min Res 21:895–901
Pulkkinen P, Jämsä T, Lochmüller EM, Kuhn V, Nieminen MT, Eckstein F (2008) Experimental hip fracture load can be predicted from plain radiography by combined analysis of trabecular bone structure and bone geometry. Osteoporos Int 19:547–558
Langton CM, Pisharody S, Keyak JH (2009) Comparison of 3D finite element analysis derived stiffness and BMD to determine the failure load of the excised proximal femur. Med Eng Phys 31:668–672
de Bakker PM, Manske SL, Ebacher V, Oxland TR, Cripton PA, Guy P (2009) During sideways falls proximal femur fractures initiate in the superolateral cortex: evidence from high-speed video of simulated fractures. J Biomech 42:1917–1925
Dragomir D, Buijs J, McEligot S, Dai Y, Entwistle R, Salas C, Melton L, Bennet K, Khosla S, Amin S (2011) Robust QCT/FEA models of proximal femur stiffness and fracture load during a sideways fall on the hip. Ann Biomed Eng 39:742–755
Buijs J, Dragomir D (2011) Validated finite element models of the proximal femur using two-dimensional projected geometry and bone density. Comput Methods Prog Biomed 104:168–174
Koivumaki J, Thevenot J, Pulkkinen P, Kuhn V, Link TM, Eckstein F, Jamsa T (2012) CT-based finite element models can be used to estimate experimentally measured failure loads in the proximal femur. Bone 50:824–829
Koivumaki JEM, Thevenot J, Pulkkinen P, Kuhn V, Link TM, Eckstein F, Jamsa T (2012) Cortical bone finite element models in the estimation of experimentally measured failure loads in the proximal femur. Bone 51:737–740
Nishiyama KK, Gilchrist S, Guy P, Cripton P, Boyd SK (2013) Proximal femur bone strength estimated by a computationally fast finite element analysis in a sideways fall configuration. J Biomech 46:1231–1236
Dall'Ara E, Luisier B, Schmidt R, Kainberger F, Zysset P, Pahr D (2013) A nonlinear QCT-based finite element model validation study for the human femur tested in two configurations in vitro. Bone 52:27–38
Mirzaei M, Keshavarzian M, Naeini V (2014) Analysis of strength and failure pattern of human proximal femur using quantitative computed tomography (QCT)-based finite element method. Bone 64:108–114
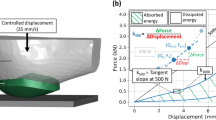
Gilchrist S, Nishiyama KK, de Bakker P, Guy P, Boyd SK, Oxland T, Cripton PA (2014) Proximal femur elastic behaviour is the same in impact and constant displacement rate fall simulation. J Biomech 47:3744–3749
Ariza O, Gilchrist S, Widmer RP, Guy P, Ferguson SJ, Cripton PA, Helgason B (2015) Comparison of explicit finite element and mechanical simulation of the proximal femur during dynamic drop-tower testing. J Biomech 48:224–232
Grassi L, Väänänen SP, Ristinmaa M, Jurvelin JS, Isaksson H (2016) How accurately can subject-specific finite element models predict strains and strength of human femora? Investigation using full-field measurements. J Biomech 49:802–806
Grassi L, Väänänen SP, Ristinmaa M, Jurvelin JS, Isaksson H (2016) Prediction of femoral strength using 3D finite element models reconstructed from DXA images: validation against experiments. Biomechanics and Modeling in Mechanobiology 1-12
Robinovitch SN, Evans SL, Minns J et al (2009) Hip protectors: recommendations for biomechanical testing-an international consensus statement (part I). Osteoporos Int 20:1977–1988
Haider IT, Speirs AD, Frei H (2013) Effect of boundary conditions, impact loading and hydraulic stiffening on femoral fracture strength. J Biomech 46:2115–2121
Weber T, Yang K, Woo R, Fitzgerald R (1992) Proximal femur strength: correlation of the rate of loading and bone mineral density. ASME Adv Bioeng BED 22:111–114
Beck TJ, Ruff CB, Warden KE, Scott WW Jr, Rao GU (1990) Predicting femoral neck strength from bone mineral data: a structural approach. Investig Radiol 25:6–18
Kanis J, McCloskey E, Johansson H, Oden A, Borgstrom F, Strom O (2010) Development and use of FRAX in osteoporosis. Osteoporos Int 21:407–413
Brekelmans WAM, Poorth HW, Slooff TJJH (1972) A new method to analyse the mechanical behaviour of skeletal parts. Acta orthop Scandinav 43:301–317
Nielson C, Bouxsein M, Freitas S, Ensrud K, Orwoll E (2009) Trochanteric soft tissue thickness and hip fracture in older men. J Clin Endocrinol Metab 94:491–496
Blaak E (2001) Gender differences in fat metabolism. Curr Opin Clin Nutr Metab Care 4:499–502
Robinovitch SN, Feldman F, Yang Y, Schonnop R, Leung PM, Sarraf T, Sims-Gould J, Loughin M (2013) Video capture of the circumstances of falls in elderly people residing in long-term care: an observational study. Lancet 381:47–54
Nasiri Sarvi M (2015) Assessment of hip fracture risk by a two-level subject-specific biomechanical model. Mechanical Engineering. Ph.D. thesis, University of Manitoba, Canada, p 164
Groen BE, Weerdesteyn V, Duysens J (2007) Martial arts fall techniques decrease the impact forces at the hip during sideways falling. J Biomech 40:458–462
Nasiri Sarvi M, Luo Y (2015) A two-level subject-specific biomechanical model for improving prediction of hip fracture risk. Clin Biomech 30:881–887
Nasiri Sarvi M, Luo Y, Sun P, Ouyang J (2014) Experimental validation of subject-specific dynamics model for predicting impact force in sideways fall. J Biomed Sci Eng 7:405–418
Pena E, Calvo B, Martinez MA, Doblare M (2007) An anisotropic visco-hyperelastic model for ligaments at finite strains. Formulation and computational aspects. Int J Solids Struct 44:760–778
Majumder S, Roychowdhury A, Pal S (2008) Effects of trochanteric soft tissue thickness and hip impact velocity on hip fracture in sideways fall through 3D finite element simulations. J Biomech 41:2834–2842
Natali AN, Carniel EL, Pavan PG (2008) Constitutive modelling of inelastic behaviour of cortical bone. Med Eng Phys 30:905–912
Malmivaara A, Heliovaara M, Knekt P, Reunanen A, Aromaa A (1993) Risk factors for injurious falls leading to hospitalization or death in a cohort of 19,500 adults. Am J Epidemiol 138:384–394
Greenspan SL, Myers ER, Maitland LA, Resnick NM, Hayes WC (1994) Fall severity and bone mineral density as risk factors for hip fracture in ambulatory elderly. JAMA 271:128–133
Laet C, Kanis JA, Oden A et al (2005) Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int 16:1330–1338
Bouxsein ML, Szulc P, Munoz F, Thrall E, Sornay-Rendu E, Delmas PD (2007) Contribution of trochanteric soft tissues to fall force estimates, the factor of risk, and prediction of hip fracture risk. J Bone Miner Res 22:825–831
Armstrong MEG, Spencer EA, Cairns BJ, Banks E, Pirie K, Green J, Wright FL, Reeves GK, Beral V, for the Million Women Study C (2011) Body mass index and physical activity in relation to the incidence of hip fracture in postmenopausal women. J Bone Miner Res 26:1330–1338
Johansson H, Kanis JA, Odén A et al (2013) A meta-analysis of the association of fracture risk and body mass index in women. J Bone Miner Res 29:223–233
Majumder S, Roychowdhury A, Pal S (2013) Hip fracture and anthropometric variations: dominance among trochanteric soft tissue thickness, body height and body weight during sideways fall. Clin Biomech 28:1034–1040
Bhan S, Levine IC, Laing AC (2014) Energy absorption during impact on the proximal femur is affected by body mass index and flooring surface. J Biomech 47:2391–2397
Choi WJ, Russell CM, Tsai CM, Arzanpour S, Robinovitch SN (2015) Age-related changes in dynamic compressive properties of trochanteric soft tissues over the hip. J Biomech 48:695–700
Derler S, Spierings AB, Schmitt KU (2005) Anatomical hip model for the mechanical testing of hip protectors. Med Eng Phys 27:475–485
Li N, Tsushima E, Tsushima H (2013) Comparison of impact force attenuation by various combinations of hip protector and flooring material using a simplified fall-impact simulation device. J Biomech 46:1140–1146
Laing AC, Robinovitch SN (2008) The force attenuation provided by hip protectors depends on impact velocity, pelvic size, and soft tissue stiffness. Journal of Biomechanical Engineering 130:
Laing AC, Robinovitch SN (2008) Effect of soft shell hip protectors on pressure distribution to the hip during sideways falls. Osteoporos Int 19:1067–1075
Choi WJ, Hoffer JA, Robinovitch SN (2010) Effect of hip protectors, falling angle and body mass index on pressure distribution over the hip during simulated falls. Clin Biomech 25:63–69
Luo Y, Nasiri Sarvi M, Sun P, Leslie WD, Ouyang J (2014) Prediction of impact force in sideways fall by image-based subject-specific dynamics model. International Biomechanics 1-14
Durkin JL, Dowling JJ, Andrews DM (2002) The measurement of body segment inertial parameters using dual energy X-ray absorptiometry. J Biomech 35:1575–1580
Luo Y, Nasiri Sarvi M (2015) A subject-specific inverse-dynamics approach for estimating joint stiffness in sideways fall. Int J Exp Comput Biomech 3:137–160
Lo J, Ashton-Miller JA (2008) Effect of pre-impact movement strategies on the impact forces resulting from a lateral fall. J Biomech 41:1969–1977
DeGoede KM, Ashton-Miller JA (2002) Fall arrest strategy affects peak hand impact force in a forward fall. J Biomech 35:843–848
Yoshikawa T, Turner CH, Peacock M, Slemenda CW, Weaver CM, Teegarden D, Markwardt P, Burr DB (1994) Geometric structure of the femoral neck measured using dual-energy X-ray absorptiometry. J Bone Miner Res 9:1053–1064
Hayes W, Myers E, Morris J, Gerhart T, Yett H, Lipsitz L (1993) Impact near the hip dominates fracture risk in elderly nursing home residents who fall. Calcif Tissue Int 52:192–198
Cc S, Hayes WC, McMahon TA (2001) Disturbance type and gait speed affect fall direction and impact location. J Biomech 34:309–317
Nag PK, Vyas H, Nag A, Pal S (2008) Applying stabilometry in characterizing floor sitting modes of women. Int J Ind Ergon 38:984–991
Nag PK, Chintharia S, Saiyed S, Nag A (1986) EMG analysis of sitting work postures in women. Appl Ergon 17:195–197
Hsiao ET, Robinovitch SN (1998) Common protective movements govern unexpected falls from standing height. J Biomech 31:1–9
Sabick MB, Hay JG, Goel VK, Banks SA (1999) Active responses decrease impact forces at the hip and shoulder in falls to the side. J Biomech 32:993–998
DeGoede KM, Ashton-Miller JA (2003) Biomechanical simulations of forward fall arrests: effects of upper extremity arrest strategy, gender and aging-related declines in muscle strength. J Biomech 36:413–420
Lo J, Ashton-Miller JA (2008) Effect of upper and lower extremity control strategies on predicted injury risk during simulated forward falls: a study in healthy young adults. J Biomech Eng 130:410–415
Nevitt MC, Cummings SR, Hudes ES (1991) Risk factors for injurious falls: a prospective study. J Gerontol 46:M164–M170
Robinovitch SN, Chiu J, Sandler R, Liu Q (2000) Impact severity in self-initiated sits and falls associates with center-of-gravity excursion during descent. J Biomech 33:863–870
Weerdesteyn V, Rijken H, Geurts ACH, Smits-Engelsman BCM, Mulder T, Duysens J (2006) A five-week exercise program can reduce falls and improve obstacle avoidance in the elderly. Gerontology 52:131–141
Weerdesteyn V, Groen BE, van Swigchem R, Duysens J (2008) Martial arts fall techniques reduce hip impact forces in naive subjects after a brief period of training. J Electromyogr Kinesiol 18:235–242
Groen BE, Smulders E, de Kam D, Duysens J, Weerdesteyn V (2010) Martial arts fall training to prevent hip fractures in the elderly. Osteoporos Int 21:215–221
Van der Zijden AM, Groen BE, Tanck E, Nienhuis B, Verdonschot N, Weerdesteyn V (2012) Can martial arts techniques reduce fall severity? An in vivo study of femoral loading configurations in sideways falls. J Biomech 45:1650–1655
Choi WJ, Wakeling JM, Robinovitch SN (2015) Kinematic analysis of video-captured falls experienced by older adults in long-term care. J Biomech 48:911–920
O'Neill TW, Varlow J, Silman AJ, Reeve J, Reid DM, Todd C, Woolf AD (1994) Age and sex influences on fall characteristics. Ann Rheum Dis 53:773–775
Iyo T, Maki Y, Sasaki N, Nakata M (2004) Anisotropic viscoelastic properties of cortical bone. J Biomech 37:1433–1437
Wu Z, Ovaert TC, Niebur GL (2012) Viscoelastic properties of human cortical bone tissue depend on gender and elastic modulus. J Orthop Res 30:693–699
Bembey AK, Oyen ML, Bushby AJ, Boyde A (2006) Viscoelastic properties of bone as a function of hydration state determined by nanoindentation. Philos Mag 86:5691–5703
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Electronic supplementary material
Supplementary Fig. 1
(PDF 120 kb)
Supplementary Fig. 2
(PDF 119 kb)
Supplementary Fig. 3
(PDF 112 kb)
Supplementary Fig. 4
(PDF 121 kb)
Rights and permissions
About this article

Cite this article
Nasiri Sarvi, M., Luo, Y. Sideways fall-induced impact force and its effect on hip fracture risk: a review. Osteoporos Int 28, 2759–2780 (2017). https://doi.org/10.1007/s00198-017-4138-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-017-4138-5