
Abstract
Summary
The P2X7 receptor is an ATP-gated cation channel. We investigated the effect of both loss-of-function and gain-of-function polymorphisms in the P2X7 receptor gene on BMD and risk of vertebral fractures and found that five polymorphisms and haplotypes containing three of these polymorphisms were associated with BMD and fracture risk.
Introduction
The P2X7 receptor is an ATP-gated cation channel. P2X7 receptor knockout mice have reduced total bone mineral content, and because several functional polymorphisms have been identified in the human P2X7 receptor gene, we wanted to investigate the effect of these polymorphisms on BMD and risk of vertebral fractures in a case–control study including 798 individuals.
Methods
Genotyping was carried out using TaqMan assays. BMD was measured using dual energy X-ray absorptiometry, and vertebral fractures were assessed by lateral spinal X-rays.
Results
The rare allele of a splice site polymorphism, 151 + 1: G-T, was associated with increased fracture risk and reduced BMD in women. Two other loss-of-function polymorphisms, Glu496Ala and Gly150Arg, were also associated with BMD. The Glu496Ala variant allele was associated with decreased lumbar spine BMD in women and decreased total hip BMD in men. The 150Arg allele was associated with decreased total hip BMD in women and men combined. The minor allele of the gain-of-function polymorphism, Ala348Thr, was associated with reduced fracture risk and increased BMD at all sites in men. The Gln460Arg variant allele, which has been associated with increased receptor function in monocytes, was associated with increased total hip BMD in women. With the exception of His155Tyr for which we found conflicting results in men and women, our results are consistent with the phenotype of the knockout mouse. Analysis of a haplotype containing Ala348Thr, Gln460Arg, and Glu496Ala showed that the effects of the haplotypes on BMD and fracture were driven by Ala348Thr in men and by Gln460Arg and Glu496Ala in women.
Conclusion
In conclusion, we found that functional polymorphisms in the P2X7 receptor gene and haplotypes containing three of these polymorphisms are associated with osteoporosis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a common skeletal disorder characterised by low bone mineral density (BMD) and microarchitectural deterioration of bone tissue, resulting in increased fracture risk [1]. The disease is caused by multiple genetic and environmental factors, as well as interactions between these factors. The genetic influence on the pathogenesis is high. Twin and family studies have suggested that between 50 % and 80 % of the interindividual variance in BMD is genetically determined depending on age and skeletal sites [2]. Fracture risk is also heritable, but several studies have shown that the inheritance of fracture risk is at least partly independent of BMD, suggesting that other factors such as bone turnover, bone geometry, and risk of falling may also mediate the genetic susceptibility to fracture [3, 4]. The effect of individual polymorphisms is, however, modest and most of the genes involved in the pathogenesis of osteoporosis are still unknown [5].
The P2X7 purinergic receptor is a ligand-gated cation channel [6] that is expressed in many cell types including cells of the immune system [7], osteoclasts [8, 9], and osteoblasts [10, 11]. P2X7 receptors are trimers and the P2X7 subunit is 595 amino acids long and consists of two hydrophobic transmembrane domains, intracellular N- and C-termini and a large extracellur domain [6]. Activation of the receptor by extracellular ATP opens the cation-selective channel allowing influx of Ca2+ and Na+ and efflux of K+ [12]. Prolonged or repeated exposure to ATP induces formation of a larger pore that allows passage of molecules up to 900 Da [13].
In cells of the immune system, P2X7 receptor activation leads to multiple downstream events, including activation of metalloproteases [14, 15], release of interleukin-1β [16] and apoptosis [17, 18]. The effects of P2X7 receptor activation in osteoclasts and osteoblasts have not been as thoroughly described, but it has been shown that P2X7 receptor activation in osteoblasts induces membrane blebbing [10, 19], stimulates differentiation, enhances mineralization [20], and increases the response to fluid shear stress [21]. In osteoclasts, activation of the P2X7 receptor leads to activation of NF-κB [22] and induction of apoptosis [23]. P2X7 receptors on osteoclasts are also involved in formation of multinucleated osteoclasts [11, 24, 25] and intercellular calcium signaling between osteoblasts and osteoclasts [26].
The importance of the P2X7 receptor in bone metabolism has been demonstrated by the characterization of a knockout model. Disruption of the P2X7 receptor gene in mice resulted in reduced total bone mineral content, decreased periosteal bone formation, increased trabecular bone resorption, and increased osteoclast surface and numbers [11]. Furthermore, the effect of mechanical loading on periosteal bone formation was strongly reduced in the knockout mice [21].
There is a considerable variation in P2X7 receptor function between humans [27]. This may be explained at least, in part, by several loss-of-function and gain-of-function polymorphisms. Eight loss-of-function polymorphisms in the gene encoding the human P2X7 receptor, P2RX7, have been well-characterized. The three most frequent of these, substitution of Val76 with Ala (rs17525809), Thr357 with Ser (rs2230911), and Glu496 with Ala (rs3751143), have minor allele frequencies between 6 and 18 % in Caucasians and cause reduced receptor function [28–31]. In contrast to these polymorphisms, a splice site polymorphism, 151 + 1G-T (rs35933842) and the nonsynonymous polymorphisms, Gly150Arg (rs28360447), Ile568Asn (rs1653624), and Arg307Gln (rs28360457), are very rare and result in complete lack of functional P2X7 receptors [28, 29, 32–34]. Four other nonsynonymous polymorphisms, Arg270His (rs7958311), His155Tyr (rs208294), Ala348Thr (rs1718119), and Gln460Arg (rs2230912), have been characterized as being gain-of-function polymorphisms using recombinant expression or have been shown to be associated with gain of P2X7 receptor function [27–29, 35].
Two recent studies have found associations between nonsynonymous polymorphisms in P2RX7 and BMD, bone loss, and vertebral fracture risk in early postmenopausal women [36, 37]. In this study, we wanted to examine if genetic variations in P2RX7 affect BMD and the risk of vertebral fractures in older Danish men and women.
Study population and methods
The AROS study population
The study was a case–control study. The cases comprised 462 osteoporotic women and men, defined by a T-score < −2.5 or at least one nontraumatic fracture of the spine, referred to the Department of Endocrinology at Aarhus University Hospital. Patients with secondary causes of osteoporosis such as vitamin D deficiency, thyroid disease, or early menopause and patients receiving medication known to influence BMD or bone turnover were excluded from the study. Vertebral fracture was defined as a 20 % or more reduction of the anterior, posterior, or central height of a vertebra as assessed by X-ray [38]. The controls comprised 336 men and women not having diseases or taking medications known to influence BMD and bone turnover. The controls were recruited from the local community by invitations posted at places of work, senior citizens clubs, schools, educational institutions, hospitals, and at general practitioners. Characteristics of the case and control groups are shown in Table 1. Analyses of association between the polymorphisms and the risk of fracture were conducted in subgroups matched for age, gender, and menopausal status (Table 2). The study was approved by the local ethical committee and conducted according to Helsinki Declaration II.
BMD measurements
BMD of the lumbar spine and the following standard sites at the hip: femoral neck, trochanter, intertrochanteric region, and Wards triangle, was assessed using dual energy X-ray absorptiometry (DXA) on a Hologic 1000 (Hologic Europe, Belgium) (CV = 1 % at the lumbar spine and 2 % at the total hip) or a Norland bone densitometer (Gammatec, Denmark) (CV = 1 % at the lumbar spine and 1.8 % at the total hip). Results obtained on the Norland densitometer were corrected for the difference between the two densitometers using the correction formulas suggested by Genant et al. [39].
Selection and genotyping of P2RX7 polymorphisms
For selection of polymorphisms in P2RX7, we searched the literature for functional polymorphisms and the dbSNP database for nonsynonymous polymorphisms with a minor allele frequency of at least 5 % in May 2009. This resulted in the identification of 11 polymorphisms. Genomic DNA was isolated from whole blood leukocytes as described by Kunkel et al. [40] or by using commercially available kits from Qiagen or Sigma-Aldrich. Genotyping was performed using TaqMan allelic discrimination assays. Assay-specific primers and allele-specific TaqMan MGB probes were obtained from Applied Biosystems as Pre-Designed or Custom TaqMan SNP Genotyping Assays. PCR was carried out with reaction mixes of 3 or 4 μl containing 5–20 ng of genomic DNA, TaqMan Universal PCR Master Mix No AmpErase UNG (Applied Biosystems) and TaqMan SNP Genotyping Assay Mix. Thermocycling was performed on an ABI 7500 FAST Real-Time PCR System using the following protocol: 95 °C for 10 min followed by 40 cycles of 92.1 °C for 15 s and 60 °C for 1 min. Pre- and post-PCR fluorescence measurements were done with the same instrument. Sequence detection software version 1.3 (Applied Biosystems) was used to call genotypes manually. The reproducibility of genotyping was determined by analyzing 45 randomly selected samples (approximately 5 % of the study population) twice. No inconsistent genotype calls were observed.
Statistical analyses
Deviation of genotype frequencies from those expected under Hardy–Weinberg equilibrium was tested in the normal controls by the χ 2 test. Pairwise linkage disequilibrium (LD) between all SNPs was calculated using Haploview v4.0 [41].
Differences in the prevalence of the genotypes between osteoporotic patients with vertebral fractures and age- and gender-matched normal controls were tested using the χ 2 test. The effect of genotypes on fracture risk was also examined by logistic regression analysis including age, body weight, and lumbar spine BMD as covariates. The effect of genotypes on measured BMD corrected for age, gender, and body weight was evaluated by analysis of variance (ANOVA), trend tests, and Student's t test for unpaired data. BMD was corrected for age, gender, and body weight based on correlation analyses in the normal individuals. The analyses were done using SPSS version 15.0.
To study the effect of haplotypes on BMD and fracture risk, we used the program haplo.stats (http://cran.r-project.org), which takes the different effects of the individual haplotypes into account. We used the function haplo.score to investigate the influence of the individual haplotypes on BMD and fracture risk and the function haplo.glm to investigate the effect size—with and without correction for covariates—of the haplotypes compared with the most common haplotype. For both analyses, different models of inheritance—additive, recessive, and dominant—were used.
The association analyses were stratified by gender because the effect on bone of P2X7 receptor deletion is more pronounced in male than female mice [11]. The level of significance was set at 0.05.
The power to detect a 10 % difference in carriers of the minor allele between women with and without vertebral fracture was 53–97 %, whereas the power to detect a 5 % difference was 17–57 %. In men, the power to detect a 10 % difference in carriers of the minor allele between patients with fracture and normal controls was 15–38 %. The power was 18–81 % and 54–100 % to detect a difference in BMD of 5 and 10 %, respectively, between women homozygous for the common allele and women carrying the minor allele. In men, the power to detect a change in BMD of 10 % between carriers of the variant allele and noncarriers was 16–87 %.
Results
P2RX7 polymorphisms and linkage disequilibrium
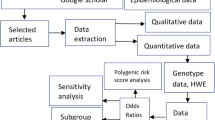
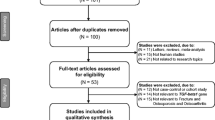
The polymorphisms genotyped in this study are depicted in Fig. 1. All polymorphisms were found to be in Hardy–Weinberg equilibrium (χ 2 = 0.01–3.57, p = 0.17–0.99). Pairwise LD calculations showed that several of the polymorphisms with a minor allele frequency above 5 % were in LD (Fig. 2).

Investigated P2RX7 polymorphisms and haplotypes. Asterisk indicates complete loss-of-function polymorphisms. Number sign indicates polymorphisms with reduced receptor function. Dagger indicates polymorphisms with increased receptor function. Section sign indicates polymorphism associated with increased receptor function most likely through linkage with other functional polymorphisms

Haploview analysis of pairwise LD between P2RX7 polymorphisms with a minor allele frequency above 5 %. Each diamond represents a pairwise LD relationship between two SNPs. The numbers within the diamonds denote D′ values multiplied by 100. Diamonds without a number indicates D′ = 1. Different shades of gray correspond to r 2 values between 0 and 1 where the extent of LD is lowered as the shading lightens. White diamonds represents r 2 = 0
Associations between genotypes and fracture risk
Table 3 shows the genotype distribution in patients with vertebral fractures and normal controls. In women, the frequency of carrying the T allele of the 151 + 1: G-T polymorphism was higher among patients with vertebral fractures 5.7 % versus 0.9 % among normal controls (χ 2 = 8.14, p = 0.004). There were only two men carrying the T allele. Using logistic regression analysis including age and the 151 + 1: G-T polymorphism, there was a significant association between the 151 + 1: G-T polymorphism and fracture risk in women (p = 0.04). When body weight and crude lumbar spine BMD was included in the model, the association disappeared (p = 0.26) suggesting that the association with fracture risk was mediated by body weight and/or BMD.
The Ala348Thr minor allele was associated with reduced risk of vertebral fractures in men. The distribution of the genotypes, AlaAla, AlaThr, and ThrThr, in men with osteoporotic vertebral fracture and normal controls were 42.9 %, 50.8 %, and 6.3 % and 31.6 %, 36.8 %, and 31.6 %, respectively; χ 2 = 12.7, p = 0.002. Logistic regression analysis including age, body weight, and the Ala348Thr polymorphism confirmed the association (p = 0.003). Inclusion of crude lumbar spine BMD in the analysis revealed that the association between the Ala348Thr polymorphism and fracture risk was partly independent of lumbar spine BMD (p = 0.03). In women, there was no association between Ala348Thr and fracture risk.
For the Glu496Ala polymorphism, there was a trend for an association between carriers of the Ala allele and increased fracture risk in men (χ2 = 3.03, p = 0.08) but not in women. None of the other polymorphisms were associated with fracture risk.
Associations between genotypes and BMD
The polymorphisms that were associated with fracture risk were also associated with BMD (Table 4). Women carrying the T allele of the 151 + 1: G-T polymorphism had lower BMD at the lumbar spine 0.763 ± 0.167 g/cm2 (mean ± SD) versus 0.855 ± 0.157 g/cm2 in women with the GG genotype (p = 0.02). A similar significant reduction in BMD was found at the total hip (p = 0.01), but at the femoral neck, the reduction in BMD was not significant. In men, BMD was also reduced in carriers of the T allele of the 151 + 1: G-T polymorphism although not significant.
The Ala348Thr variant allele was associated with increased BMD in men. In men homozygous for the 348Thr allele, BMD at the lumbar spine was 0.948 ± 0.188 g/cm2 compared with 0.886 ± 0.163 g/cm2 and 0.841 ± 0.143 g/cm2 in men with AlaThr and AlaAla genotypes, respectively (p = 0.04). The same pattern of association was found at the femoral neck (p = 0.04) and total hip (p = 0.01). At all sites, trend test showed evidence of an allele dose effect (p = 0.01, p = 0.02, and p = 0.003, respectively). In women, BMD was also highest for the ThrThr genotype, but the differences in BMD between genotypes were not significant.
BMD at the hip and lumbar spine was also increased for the minor allele of the Gln460Arg polymorphism, which was in LD with the Ala348Thr polymorphism. In contrast to the Ala348Thr polymorphism, the difference in BMD between the Gln460Arg genotypes was not significant in men, but it was significant at the total hip in women (p = 0.01). As for the Ala348Thr polymorphism, there was evidence of an allele dose effect (p = 0.003 for trend).
A significant association was also found between the Glu496Ala polymorphism and total hip BMD in women (p = 0.01). BMD at the total hip was lowest in women heterozygous for the polymorphism, but when carriers of the Ala allele were compared with noncarriers, BMD at the total hip was reduced in carriers of the Ala allele (0.772 ± 0.119 g/cm2 versus 0.804 ± 0.133 g/cm2, p = 0.01). In men, carriers of the 496Ala allele had reduced BMD at the lumbar spine (p = 0.02).
For the rare Gly150Arg polymorphism, BMD was decreased in carriers of the Arg allele. In women, the difference was borderline significant at the total hip (p = 0.07). However, when men and women were combined, the difference was significant (p = 0.047).
The His155Tyr minor allele was associated with decreased lumbar spine BMD in women (p = 0.03) and women carrying the Tyr allele had also lower BMD at the femoral neck (p = 0.08) and total hip (p = 0.03). In men, however, BMD was higher for the TyrTyr genotype compared with men carrying the His allele at the femoral neck (not significant) and total hip (p = 0.04). None of the other polymorphisms were associated with BMD at any site.
P2RX7 haplotypes
Three polymorphisms, Ala348Thr, Gln460Arg, and Glu496Ala, which were associated with fracture risk and/or BMD were in LD (Fig. 2), and therefore, haplotypes could be reconstructed. Although the Thr357Ser polymorphism was in LD with these polymorphisms, it was not included in the haplotype analysis because it did not affect BMD or fracture risk. Four common haplotypes comprising more than 99 % of all haplotypes were found. These were designated haplotype 1 (Ala348-Gln460-Glu496) accounting for 42.7 % of the alleles, haplotype 2 (Thr348-Gln460-Glu496) accounting for 22.0 % of the alleles, haplotype 3 (Thr348-Arg460-Glu496) accounting for 18.8 % of the alleles, and haplotype 4 (Ala348-Gln460-Ala496) accounting for 16.3 % of the alleles (Fig. 1).
Associations between haplotypes and fracture risk
Using the haploscore function of haplostats, we found that haplotype 2 was associated with decreased fracture risk in men (additive model p = 0.006, dominant model p = 0.009) and that there was a trend for an association between haplotype 4 and increased fracture risk in men (additive model p = 0.05, dominant model p = 0.08). The odds ratio for vertebral fracture was 0.42 (95 % CI 0.22–0.83) in men with one copy of haplotype 2 compared with men that are homozygous for haplotype 1, assuming an additive model. Similar results were obtained after adjusting for age and body weight. None of the haplotypes were associated with fracture risk in women.
Associations between haplotypes and BMD
Haploscore analysis of the association between BMD and haplotypes in men showed that haplotype 2 was associated with increased BMD at the lumbar spine and femoral neck assuming an additive model (p = 0.047 and p = 0.049, respectively) and that haplotypes 1 and 4 were associated with decreased BMD at the total hip (p = 0.02 for both additive and dominant models) and lumbar spine (dominant model p = 0.04), respectively. Using the haplo.glm function and assuming an additive model, we found that in men, each allele of haplotype 2 increased BMD at the lumbar spine, femoral neck, and total hip with 0.055 ± 0.027 g/cm2 (mean ± SEM), 0.047 ± 0.021 g/cm2, and 0.060 ± 0.028 g/cm2, respectively, compared with haplotype 1 (p = 0.03–0.04). A similar effect was found after correction for age and body weight (p = 0.03–0.048). Haplotype 3 increased BMD at the total hip in men by 0.062 ± 0.026 g/cm2 compared with haplotype 1 assuming an additive model (p = 0.02). The association was, however, only borderline significant after correction for age and body weight (p = 0.06).
Among women, the haploscore analysis showed that haplotype 3 was associated with increased BMD at the total hip assuming a recessive model (p = 0.007) and that haplotype 4 was associated with reduced total hip BMD assuming a dominant model (p = 0.01). Haplo.glm analysis assuming the same models showed that haplotype 3 increased BMD at the total hip with 0.111 ± 0.04 g/cm2 (p = 0.006) and that haplotype 4 reduced BMD at the total hip with 0.039 ± 0.015 g/cm2 (p = 0.01) compared with haplotype 1. Similar effects were found after correction for age and body weight.
Discussion
In the present study, we have investigated the effect on the risk of osteoporotic vertebral fractures and BMD of nonsynonymous SNPs with a minor allele frequency above 5 % and any functional polymorphisms in P2RX7. The variant alleles of three loss-of-function polymorphisms, 151 + 1: G-T, Gly150Arg, and Glu496Ala, were associated with decreased BMD and/or reduced fracture risk.
The 151 + 1: G-T polymorphism is a splice site polymorphism, which results in complete loss-of-function because no mRNA can be detected from the variant allele [32]. The effect we found of this polymorphism on fracture risk in women seemed to be mediated through effects on BMD and/or body weight because the association was abolished by adjustment for these covariates.
The rare allele of Gly150Arg has been associated with decreased pore activity in monocytes [27], and recent studies using recombinant expression have shown that this polymorphism is a lack-of-function polymorphism [28]. The glycine residue is completely conserved among the different P2X receptors suggesting that a larger side chain cannot be tolerated at this position [13].
It has been shown that the variant allele of the Glu496Ala polymorphism reduces pore function but conflicting results have been obtained as to whether the polymorphism also affects the function of the receptor as a small cation channel [28, 31, 42]. Furthermore, in an in vitro study, it has been demonstrated that osteoclasts with the 496 AlaAla genotype are less affected by ATP-induced apoptosis than osteoclasts with the GluGlu and GluAla genotypes [23]. In accordance with the effect of this polymorphism in osteoclasts, we found an association between the Ala allele and decreased BMD in both women and men and a borderline significant association with increased fracture risk in men. In the Danish Osteoporosis Prevention Study (DOPS), the Ala allele was associated with increased fracture risk but there was no association with perimenopausal BMD, hip geometry, or postmenopausal bone loss [23, 43].
We did not find any effect on BMD or fracture risk of the two complete loss-of-function polymorphisms: Arg307Gln and Ile568Asn. The 307Gln allele has recently been shown to be associated with decreased BMD in Scottish postmenopausal women [36] and with increased bone loss in DOPS [37] as well as increased risk of total hip replacement revision [44]. The lack of replication in our study may be due to limited power for the very rare polymorphisms. In the DOPS cohort, the 568Asn allele was found to be associated with enhanced gain of bone mass in women treated with hormones for 10 years and with decreased risk of vertebral fractures in women not treated with hormones. However, the number of vertebral fractures in that study was limited and only five of the women treated with hormones were carriers of the Asn allele [23].
For His155Tyr, Ala348Thr, and Gln460Arg, which all have been demonstrated to be associated with increased P2X7 receptor function [27, 28, 35], we found associations between the variant alleles and increased BMD and/or decreased fracture risk. The minor allele of Ala348Thr was in addition to increased BMD at all sites in men also associated with decreased risk of vertebral fractures in men. Adjustment for lumbar spine BMD revealed that the association with reduced fracture risk was only partly explained by the increased BMD. This is in line with results from DOPS, where an association with decreased risk of vertebral fractures but not BMD was found [37].
The Ala348Thr polymorphism is located in the second transmembrane region, which forms the channel [45]. Although the corresponding residue in the rat P2X2 receptor is not part of the water accessible surface of the open channel [46], two recent studies using recombinant expression has shown that this polymorphism possesses both increased channel and pore function [28, 47].
In accordance with our findings, an association between the 460Arg allele and increased femoral neck BMD was found in the DOPS cohort [37]. However, studies using recombinant P2X7 receptors could not confirm that this polymorphism is a gain-of-function polymorphism [28, 29], and it is, therefore, likely that the clinical effects of this polymorphism are caused by another polymorphism in linkage disequilibrium with this polymorphism. We, therefore, examined whether polymorphisms within or close to P2RX7 have an effect on the expression of the gene in lymphoblastoid cell lines using a public available database [48]. Indeed there was an association between the 460Arg allele and increased expression levels of P2RX7 (p = 3.6 × 10−5).
Our results for the individual polymorphisms are generally in accordance with the phenotype of the knockout mouse described by Ke et al. [11]. Regarding the His155Tyr polymorphism, our results in men, but not women, are consistent with the knockout mouse. Due to the number of statistical tests performed in this study, it is possible that the results in women are a chance finding. We found two men, who are homozygous for a complete loss-of-function polymorphism. Similar to the knockout mouse, these men do not have an extreme bone phenotype. The bone phenotype of another P2X7 receptor knockout mouse model has been characterized by Gartland et al. [49]. These mice had a normal bone phenotype with the exception of increased cortical bone thickness. The inconsistency between the two mouse models could be caused by the different strategies used to generate the knockout mice or by differences in their genetic background.
The analysis of haplotypes containing the Ala348Thr, Gln460Arg, and Glu496Ala polymorphisms showed that there were several associations between haplotypes, BMD, and risk of vertebral fractures. These haplotypes have not been studied in relation to osteoporosis previously, but functional studies using recombinant expression have shown that both haplotypes containing the 348Thr allele (haplotypes 2 and 3) have increased P2X7 receptor function and it was suggested that the clinical effects of Gln460Arg are caused by linkage with Ala348Thr [29]. This is in accordance with our findings in men; however, our results in women suggest that the effects of the haplotypes are not only caused by the Ala348Thr polymorphism because we found an association between haplotype 3 and increased BMD but no association with haplotype 2. Since Gln460Arg is a nonfunctional polymorphism, the effect of haplotype 3 may be caused by a polymorphism that is not part of the investigated haplotype. When haplotype 4 was compared with haplotype 1, we found an association with decreased total hip BMD in women but no association in men pointing to an effect of Glu496Ala in women. An association with decreased BMD is consistent with the in vitro study where this haplotype was shown to have decreased receptor function [29].
Our study has several strengths as well as limitations. A strength of the study is that individuals with secondary osteoporosis were excluded from the study whereby confounding factors were reduced. A limitation is, on the other hand, that we have no information about smoking status, calcium intake, and physical activity. Especially information about physical activity could have been important in this study as the response to mechanical loading was suppressed in P2X7 receptor knockout mice [21]. Another limitation of this study is that we have focused primarily on nonsynonymous polymorphisms and have not covered the entire genetic variation in P2RX7 by selecting tag SNPs, and therefore, it cannot be excluded whether additional polymorphisms including common regulatory polymorphisms contribute to the genetic influence of P2RX7 on osteoporosis.
The power of the study was adequate to detect effects of the common polymorphisms in P2RX7, but the power to detect small effect sizes for the rare polymorphisms was limited especially in the male subgroup. The number of statistical tests carried out in this study is large and attempts to correct for multiple testing are, therefore, desirable. Bonferroni correction is generally considered to be too conservative as the polymorphisms are in linkage disequilibrium and the phenotypes, fracture risk, and BMD at different sites, are not independent. If we adjust for the number of independent polymorphisms using the method suggested by Nyholt et al. [50], the significance level is p = 0.0047 and the associations between fracture risk and the 151 + 1: G-T polymorphism in women and Ala348Thr in men as well as the associations between BMD at the total hip and the Ala348Thr polymorphism in men and Gln460Arg in women would still be significant. Furthermore, if the majority of the associations found in this study were due to chance, it would have been expected that the directions of the associations were random and that there was no overall concordance between the functional and clinical effects of the polymorphisms and the phenotype of the knockout mice. However, as discussed, there is fine concordance between our results and the functional studies. Moreover, the results we obtained for three of the common polymorphisms, which have been studied before in relation to osteoporosis, were in line with the previous results [23, 37]. In contrast to the previous studies, our study included both women and men, and the number of vertebral fractures was substantial.
In conclusion, we have shown that functional polymorphisms in P2RX7 are associated with BMD and risk of vertebral fractures. Nevertheless, our and the previous findings need to be replicated and extended in larger studies before firm conclusions can be drawn about the importance of genetic variants in P2RX7 for bone mass and fracture risk.
References
Kanis JA, Melton LJ III, Christiansen C, Johnston CC, Khaltaev N (1994) The diagnosis of osteoporosis. J Bone Miner Res 9:1137–1141
Gueguen R, Jouanny P, Guillemin F, Kuntz C, Pourel J, Siest G (1995) Segregation analysis and variance components analysis of bone mineral density in healthy families. J Bone Miner Res 10:2017–2022
Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, Cauley J, Black D, Vogt TM (1995) Risk factors for hip fracture in white women. Study of Osteoporotic Fractures Research Group. N Engl J Med 332:767–773
Andrew T, Antioniades L, Scurrah KJ, MacGregor AJ, Spector TD (2005) Risk of wrist fracture in women is heritable and is influenced by genes that are largely independent of those influencing BMD. J Bone Miner Res 20:67–74
Rivadeneira F, Styrkarsdottir U, Estrada K, Halldorsson BV, Hsu YH, Richards JB, Zillikens MC, Kavvoura FK, Amin N, Aulchenko YS, Cupples LA, Deloukas P, Demissie S, Grundberg E, Hofman A, Kong A, Karasik D, van Meurs JB, Oostra B, Pastinen T, Pols HA, Sigurdsson G, Soranzo N, Thorleifsson G, Thorsteinsdottir U, Williams FM, Wilson SG, Zhou Y, Ralston SH, van Duijn CM, Spector T, Kiel DP, Stefansson K, Ioannidis JP, Uitterlinden AG (2009) Twenty bone-mineral-density loci identified by large-scale meta-analysis of genome-wide association studies. Nat Genet 41:1199–1206
Surprenant A, Rassendren F, Kawashima E, North RA, Buell G (1996) The cytolytic P2Z receptor for extracellular ATP identified as a P2X receptor (P2X7). Science 272:735–738
Di Virgilio F, Chiozzi P, Ferrari D, Falzoni S, Sanz JM, Morelli A, Torboli M, Bolognesi G, Baricordi OR (2001) Nucleotide receptors: an emerging family of regulatory molecules in blood cells. Blood 97:587–600
Hoebertz A, Townsend-Nicholson A, Glass R, Burnstock G, Arnett TR (2000) Expression of P2 receptors in bone and cultured bone cells. Bone 27:503–510
Naemsch LN, Dixon SJ, Sims SM (2001) Activity-dependent development of P2X7 current and Ca2+ entry in rabbit osteoclasts. J Biol Chem 276:39107–39114
Gartland A, Hipskind RA, Gallagher JA, Bowler WB (2001) Expression of a P2X7 receptor by a subpopulation of human osteoblasts. J Bone Miner Res 16:846–856
Ke HZ, Qi H, Weidema AF, Zhang Q, Panupinthu N, Crawford DT, Grasser WA, Paralkar VM, Li M, Audoly LP, Gabel CA, Jee WSS, Dixon SJ, Sims SM, Thompson DD (2003) Deletion of the P2X(7) nucleotide receptor reveals its regulatory roles in bone formation and resorption. Mol Endocrinol 17:1356–1367
Khakh BS, North RA (2006) P2X receptors as cell-surface ATP sensors in health and disease. Nature 442:527–532
North RA (2002) Molecular physiology of P2X receptors. Physiol Rev 82:1013–1067
Gu B, Bendall LJ, Wiley JS (1998) Adenosine triphosphate-induced shedding of CD23 and L-selectin (CD62L) from lymphocytes is mediated by the same receptor but different metalloproteases. Blood 92:946–951
Gu BJ, Wiley JS (2006) Rapid ATP-induced release of matrix metalloproteinase 9 is mediated by the P2X7 receptor. Blood 107:4946–4953
Solle M, Labasi J, Perregaux DG, Stam E, Petrushova N, Koller BH, Griffiths RJ, Gabel CA (2001) Altered cytokine production in mice lacking P2X(7) receptors. J Biol Chem 276:125–132
Ferrari D, Los M, Bauer MK, Vandenabeele P, Wesselborg S, Schulze-Osthoff K (1999) P2Z purinoreceptor ligation induces activation of caspases with distinct roles in apoptotic and necrotic alterations of cell death. FEBS Lett 447:71–75
Humphreys BD, Rice J, Kertesy SB, Dubyak GR (2000) Stress-activated protein kinase/JNK activation and apoptotic induction by the macrophage P2X7 nucleotide receptor. J Biol Chem 275:26792–26798
Panupinthu N, Zhao L, Possmayer F, Ke HZ, Sims SM, Dixon SJ (2007) P2X7 nucleotide receptors mediate blebbing in osteoblasts through a pathway involving lysophosphatidic acid. J Biol Chem 282:3403–3412
Panupinthu N, Rogers JT, Zhao L, Solano-Flores LP, Possmayer F, Sims SM, Dixon SJ (2008) P2X7 receptors on osteoblasts couple to production of lysophosphatidic acid: a signaling axis promoting osteogenesis. J Cell Biol 181:859–871
Li J, Liu D, Ke HZ, Duncan RL, Turner CH (2005) The P2X7 nucleotide receptor mediates skeletal mechanotransduction. J Biol Chem 280:42952–42959
Korcok J, Raimundo LN, Ke HZ, Sims SM, Dixon SJ (2004) Extracellular nucleotides act through P2X7 receptors to activate NF-kappaB in osteoclasts. J Bone Miner Res 19:642–651
Ohlendorff SD, Tofteng CL, Jensen JE, Petersen S, Civitelli R, Fenger M, Abrahamsen B, Hermann AP, Eiken P, Jorgensen NR (2007) Single nucleotide polymorphisms in the P2X7 gene are associated to fracture risk and to effect of estrogen treatment. Pharmacogenet Genomics 17:555–567
Gartland A, Buckley KA, Bowler WB, Gallagher JA (2003) Blockade of the pore-forming P2X7 receptor inhibits formation of multinucleated human osteoclasts in vitro. Calcif Tissue Int 73:361–369
Pellegatti P, Falzoni S, Donvito G, Lemaire I, Di VF (2011) P2X7 receptor drives osteoclast fusion by increasing the extracellular adenosine concentration. FASEB J 25:1264–1274
Jorgensen NR, Henriksen Z, Sorensen OH, Eriksen EF, Civitelli R, Steinberg TH (2002) Intercellular calcium signaling occurs between human osteoblasts and osteoclasts and requires activation of osteoclast P2X7 receptors. J Biol Chem 277:7574–7580
Denlinger LC, Coursin DB, Schell K, Angelini G, Green DN, Guadarrama AG, Halsey J, Prabhu U, Hogan KJ, Bertics PJ (2006) Human P2X7 pore function predicts allele linkage disequilibrium. Clin Chem 52:995–1004
Roger S, Mei ZZ, Baldwin JM, Dong L, Bradley H, Baldwin SA, Surprenant A, Jiang LH (2010) Single nucleotide polymorphisms that were identified in affective mood disorders affect ATP-activated P2X7 receptor functions. J Psychiatr Res 44:347–355
Stokes L, Fuller SJ, Sluyter R, Skarratt KK, Gu BJ, Wiley JS (2010) Two haplotypes of the P2X(7) receptor containing the Ala-348 to Thr polymorphism exhibit a gain-of-function effect and enhanced interleukin-1beta secretion. FASEB J 24:2916–2927
Shemon AN, Sluyter R, Fernando SL, Clarke AL, Dao-Ung LP, Skarratt KK, Saunders BM, Tan KS, Gu BJ, Fuller SJ, Britton WJ, Petrou S, Wiley JS (2006) A Thr357 to Ser polymorphism in homozygous and compound heterozygous subjects causes absent or reduced P2X7 function and impairs ATP-induced mycobacterial killing by macrophages. J Biol Chem 281:2079–2086
Gu BJ, Zhang W, Worthington RA, Sluyter R, Dao-Ung P, Petrou S, Barden JA, Wiley JS (2001) A Glu-496 to Ala polymorphism leads to loss of function of the human P2X7 receptor. J Biol Chem 276:11135–11142
Skarratt KK, Fuller SJ, Sluyter R, Dao-Ung LP, Gu BJ, Wiley JS (2005) A 5′ intronic splice site polymorphism leads to a null allele of the P2X7 gene in 1–2 % of the Caucasian population. FEBS Lett 579:2675–2678
Wiley JS, Dao-Ung LP, Li C, Shemon AN, Gu BJ, Smart ML, Fuller SJ, Barden JA, Petrou S, Sluyter R (2003) An Ile-568 to Asn polymorphism prevents normal trafficking and function of the human P2X7 receptor. J Biol Chem 278:17108–17113
Gu BJ, Sluyter R, Skarratt KK, Shemon AN, Dao-Ung LP, Fuller SJ, Barden JA, Clarke AL, Petrou S, Wiley JS (2004) An Arg307 to Gln polymorphism within the ATP-binding site causes loss of function of the human P2X7 receptor. J Biol Chem 279:31287–31295
Cabrini G, Falzoni S, Forchap SL, Pellegatti P, Balboni A, Agostini P, Cuneo A, Castoldi G, Baricordi OR, Di Virgilio F (2005) A His-155 to Tyr polymorphism confers gain-of-function to the human P2X7 receptor of human leukemic lymphocytes. J Immunol 175:82–89
Gartland A, Skarratt KK, Hocking LJ, Parsons C, Stokes L, Jorgensen NR, Fraser WD, Reid DM, Gallagher JA, Wiley JS (2012) Polymorphisms in the P2X7 receptor gene are associated with low lumbar spine bone mineral density and accelerated bone loss in post-menopausal women. Eur J Hum Genet. doi:10.1038/ejhg.2011.245:
Jorgensen NR, Husted LB, Skarratt KK, Stokes L, Tofteng CL, Kvist T, Jensen JE, Eiken P, Brixen K, Fuller S, Clifton-Bligh R, Gartland A, Schwarz P, Langdahl BL, Wiley JS (2012) Single-nucleotide polymorphisms in the P2X7 receptor gene are associated with post-menopausal bone loss and vertebral fractures. Eur J Hum Genet. doi:10.1038/ejhg.2011.253:
McCloskey EV, Spector TD, Eyres KS, Fern ED, O'Rourke N, Vasikaran S, Kanis JA (1993) The assessment of vertebral deformity: a method for use in population studies and clinical trials. Osteoporos Int 3:138–147
Genant HK, Grampp S, Gluer CC, Faulkner KG, Jergas M, Engelke K, Hagiwara S, van Kuijk C (1994) Universal standardization for dual x-ray absorptiometry: patient and phantom cross-calibration results. J Bone Miner Res 9:1503–1514
Kunkel LM, Smith KD, Boyer SH, Borgaonkar DS, Wachtel SS, Miller OJ, Breg WR, Jones HW Jr, Rary JM (1977) Analysis of human Y-chromosome-specific reiterated DNA in chromosome variants. Proc Natl Acad Sci USA 74:1245–1249
Barrett JC, Fry B, Maller J, Daly MJ (2005) Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics 21:263–265
Boldt W, Klapperstuck M, Buttner C, Sadtler S, Schmalzing G, Markwardt F (2003) Glu496Ala polymorphism of human P2X7 receptor does not affect its electrophysiological phenotype. Am J Physiol Cell Physiol 284:C749–C756
Nissen N, Madsen JS, Bladbjerg EM, Beck Jensen JE, Jorgensen NR, Langdahl B, Abrahamsen B, Brixen K (2009) No association between hip geometry and four common polymorphisms associated with fracture: the Danish osteoporosis prevention study. Calcif Tissue Int 84:276–285
Mrazek F, Gallo J, Stahelova A, Petrek M (2010) Functional variants of the P2RX7 gene, aseptic osteolysis, and revision of the total hip arthroplasty: a preliminary study. Hum Immunol 71:201–205
Kawate T, Michel JC, Birdsong WT, Gouaux E (2009) Crystal structure of the ATP-gated P2X(4) ion channel in the closed state. Nature 460:592–598
Kracun S, Chaptal V, Abramson J, Khakh BS (2010) Gated access to the pore of a P2X receptor: structural implications for closed-open transitions. J Biol Chem 285:10110–10121
Sun C, Chu J, Singh S, Salter RD (2010) Identification and characterization of a novel variant of the human P2X(7) receptor resulting in gain of function. Purinergic Signal 6:31–45
Dixon AL, Liang L, Moffatt MF, Chen W, Heath S, Wong KC, Taylor J, Burnett E, Gut I, Farrall M, Lathrop GM, Abecasis GR, Cookson WO (2007) A genome-wide association study of global gene expression. Nat Genet 39:1202–1207
Gartland A, Buckley KA, Hipskind RA, Perry MJ, Tobias JH, Buell G, Chessell I, Bowler WB, Gallagher JA (2003) Multinucleated osteoclast formation in vivo and in vitro by P2X7 receptor-deficient mice. Crit Rev Eukaryot Gene Expr 13:243–253
Nyholt DR (2004) A simple correction for multiple testing for single-nucleotide polymorphisms in linkage disequilibrium with each other. Am J Hum Genet 74:765–769
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Husted, L.B., Harsløf, T., Stenkjær, L. et al. Functional polymorphisms in the P2X7 receptor gene are associated with osteoporosis. Osteoporos Int 24, 949–959 (2013). https://doi.org/10.1007/s00198-012-2035-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-012-2035-5