
Abstract
Summary
A total of 507,671 people ≥65 experienced hip fractures between 2000 and 2005. In 2005, 94,471 people ≥65 were hospitalized due to hip fractures, corresponding to a 28.5% increase over 6 years. Most fractures occurred in patients ≥75 (82.9%; n = 420,890; +16% across 6 years), particularly in women (78.2%; n = 396,967).
Introduction
We aimed to analyze incidence and costs of hip fractures in Italy over the last 6 years.
Methods
We analyzed the national hospitalization and DRG databases concerning fractures occurred in people ≥65 between 2000 and 2005.
Results
A total of 507,671 people ≥65 experienced hip fractures across 6 years, resulting in about 120,000 deaths. In year 2005 94,471 people aged ≥65 were hospitalized due to hip fractures, corresponding to a 28.5% increase over 6 years. The majority of hip fractures occurred in patients ≥75 (82.9%; n = 420,890; +16% across 6 years) and particularly in women (78.2%; n = 396,967). Among women, 84.2% of fractures (n = 334,223; +28.0% over 6 years) were experienced by patients ≥75, which is known to be the age group with the highest prevalence of osteoporosis, accounting for 68.6% of the overall observed increase in the total number of fractures. Hip fractures in men ≥75 increased by 33.1% (up to 16,540). Hospitalization costs increased across the six examined years (+36.1%) reaching 467 million euros in 2005, while rehabilitation costs rose up to 531 million in the same year.
Conclusions
Hip fractures of the elderly are increasing and represent a major health problem in industrialized countries such as Italy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Demographic trends of the last 50 years have increased life expectancy and changed the age profile of populations in developed countries. Italy has one of the highest life expectancies in the world: according to the Italian National Institute for Statistics (ISTAT), life expectancy at birth increased at a rate of 4 months/year from 1950 to 2005, reaching 77.8 years for men and 86.9 years for women [1, 2], but it is estimated to rise up to 78.4 and 87.4 years, respectively, by 2010 [1, 2]. In Italy, 18% of the population is actually over 65 years of age [1]; within the next decade, this age group may exceed 22% of the population [3]. Moreover, 4% of this group is already ≥80 years of age [1]. For these reasons, Italy represents an interesting international case study for determining social and economic burden of aging-related diseases, because of the increasing weight of older age groups within the general population (resulting in the inversion of the age pyramid), which is a general phenomenon observed in all industrialized countries.
Therefore, observations made in Italy could be relevant for many other industrialized countries facing similar problems of aging of the population. Increased life expectancy is associated with a greater frailty of elderly people and a higher prevalence of chronic and degenerative diseases. Osteoporosis and its complications—especially hip fractures—represent a challenge for health professionals and decision makers in the twenty-first century. The World Health Organization considers osteoporosis to be second only to cardiovascular diseases as a critical health problem [4], and in our previous study, we have shown that incidence and costs of hip fractures in Italy are already comparable to those of acute myocardial infarction [5]. Furthermore, hip fractures have a 5% acute mortality rate and 15–25% 1-year mortality [6, 7]. Once hip fracture has occurred, the ability to walk is completely lost in 20% of cases, and only 30–40% of patients recover a degree of autonomy comparable to the period before the fracture [8–11]. The main Epidemiological Study on the Prevalence of Osteoporosis in Italy (ESOPO) reported a high prevalence of osteoporosis: 23% among all women, with age-specific rates ranging from 9% (40- to 49-year-olds) to 45% (70- to 79-year-olds), and almost 15% in men aged ≥60 years [12, 13]. According to these percentages, about four million of Italian women and 800,000 men are thought to be affected by osteoporosis [2], although an overestimation of these prevalence data cannot be excluded because the ESOPO study was conducted by using QUS measurements and not DEXA [13–15]. It is known that osteoporosis is a condition that enhances the risk of fracture, especially vertebral and hip fractures [16]. Each year in Italy, almost 18,000 elderly people become completely disabled as a consequence of hip fractures, resulting in inestimable human suffering and substantial social costs [2]. Despite these observations, no detailed data were available about the incidence and costs of hip fractures in the elderly Italian population before our first analyses carried out in 2005–2006 [4, 17, 18], demonstrating a worrisome lack of appreciation concerning the severity of this pathology. In this extension study, we aimed to determine the burden of hip fractures in the Italian elderly population and its trend across 6 years.
Materials and methods
Information concerning all hospitalizations occurring in Italian public and private care setting are registered in hospital discharge records, which are collected at the Italian Ministry of Health (national hospitalization database, SDO). These information are anonymous and include patient’s age, diagnosis, procedures performed, and length of the hospitalization. This study is an extension of our previously published work addressing (with the same methodology) the incidence and costs of hip fractures compared to acute myocardial infarction in the Italian population in a 4-year survey (1999–2002). The present manuscript focuses on the number of hospitalizations for hip fracture in Italy, their incidence, and the direct cost of hospitalization and rehabilitation during the years 2000 through 2005. Actually, it does overlap with previously published data by 3 years (2000 to 2002) and the number of hip fractures (and their costs) shown in the current study are consistent with the previously published figures. We assumed that almost all hip fractures occurred in the elderly result in hospitalization. Therefore, in order to determine the incidence of hip fractures in the Italian population aged ≥65 years old, we analyzed the national hospitalization database (SDO) maintained at the Italian Ministry of Health. The study period (from year 2000 to 2005) was chosen because it reflects the most recently available nationwide clinical (hospitalization records) and demographic data. Population data were obtained from the National Institute for Statistics (ISTAT) for each of the considered years [1].
Hip fractures were defined by the following ICD-9CM diagnosis codes (major diagnosis): 820.0–820.1 (femoral neck fractures), 820.2–820.3 (per-trochanteric femoral fractures), and 820.8, 820.9, and 821.1 (other femoral fractures). Data were stratified by gender and into three age groups (65–74 and ≥75 years) and were processed using Stata (StataCorp, College Station, USA) and Excel (Microsoft, Redmond, USA) softwares. Hip fractures in patients aged 45 to 64 represented about 8% of all fractures and were excluded from the analysis as conservatively considered as unlikely to be osteoporotic. We performed descriptive statistical analyses of the incidence in each gender and age subgroup across the six examined years. Analyses of direct costs were based on the costs ascribed to diagnosis-related groups (DRGs), according to the Ministerial Decree DM 549 of 30 June 1997. This law defined the national DRG rate list adopted during the 6 years examined in our study, whose values have been only slightly revised after 2005. However, the Italian system allows each region to drop the DRG value at the local level and the average reduction adopted is about 15%. Therefore, in the present analysis, we used the 1997 DRG rates reduced by 15% in order to be more conservative. DRGs considered relevant to hip fractures were: 209 (surgical procedures on major joints and hip replacement), 210–211 (hip and femur surgery), and 235–236 (hip, femur, or pelvis fractures). Because not all patients assigned these DRGs had a main diagnosis of hip fracture (i.e., osteoarthritis accounts for a substantial number of hip replacements), we asked the Ministry of Health to determine the percentage of costs due to hip fracture for each DRG. The analysis was performed for patients living in Lazio (including Rome), a region with 5.3 million inhabitants, with an aging index comparable to the national average [1] and a number of large hospital and orthopedic centers. The information provided by the Ministry of Health was consistent with the findings we obtained on a smaller sample of almost one million people assisted by the local health authority of Lecce [19]. According to this analysis performed by the Ministry of Health, 30% of costs ascribed to DRG 209 and 80% of costs ascribed to DRGs 210, 211, plus 100% of DRGs 235 and 236 were attributable to a main diagnosis of hip fracture. We considered these rates to represent the weight of hip fracture-related costs for each DRG. The analysis of direct costs was conducted assuming that the length of hospitalization for hip fractures did not exceed the average values calculated in the DRG rates. Table 1 resumes the cost parameters considered for DRGs analysis.
Although our study intended to focus on hospitalization costs, because they could be more accurately measured thanks to the availability of institutional databases (i.e., hospitalization records), we have also provided a detailed estimation of rehabilitation costs following hip fractures, as they are supposed to be at least comparable to the costs directly related to hospitalization [5]. This secondary cost analysis was carried out according to the most recently published Italian data and official rate lists (Fig. 1). First of all, we assumed that 5% of patients currently die few days after the fracture (acute mortality rate) [5, 6, 20, 21]. Among the patients who survive (95% of people hospitalized), 13.5% begin immediately 1-month in-hospital intensive rehabilitation programs (average cost—6,600 Euros/subject) [22, 23]. At the end of this in-hospital intensive rehabilitative period, 10% of these patients move to long-term facilities after leaving the hospital (average yearly cost—9,920 Euros/patient) [22, 23]. We have then to consider that 18.2% of the subjects who survived (namely 95% of people hospitalized) become directly institutionalized because of the hip fracture (9,920 Euros/patient) [22] and that 63% of these people immediately treated in nursing homes undergo in-hospital rehabilitation (6,600 Euros/patient) [22] at the end of the institutionalization period [22]. All the remaining patients (63.3% of patients discharged alive from the hospital) enter the home-based rehabilitation program provided by the Italian Local Health Authorities, which consists in a 3-month therapeutical cycle (2,304 Euros/patient, according to the Regional healthcare services rate lists and to the Italian Society of Rehabilitative Medicine, SIMFER) [22]. Furthermore, within 6 months from their hospitalization, 13.2% of the overall fractured people discharged alive from the hospital are treated at ambulatories ruled by the Local Health Authorities (1,767 Euros/patient) [24], after having completed other kinds of rehabilitative programs (both home-based or in-hospital and nursing homes rehabilitation), but 40% of these patients treated at ambulatorial level need to be hospitalized once again to undergo in-hospital rehabilitation (6,600 Euros/patient) [22]. Social costs, indirect costs, and those related to the loss of productivity of patients and their relatives were not computed in this study.

Flow chart showing the percentages used for the different rehabilitative outcomes of fractured patients
Results
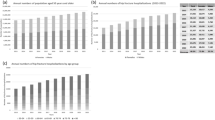
The total number of hip fractures which occurred in Italy among people ≥65 years of age between 2000 and 2005 is 507,671, as resulted by the analysis of hospitalization records concerning the ICD-9CM diagnosis codes considered. Hip fractures were 73,493 in year 2000 (16,037 men and 57,456 women), 78,354 in year 2001 (16,869 men and 61,485 women), 80,804 (17,297 men and 63,507 women) in year 2002, 89,796 (19,720 men and 70,076 women) in year 2003, 90,753 (19,872 men and 70,881 women) in 2004 and rose up to 94,471 in 2005 (20,909 men and 73,562 women), with an overall increase of 28.5% over 6 years (Table 2).
Considering all 6 years together, 82.9% of total hip fractures occurred in patients 75 years of age or older (n = 420,890 fractures), with women accounting for 78.2% of all fractures (n = 396,967). Among women, 84.2% of hip fractures (n = 334,223) were experienced by patients ≥75 years of age (Table 2). The number of fractures in this subgroup of women increased by 28.0% over 6 years and accounted for 68.6% of the overall observed increase in the total number of hip fractures between 2000 and 2005 (Table 2). In the same period, hip fractures in men passed from 16,037 cases in year 2000 to 20,909 in year 2005, with an increase of 30.3% over 6 years. Hip fractures occurred in men aged ≥75 years increased by 33.1% reaching a total of 16,540 cases in 2005 vs. 12,426 fractures of year 2000 (Table 2). Breakdown by age and gender confirmed the marked increase with age and the predominance of women. The incidence of hip fractures observed among women was three or four times higher than that of men in the two older age groups, with a progressive increase between 2000 and 2005 for both genders, particularly in the oldest age group.
Also the incidence of hip fractures per 10,000 inhabitants has increased year by year between 2000 and 2005, with this trend being marked in people aged 75 years and over (Table 3). For this age group, the incidence per 10,000 men was 91.9 in 2005 vs. 77.9 of year 2000, showing an increase of 17.9%. The incidence per 10,000 women aged ≥75 was 196.7 in year 2005 vs. 165.8 of year 2000, corresponding to an increase of 18.6% across 6 years. The incidence per 10,000 inhabitants increased also in the age group 65–74, passing within 6 years from 29.8 to 34.8 (+16.7%) and from 13.9 to 16.2 (+16.5%) in women and in men, respectively (Table 3). The mean duration of hospitalization ranged from 14.0 to 16.7 days for all age and gender categories in each year examined, thus not exceeding the allowed average values provided by the DRGs official rate list (Table 1).
Direct hospitalization costs of hip fractures occurred in adult patients aged ≥45 increased from 442 to 548 million Euros (+23.9% across 6 years), with elderly people accounting for approximately 83% of these total costs (Table 4). As shown in Table 4, direct costs sustained for hip fractures occurred in people aged ≥65 were estimated in 343 million Euros in year 2000, 373 million in 2001, 394 million in 2002, 433 million in 2003, 448 million in 2004, and 467 million in 2005 (+36.1% across 6 years). Pooling together data concerning all the six examined years, hospitalizations due to hip fractures in the elderly resulted in expenditures for approximately 2.5 billion Euros, which need to be added to rehabilitation costs. Table 5 summarizes direct costs sustained for hospitalizations and rehabilitation costs due to hip fractures in people aged ≥65 from 2000 to 2005. Rehabilitation costs have been found to be higher than hospitalization costs, and were estimated in 392 million Euros in year 2000, 418 million in 2001, 431 million in 2002, 480 million in 2003, 485 million in 2004, and 531 million in 2005 (Table 5). Rehabilitation costs increased by 35.4% across 6 years and represented more than 50% of total direct costs. As shown in Table 5, overall direct costs sustained both for hospitalizations and rehabilitation following hip fractures occurred in elderly people were estimated in 735 million Euros in year 2000, 791 million in 2001, 825 million in 2002, 913 million in 2003, 933 million in 2004, and almost one billion Euros in year 2005.
Discussion
This Italian study is of special interest because it has been carried out analyzing the national hospitalization database; thus, the data reported should be regarded as estimates closely reflecting the real situation. We believe that hospitalizations due to hip fractures registered in the national database at the Ministry of Health represent the best possible surrogate of fractures true incidence. The analysis of hospitalization records is a methodology that have been used in recent years by several authors from different countries (Switzerland, France, Germany, Austria, Italy), in order to closely determine the incidence of hip fractures and cardiovascular diseases [5, 19, 25–30]. Moreover, a British study has found an excellent accuracy and reliability of the clinical indicators related to hip fractures hospitalization records [31]. However, it should be considered that a small proportion of hospitalizations (possibly 3–5%) may represent readmissions for the same persons, and a very small number of hip fractures may not result in hospitalization. It is also important to point out the assumption that in this analysis, all hip fractures were considered, independently of underlying osteoporosis or not, and no osteoporosis attribution rates were applied because it still does not exist a specific codification for osteoporotic fractures. On the other hand, the most frequent underlying cause of hip fractures in the elderly (which represent the majority of cases recorded in the hospitalization database) is osteoporosis, and almost 83% of hip fractures were found to have been experienced by patients 75 years of age or older, in accordance with the higher prevalence of osteoporosis in this age group [5]. It must be pointed out also that we included in the analysis also the ICD9-CM codes 821, which comprises fractures of the femoral shaft (and other not defined hip fractures), whereby 821.0 are closed fractures and 821.1 are open fractures (generally high energy trauma fractures). However, their number in the elderly population represented a small percentage of all hip fractures computed (about 7–8% each year), and patients with osteoporosis may also break after a high-energy trauma.
Our findings seem to be consistent with IOF estimations concerning the overall incidence and costs of hip fractures in Italy [32] and provides further detailed information regarding the costs specifically generated by elderly people. Furthermore, these results are consistent with the national hospitalization database analyses of the surgical interventions following hip fractures we had already performed [18] and with data from other European [27, 33–39] and non-European countries [40, 41], where an increasing trend of hip fractures incidence and costs was shown for many industrialized countries. On the opposite, some previously published studies concerning Sweden [42], Switzerland [30, 43], Australia [44], and Canada [45] have found a reversal in hip fractures incidence, mainly for women. These differences can be explained considering the higher incidence of hip fractures among oldest age groups in those countries where effective preventive strategies have not yet been fully implemented, especially for nursing home residents, whose risk of fractures is two- or threefold higher than community dwelling elderly people [46]. Actually, some authors have suggested that the decrease in secular hip fractures trend observed in some countries may be attributable to the reduction of hip fractures in nursing homes [43].
In line with the commonly accepted approach in health economics, we used DRGs in order to calculate direct costs of hip fractures, for the reason that this method enabled us to accurately measure the financial consequences of hospitalizations. A 15% average reduction for each DRG was adopted in order to overcome the differences between the regions in cutting the national rate-list values. Another main contribution of this manuscript is the attempt (on the basis of the available national literature) of quantifying rehabilitation costs, which were found to be higher than direct hospitalization costs (Table 5). However, there are still many differences between the Italian regions concerning the post-acute treatments, with Northern Italy having a higher number of people institutionalized after hip fracture and more patients staying at home in Southern Italy, according to the data provided by the Italian Society of Rehabilitative Medicine.
Although our study was primarily focused on determining the number of hospitalizations and direct costs following hip fractures, a full evaluation of the problem would also require to consider the burden—in terms of health and economic resources—of mortality and disability. The average yearly mortality rate for hip fractures is currently 15–25% [5, 6, 20, 21], and we have computed that no less than 120,000 people died in Italy because of hip fractures from year 2000 to 2005. It has also been estimated that each year 18,000 patients become disabled as a consequence of hip fracture, generating yearly costs (financial aid provided by the State) of 80–100 million Euros [2]. Furthermore, long-term costs related to hip fractures occurred in previous years should also be considered for a detailed cost analysis, as assessed in other European studies [47]. Indirect costs related to hip fractures are not easily assessable, although the International Osteoporosis Foundation (IOF) has estimated them to account for 20% of overall direct costs [3]. In this perspective, total costs generated by hip fractures in the elderly Italian population are now estimated to exceed 1.3 billion Euros/year. Our study confirms the findings of our previous analyses [5, 17, 18] and highlights the high social impact of hip fractures in elderly people. However, the large database of the Italian hospital records offers the opportunity of new studies concerning the differences across hip fracture types, such as between neck and trochanter fractures, which could be of particular interest especially for orthopedic surgeons.
Conclusion
According to our estimations, overall direct costs (due both to hospitalizations and rehabilitation) sustained in Italy for hip fractures in the elderly are now close to one billion Euros/year, showing a continuous increasing trend from 2000 to 2005. This study shows that in the Italian population aged ≥65, hospitalizations following hip fracture and their related costs are growing progressively, representing a serious medical and public health problem. Italy, such as all industrialized countries where the number of elderly people is still increasing, should, therefore, adopt adequate preventive strategies aimed to reduce the risk of hip fractures (i.e., osteoporosis prevention and fall prevention), especially in the oldest age groups.
References
National Institute for Statistics (2005) Italian Statistics. National Institute for Statistics, Rome
WHO statistical information system (WHOSIS), http://apps.who.int/whosis/database/life_tables/life_tables_process.cfm?path=whosis,life_tables&language=english
Italian Senate Health Commission (eds) (2002) Official Report of the Survey on Osteoporosis. Italian Senate, Rome
Kanis JA et al (2008) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 19(4):399–428
Piscitelli P, Guida G, Iolascon G et al (2007) Incidence and costs of hip fractures vs. acute myocardial infarction in the Italian population: a 4 years survey. Osteoporos Int 18:211–219
Keene GS, Parker MJ, Pryor GA (1993) Mortality and morbidity after hip fractures. BMJ 307:1248–1250
Meyer HE, Tverdal A, Falch JA, Pedersen JI (2000) Factors associated with mortality after hip fracture. Osteoporos Int 11:228–232
Hagsten B et al (2006) Health-related quality of life and selfreported ability concerning ADL and IADL after hip fracture: a randomized trial. Acta Orthop 77(1):114–119
Di Monaco M et al (2006) Muscle mass and functional recovery in women with hip fracture. Am J Phys Med Rehabil 85(3):209–215
Zimmermann S et al (2006) The lower extremity gain scale: a performance-based measure to assess recovery after hip fracture. Arch Phys Med Rehabil 87(3):430–436
Latham NK (2006) Pattern of functional change during rehabilitation of patients with hip fracture. Arch Phys Med Rehabil 87(1):111–116
Adami S, Giannini S, Giorgino R et al (2003) The effect of age, weight, and lifestyle factors on calcaneal quantitative ultrasound: the ESOPO study. Osteoporos Int 14:198–207
Siris ES, Brenneman SK, Barrett-Connor E, Miller PD, Sajjan S, Berger ML, Chen YT (2006) The effect of age and bone mineral density on the absolute, excess, and relative risk of fracture in postmenopausal women aged 50–99: results from the National Osteoporosis Risk Assessment (NORA). Osteoporos Int 17(4):565–574
Krieg MA, Cornuz J, Ruffieux C et al (2006) Prediction of hip fracture risk by quantitative ultrasound in more than 7000 Swiss women > or =70 years of age: comparison of three technologically different bone ultrasound devices in the SEMOF study. J Bone Miner Res 21(9):1457–1463
Maggi S et al (2006) Quantitative heel ultrasound in a population-based study in Italy and its relationship with fracture history: the ESOPO study. Osteoporos Int 17:237–244
Riggs BL, Melton LJ 3rd (1995) The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone 17(5 Suppl):505S–511S17
Iolascon G, Guida G et al (2007) Hip fractures in Italy, analysis of DRG data. Aging Clin Exp Res 19(3):2–4
Piscitelli P, Iolascon G, Guida G et al (2005) Femoral fractures and orthopaedic surgery in Italy. J Orthopaed Traumatol 6:202–205
Piscitelli et al (2006) Incidence and costs of hip fractures vs. acute myocardial infarction in the population of Local Health Authorities ASL Lecce/1 and ASL Lecce/2: a 2 years survey. Ital J Public Health 3(2):75–77 Year 4
Browner WS, Pressman AR, Nevitt MC, Cummings SR (1996) Mortality following fractures in older women. The study of osteoporotic fractures. Arch Intern Med 156:1521–1525
Center JR, Nguyen TV, Schneider D et al (1999) Mortality after all major types of osteoporotic fracture in men and women: an observational study. Lancet 353(9156):878–882
Tediosi F et al (2003) La valutazione economica dei percorsi assistenziali dei soggetti con Ictus e frattura femore in toscana. Mecosan 48(1):67–82 article in Italian
Visentin P, Ciravegna R, Fabris F (1997) Estimating the cost per avoided hip fracture by osteoporosis treatment in Italy. Maturitas 26:185–192
Tediosi F et al (2004) L'assistenza ospedaliera e riabilitativa per le fratture osteoporotiche in Toscana. Polit Sanit 5(2):61–69 (article in Italian)
Icks A, Haastert B, Becker C, Meyer G (2008) Trend of hip fracture incidence in Germany 1995–2004: a population-based study. Osteoporos Int 19:1139–1145
Maravic M, Le Bihan C, Landais P, Fardellone P (2005) Incidence and cost of osteoporotic fractures in France during 2001. A methodological approach by the national hospital database. Osteoporos Int 16:1475–1480
Mann E, Icks A, Haastert B, Meyer G (2009) Hip fracture incidence in the elderly in Austria: an epidemiological study covering the years 1994 to 2006. BMC Geriatr 8:35 2008
Caldarola P, Cuonzo M et al (2008) Epidemiology of heart failure in Apulia Region. G Ital Cardiol 10:135–139
Lippuner K, von Overbeck J, Perrelet R et al (1997) Incidence and direct medical costs of hospitalizations due to osteoporotic fractures in Switzerland. Osteoporos Int 7:414
Lippuner K et al (2005) Epidemiology and direct medical costs of osteoporotic fractures in men and women in Switzerland. Osteoporos Int 16(SUP 2):S8–S17
Pervez H, Bhargwa A, Parker MJ (2003) Accuracy and reliability of the clinical indicators related to hip fractures. Injury 34:522–524
International Osteoporosis Foundation (2002) Osteoporosis in the European Community: a call for action. International Osteoporosis Foundation, Lyon
Autier P, Haentjens P, Bentin J et al (2000) Costs induced by hip fractures: a prospective controlled study in Belgium. Belgian Hip Fracture Study Group. Osteoporos Int 11:373–380
Dolan P, Torgerson DJ (1998) The cost of treating osteoporosis fractures in the United Kingdom female population. Osteoporos Int 8:611–617
Johnell O, Gullberg B, Allander E, Kanis JA (1992) The apparent incidence of hip fracture in Europe: a study of national register sources.MEDOS Study Group. Osteoporos Int 2:298–302
Vestergaard P, Rejnmark L, Mosekilde L (2008) Strongly increasing incidence of hip fractures in Denmark from 1977 to 1999. Ugeskr Laeger 170:621–623
Hernandez JL, Olmos JM, Alonso MA, Gonzales-Fernandez CR, Martinez J, Pajaron M, Llorca J, Gonzales-Macias J (2006) Trend in hip fracture epidemiology over a 14-year period in a Spanish population. Osteoporos Int 17:464–470
Lönnroos E, Kautianinen H, Karppi P, Huusko T, Kiviranta I, Sulkava R (2006) Increased incidence of hip fractures. A population based-study in Finland. Bone 39:623–627
Bjorgul K, Reikeras O (2007) Incidence of hip fracture in southeastern Norway. Int Orthop 31:665–669
Ray NF, Chan JK, Thamer M, Melton LJ 3rd (1997) Medical expenditures for treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res 12(1):24–35
Hagino H, Katagiri H, Okano T, Yamamoto K, Teshima R (2005) Increasing incidence of hip fracture in Tottori Prefecture, Japan: trend from 1986 to 2001. Osteoporos Int 16:1963–1968
Löfmann O, Berglund K, Larsson L, Toss G (2002) Changes in hip fracture epidemiology: redistribution between ages, genders and fracture types. Osteoporos Int 13:18–25
Chevalley T, Guilley E, Herrmann FR, Hoffmeyer P, Rapin CH, Rizzoli R (2007) Incidence of hip fracture over a 10-year period (1991–2000): reversal of a secular trend. Bone 40:1284–1289
Chang KP, Center JR, Nguyen TV, Eisman JA (2004) Incidence of hip and other osteoporotic fractures in elderly men and women: Dubbo Osteoporosis Epidemiology Study. J Bone Miner Res 19:532–536
Jaglal SB, Weller I, Mamdani M, Hawker G, Kreder H, Jakkimainen L, Adachi JD (2005) Population trends in BMD testing, treatment, and hip and wrist fracture rates: are the hip fracture projections wrong? J Bone Miner Res 20:898–905
Sugarman JR, Connell FA, Hansen A, Helgerson SD, Jessup MC, Lee H (2002) Hip fracture incidence in nursing home residents and community-dwelling older people, Washington State, 1993–1995. J Am Geriatr Soc 50:1638–1643
Borgstrom F et al (2007) The societal burden of osteoporosis in Sweden. Bone 40(6):1602–1609
Acknowledgments
We thank Dr. L. Lispi and D. Del Gigante (General Direction for Planning Affairs, Italian Ministry of Health) for their help in the analysis of national hospitalization data. Many thanks to the CERSUM research group on osteoporosis (Euro Mediterranean Scientific Biomedical Institute, ISBEM/IFC CNR, Brindisi).
Conflicts of interest
AD, AM, SG, PM, MM, EQ, FC, FF, GC, MLB, GC, AG, GG, RG, GI have received research grant and funding for consulting/speaking by Merck, Sanofi-Aventis, Novartis, Stroder-Servier, Procter & Gamble, Ely Lilly, Roche, Glaxo; PP has received once funding for consulting/speaking by Sanofi-Aventis; FG, AM, GC, MC, LDP, MB, ES, OB, BF: no disclosures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Piscitelli, P., Gimigliano, F., Gatto, S. et al. Hip fractures in Italy: 2000–2005 extension study. Osteoporos Int 21, 1323–1330 (2010). https://doi.org/10.1007/s00198-009-1084-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-009-1084-x