
Abstract
Introduction
Kyphoplasty has been shown to restore vertebral height and sagittal alignment. Proponents of vertebroplasty have recently demonstrated that many vertebral compression fractures (VCFs) are mobile and positional correction can lead to clinically significant height restoration. The current investigation tested the hypothesis that positional maneuvers do not achieve the same degree of vertebral height correction as kyphoplasty balloon tamps for the reduction of low-energy VCFs.
Methods
Twenty-five consecutive patients with a total of 43 osteoporotic VCFs were entered into a prospective analysis. Each patient was sequentially evaluated for postural and balloon vertebral fracture reduction. Preoperative standing and lateral radiographs of the fractured vertebrae were compared with prone cross-table lateral radiographs with the patient in a hyper-extension position and on pelvic and sternal rolls. Following positional manipulation, patients underwent a unilateral balloon kyphoplasty. Postoperative standing radiographs were evaluated for the percentage of height restoration related to positioning and balloon kyphoplasty.
Results
In the middle portion of the vertebrae, the percentage available for restoration restored with extension positioning was 10.4% (median 11.1%) and after balloon kyphoplasty was 57.0% (median 62.2%). This difference was statistically significant (p<0.001). Thus, kyphoplasty provided an additional 46.6% of the height available for restoration from the positioning alone. With operative positioning, 51.2% of VCFs had >10% restoration of the central portion of the vertebral body, whereas 90.7% of fractures improved at least 10% following balloon kyphoplasty (p<0.002).
Conclusion
Although this study supports the concept that many VCFs can be moved with positioning, balloon kyphoplasty enhanced the height reduction >4.5-fold over the positioning maneuver alone and accounted for over 80% of the ultimate reduction. If height restoration is the goal, kyphoplasty is clearly superior in most cases to the positioning maneuver alone.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Vertebral compression fractures (VCFs) are common and have an estimated incidence of 700,000 per year in the United States [1]. VCFs are usually caused by osteoporosis and, as the population continues to age, the incidence of osteoporotic VCFs is likely to increase 4-fold during the next 50 years [2]. Nonsurgical treatment of VCFs includes analgesics, initial bed rest, initiation of osteoporosis medication, and, ultimately, physical therapy [3]. Despite appropriate treatment and therapy, over a third of VCFs become chronically painful [2, 4]. To address this problem, minimally invasive techniques such as vertebroplasty and kyphoplasty have been developed to reduce fracture-related pain and have been shown to be effective in the short term [3, 5–11].
Vertebroplasty has been performed in the United States since 1993 and involves the percutaneous injection of bone cement into a collapsed vertebral body. Numerous reports have demonstrated statistically significant pain relief and the restoration of activities of daily living after undergoing vertebroplasty [3, 6, 7, 12]. However, vertebroplasty does not expand the collapsed vertebral body and depends on positioning to address spinal deformity. In the osteoporotic spine, a kyphotic deformity alters the biomechanical environment and may favor additional fractures [13, 14]. This led to the development of kyphoplasty, which combines vertebroplasty with balloon angioplasty [10]. Using a transpedicular or extrapedicular route, a cannula is introduced into the vertebral body, followed by the insertion of an inflatable bone tamp, which directly reduces the fracture and restores vertebral body height prior to the injection of cement. Initial studies have shown good clinical results, along with the restoration of vertebral body height [9, 15–17]. Lieberman et al. reported on 70 consecutive kyphoplasty procedures and found that 70% of the vertebral bodies gained 47% of their lost height. In addition, the balloon tamp creates a preformed low-pressure cavity and, thus, carries a lower risk of cement extravasation [11]. For these reasons, some authors have advocated that kyphoplasty is a superior surgical technique compared to vertebroplasty because it addresses both fracture-related pain and associated spinal deformity by using an inflatable bone tamp [10, 11]. Other authors have advocated that vertebroplasty is a superior procedure because it is a quicker and less expensive procedure. In addition, it has recently been demonstrated that many VCFs are mobile and positional correction can lead to clinically significant height restoration without the use of a balloon tamp [18]. The purpose of this study was to test the hypothesis that positional maneuvers do not restore the same magnitude of vertebral height as kyphoplasty balloon tamps in the reduction of low-energy VCFs.
Methods
Twenty-five consecutive patients who met the protocol inclusion criteria and subsequently underwent balloon kyphoplasty were evaluated prospectively following approval by the Institutional Review Board. These criteria included the presence of an osteoporotic VCF, with persistent pain graded at least 4 out of 10, which was refractory to a minimum of 4 weeks of conservative therapy, and preoperative, intraoperative, and postoperative imaging studies. Initial management included short-term bed rest, physical therapy with extension exercises, anti-inflammatory medication, and narcotics. This patient cohort had a total of 43 VCFs. All patients had a magnetic resonance imaging (MRI) scan performed and had evidence of edema in the fractured vertebral body on T2-weighted images. Laboratory values were evaluated to rule out other associated conditions, such as osteomalacia, endocrinopathy, or malignancy. Malignancy-associated VCF was an exclusion criteria and only those patients with osteoporotic VCFs were included in this study.
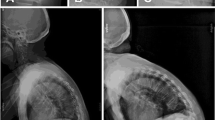
All patients had preoperative standing anterior–posterior (AP) and lateral radiographs, which were centered on the fractured vertebra. Based on these radiographs, an independent observer not involved in the surgery determined the nearest nonfractured, nonmobile vertebra (reference vertebra) and measured the anterior, posterior, and middle areas of this body to the nearest millimeter, based on the techniques used by Faciszewski and McKiernan [19] and McKiernan et al. [20]. These values were then compared to the fractured (index) level(s) and a percentage was obtained for each of the three areas of the vertebral body.
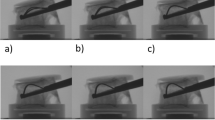
At the time of surgery, patients were placed in the prone position with a bolster placed under the sternum and pelvis to maintain an extension position in order to reduce the kyphotic deformity. While in this position, anteroposterior (AP) and lateral fluoroscopic images were obtained. A percentage was calculated from the intraoperative radiographs using the height of the same “normal vertebral body” versus the anterior, posterior, and middle borders of the fractured vertebral body. These values were used to calculate the percentage restoration relative to lost vertebral height and the percentage restoration relative to referent vertebral height. The height gained during this positioning portion of the procedure was considered to be solely due to dynamic fracture mobility.
After the positioning portion of the study was performed, an incision was made in order to percutaneously place an inflatable bone tamp (IBT) into the fractured vertebral body via a unipedicular approach. Bone tamp inflation was performed to elevate the depressed vertebral body end plate to restore height and to create a cavity for cement placement. After the reduction was complete, methylmethacrylate cement was inserted using a syringe into the vertebral body. The patients were admitted to the hospital overnight and postoperative standing radiographs were taken and evaluated for the percentage of height restoration relative to lost vertebral height and the percentage restoration relative to referent vertebral height. The additional height gained during this portion of the procedure was attributed to the kyphoplasty procedure.
In order to calculate the digitization precision error, 18 randomly selected nonfractured and fractured vertebral bodies were measured in three dimensions. From these values, the coefficient of variation (%CV) and standard deviation (SD) were obtained. To test for precision in measurements, we used the intra-class correlation. Paired-samples 2-tailed t-tests were used to test differences after kyphoplasty, with the level of statistical significance set at 0.05.
Results
The mean patient age was 71 years and 21 patients (84%) were women. The mean fracture age was 340 days. Four patients (16%) had fractures less than 3 months old and 21 patients (84%) with fractures greater than 3 months old. There were no instances of death, symptomatic pulmonary embolism, or neurologic injury following the procedure. Asymptomatic cement leakage occurred in 8% of patients.
Digitization precision errors expressed as %CV were 4.1%, 4.4%, and 3.1% for the anterior, middle, and posterior portions of the vertebral body, respectively. The standard deviations were 0.5 mm, 0.5 mm, and 0.4 mm for the anterior, middle, and posterior portions of the vertebral body, respectively. The intra-class correlations were 0.95, 0.9, and 0.98 for the anterior, medial, and posterior portions of the vertebral body, respectively.
The absolute height restored, calculated as a percentage of the adjacent vertebral body, was calculated. This measurement did not take into account the amount of height lost preoperatively, but only the absolute amount of correction achieved. The average preoperative vertebral height in the anterior portion of the vertebral body was 64%, which increased to 66% after extension positioning (range 27% to 100%; median 66%), but the change was not statistically significant (p=0.26). After kyphoplasty, the height increased to 75% of the normal vertebral body (range 25% to 100%; median 73%) following kyphoplasty. The additional height gained from kyphoplasty was statistically significant (p<0.001).
The average preoperative vertebral height in the central portion of the vertebral body was 60.1%. After extension positioning, the central height increased to an average of 66.2% (range 27% to 97%; median 68%), which was statistically significant (p=0.006). After kyphoplasty, the central height further increased to an average of 82.3% (range 42% to 100%; median 88%). This additional 16% height increase gained following kyphoplasty was significant (p<0.001). With operative positioning, 51.2% of VCFs had >10% restoration of the central portion of the vertebral body, compared with 90.7% after balloon kyphoplasty.
The average preoperative vertebral height in the posterior portion of the vertebral body was 89%. After extension positioning, the posterior height remained at 89% (range 67% to 100%; median 90%). After kyphoplasty, the posterior height increased to an average of 92% (range 64% to 100%; median 95%) (p=0.017).
In the anterior portion of the vertebrae, the average preoperative fractured vertebral body height compared to the referent vertebral body was 64%, and an average of 36% percent was available for restoration. Postural maneuvering, based on the intraoperative radiographs with the patient in the extension position, on average, restored 1% (range −288% to 87%; median 14%) of the percentage available for restoration. After kyphoplasty was performed, an average of 29% (range −30% to 100%; median 22%) of the percentage height available for restoration was restored. This difference was statistically significant (p=0.002). Thus, while positioning provided an average of 1% restoration, kyphoplasty provided an additional 28% restoration in the anterior portion of the vertebrae.
In the middle portion of the vertebrae, the average preoperative fractured vertebral body height compared to a referent vertebrae was 60.1%. Thus, the average percentage available for restoration was 39.9%. Postural maneuvering, based on the intraoperative radiographs with the patient in the extension position, on average, restored 10.4% (range −132% to 92%; median 11.1%) of the percentage available for restoration. After kyphoplasty was performed, on average, 57.0% (range −46% to 100%; median 62.2%) of the percentage height available for restoration was restored, which was significantly greater than with extension positioning alone (p<0.001) (Fig. 1). Thus, while positioning provided an average of 10.4% restoration, kyphoplasty provided an additional 46.5% restoration in the central portion.

Percentage of the height available for restoration restored of the anterior, medial, and posterior vertebral body height
In the posterior portion of the vertebrae, the average preoperative fractured vertebral body height compared to the referent vertebrae was 89%, leaving 11% available for restoration. After extension positioning, the fractured vertebrae lost an average of additional 5% of the height available for restoration (range −233% to 100%; median 0%) After kyphoplasty was performed, an average of 20% (range −168% to 100%; median 0%) of the percentage height available for restoration was restored, which was statistically greater than with extension alone (p=0.023).
Discussion
Proponents of vertebroplasty have recently demonstrated that many VCFs are mobile and positional correction can lead to clinically significant height restoration [18]. A recent study by McKiernan et al. demonstrated that 50% of patients presenting for vertebroplasty had evidence of one or more mobile fractures. Anterior vertebral height in these fractures doubled postoperatively and improved to more than 70% of normal [18]. The drawback to their study was that patients were positioned in the supine position with a 4-inch foam bolster in place to allow gravity-assisted vertebral extension. Although this demonstrates fracture mobility, this is not the position used intraoperatively to reduce the fracture. Our study, in which patients were placed in the prone position with bolsters beneath the sternum and pelvis, also supports this concept that many VCFs can be partially reduced with extension positioning alone. After positioning, the central vertebral body height increased to an average of 66.2%, which was statistically significant. In addition, in the central portion of the vertebral body, at least half of the fractures gained 10% or more in height.
Despite the fact that many VCFs can be moved with positioning, our hypothesis was that positional maneuvers alone, as are performed during vertebroplasty, do not achieve the same degree of vertebral height correction as kyphoplasty balloon tamps for the reduction of low-energy VCFs. Our data supports this hypothesis because balloon kyphoplasty enhanced the height reduction >4.5-fold over the positioning maneuver alone and accounted for over 80% of the ultimate reduction. Even in those patients with marked positional improvement, kyphoplasty provided statistically significant additional height restoration of all segments of the vertebral body. If height restoration is the goal, kyphoplasty is clearly superior in most cases to the positioning maneuver alone.
Anatomic reduction is a cardinal principle of fracture treatment, and it is intuitive to try and restore vertebral body height; however, restoration of vertebral body height has not yet been shown to result in additional pain relief or benefit the quality of life in patients with osteoporotic VCFs. Our results demonstrate that kyphoplasty enhances reduction compared to postural positioning alone. However, this was not a clinical study, and we cannot conclude if this additional height corresponded to any additional pain relief. For example, in the anterior portion of the vertebral body, kyphoplasty provided an average improvement of 9% of vertebral body height compared to postural positioning and an improvement in 16% in the medial portion of the vertebral body. Although these numbers are statistically significant, we cannot conclude that this percentage of vertebral body height restoration is clinically significant. In addition, this was a short-term radiographic study and further studies are warranted in order to determine if the additional height restoration obtained during kyphoplasty is maintained in the long term.
Another limitation of this study was that all of our kyphoplasty procedures were performed using a unipedicular approach. The current gold standard technique for the kyphoplasty procedure is to use the bipedicular approach. A recent study using a bipedicular approach was performed by Crandall et al. and demonstrated similar results with the restoration of 58–86% of normal vertebral body height in acute fractures and the restoration of 56–79% restoration in chronic fractures [5]. They concluded that fracture reduction was most effective in the acute stage. Our results compared to the recent literature demonstrate that the unipedicular approach may be as effective compared to a bipedicular approach and is less expensive and less time consuming. Recent cadaveric studies concluded that there were no differences between the mechanical strength or height attained between bilateral and unilateral vertebroplasty procedures and that there was no greater risk for the noncemented side to toggle in the coronal plane [21, 22]. Further studies are indicated to determine if a unipedicular approach is similar in effectiveness compared to using two balloon tamps.
In conclusion, kyphoplasty affords approximately an 80% enhanced reduction over postural positioning alone. In those fractures where height restoration is desired, kyphoplasty is a reliable and safe method to rectify the vertebral status.
References
Riggs BL, Melton LJ 3rd (1986) Involutional osteoporosis. N Engl J Med 314(26):1676–1686
Riggs BL, Melton LJ 3rd (1995) The worldwide problem of osteoporosis: Insights afforded by epidemiology. Bone 17(5 Suppl):505S–511S
Watts NB, Harris ST, Genant HK (2001) Treatment of painful osteoporotic vertebral fractures with percutaneous vertebroplasty or kyphoplasty. Osteoporosis Int 12(6):429–437
Lyles KW, Gold DT, Shipp KM, Pieper CF, Martinez S, Mulhausen PL (1993) Association of osteoporotic vertebral compression fractures with impaired functional status. Am J Med 94(6):595–601
Crandall D, Slaughter D, Hankins PJ, Moore C, Jerman J (2004) Acute versus chronic vertebral compression fractures treated with kyphoplasty: early results. Spine J 4(4):418–424
Evans AJ, Jensen ME, Kip KE, DeNardo AJ, Lawler GJ, Negin GA, Remley KB, Boutin SM, Dunnagan SA (2003) Vertebral compression fractures: pain reduction and improvement in functional mobility after percutaneous polymethylmethacrylate vertebroplasty—retrospective report of 245 cases. Radiology 226(2):366–372
Mathis JM, Barr JD, Belkoff SM, Barr MS, Jensen ME, Deramond H (2001) Percutaneous vertebroplasty: a developing standard of care for vertebral compression fractures. Am J Neuroradiol 22(2):371–381
Mathis JM, Ortiz AO, Zoarski GH (2004) Vertebroplasty versus kyphoplasty: a comparison and contrast. Am J Neuroradiol 25(5):840–845
Phillips FM, Ho E, Campbell-Hupp M, McNally T, Todd Wetzel F, Gupta P (2003) Early radiographic and clinical results of balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Spine 28(19):2260–2267
Lieberman IH, Dudeney S, Reinhardt MK, Bell G (2001) Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine 26(14):1631–1638
Lieberman I, Reinhardt MK (2003) Vertebroplasty and kyphoplasty for osteolytic vertebral collapse. Clin Orthop 415(Suppl):S176–S186
Barr JD, Barr MS, Lemley TJ, McCann RM (2000) Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine 25(8):923–928
Belmont PJ Jr, Plly DW Jr, Cunningham BW, Klemme WR (2001) The effects of hook pattern and kyphotic angulation on mechanical strength and apical rod strain in a long-segment posterior construct using a synthetic model. Spine 26(6):627–635
White AA 3rd, Panjabi MM, Thomas CL (1977) The clinical biomechanics of kyphotic deformities. Clin Orthop 128:8–17
Ledlie JT, Renfro M (2003) Balloon kyphoplasty: one-year outcomes in vertebral body height restoration, chronic pain, and activity levels. J Neurosurg 98(1 Suppl):36–42
Dudeney S, Lieberman IH, Reinhardt MK, Hussein M (2002) Kyphoplasty in the treatment of osteolytic vertebral compression fractures as a result of multiple myeloma. J Clin Oncol 20(9):2382–2387
Rhyne A 3rd, Banit D, Laxer E, Odum S, Nussman D (2004) Kyphoplasty: report of eighty-two thoracolumbar osteoporotic vertebral fractures. J Orthop Trauma 18(5):294–299
McKiernan F, Jensen R, Faciszewski T (2003) The dynamic mobility of vertebral compression fractures. J Bone Miner Res 18(1):24–29
Faciszewski T, McKiernan F (2002) Calling all vertebral fractures classification of vertebral compression fractures: a consensus for comparison of treatment and outcome. J Bone Miner Res 17(2):185–191
McKiernan F, Faciszewski T, Jensen R (2003) Reporting height restoration in vertebral compression fractures. Spine 28(22):2517–2521
Tohmeh AG, Mathis JM, Fenton DC, Levine AM, Belkoff SM (1999) Biomechanical efficacy of unipedicular versus bipedicular vertebroplasty for the management of osteoporotic compression fractures. Spine 24(17):1772–1776
Steinmann J, Tingey CT, Cruz G, Dai Q (2005) Biomechanical comparison of unipedicular versus bipedicular kyphoplasty. Spine 30(2):201–205
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shindle, M.K., Gardner, M.J., Koob, J. et al. Vertebral height restoration in osteoporotic compression fractures: kyphoplasty balloon tamp is superior to postural correction alone. Osteoporos Int 17, 1815–1819 (2006). https://doi.org/10.1007/s00198-006-0195-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0195-x