
Abstract
Introduction
Areal bone mineral density (BMD) and calcaneal quantitative ultrasound (QUS) measures are correlated, and both traits predict osteoporotic fracture risk independently. However, few studies have examined whether common genetic effects (i.e., pleiotropy) exist between these traits in extended families. In this study, we estimated the additive genetic correlation and random environmental correlation between BMD measured at various skeletal sites and calcaneal QUS measures.
Methods
Our sample included 537 adults (251 men and 286 women) from 110 families participating in the Fels Longitudinal Study. Total hip, femoral neck, lumbar spine, and total body BMD were measured using dual energy X-ray absorptiometry. Three measures of calcaneal structure – broadband ultrasound attenuation (BUA), speed of sound (SOS), and quantitative ultrasound index (QUI) – were collected from the non-dominant heel using the Sahara sonometer. Applying a variance components-based maximum likelihood method, we estimated the heritability of each trait and estimated the genetic and environmental correlations between the different BMD and QUS measures.
Results
Heritability estimates were significant for all measures of BMD and QUS ranging from 0.55 to 0.78. Significant non-zero genetic correlations were found between the different BMD and QUS measures. All genetic correlations were also significantly different from 1. Genetic correlations between total hip BMD and each of the QUS measures were 0.63 with BUA, 0.50 with SOS, and 0.56 with QUI. For femoral neck BMD, genetic correlations were similar to those between total hip BMD and QUS measures. Genetic correlations between BMD of the lumbar spine and QUS measures ranged from 0.34 to 0.38, and those between total body BMD and QUS measures, from 0.51 to 0.54. In contrast, all random environmental correlations were not significantly different from zero.
Conclusion
This study demonstrates that BMD and calcaneal QUS measures among healthy men and women are significantly heritable and are, in part, jointly influenced by a common set of underlying genes. Additionally, this study also provides evidence for a unique set of genes that independently influences each individual trait.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Over 34 million people have low bone mass in the United States, and it is estimated that over ten million people age 50 and older will develop osteoporosis in the hip [1, 2]. Fractures are the clinical manifestation of osteoporosis, and one of the most common causes of functional disability and subsequent mortality in aging populations [3]. In recent years, there has been particular interest in understanding the complex genetic nature of bone metabolism to evaluate and reduce the risk of osteoporosis [4].
There are significant genetic influences on areal bone mineral density (BMD) measured using various bone densitometers [4–9], and areal BMD is highly heritable with estimates as high as 0.80 in human twin pair and family studies [6–8]. Other measures of bone strength, including quantitative ultrasound (QUS) measures, are significantly heritable as well [10–12]. QUS measures are correlated with areal BMD and predict osteoporotic fracture risk independent of bone mass [13–16]. We recently reported that QUS measures were significantly heritable in the range of 0.52 to 0.75 for broadband ultrasound attenuation (BUA) and speed of sound (SOS) [10]. Studies of animals and humans have suggested that QUS measures not only assess bone mass but additional properties (e.g., porosity or elasticity) of bone as well [17, 18]. Since these characteristics might be captured by QUS measures, it is reasonable to examine both areal BMD and QUS measures in the assessment of risk and management of osteoporosis [19, 20]. Examining the co-variation between areal BMD and QUS measures may provide more information on the genetic control of different bone characteristics. A few studies have investigated the genetic relationship between these two measures of bone, but these studies used primarily a twin pair study design with known limitations. These studies found genetic correlations of varied magnitude between BMD at various skeletal sites and QUS measured in the heel or forearm [12, 21], and each reported a significant degree of pleiotropy between BMD and QUS measures as well as some unique genetic effects for each trait. For example, Knapp et al. showed that less than 40% of the genetic variance in SOS at the radius was explained by common genes shared with BMD at the same skeletal site [21]. Taking advantage of the extended and nuclear family structure of the Fels Longitudinal Study cohort, the objective of the study reported here was to estimate the heritability of areal BMD measures in the total hip, femoral neck, lumbar spine and total body among white men and women over a wide age range. In addition, we estimated the genetic and environmental correlations between the different measures of bone to assess the extent of common and unique genetic effects between areal BMD and calcaneal QUS measures.
Materials and methods
Study population
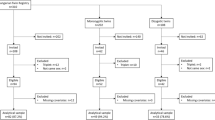
The Fels Longitudinal Study began in 1929 and is the largest and longest running study of human growth, development, and body composition changes over the lifespan [22]. Approximately 1200 serial participants are currently enrolled. Individuals in the Fels Longitudinal Study represent over 200 families, ranging in size from small nuclear families to large, four generation, extended families. There were 608 adults (over 18 years old) with at least one set of concurrent BMD and heel QUS measurements at the same visit between October 1999 and October 2003. We excluded study participants with artificial bone structures (e.g., hip replacement) or with spurious dual energy X-ray absorptiometry (DXA) scans (n=34). A total of 37 individuals who had missing information for smoking, alcohol consumption status, physical activity, or menopausal status were also excluded. This resulted in a total of 537 Caucasian adults aged 18 to 91 years. The 537 individuals in this study sample were from 110 families. Table 1 shows the number and types of relative pairings that exist among the 537 individuals. Informed consent was approved by the Wright State University Institutional Review Board for Human Subjects Research and was obtained from participants.
Bone measurements
Total body areal BMD (in grams per square centimeter) was measured by DXA using a Hologic QDR 4500 Elite densitometer (Hologic, Waltham, MA, USA) following the manufacturer’s protocol. Additionally, lumbar spine (L1–L4) and total hip (femoral neck) BMD were measured. The coefficients of variation (CV) for total body, femoral neck, and lumbar spine were 0.47, 2.37, and 3.13%, respectively.
Three measures of calcaneal structure, BUA (in decibels per hertz), SOS (in meters per second), and quantitative ultrasound index (QUI), were collected in the non-dominant heel using the gel-based Sahara bone sonometer (Hologic). Calibration of the bone sonometer was automatic by the direct apposition of the transducers before positioning of the participants’ heel into the device. The CVs for duplicated measures of BUA, SOS, and QUI were 3.7, 0.22, and 2.6%, respectively [10].
Covariate measurements
Body weight and stature were measured according to standard anthropometric methods [23]. Weight (in kilograms) was recorded to the nearest 0.1 kg at the clinic visit without shoes or heavy clothing, and stature (in centimeters) was measured to the nearest 0.1 cm without shoes. Body mass index (BMI) was calculated from body weight and stature (in kilograms per square meter). Smoking, alcohol consumption status, physical activity, and menopausal status were collected by questionnaire. Current smokers and past smokers of cigarettes, cigars, or pipes were coded as ever-smokers. Alcohol users consumed a 12-oz bottle of beer, 4 oz of wine, or 1 oz of hard liquor once or more weekly. Physical activity was assessed using the sport activity sub-score of the Baecke questionnaire of habitual physical activity [24]. Women who did not menstruate in the 12 months preceding their study visit, or had surgical menopause (i.e., bilateral oophorectomy), were categorized as postmenopausal.
Quantitative genetic analysis
We used a maximum likelihood variance decomposition method for pedigree data to obtain heritability estimates (h 2) of the different measures of bone and to estimate the additive genetic correlation (ρ G ) and random environmental correlation (ρ E ) between the different BMD and QUS measures. Procedures were implemented using Sequential Oligogenic Linkage Analysis Routines (SOLAR v2.12) [25]. In this approach, the covariance matrix for a pedigree is given by:
where Φ is the n×n matrix of kinship coefficients that structures \(\sigma ^{2}_{g} \), the variance due to additive effects of genes; and I is an identity matrix of order n that serves as the structuring matrix for \(\sigma ^{2}_{e} ,\) the variance due to unmeasured, non-genetic factors. Heritability (expressed as \(\left. {{\sigma ^{2}_{G} } \mathord{\left/ {\vphantom {{\sigma ^{2}_{G} } {\sigma ^{2}_{P} }}} \right. \kern-\nulldelimiterspace} {\sigma ^{2}_{P} }} \right)\) is the proportion of the total phenotypic trait variance \({\left( {\sigma ^{2}_{P} } \right)}\) attributable to the additive effects \({\left( {\sigma ^{2}_{G} } \right)}\) of genes. The null hypothesis is that the additive genetic variance \({\left( {\sigma ^{2}_{G} } \right)}\) equals zero. Significance was tested formally by comparing the likelihood of a restricted model in which \(\sigma ^{2}_{G} \) was set to equal zero with that of a model in which \(\sigma ^{2}_{G} \) was estimated. The mean effects of potential covariates were screened for significance (p<0.05) in a similar manner.
Following the initial quantitative genetic analysis, bivariate quantitative genetic analyses between the BMD and QUS measures were performed, also using SOLAR, to determine the extent to which shared genetic and environmental factors influence the covariation of the two sets of phenotypes. Significant covariates from the initial univariate analyses were retained for all bivariate quantitative genetic analyses. For the bivariate analysis, the phenotypic covariance between two individuals for two different traits is given by a 2×2 covariance matrix whose elements were defined as:
where 1 and 2 indicate the two traits of interest (i.e., BMD and QUS), ρ G is the additive genetic correlation between the two traits, and ρ E is the random unmeasured environmental correlation between the traits [26]. The significance of the genetic correlations between BMD and QUS measures was assessed by the likelihood ratio test and by comparing the general model against the nested model where ρ G was constrained to equal zero. A likelihood ratio test of the restricted model that is significantly worse than that of the general models is considered evidence for a significant genetic correlation between the two traits. Similarly, estimates of ρ G not significantly different from 1 represent completely shared genetic effects (i.e., complete pleiotropy). The significance of environmental correlations was also tested in the same manner using the likelihood ratio test by comparing the general model to a nested model with ρ E fixed to zero.
Results
Table 2 presents means and standard deviations for demographic and lifestyle characteristics of the 537 participants. The age of participants ranged from 18 to 91 years, with a mean of 46.2 years and a standard deviation of 16 years. Age was not different between sexes, but men were significantly heavier and taller than women. There was no significant difference in the level of BMI between men and women. Men were more commonly ever-smokers and consumed alcohol more regularly than women (p<0.05). For bone mass measures, all BMD means were higher among men than among women. For the QUS measures, only the BUA mean was significantly higher in men than women.
Table 3 shows the heritability estimates for all traits examined. All heritability (h 2) estimates were significant(p<0.000001): h 2=0.68 for the total hip, h 2=0.67 for the femoral neck, h 2=0.64 for the lumbar spine, and h 2=0.67 for the total body. The total effect of all significant covariates on phenotypic variation in the BMD measures was 14–38%. Age, sex, BMI, and physical activity were significant covariates for all BMD measures, while menopausal status was a significant covariate for BMD in the lumbar spine as well. For the heel QUS measures, heritability estimates ranged from 0.55 to 0.78, and less than 10% of the phenotypic variance of each trait was explained by covariates [10].
Phenotypic correlations between total hip BMD and QUS measures were: 0.44 with BUA, 0.43 with SOS, and 0.45 with QUI. The correlations between femoral neck BMD and QUS measures were: 0.40 with BUA, 0.36 with SOS, and 0.39 with QUI. Similarly, the correlations between lumbar spine BMD and QUS measures were 0.32, 0.30, and 0.32, respectively. The phenotypic correlation between total body BMD and SOS (r=0.42) was slightly higher than that between total body BMD and BUA (r=0.37). Table 4 shows the genetic correlations between BMD in the total hip, femoral neck, lumbar spine and total body with the QUS measures. All additive genetic correlations (ρ G ) were significantly greater than zero at p<0.01, indicating significant shared genetic effects. For total hip BMD, ρ G ± standard error (SE) was 0.63±0.11 with BUA, 0.50±0.10 with SOS, and 0.56±0.10 with QUI. For femoral neck BMD, ρ G ± SE was 0.62±0.11 with BUA, 0.40±0.10 with SOS, and 0.48±0.10 with QUI (p<0.00001). In general, the genetic correlations between BMD of the lumbar spine and QUS measures were lower: ρ G ± SE was 0.38±0.12 with BUA, 0.34±0.10 with SOS, and 0.35±0.11 with QUI. For total body BMD, ρ G ± SE was 0.51±0.12 with BUA, 0.52±0.09 with SOS, and 0.54±0.10 with QUI. In addition, all genetic correlations were significantly different from 1 (p<0.0001), indicating incomplete pleiotropy.
Environmental correlations between BMD and QUS measures were minimal, ranging from 0.17 to 0.25 for total hip BMD, 0.05 to 0.24 for femoral neck BMD, 0.22 to 0.24 for lumbar spine BMD, and 0.13 to 0.17 for total body BMD (Table 5). All environmental correlations were not significantly different from zero, indicating the lack of correlated response to non-genetic factors among the traits examined.
Discussion
We estimated the heritability of areal BMD in several body regions, and estimated the additive genetic and random environmental correlations between areal BMD and QUS measures of the non-dominant heel among Caucasian men and women. Our results show that areal BMD measures are heritable and that the genetic correlations between BMD and QUS measures are moderate, indicating significant shared genetic effects between these different measures of bone strength. For BMD measurements taken at the total hip and femoral neck, approximately 16–40% of the genetic variance is shared with QUS measures. We also found evidence of unique, unshared genetic effects influencing BMD and the QUS measures independently.
Our heritability estimates of areal BMD are comparable with findings from several family studies that reported a similar range of heritability [6, 7, 27, 28]. At the total hip and femoral neck, additive genetic effects account for approximately 68% of the total variation of BMD after the simultaneous adjustment for covariates. Similarly, we found that 64% of the variance of lumbar spine, and 67% of the variance of total body BMD is explained by additive genetic effects. Using comparable data from the Framingham Osteoporosis Study, Karasik et al. reported heritabilities in the range of 0.54 to 0.61 for femoral neck BMD and a principal component derived from different measures of hip BMD [29]. Similarly, Deng et al. estimated the heritability of hip BMD to be 0.65 in white families [30]. The heritability estimates of QUS measures obtained here are also consistent with results from other studies [11, 12, 21].
To date, most genetic studies have focused on estimating genetic effects on variation in areal BMD measures obtained from DXA, but these measures of bone mass do not provide direct information pertaining to bone structure, an important predictor of bone strength. Consequently, other measures of bone strength, including QUS measures, have been examined in many studies because of their ability to predict fracture independent of BMD [11, 31, 32]. BUA or SOS is significantly correlated with BMD at the same site [33] and other skeletal sites [14, 34]. The current study shows phenotypic correlations between BUA and hip BMD measurements (r=0.39 – 0.42, p<0.001) similar to those obtained in previous studies [14, 35]. Still other studies have shown skeletal site-matched phenotypic correlations between calcaneal QUS and calcaneal BMD that were higher and in the range of 0.56 to 0.82 [33, 36, 37]. Despite these moderate to high phenotypic correlations, it is still evident that BMD measures do not perfectly predict measures of QUS. Between 35 and 50% of the phenotypic variability in each trait can be explained by other factors.
In our study, we found that only 14% of the genetic variance of lumbar spine BMD was explained by genes influencing calcaneal BUA. Therefore, approximately 86% of the genetic variance of lumbar spine BMD is explained by genes independent from those shared with BUA. Our results also demonstrate that 26% of the genetic variance of total body BMD and approximately 40% of the genetic variance of hip BMD are shared with genes influencing BUA measures. Shared genetic effects between the different BMD measures and SOS are somewhat lower. Genes shared with SOS accounted for between 12% of the genetic variance of lumbar spine BMD and 27% of the genetic variance of total body BMD. Thus, it is evident that a substantial proportion of the genetic variance in BMD measures is not shared with QUS measures.
This result is not surprising since many epidemiologic studies have demonstrated that lower calcaneal BUA is a significant risk factor for hip and vertebral fractures independent of BMD [14, 19, 38]. Because of certain methodological shortcomings related to QUS in the clinical setting, such as uni-directional measurement instead of three orthogonal directional measurements, some studies suggest that QUS measures only weakly reflect bone mass [39, 40]. On the other hand, other studies suggest that QUS measures at the calcaneus or other peripheral skeletal sites exhibit structural properties, including elasticity or porosity of trabeculae, that are not ascertained using standard DXA technology that measures bone mass [18, 41, 42]. Our results show a similar correlational pattern, but with a stronger magnitude of genetic correlation, as one study of twin pairs [12]. In that study of 93 female twin pairs, Howard et al. reported the genetic correlation to range from 0.43 to 0.51 between BUA and BMD measured at the lumbar spine, femoral neck, and total body, and from 0.32 to 0.45 between velocity of sound and BMD measurements [12]. In addition, as much as 90% of the variance in SOS was not accounted for by genes also influencing femoral neck BMD. In another study of 215 female twin pairs in which skeletal sites were matched, less than half of the genetic variance of SOS at the radius was explained by BMD at the radius [21]. Taken collectively with the results of other studies, our results are consistent with the premise that there are some unique genetic factors controlling BMD that do not influence QUS, and vice versa. These results have important implications for osteoporosis gene discovery efforts. Depending upon the phenotype assessed, we would be likely to find genes controlling variation in both sets of traits simultaneously, but also to discover different genes influencing each trait independently. Further, the absence of significant environmental correlations between these measures also suggests that the traits pairs do not respond to environmental, non-genetic factors in the same manner [43].
Our study has several strengths, including its family-based study design and the fact that a variety of osteoporosis risk factors were controlled for in the statistical genetic analysis. First, extended pedigree study designs have specific advantages compared with studies of twins because in the former relatives live in many different households, thereby minimizing the impact of a common household environment. There is some evidence that the twin study design may overestimate heritability since it assumes that monozygotic twin and dizygotic twin pairs share common environmental factors to the same degree [43]. Second, we included several important risk factors for osteoporosis, such as age, sex, smoking, physical activity, adiposity and menopausal status, in our models to minimize the possible confounding effects of certain environmental factors on phenotypic variation in BMD and QUS measures.
This study has some potential limitations. Study participants are Caucasians residing mostly in southwestern Ohio. Consequently, we may not be able to generalize our findings to other socio-economic groups or ethnic populations as the estimation of heritabilities and genetic correlations is population-specific. We adjusted for a number of environmental risk factors in our analyses, but heritability may also be influenced by the differential effects of different environmental factors operating in various populations. Finally, the calcaneal QUS measures examined in our study are not skeletal site-matched with the areal BMD measures. Thus, we were not able to directly estimate the shared genetic association between BMD and QUS measures in the same region of the body. Nevertheless, our results are still comparable to results from other studies for the phenotypic and genetic correlations between skeletal site-matched BMD and QUS [21, 33, 36, 37].
In summary, this study shows that areal BMD measures are moderately heritable and are, in part, jointly influenced by a common set of genes that also influences variation in calcaneal QUS measures. Additionally, this study demonstrates evidence for a different set of genes unique to each trait that independently influences areal BMD and calcaneal QUS measures. The identification of joint and individual genetic influences on areal BMD and QUS measures provides important insights into the genetic architecture of these related traits. These insights may help to guide future genetic studies of osteoporosis risk through a better characterization of the phenotypes to be examined. Future studies can be planned that exploit the pleiotropic relationships among these traits to increase statistical power and increase the likelihood of identifying osteoporosis susceptibility genes. Further characterization and localization of the putative genes influencing variation in multiple bone strength measures will lead to important advances in the assessment and treatment of osteoporosis risk.
References
National Osteoporosis Foundation (2002) America’s bone health: the state of osteoporosis and low bone mass in our nation. National Osteoporosis Foundation, Washington D.C.
Looker AC, Wahner HW, Dunn WL, Calvo MS, Harris TB, Heyse SP, Johnston CC Jr, Lindsay R (1998) Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int 8:468–489
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359:1761–1767
Huang QY, Recker RR, Deng HW (2003) Searching for osteoporosis genes in the post-genome era: progress and challenges. Osteoporos Int 14:701–715
Gueguen R, Jouanny P, Guillemin F, Kuntz C, Pourel J, Siest G (1995) Segregation analysis and variance components analysis of bone mineral density in healthy families. J Bone Miner Res 10:2017–2022
Deng HW, Chen W-M, Conway T, Zhou Y, Davies KM, Stegman MR, Deng HW, Recker RR (2000) Determination of bone mineral density of the hip and spine in human pedigrees by genetic and life-style factors. Genet Epidemiol 19:160–177
Mitchell BD, Kammerer CM, Schneider JL, Perez R, Bauer RL (2003) Genetic and environmental determinants of bone mineral density in Mexican Americans: results from the San Antonio Family Osteoporosis Study. Bone 33:839–846
Pocock NA, Eisman JA, Hopper JL, Yeaste MG, Sambrook PN, Eberl S (1987) Genetic determinants of bone mass in adults: a twin study. J Clin Invest 80:706–710
Slemenda CW, Christian JC, Williams CJ, Norton JA, Johnston CC Jr (1991) Genetic determinants of bone mass in adult women: a reevaluation of the twin model and the potential importance of gene interaction on heritability estimates. J Bone Miner Res 6:561–567
Lee M, Czerwinski SA, Choh AC, Towne B, Demerath EW, Chumlea WC, Sun SS, Siervogel RM (2004) Heritability of calcaneal quantitative ultrasound measures in healthy adults from the Fels Longitudinal Study. Bone 35:1157–1163
Arden NK, Baker J, Hogg C, Baan K, Spector TD (1996) The heritability of bone mineral density, ultrasound of the calcaneus and hip axis length: a study of postmenopausal twins. J Bone Miner Res 11:530–534
Howard GM, Nguyen TV, Harris M, Kelly PJ, Eisman JA (1998) Genetic and environmental contributions to the association between quantitative ultrasound and bone mineral density measurements: a twin study. J Bone Miner Res 13:1318–1327
Sahota O, San P, Cawte SA, Pearson D, Hosking DJ (2000) A comparison of the longitudinal changes in quantitative ultrasound with dual-energy X-ray absorptiometry: the four-year effects of hormone replacement therapy. Osteoporos Int 11:52–58
Bauer DC, Gluer CC, Cauley JA, Vogt TM, Ensrud KE, Genant HK, Black DM (1997) Broadband ultrasound attenuation predicts fractures strongly and independently of densitometry in older women. A prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med 157:629–634
Frost ML, Blake GM, Fogelman I (2002) A comparison of fracture discrimination using calcaneal quantitative ultrasound and dual X-ray absorptiometry in women with a history of fracture at sites other than the spine and hip. Calcif Tissue Int 71:207–211
Khaw KT, Reeve J, Luben R, Bingham S, Welch A, Wareham N, Oakes S, Day N (2004) Prediction of total and hip fracture risk in men and women by quantitative ultrasound of the calcaneus: EPIC-Norfolk prospective population study. Lancet 363:197–202
van den Bergh JP, van Lenthe GH, Hermus AR, Corstens FH, Smals AG, Huiskes R (2000) Speed of sound reflects Young’s modulus as assessed by microstructural finite element analysis. Bone 26:519–524
Bouxsein ML, Radloff SE (1997) Quantitative ultrasound of the calcaneus reflects the mechanical properties of calcaneal trabecular bone. J Bone Miner Res 12:839–846
Hans D, Srivastav SK, Singal C, Barkmann R, Njeh CF, Kantorovich E, Gluer CC, Genant HK (1999) Does combining the results from multiple bone sites measured by a new quantitative ultrasound device improve discrimination of hip fracture? J Bone Miner Res 14:644–651
Gluer CC, Hans D (1999) How to use ultrasound for risk assessment: a need for defining strategies. Osteoporos Int 9:193–195
Knapp K, Andrew T, Macgregor A, Blake GM, Fogelman I, Spector T (2003) An investigation of unique and shared gene effects on speed of sound and bone density using axial transmission quantitative ultrasound and DXA in twins. J Bone Miner Res 18:1525–1530
Roche AF (1992) Growth, maturation, and body composition: the Fels Longitudinal Study, 1929–1991. Cambridge University Press, Cambridge; New York, NY
Lohman T, Martorell R, Roche AF (1988) Anthropometric standardization reference manual. Human Kinetics, Champaign, IL, U S A
Baecke JAH, Burema J, Frijters JER (1982) A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36:936–942
Almasy L, Blangero J (1998) Multipoint quantitative-trait linkage analysis in general pedigrees. Am J Hum Genet 62:1198–1211
Almasy L, Dyer TD, Blangero J (1997) Bivariate quantitative trait linkage analysis: Pleiotropy versus co-incident linkages. Genet Epidemiol 14:953–958
Brown LB, Streeten EA, Shuldiner AR, Almasy LA, Peyser PA, Mitchell BD (2004) Assessment of sex-specific genetic and environmental effects on bone mineral density. Genet Epidemiol 27:153–161
Nguyen TV, Livshits G, Center JR, Yakovenko K, Eisman JA (2003) Genetic determination of bone mineral density: evidence for a major gene. J Clin Endocrinol Metab 88:3614–3620
Karasik D, Cupples LA, Hannan MT, Kiel DP (2004) Genome screen for a combined bone phenotype using principal component analysis: the Framingham study. Bone 34:547–556
Deng HW, Mahaney MC, Williams JT, Li J, Conway T, Davies KM, Li J-L, Deng HW, Recker RR (2002) Relevance of the genes for bone mass variation to susceptibility to osteoporotic fractures and its implications to gene search for complex human diseases. Genet Epidemiol 22:12–25
Lenchik L, Hsu FC, Register TC, Lohman KK, Freedman BI, Langefeld CD, Bowden DW, Carr JJ (2004) Heritability of spinal trabecular volumetric bone mineral density measured by QCT in the Diabetes Heart Study. Calcif Tissue Int 75:305–312
Slemenda CW, Turner CH, Peacock M, Christian JC, Sorbel J, Hui SL, Johnston CC (1996) The genetics of proximal femur geometry, distribution of bone mass and bone mineral density. Osteoporos Int 6:178–182
Gluer CC, Vahlensieck M, Faulkner KG, Engelke K, Black D, Genant HK (1992) Site-matched calcaneal measurements of broad-band ultrasound attenuation and single X-ray absorptiometry: do they measure different skeletal properties? J Bone Miner Res 7:1071–1079
Wu C, Hans D, He Y, Fan B, Njeh CF, Augat P, Richards J, Genant HK (2000) Prediction of bone strength of distal forearm using radius bone mineral density and phalangeal speed of sound. Bone 26:529–533
Frost ML, Blake GM, Fogelman I (2001) Does the combination of quantitative ultrasound and dual-energy X-ray absorptiometry improve fracture discrimination? Osteoporos Int 12:471–477
Langton CM, Langton DK (2000) Comparison of bone mineral density and quantitative ultrasound of the calcaneus: site-matched correlation and discrimination of axial BMD status. Br J Radiol 73:31–35
Kang C, Speller R (1998) Comparison of ultrasound and dual energy X-ray absorptiometry measurements in the calcaneus. Br J Radiol 71:861–867
Gluer CC, Eastell R, Reid DM, Felsenberg D, Roux C, Barkmann R, Timm W, Blenk T, Armbrecht G, Stewart A, Clowes J, Thomasius FE, Kolta S (2004) Association of five quantitative ultrasound devices and bone densitometry with osteoporotic vertebral fractures in a population-based sample: the OPUS Study. J Bone Miner Res 19:782–793
Hans D, Arlot ME, Schott AM, Roux JP, Kotzki PO, Meunier PJ (1995) Do ultrasound measurements on the os calcis reflect more the bone microarchitecture than the bone mass?: a two-dimensional histomorphometric study. Bone 16:295–300
Langton CM, Njeh CF, Hodgskinson R, Currey JD (1996) Prediction of mechanical properties of the human calcaneus by broadband ultrasonic attenuation. Bone 18:495–503
Sakata S, Barkmann R, Lochmuller EM, Heller M, Gluer CC (2004) Assessing bone status beyond BMD: evaluation of bone geometry and porosity by quantitative ultrasound of human finger phalanges. J Bone Miner Res 19:924–930
Cortet B, Boutry N, Dubois P, Legroux-Gerot I, Cotten A, Marchandise X (2004) Does quantitative ultrasound of bone reflect more bone mineral density than bone microarchitecture? Calcif Tissue Int 74:60–67
Lynch M, Walsh B (1998) Genetics and analysis of quantitative traits. Sinauer, Sunderland, MA, U S A
Acknowledgements
We are thankful for the participation of the families in the Fels Longitudinal Study and the assistance of our research staff. This study was supported by National Institutes of Health grants (AR052147, HD12252, HL69995, DK64870, DK64391). This study was presented in part at the American Society for Bone and Mineral Research 26th Annual Meeting in 2004.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, M., Czerwinski, S.A., Choh, A.C. et al. Unique and common genetic effects between bone mineral density and calcaneal quantitative ultrasound measures: the Fels Longitudinal Study. Osteoporos Int 17, 865–871 (2006). https://doi.org/10.1007/s00198-006-0075-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0075-4