
Abstract
To estimate the prevalence and the related risk factors of low bone mineral density of the calcaneus and the distal radius, a community-based study was conducted in three rural areas of Korea. A total of 1420 women and 732 men aged 40 years and older participated in this study. Information on sociodemographic characteristics and the potential risk factors for osteoporosis were collected by an interviewer-administered standardized questionnaire. Bone mineral density (BMD) of the calcaneus and the distal radius were measured by dual-energy X-ray absorptiometry (DXA). Three hundred and seventeen women and 183 men aged 20–29 years who participated in a regular health check-up were used as a reference population. Osteoporosis was defined using WHO criteria. Odds ratios of the risk factors of osteoporosis were calculated by the unconditional logistic regression model. The standardized prevalence of osteoporosis of the calcaneus was 8.4% for males and 27.3% for females using the Korean population of year 2000 as a standard population. The standardized prevalence of osteoporosis of the distal radius was 4.2% for males and 18.8% for females. Older age and lower body mass index (BMI) were related with low BMD in both the calcaneus and distal radius in males and females. The duration after menopause and the number of live births were an independent risk factor for osteoporosis of the calcaneus (OR=1.1, 95% CI=1.00–1.11; the duration after menopause; OR=2.0, 95% CI=1.20–3.35, the number of live birth) and a familial history of non-traumatic fractures or osteoporosis among the first-degree relatives was significantly related to a increased risk of osteoporosis of the distal radius in females (OR=2.9, 95% CI=1.36–6.31).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is defined as a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of the bone tissue, leading to enhanced bone fragility and a consequent increased fracture risk [1]. Low bone mineral density (BMD) is a good predictor of the development of non-pathologic fractures [2]. According to the WHO criteria, osteoporosis is defined as a BMD 2.5 SD or more below the peak bone mass of a young, healthy sex- and race-matched reference population [1], and osteopenia is defined as a BMD between 1.0 and 2.5 SD below the peak bone mass. The expected life span of the Korean population is increasing as in most western countries. In 2000, the proportion of elders, defined as 65 years old or more, in the Korean population was 7.4% and in 2020 it is expected to reach 15.1% [3]. This trend indicates that osteoporosis related fractures may become a major health problem in elderly people in Korea.
The prevalence of osteoporosis determined by previous studies conducted mainly among Caucasians ranges from 4.1% to 38.0% [4,5,6,7,8,9,10,11,12,13]. These discrepancies might be due to several factors, including subjects studied (e.g. ethnicity, age), the reference populations used, measuring sites (lumbar spine, femoral neck, calcaneus, distal radius) and the measuring method [dual-energy X-ray absorptiometry (DXA), single-energy X-ray absorptiometry, quantitative ultrasonography].
Risk factors of osteoporosis such as age, menopause, family history of fracture and obesity have shown consistent results in many studies [14,15,16,17], whereas other factors (e.g. deficiency of calcium and vitamin D, decreased physical activity, cigarette smoking, long-term use of some drugs, such as corticosteroids, GnRH antagonists, thyroxine, and some anticancer drugs remain inconclusive. Although DXA is an optimum method to estimate bone mass in a clinical setting [18], relatively few studies have been performed upon measuring the BMD of the calcaneus or distal radius using this technique. Moreover, most of the studies have been conducted in Caucasians and no large-scale community-based study using DXA, including both males and females and an analysis of risk factors, has been conducted in Korea. Thus, we conducted the community-based study to estimate the prevalence of low bone mineral density using DXA and to identify risk factors with respect to low bone mineral density in the Korean population.
Materials and methods
Subjects
Three rural areas of South Korea were selected for this study. All residents aged 40 years and older were invited to participate. One area, Sinbuk-up, Chunchon City, located in the northern part of South Korea, consisted of 4181 (1950 males and 2231 females) residents aged 40 years and older. Of these, 660 residents (233 males and 427 females) participated (participation rate 16%). Another area, Kangwha-up, located in the western part of Korea, had 3448 residents aged 40 years and older. Of these, 943 residents (273 males and 670 females) participated (participation rate 27%). The third area included three counties in Chungju City, located in the center of Korea, consisted of 8054 residents aged 40 years and older. Of these, 713 residents (282 males and 431 females) participated (participation rate 9%). Finally, a total of 788 males and 1528 females aged 40 years and older were recruited. Of these, 732 males and 1420 females with both BMD measurements remained in this study. Informed consent was obtained from all participants.
Questionnaire and examination
A standardized questionnaire was used to evaluate the risk factors for osteoporosis, including sociodemographic factors, past and current medical history, medication history, family history on osteoporosis of non-traumatic fractures, smoking and drinking habits, and physical activity. For females, reproduction history including age at menarche, age at menopause, reason for menopause, numbers of full-term pregnancies and live births, duration of breastfeeding, history of abortions (both spontaneous and artificial), and use of oral contraceptives and hormone replacement therapy (HRT) were obtained. All interviews were conducted by trained interviewers, and participants’ heights and weights were recorded.
Measurement of bone mineral density
BMD of the right calcaneus and distal radius were measured by DXA using Lunar PIXI instruments. Calibration was done daily. A total of 317 healthy Korean females and 183 healthy Korean males aged 20–29 who participated in a regular health check-up were used as the reference population. The mean and the standard deviation (SD) of calcaneus BMD in young males and females was 0.613±0.100 and 0.494±0.076, respectively. The mean and SD of distal radius in males and females was 0.550±0.064 and 0.465±0.061, respectively (Table 1). As the WHO T-score criteria, subjects were categorized as: osteopenia, BMD values between 1 and 2.5 SD, osteoporosis, BMD values ≥2.5 SD below the mean of a young Korean reference population (Table 1).
Analysis
To estimate the prevalence of osteoporosis, the age- and sex-specific prevalences of osteoporosis were calcuated. The age-standardized prevalence was calculated using distribution of Korean population for the year 2000 [3] and the World Standard Population as standard populations [19]. A logistic regression model was used to estimate the odds ratios of the risk factors for osteoporosis. Persons categorized as having normal BMD were regarded as controls and persons with a BMD in the osteoporotic range were regarded as cases. All analysis was performed stratified by sex and the BMD measuring sites.
Results
The demographic characteristics and distributions of the selected risk factors of the study population are listed in Table 2.
Tables 3 and 4 show the age- and sex-specific, and the standardized prevalences of osteoporosis of the calcaneus and of the distal radius. The standardized prevalence of the osteoporosis of the calcaneus of 40 years old or more was 8.4% for males and 27.3% for females, using the year 2000 Korean population as the standard population. The standardized prevalence of the osteoporosis of distal radius was 4.2% and 18.8% for males and females, respectively.
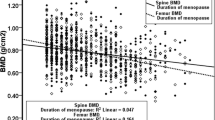
Tables 5 and 6 display the odds ratios of selected risk factors for osteoporosis. The most consistent results observed across both sexes and measuring sites were that the risk of osteoporosis increased as age increased, and decreased as the body mass index increased. There was a significant association between educational levels and calcaneal BMD in both males and females; individuals educated at or over high school level had a decreased risk of osteoporosis compared with individuals educated at elementary school level (OR=0.4, 95% CI=0.18–1.00 in males; OR=0.2, 95% CI=0.06–0.82 in females). The duration after menopause and the number of live births were independent risk factors of calcaneus in females (OR=1.1, 95% CI=1.00–1.11, duration after menopause; OR=2.0, 95% CI=1.20–3.35, number of live births). A positive family history of non-traumatic fractures or osteoporosis increased the risk of osteoporosis of the distal radius in females (OR=2.9, 95% CI=1.36–6.31).
Discussion
In the present study, the prevalence of osteoporosis of the calcaneus and the distal radius was estimated in three Korean rural communities. The prevalences of osteoporosis were 8.4% for males and 27.3% for females in the calcaneus and 4.2% and 18.8% for males and females in the distal radius after standardizing for age distribution of the Korean population.
Comparing the prevalences of osteoporosis reported in different studies is not easy due to the different measuring sites used, the age range of the study participants, and of the reference populations. Table 7 summarizes the results of previous studies, and shows that the prevalence of osteoporosis varies significantly between countries. Few studies have presented adjusted prevalence rates using either age distributions of their own countries or those of the World Standard Population.
A Chinese study on the BMD of the calcaneus reported age specific prevalences for osteoporosis in males and females [11]. These prevalences were lower than our results for both sexes (Table 7); in our study, age-standardized prevalences of osteoporosis of subjects aged 60 years and older were 62.8% for females and 20.7% for males. In a sample of a Bulgarian female referral population, the authors reported that osteoporosis of the distal radius was found in 20% of all females aged 50 years and older [10]. The age-specific prevalence of the Bulgarian study was lower than that obtained in the present study for all age groups. In a Japanese study, Iki et al. (2001) estimated the prevalence of osteoporosis of the distal radius in the Japanese population at age 50–79 years as 36.6% [5], which is similar to our result; in this study, age-standardized prevalence of osteoporosis of the women aged 50–79 years and older was 41.4%.
The reason why our subjects showed a relatively higher prevalence might be due to the differences in the reference values, the BMD measuring devices, and/or the criteria used to define osteoporosis. The higher prevalence observed in this study, however, is more likely due to the characteristics of the subjects recruited; our study subjects were older, had lower BMI (overall mean BMI: 24.3 kg/m2), and were less educated (more than 90% of the subjects under middle school education) than the subjects reported previously.
Although peripheral BMD measurements are not usually used in regular clinical practice, they could be applied to a large scale community-based survey because of their easy accessibilities and fair predictability of fracture occurrence. Stone et al. (2003) reported that peripheral BMD measurements (e.g. calcaneus, distal radius) had almost equivalent predictability to central BMD measurement for risk of fracture of various anatomical sites [19]. Sweeney et al. (2002) also reported that the calcaneus BMD showed high sensitivity and specificity in predicting the low BMD of femoral neck and lumbar spine [20].
In the risk factor analysis, an older age and a lower body mass index were found to be consistent risk factors for males and females as shown in previous many reports. BMI has been found to be inversely associated with fracture risk and bone mass in many studies, but the mechanism is unclear. Higher impact during weight-bearing activities, nutritional conditions and hormonal effects are possible mechanisms for the protective effect of a higher BMI [17]. A positive family history for non-traumatic fractures or osteoporosis showed increased risk only in female distal radius. Increased risks of osteoporosis in those with a family history of osteoporosis or non-traumatic fracture are suggested to indicate a genetic contribution to the development of osteoporosis.
There is no association between BMD and alcohol drinking. Moderate alcohol consumption has been related to a higher BMI by some studies [21,22], but others have failed to show this association [23,24]. Alcohol might affect bone density by increasing levels of endogenous estrogen [22]. A recent meta-analysis of cigarette smoking and bone mineral density showed that bone loss was greater only in postmenopausal women who smoked, not in premenopausal women [25]. However, Grainge et al. (1998) reported that BMD was significantly reduced in both pre- and postmenopausal women who smoked at all five BMD measuring sites examined [24]. Although only a small percentage of females smoke (6%), this studies showed no association between smoking and osteoporosis in both males and females.
The limitations of our study include the following. The participation rates were low (9–27%) and the study population contained more persons in the 60–70 age group than the eligible population. In addition, older subjects are more likely to be less educated and vulnerable to the risk factors of low BMD. Inaccurate recall and BMD measurement errors are also likely to have occurred. However, such a misclassification bias would result in an underestimation of the true association.
Further studies combining risk factors and genetic predisposing factors would give informative insights into the pathogenesis and the preventive strategies of osteoporosis.
References
World Health Organization (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Technical Report Series No. 843. WHO, Geneva
Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE, Cauley J, Black D, Vogt TM for the Study of Osteoporotic Fractures Research Group (1995) Risk factors for hip fracture in white women. N Engl J Med 332:767–773
Korea National Statistical Office. http://www.nso.go.kr
Limpaphayom KK, Taechakraichana N, Jaisamrarn U, Bunyavejchevin S, Chaikittisikpa S, Poshyachinda M, Taechamahachai C, Havanond P, Onthuam Y, Lumbiganon P, Kamolratanakul P (2001) Prevalence of osteopenia and osteoporosis in Thai women. Menopause 8:65–69
Iki M, Kagamimori S, Kagawa Y, Matsuzaki T, Yoneshima H, Marumo F (2001) Bone mineral density of the spine, hip and distal forearm in representative samples of the Japanese female population: Japanese Population-Based Osteoporosis (JPOS) Study. Osteoporos Int 12:529–537
Li N, Ou P, Zhu H, Yang D, Zheng P (2002) Prevalence rate of osteoporosis in the mid-aged and elderly in selected parts of China. Chin Med J 115:773–775
Tenenhouse A, Joseph L, Kreiger N, Poliquin S, Murray TM, Blondeau L, Berger C, Hanley DA, Prior JC (2000) Estimation of the prevalence of low bone density in Canadian women and men using a population-specific DXA reference standard: the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos Int 11:897–904
Smeets-Goevaers CG, Lesusink GL, Papapoulos SE, Maartens LW, Keyzer JJ, Weerdenburg JP, Beijers LM, Zwinderman AH, Knottnerus JA, Pols HA, Pop VJ (1998) The prevalence of low bone mineral density in Dutch perimenopausal women: the Eindhoven perimenopausal osteoporosis study. Osteoporos Int 8:404–409
Looker AC, Orwoll ES, Johnston CC, Lindsay RL, Wahner HW, Dunn WL, Calvo MS, Harris TG, Heyse SP (1997) Prevalence of low femoral bone density in older U.S. adults from NHANES III. J Bone Miner Res 12:1761–1768
Boyanov M, Popivanov P (2002) Prevalence of low forearm bone density in a Bulgarian female referral population. Osteoporos Int 13:288–295
Xu SZ, Zhou W, Mao XD, Xu J, Xu LP, Ren JY (2001) Reference data and predictive diagnostic models for calcaneus bone mineral density measured with single-energy X-ray absorptiometry in 7428 Chinese. Osteoporos Int 12:755–762
Kim CH, Kim YI, Choi CS, Park JY, Le MS, Lee SI, Kim GS (2000) Prevalence and risk factors of low quantitative ultrasound values of calcaneus in Korean elderly women. Ultrasound Med Biol 26:35–40
Maalouf G, Salem S, Sandid M, Attallah P, Eid J, Saliba N, Nehme I, Johnell O (2000) Bone mineral density of the Lebanese reference population. Osteoporos Int 11:756–764
Consensus Development Conference Report (1993) Diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med 94:646–650
Boyle P, Leon ME, Autier P (2001) Epidemiology of osteoporosis. J Epidemiol Biostat 6:185–192
Kanis JA (2002) Diagnosis of osteoporosis and assessment of fracture risk. Lancet 359:1929–1936
National Institutes of Health (2000) Osteoporosis prevention, diagnosis, and therapy. Consensus Statement, March 27–29, vol. 17(1)
Melton LJ III, Atkinson EJ, O’Connor MK, O’Fallon WM, Riggs BL (1998) Bone density and fracture risk in men. J Bone Miner Res 13:1915–1923
Stone KL, Seeley DG, Lui LY, Cauley JA, Ensrud K, Browner W, Nevitt M, Cummings SR (1993) BMD at multiple sites and risk of fracture of multiple types: long-term results from the study of osteoporotic fractures. J Bone Miner Res 2003 18:1947–1954
Sweeney AT, Malabanan AO, Blake MA, Weinberg J, Yurner A, Ray P, Holick MF (1995) Bone mineral density assessment: comparison of dual-energy X-ray absorptiometry measurements at the calcaneus, spine, and hip. J Clin Densitom 2002 5:57–62
Holbrook TL, Barrett-Connor E (1994) A prospective study of alcohol consumption and bone mineral density. BMJ 306:1506–1509
Felson Dt, Zhang Y, Hannan MT, Kannel WB, Kiel DP (1998) Alcohol intake and bone mineral density in elderly men and women. The Framingham Study. Am J Epidemiol 142:485–492
Hu JF, Zhao XH, Chen JS, Fitpatrick J, Parpia B, campbe TC (1997) Bone density and lifestyle characteristics in premenopausal and postmenopausal Chinese women. Osteoporos Int 4:288–297
Grainge MJ, Coupland CAC, Cliffe SJ, Chilvers CED, Hosking DJ (1998) Cigarette smoking, alcohol and caffeine consumption, and bone mineral density in postmenopausal women. Osteoporos Int 8:355–363
Law MR, Hackshaw AK. A meta-analysis of cigarette smoking, bone mineral density and risk of hip fracture: recognition of a major effect. BMJ 315:841–846
Acknowledgements
This study was supported by a grant from the Korean Ministry of Health and Welfare (01-PJ1-PG1-01CH08-0001).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shin, A., Choi, JY., Chung, HW. et al. Prevalence and risk factors of distal radius and calcaneus bone mineral density in Korean population. Osteoporos Int 15, 639–644 (2004). https://doi.org/10.1007/s00198-004-1587-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-004-1587-4