
Abstract
Hypovitaminosis D can result in low bone mass. The prevalence of hypovitaminosis D has public health implications, especially where data are lacking. Since diet and sunlight are the two souces of vitamin D, the results obtained in one geographical region may not be universally applicable. The aim of this study is to characterize the prevalence and seasonal variation of hypovitaminosis D and its relationship to bone metabolism in community dwelling postmenopausal Hungarian women. We determined serum levels of 25-hydroxyvitamin D (25-OH-D), PTH, osteocalcin (OC), degradation products of C-terminal telopeptides of type-I collagen (CTx), dietary calcium intake and BMD at L2–L4 lumbar spine (LS) and femur neck (FN) in 319 randomly selected ambulatory postmenopausal women. The prevalence of hypovitaminosis D (serum 25-OH-D≤50 nmol/l) was 56.7%. On comparing patients with normal and low 25-OH-D, a significant difference was found in age (61.6±8.5 years versus 67.3±9.9 years; P<0.001), PTH (3.9±1.9 pmol/l versus 4.3±2.7 pmol/l; P<0.05), FN BMD (0.802±0.123 g/cm2 versus 0.744±0.125 g/cm2; P<0.001) and dietary calcium intake (714.4±199.4 g/day versus 607.9±233 g/day; P<0.001). Osteoporotic patients had a significantly lower 25-OH-D (37.6±19.8 nmol/l versus 56.4±24 nmol/l; P<0.001) and dietary calcium intake (519.2±244.5 mg/day versus 718.2±164.3 mg/day; P<0.001). After controlling for all other variables, 25-OH-D was found to be significantly associated with age, the average hours of sunshine in the 3 months prior to 25-OH-D level determination and dietary calcium intake (r 2=0.190; P<0.001). For FN BMD, significant independent predictors were age, body mass index, 25-OH-D and dietary calcium intake (r 2=0.435; P<0.001). The prevalence of hypovitaminosis D during spring, summer, autumn and winter was 71%, 46.3%, 49.4% and 56.7%, respectively. There was significant seasonal variation in 25-OH-D, PTH, OC, calcium intake and FN BMD. There is a high prevalence of hypovitaminosis D in healthy postmenopausal Hungarian women, and FN BMD is associated with serum 25-OH-D and dietary calcium intake.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vitamin D plays a vital role in maintenance of skeletal health [1]. Vitamin D deficiency and consequent secondary hyperparathyroidism are known to cause a decrease in bone mineral density (BMD) and increase in bone turnover [2, 3, 4]. A low serum 25-hydroxyvitamin D (25-OH-D) concentration is the hallmark of vitamin D deficiency. As such, serum 25-OH-D is an index of body vitamin D status [5, 6]. The determination of the prevalence of hypovitaminosis D has public health implications with regards to formulation of strategies to reduce the burden of metabolic bone diseases and their intermingling with “pure” osteoporosis, especially in the elderly, not disregarding other implications. Several studies [7, 8, 9, 10, 11, 12, 13, 14] have characterized the prevalence of hypovitaminosis D in healthy postmenopausal women, but these data are lacking for a Hungarian population. Serum 25-OH-D is the most important clinically available measurement of vitamin D status, reflecting lifestyle and dietary habits [15]. Since diet and sunlight are the two sources of vitamin D, the results obtained in other geographical areas may not be readily applicable to our population.
The aim of this study is to characterize the prevalence and seasonal variation of hypovitaminosis D and its relationship to parathyroid hormone, dietary calcium intake, biochemical markers of bone turnover and BMD at the lumbar spine and the femur neck in a random population sample of community dwelling postmenopausal women in Hungary.
Materials and methods
Postmenopausal women residing in Debrecen, Hungary (latitude: 47°29’25”, longitude: 21°36’39”, altitude: 107.9 m) were invited to participate in the study. A total of 319 participants who gave written informed consent (permission was received from the local research ethics committee) and fulfilled the inclusion/exclusion criteria were included in the study. Recruitment was possible through out the year 2002 (January to December).
The regional osteoporosis center at Debrecen (established in 1992) is the only center in the city (population 230,000) having densitometers with possibility for axial measurements, and on average we examine 7000 patients per year. Approximately one-third of the patients are examined solely for the purpose of screening for postmenopausal osteoporosis.
In this study, we invited those patients for participation who were referred to us for initial evaluation solely for the purpose of postmenopausal osteoporosis screening. Referring was based on postmenopausal status only, and since we did not influence referral, we regard the study population as randomly selected.
Inclusion criteria were: postmenopausal, ambulatory, community dwelling, resident of Debrecen, referred to us for initial evaluation, solely for the purpose of screening of postmenopausal osteoporosis (first bone mineral density measurement), and generally regarded as healthy.
Exclusion criteria were known prevalent metabolic bone disease, severe liver or renal disease, use of medication influencing bone metabolism (including calcium and vitamin D supplementation) and history of osteoporotic fracture.
Detailed medical history was collected and standard laboratory examinations were performed (any abnormal values resulted in exclusion). All patients had normal values for serum calcium and phosphorus. A trained study nurse administered a validated questionnaire to assess daily dietary calcium intake.
Dual energy X-ray absorptiometry examination was performed using the LUNAR Prodigy (GE-Lunar Corp., Madison, Wisc., USA) densitometer. BMD was measured at L2–L4 lumbar spine (LS) and femur neck (FN). The coefficient of variation (CV) of the technique at our institute was 0.8% using the anatomical spine phantom measure daily.
BMD was expressed as T-score, number of standard deviations from the mean of young women attaining peak bone mass, using the normative reference values (German) provided by the manufacturer. Normalcy, osteopenia and osteoporosis were defined according to the WHO classification [16].
Morning blood samples (after overnight fasting) were collected. Serum 25-OH-D and intact parathyroid hormone (PTH) were measured using radioimmunoassay and immunoradiometric assay, respectively (Diasorin Inc., Stillwater, Minn., USA). Serum osteocalcin (OC) and serum degradation products of C-terminal telopeptides of type-I collagen (CTx) were measured using electrochemiluminiscence immunoassay (Roche Diagnostics GmbH, Mannheim, Germany). The inter-assay CV was <13% for 25-OH-D, <11% for PTH, <5% for OC and <7% for CTx.
Hypovitaminosis D was defined as serum 25-OH-D levels ≤50 nmol/l as suggested by Lips [17].
The daily hours of sunshine in our region were obtained from the Hungarian Meteorological Service.
Descriptive statistics are presented as mean, median, range and standard deviation (SD), as applicable. The Kolmogorov-Smirnov test was used to check for normality of distribution. The Mann-Whitney U-test was used to compare the means between two groups. One-way analysis of variance (ANOVA) was used for group comparison. Correlation between variables was tested using regression analysis. A value of P<0.05 was considered statistically significant. All analyses were performed with the Statistical Package for Social Sciences (SPSS) statistical software for Windows, version 9.0 (SPSS Inc., Ill., USA).
Results
The characteristics of the patients in this cross-sectional study are shown in Table 1. The prevalence of hypovitaminosis D was 56.7%. The percentage of patients having normal, osteopenic and osteoporotic T-scores at the LS was 14.4%, 34.5% and 50.8%, respectively and at the FN was 21.9%, 39.5% and 38.6%, respectively. The average dietary calcium intake was lower than the recommended dietary calcium intake [18] in the studied postmenopausal women.
On comparing patients with normal and low 25-OH-D, significant differences were found in age (61.6±8.5 years versus 67.3±9.9 years; P<0.001), PTH (3.9±1.9 pmol/l versus 4.3±2.7 pmol/l; P<0.05), FN BMD (0.802±0.123 g/cm2 versus 0.744±0.125 g/cm2; P<0.001) and dietary calcium intake (714.4±199.4 g/day versus 607.9±233 g/day; P<0.001).
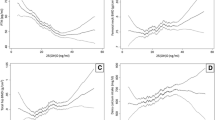
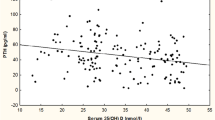
There was a significant correlation between 25-OH-D and age (r=−0.367; P<0.001), the average hours of sunshine in the 3 months prior to 25-OH-D level determination (r=0.308; P<0.001) and dietary calcium intake (r=0.288, P<0.001); PTH and CTx (r=0.117; P<0.05); LS BMD and age (r=−0.317; P<0.001), body mass index (BMI) (r=0.230; P<0.001), 25-OH-D (r=0.111; P<0.05) and dietary calcium intake (r=0.176; P<0.005); FN BMD and age (r=−0.583; P<0.001), BMI (r=0.362; P<0.001), 25-OH-D (r=0.322; P<0.001) and dietary calcium intake (r=0.325; P<0.001).
Based on the LS T-score, there was a significant difference between normal and osteoporotic subgroups in dietary calcium intake (711.3±182 mg/day versus 620.6±237.8 mg/day; P<0.05). Based on the FN T-score, there was a significant difference (P<0.001) between normal and osteoporotic subgroups in 25-OH-D (56.4±23.9 versus 37.6±19.8 nmol/l) and dietary calcium intake (781.2±164.3 mg/day versus 519.2±244.5 mg/day).
The prevalence of hypovitaminosis D during spring, summer, autumn and winter was 71%, 46.3%, 49.4% and 56.7%, respectively.
Table 2 shows the mean (range) values of LS and FN BMD, 25-OH-D, PTH, OC, CTx, dietary calcium intake and hours (median, range) of daily sunshine in the different seasons. There was a statistically significant difference in FN BMD between spring and summer, and autumn (P<0.05); in PTH levels between spring and summer, and autumn (P<0.05); in OC levels (P<0.05) between autumn and spring, and summer; and in dietary calcium intake between spring and autumn (P<0.01).
After controlling for all other variables, 25-OH-D was found to be significantly associated with age, the average hours of sunshine in the 3 months prior to serum 25-OH-D level determination and dietary calcium intake (r 2=0.190; P<0.001). For FN BMD, significant independent predictors were age, BMI, 25-OH-D and dietary calcium intake (r 2=0.435; P<0.001). Age and BMI (r 2=0.148; P<0.001) were the only significant independent predictors for LS BMD.
Discussion
Vitamin D is needed to maintain calcium absorption and skeletal integrity as much in older as in younger people. We get vitamin D from sunlight exposure and food. In the skin, sunlight (ultraviolet radiation) stimulates the conversion of 7-dehydrocholesterol to previtamin D, which is spontaneously converted to cholecalciferol. Foods such as diary products, eggs and fish contain a little vitamin D; in general food is not fortified in Hungary and in addition, there is no uniform fortification policy in Europe. Whatever the source of vitamin D, it is then converted sequentially to 25-OH-D in the liver and 1,25-dihydroxyvitamin D, the active hormone, in the kidneys.
Determining the amount provided by the sun or food is difficult. The duration and intensity of exposure to sunlight are not easily measurable, and age, skin pigmentation, sunscreens, clothing and even window glass reduce its effects [19]. In equatorial regions exposure to the sun alone is adequate, but at latitudes above 40° north or south and higher, people make little vitamin D in the winter.
Measurement of serum 25-OH-D provides direct information. Although its concentration depends on vitamin D production and intake, its serum half-life is much longer than that of vitamin D (weeks versus hours), and it therefore provides an integrated assessment of vitamin D status. Serum 25-OH-D concentrations depend on age, sunlight exposure, vitamin D dietary intake, or supplementation.
All the patients studied were Caucasian, which is true for the majority of the Hungarian population. As such, the study population can be regarded as representative of the general population.
Comparing our results with other studies involving similarly large numbers of community dwelling postmenopausal women, the prevalence of hypovitaminosis D found in our study population is higher than that reported in other European countries [8, 9, 11, 12, 13]. The difference was even larger in spring. This finding can only partly be attributed to the higher cut-off level of 50 nmol/l used by us, although it may depend on the comparability of the assays for 25-OH-D used in the different studies.
The main factors contributing to vitamin D insufficiency are poor vitamin D intake, low sunlight exposure, and disorders or drugs known to affect vitamin D metabolism [15]. In our study population, secondary causes affecting vitamin D metabolism were excluded. On the other hand, low calcium intake is known to increase PTH secretion [20], causing high serum 1,25-dihydroxyvitamin D production resulting in increased catabolism of 25-OH-D, thereby decreasing serum 25-OH-D and inducing or aggravating vitamin D deficiency. We found an association between dietary calcium intake and serum 25-OH-D.
As could be anticipated, the serum PTH exhibited an inverse seasonal variation with high levels in spring and low levels in summer. Others [21, 22] have also reported similar variations.
The highest hours of sunshine were noted in summer and the lowest in winter, whereas the highest 25-OH-D levels were observed in autumn and the lowest in spring. Therefore serum 25-OH-D levels depend on the duration of sunshine in the previous season. It is important to note that the seasonal variation in 25-OH-D went hand in hand with the variation in FN BMD. It is difficult to draw conclusions about seasonal variation in BMD from the data presented, given that different patients were assessed at different times of the year, and that BMD changes relatively slowly in each patient. The only way in which seasonal variation in BMD can be accurately assessed is to measure the same patients repeatedly in different seasons over time, which would probably show little to no significant seasonal change in a short interval.
The increased serum PTH causes an increase in bone turnover, which is usually associated with cortical bone loss [23]. We found a significant positive correlation between PTH and CTx, but no correlation with BMD.
A German study [24] showed seasonal variation in biochemical markers of bone turnover. We found such variation only in the OC levels. It has been shown [13, 25, 26] that the increase in serum PTH and bone resorption and formation markers is consistent with increased bone turnover and bone loss in patients with vitamin D deficiency. We found that decreased bone mass at the FN was associated mainly with serum 25-OH-D levels and dietary calcium intake, but we failed to show an association with PTH and the biochemical markers of bone turnover. In cross-sectional studies, a positive relationship has been observed between serum 25-OH-D and BMD of the hip [3, 4, 19]; our results support this finding.
The limitations of our study include those associated with cross-sectional studies. Given the uncertain predictive power of clinical risk factors of osteoporosis, we felt that this population sample, selected by age truncation and exclusion of known bone diseases and vitamin D supplementation, is a fairly acceptable approximation of a postmenopausal female population sample. Although we found an effect of the variation in sunshine hours on serum 25-OH-D levels, we did not assess the direct individual personal sunlight exposure.
Our most important finding is the high prevalence of hypovitaminosis D (even higher in spring) in the Hungarian postmenopausal community dwelling women and the association of low serum 25-OH-D and dietary calcium intake with low femur neck bone mineral density. These findings most probably have public health implications and may help formulate health policies in our part of Europe, since our results may well be applicable to other countries in socioeconomic transition. We believe that universal vitamin D and calcium supplementation, especially in winter, can be beneficial and cost effective at a population level.
References
Omdahl JL, Garry PJ, Hunsaker LA, Hunt WC, Goodwin JS (1982) Nutritional status in a healthy elderly population: vitamin D. Am J Clin Nutr 36:1225–1233
Khaw KT, Sneyd MJ, Compston J (1992) Bone density parathyroid hormone and 25-hydroxyvitamin D concentrations in middle aged women. BMJ 305:273–277
Ooms ME, Lips P, Roos JC et al (1995) Vitamin D status and sex hormone binding globulin: determinants of bone turnover and bone mineral density in elderly women. J Bone Miner Res 10:1177–1784
McAuley KA, Jones S, Lewis-Barned NJ, Manning P, Goulding A (1997) Low vitamin D status is common among elderly Dunedin women. N Z Med J 110:275–277
Dawson-Hughes B, Dallal GE, Krall EA, Harris S, Sokoll LJ, Falconer G (1991) Effect of vitamin D supplementation on wintertime and overall bone loss in healthy postmenopausal women. Ann Int Med 115:505–512
Hollis BW (1996) Assessment of vitamin D nutritional and hormonal status: what to measure and how to do it. Calcif Tissue Int 58:4–5
Tsai KS, Hsu SH, Cheng JP, Yang RS (1997) Vitamin D stores of urban women in Taipei: effect on bone density and bone turnover, and seasonal variation. Bone 20:371–374
Chapuy MC, Preziosi P, Maamer M et al (1997) Prevalence of vitamin D insufficiency in an adult normal population. Osteoporos Int 7:439–443
Bettica P, Bevilacqua M, Vago T, Norbiato G (1999) High prevalence of hypovitaminosis D among free-living postmenopausal women referred to an osteoporosis outpatient clinic in northern Italy for initial screening. Osteoporos Int 9:226–229
Gannage-Yared MH, Chemali R, Yaacoub N, Halaby G (2000) Hypovitaminosis D in a sunny country: relation to lifestyle and bone markers. J Bone Miner Res 15:1856–1862
Brot C, Vestergaard P, Kolthoff N, Gram J, Hermann AP, Sorensen OH (2001) Vitamin D status and its adequacy in healthy Danish perimenopausal women: relationships to dietary intake, sun exposure and serum parathyroid hormone. Br J Nutr 86:S97–103
Kauppinen-Makelin R, Tahtela R, Loyttyniemi E, Karkkainen J, Valimaki MJ (2001) A high prevalence of hypovitaminosis D in Finnish medical in- and outpatients. J Int Med 249:559–563
Mezquita-Raya P, Munoz-Torres M, Luna JD et al (2001) Relation between vitamin D insufficiency, bone density, and bone metabolism in healthy postmenopausal women. J Bone Miner Res 16:1408–1415
Rassouli A, Milanian I, Moslemi-Zadeh M (2001) Determination of serum 25-hydroxyvitamin D(3) levels in early postmenopausal Iranian women: relationship with bone mineral density. Bone 29:428–430
Silverberg SJ, Fitzpatrick LA, Bilezikian JP (1996) The role of parathyroid hormone and vitamin D in the pathogenesis of osteoporosis. In: Marcus R, Feldman D, Kesley J (eds) (1996) Osteoporosis. Academic Press, San Diego, pp 716–726
Kanis JA, Melton LJ 3rd, Christiansen C, Johnston CC, Khaltaev N (1994) The diagnosis of osteoporosis. J Bone Miner Res 9:1137–1141
Lips P (2001) Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 22:477–501
Anonymous (1994) National Institute of Health Consensus Conference. Optimal calcium intake. JAMA 272:1942–1948
Holick MF (1994) Vitamin D—new horizons for the 21st century. Am J Clin Nutr 60:619–630
Heaney RP, Gallagher JC, Johnston CC, Neer R, Parfitt AM, Whedon GD (1982) Calcium nutrition and bone health in the elderly. Am J Clin Nutr 36:986–1013
Krall EA, Sahyoun N, Tannenbaum S, Dallal GE, Dawson-Hughes B (1989) Effect of vitamin D intake on seasonal variations in parathyroid hormone secretion in postmenopausal women. N Engl J Med 321:1777–1783
Lips P, Netelenbos JC, Jongen MJ et al. (1982) Histomorphometric profile and vitamin D status in patients with femoral neck fracture. Metab Bone Dis Relat Res 4:85–93
Silverberg SJ, Shane E, de la Cruz L et al (1989) Skeletal disease in primary hyperparathyroidism. J Bone Miner Res 4:283–291
Woitge HW, Scheidt-Nave C, Kissling C et al. (1998) Seasonal variation of biochemical indexes of bone turnover: results of a population-based study. J Clin Endocrinol Metab 83:68–75
Sahota O, Masud T, San P, Hosking DJ (1999) Vitamin D insufficiency increases bone turnover markers and enhances bone loss at the hip in patients with established vertebral osteoporosis. Clin Endocrinol (Oxf) 51:217–221
Marcus R, Madvig P, Young G (1984) Age-related changes in parathyroid hormone and parathyroid hormone action in normal humans. J Clin Endocrinol Metab 58:223–230
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bhattoa, H.P., Bettembuk, P., Ganacharya, S. et al. Prevalence and seasonal variation of hypovitaminosis D and its relationship to bone metabolism in community dwelling postmenopausal Hungarian women. Osteoporos Int 15, 447–451 (2004). https://doi.org/10.1007/s00198-003-1566-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-003-1566-1