
Abstract
The aim of this study was to determine the contribution of constitutional and lifestyle variables on the subsequent risk of distal forearm (Colles') fracture in a multinational, multicenter, population-prospective study. A total of 15,745 subjects from the European Vertebral Osteoporosis Study, who had completed a baseline questionnaire on lifestyle and constitutional factors, were followed up annually using a validated questionnaire to ascertain the occurrence of new fractures. Risks are expressed as hazard ratios (with 95% confidence intervals) derived from a Cox proportional hazards regression model. The incidence of Colles' fracture was 1.7 and 7.3 per 1000 person years in men and women, respectively. In women delayed menarche, over the age of 15 years, was associated with a modest increased risk [HR 1.5 (range 1.1–2.0)]. Regular walking in that group also increased the risk [HR 1.6 (1.2–2.2)] perhaps reflecting the increased exposure to risk of falling. None of the other factors examined revealed any important influences. The results are broadly in line with the few other published prospective studies suggesting only a modest role for these factors in influencing susceptibility to fracture.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colles' fracture (fracture of the distal radius) is one of the most common sites of osteoporotic fracture and contributes to significant morbidity. Future lifetime risk in a woman is reported to be 15% at age 50 years [1] in the U.S. and over 20% at age 45 years [2] in Sweden. By contrast, the age-specific incidence in men is 25% of that [2].
As with all osteoporotic fractures, the occurrence of Colles' fracture is explained by a fall in an individual with low bone density; thus, risk factors for the fracture might be anticipated to be those associated with these two processes, including some such as frailty, that might be common to both.
Retrospective data suggest that low bone mineral density (BMD) may be of limited importance in predicting susceptibility in those aged over 65 years [3]. Decreased bone density has been shown in prospective studies, however, to be an important predictor of future Colles' risk. In the Study of Osteoporotic Fractures (SOF), women in lowest quintile of BMD had four times the risk of fracture compared with those in the highest quintile [4]. In the recently reported Dubbo study there was a 50% increased fracture risk per standard deviation reduction in BMD, which was observed in both genders [5]. In addition, given the risks of low BMD, it is perhaps surprising that few lifestyle risk factors have been shown to be predictive of future Colles' fracture in either gender. The data are not consistent, however, with some studies, for example, Hemenway et al. [6], suggesting that lifestyle factors are important, whereas recent studies have suggested only a limited role for physical inactivity, smoking, body mass, and co-morbidity [4, 7, 8, 9]. There are, however, suggestions of a modest effect of female reproductive variables on risk [10]. The data on physical activity are indeed supportive that those who are the most active are at greatest risk [3, 9, 11], suggesting that exercise increases the likelihood of exposure to falls. The major difference in incidence between the genders, however, remains unexplained.
We therefore analyzed the data from the European Prospective Osteoporosis Study (EPOS) to determine the role of host and lifestyle factors on the subsequent risk of Colles' fracture in both men and women.
Subjects and methods
Study design
A prospective population study was used based on questionnaire follow-up to determine the occurrence of fractures in subjects who had completed a baseline interview on potential risk factors.
Baseline interview
Subjects were recruited from the prospective phase (EPOS) of the European Vertebral Osteoporosis Study. In brief, subjects aged 50–79 years were recruited from population-based sampling frames from 36 European centers, with the aim of recruiting 50 in each of the 5-year age bands from 50–54 to 75–79 years. Details of recruitment and the response rate (median center 54%) to the baseline survey are described elsewhere [12]. Each subject was interviewed using a validated risk factor questionnaire, shown to be reproducible between centers [13]. Current physical activity level was based on average time spent daily on walking and cycling. Data was also collected on the exposure to heavy occupational and related physical activity during three age periods. Subjects were asked to self-rate their current health status. Women were asked to recall their ages at menarche and at natural menopause and data were collected on oral contraceptive and post-menopausal hormone use. Current steroid use was also obtained. Height and weight were measured in all subjects.
There were no important differences between questionnaire responders and an intensively followed-up sample of nonresponders in the key factors investigated. In a subset of the original population BMD measurements were also made, details of which are described in elsewhere [14].
Follow-up
In all, 31 of the 36 originally participating centers agreed to follow up the subjects studied. These centers provided 7604 men and 8141 women eligible for follow-up. Each subject was sent an annual questionnaire, (every 6 months for the German Centers) asking about fractures and falls in the intervening period. Self-reports of fractures were validated by local review of medical records with the aim of ascertaining if there was possible radiographic evidence of a fracture. The sensitivity and specificity of the questionnaire has been shown to be excellent, with both proportions over 0.9 for Colles' fracture in these populations [15]. For the purposes of analysis, Colles' fracture was defined by radiographic evidence of fracture of the distal radius or self-reported by the subject on a body manikin as occurring in the wrist. In all, only 15 (8%) of the 188 fractures reported were not verified by medical records.
Analysis
All risk factor variables were stratified into categories for subsequent analysis. Body mass index was divided by quintile. Physical activity was categorized into those reporting only light or moderate activity vs those reporting heavy activity, at each of the three age periods of life considered. Walking was categorized into those reporting more than 30 min per day. Smoking was categorized into ever or never and alcohol into less than once per week or above that level. Other stratifications for all these variables were also investigated without any important impact on the results.
The date of Colles' fracture was used in a Cox proportional hazards regression model to determine the risk of fracture in relation to the baseline variables considered. Subjects were followed up to the date of last received follow-up questionnaire or death. Analyses were undertaken stratified by gender and adjusted for age. Analyses were also repeated after excluding the 8% of unverified fracture cases. The risk factor results were identical and thus the analyses presented includes all the fracture cases. Subsequent analyses were adjusted for institution, but as this had little effect, the institution unadjusted rates are presented. The analyses were also repeated including all the risk factors using a multivariate model. All analyses were undertaken using STATA version 6 (STATA Corp.)
Results
In all, there was a very low loss-to-follow-up rate. After excluding the 284 men and 167 women who had died, 6451 (88%) and 6936 (87%) of the men and women, respectively, were followed-up.
The mean (and the median) follow-up were approximately 3.0 years in both genders, and the total person years of follow-up was 19,662 in men and 21,072 in women. There were 34 Colles' fractures in men and 154 in women, equivalent to incidence rates of 1.7 per 1000 (95% CI 1.1–2.3) and 7.3 per 1000 (95% CI 6.1–8.5) person years, respectively. Despite the large study size, the number of fractures in men was small; thus, the confidence intervals around the risk estimates of the predictors examined were too wide for useful comment; consequently, only the results from the risk factor data in women are presented.
A comparison was undertaken of the baseline questionnaire data between those participating and not participating in the follow-up (Table 1), and showed that the nonparticipants were less likely to be regular walkers, more likely to report poor health, and have a slightly higher body mass index, a difference which was statistically significant. In that gender, apart from a greater use of oral contraceptives in the participants, there were no other differences in the hormonal and gynecological variables collected at baseline.
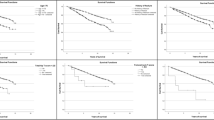
The univariate risk factors in women, adjusted only for age, for the major lifestyle and related host factors, are shown in Table 2. In brief, there were no risk factors recorded on the questionnaire that were strong risk factors of Colles' fracture. Most of the hazard ratios in women were around unity with relatively narrow confidence intervals suggesting that the study did not miss a major effect. Increased body mass index was not protective. Similarly, alcohol, smoking, and consumption of calcium-containing foods had little effect. Perhaps surprisingly, even those who self-reported their general health to be below satisfactory did not have an important subsequent increased risk (HR 1.1, 95% CI 0.8–1.6). The level of physical activity at three periods of adult life did not predict future fracture. Interestingly, those who walked outdoors or cycled more than 1 h/day had a 60% increased risk. The only "positive" finding emerged from consideration of the data on hormonal and reproductive factors; thus, women with a delayed age at menarche (above the age of 15 years) had a 50% increased risk of fracture. There was, however, no influence of age at menopause. On multivariate analysis the findings remain broadly unaltered (Table 2), the increased risk from walking still being apparent; however, those who had a menarchal age of 15 years or over were no longer at significantly increased risk. The number of all participants who had had a baseline BMD [13] was too small for useful analysis on the risk of Colles' fracture.
Discussion
This was a very large population-based prospective study, across a number of populations in Europe with high follow-up rates and utilizing a validated approach to the detection of distal radius fracture. The main finding is thus "disappointing" in revealing very little evidence that lifestyle/host factors are linked to Colles' fracture. As discussed below, however, our findings are consistent with previous reports and other recently published prospective studies.
There are some methodological issues that need to be addressed before reaching conclusions on the role of lifestyle factors in this fracture. Firstly, there is always the possibility of selection bias introduced by the population sampling, nonresponse to initial baseline survey, and loss to follow-up. These factors are unlikely to be important in explaining the results observed. The samples in each center were derived from true population sampling frames [11], and a detailed analysis of the baseline nonresponders did not reveal any bias toward a higher or lower risk of fracture [16]. More importantly, the follow-up in those who participated in the baseline was high and again, as shown in Table 2, the differences that did emerge were not consistently in the direction of either a presumed higher or lower risk of fracture, although participants were less likely to report poor general health and, in women, were less regular walkers. Furthermore, such nonparticipation could have only influenced the results if the relationship between risk factors and participation was selectively different between those developing and not developing a fracture, which seems unlikely.
A second concern is that the levels of inaccuracy in the baseline assessment was such that random misclassification achieved the level that reduced the likelihood of finding real differences. The reproducibility of the questionnaire had already been demonstrated to be good [13]. Furthermore, the construct validity of some of the items had already been proven in relation to vertebral deformity; thus, we have already demonstrated that low body mass, decreased walking, heavy activity in men, regular alcohol use, and some of the gynecological variables ascertained by this approach were associated with vertebral deformity [17, 18, 19, 20].
These results also confirm findings from other studies using different approaches, thereby supporting our conclusions; thus, in the U.S. Health Professionals Study of men there were few risk factors for wrist fracture including the absence of an effect for smoking, alcohol, and body mass [8]. No influence was found for general health, physical activity, or smoking in a case control study from Sweden [10]; indeed, those authors concluded that "lifestyle factors did not discriminate between fracture patients and controls." More recently, the Dubbo prospective study revealed very few risk factors for fracture apart from low femoral neck bone density in both genders, low dietary calcium in men, and a history of falls in women [4]. Similarly, the Study of Osteoporotic Fractures prospective study, restricted to women over 65 years, identified recurrent falling as the most important lifestyle factor [21]. The Blue Mountains Eye Study [9] also found few lifestyle risk factors but no recent vigorous activity was strongly protective. Interestingly, a recent study from the Mayo Clinic failed to find an important contribution from factors associated with secondary osteoporosis to distal forearm fracture risk [22], unlike their influence on hip and spinal fracture.
The suggestion from our data that a delayed age at menarche is interesting and consistent with the results of the possible protective effect of a late menopause found in the Swedish Study [10]. We also found a relationship of similar strength with age at menopause, but the confidence interval did not exclude unity; the latter is possibly more difficult to define accurately given variations in definition and the impact of artificial menopause. We had previously demonstrated good reproducibility of recalled menopausal age in this population [12].
The BMD was only assessed in a modest subsample of these subjects at baseline [14], mainly for resource reasons, and thus there were insufficient data to examine the role of BMD in predicting fracture. Distal forearm fracture is related to low bone mass, although the strength of the association is variable and may be modest [4, 5, 23]. In particular, BMD is less predictive of postmenopausal fracture [5]. These data suggest that this fracture is more related to peak bone mass rather than subsequent loss; hence, it is perhaps not surprising that "current" lifestyle factors have little effect.
Finally, wrist fracture results from a fall and there are several subject characteristics that predict falling including poor eyesight, postural instability, and general frailty [9, 24, 25]. Most of these factors were not assessed in the current study, although we were surprised that poor self-reported general health did not emerge as a risk factor. Our data did show that those who walk the most were at greatest risk. This is consistent with a previous case control study [11] and suggests that any beneficial effect of this exercise on bone and muscle mass is attenuated by the increased exposure to the potential for falling.
The conclusion from the existing literature, confirmed by the present study, is that the typical "osteoporotic" lifestyle factors assessed do not suggest areas for prevention of distal radius fracture; thus, greater emphasis needs to be focused on factors such as poor vision [9] which increase the risk of falling.
References
Cummings SR, Black DM, Rubin SM (1989) Lifetime risks of hip, Colles, or vertebral fracture and coronary heart disease among white postmenopausal women. Arch Intern Med 149:2445–2448
Kanis JA, Johnell O, Oden A, Sernbo I, Redlund-Johnell I, Dawson A et al. (2000) Long-term risk of osteoporotic fracture in Malmo. Osteoporosis Int 11:669–674
Earnshaw SA, Cawte SA, Worley A, Hosking DJ (1998) Colles' fracture of the wrist as an indicator of underlying osteoporosis in postmenopausal women: a prospective study of bone mineral density and bone turnover rate. Osteoporosis Int 8:53–60
Kelsey JL, Browner WS, Seeley DG, Nevitt MC, Cummings SR (1992) Risk factors for fractures of the distal forearm and proximal humerus. The Study of Osteoporotic Fractures Research Group. Am J Epidemiol 135:477–489
Nguyen TV, Center JR, Sambrook PN, Eisman JA (2001) Risk factors for proximal humerus, forearm, and wrist fractures in elderly men and women: the Dubbo Osteoporosis Epidemiology Study. Am J Epidemiol 153:587–595
Hemenway D, Colditz GA, Willett WC, Stampfer MJ, Speizer FE (1988) Fractures and lifestyle: effect of cigarette smoking, alcohol intake, and relative weight on the risk of hip and forearm fractures in middle-aged women. Am J Public Health 78:1554–1558
Mallmin H, Ljunghall S (1992) Incidence of Colles' fracture in Uppsala. A prospective study of a quarter-million population. Acta Orthop Scand 63:213–215
Hemenway D, Azrael DR, Rimm EB, Feskanisch D, Willett WC (1994) Risk factors for wrist fracture: effect of age, cigarettes, alcohol, body height, relative weight, and handedness on the risk for distal forearm fractures in men. Am J Epidemiol 140:361–367
Ivers RQ, Cumming RG, Mitchell P, Peduto AJ (2002) Risk factors for fractures of the wrist, shoulder and ankle: the Blue Mountains Eye Study. Osteoporosis Int 13:513–518
Mallmin H, Ljunghall S, Persson I, Bergstrom R (2002) Risk factors for fractures of the distal forearm: a population-based case-control study. Osteoporosis Int 4:298–304
O'Neill TW, Marsden D, Adams JE, Silman AJ (1996) Risk factors, falls, and fracture of the distal forearm in Manchester, UK. J Epidemiol Community Health 50:288–292
O'Neill TW, Marsden D, Matthis C, Raspe H, Silman AJ (1995) European Vertebral Osteoporosis Study Group. Survey response rates: national and regional differences in a European multicentre study of vertebral osteoporosis. J Epidemiol 49:87–93
O'Neill TW, Cooper C, Cannata JB, Diaz-Lopez JB, Hoszowski K, Johnell O et al. (1994) Reproducibility of a questionnaire on risk factors for Osteoporosis in a Multicentre Prevalence Survey: the European Vertebral Osteoporosis Study. Int J Epidemiol 23:559–565
Lunt M, Felsenberg D, Adams J, Benevolenskaya L, Cannata J, Dequeker J et al. (1997) Population based geographic variations in DXA bone density in Europe: The EVOS study. European Vertebral Osteoporosis. Osteoporosis Int 7:175–189
Ismail AA, O'Neill TW, Cockerill W, Finn JD, Cannata JB, Hoszowski K et al. (2000) Validity of self-report of fractures: results from a prospective study in men and women across Europe. EPOS Study Group. European Prospective Osteoporosis Study Group. Osteoporos Int 11:248–254
O'Neill TW, Marsden D, Silman AJ (1995) Differences in the characteristics of responders and non-responders in a prevalence survey of vertebral osteoporosis. European Vertebral Osteoporosis Study Group. Osteoporosis Int 5:327–334
Johnell O, O'Neill T, Felsenberg D, Kanis J, Cooper C, Silman AJ et al. (1997) Anthropometric measurements and vertebral deformities. Am J Epidemiol 146:287–293
Silman AJ, O'Neill TW, Cooper C, Kanis J, Felsenberg D (1997) Influence of physical activity on vertebral deformity in men and women: results from the European Vertebral Osteoporosis Study. J Bone Miner Res 12:813–819
Diaz MN, O'Neill TW, Silman AJ (1997) The influence of family history of hip fracture on the risk of vertebral deformity in men and women: the European Vertebral Osteoporosis Study. Bone 20:145–149
O'Neill TW, Silman AJ, Naves-Diaz M, Cooper C, Kanis J, Felsenberg D (1997) Influence of hormonal and reproductive factors on the risk of vertebral deformity in European Women. European Vertebral Osteoporosis Study Group. Osteoporosis Int 7:72–78
Vogt MT, Canley JA, Tomaino MM et al. (2002) Distal radial fractures in older women: a 10-year follow-up study of descriptive characteristics and risk factors. J Am Geriatric Soc 50:97–103
Melton LJ III, Achenbach SJ, O'Fallon WM, Khosla S (2002) Secondary osteoporosis and the risk of distal forearm fractures in men and women. Bone 31:119–125
Honkanen R, Kroger H, Tuppurainen M, Alhava E, Saarikoski S (1995) Fractures and low axial bone density in perimenopausal women. J Clin Epidemiol 48:881–888
Jones G, Nguyen T, Sambrook PN, Lord SR, Kelly PJ, Eisman JA (1995) Osteoarthritis, bone density, postural stability, and osteoporotic fractures: a population based study. J Rheumatol 22:921–925
Lord SR, Sambrook PN, Gilbert C, Kelly PJ, Nguyen T, Webster IW et al.(1994) Postural stability, falls and fractures in the elderly: results from the Dubbo Osteoporosis Epidemiology Study. Med J Aust 160:684–691
Acknowledgements
Project leaders of the European Prospective Osteoporosis Study Group are as follows: J. Reeve, A.J. Silman. Data Management: T.W. O'Neill, J.D. Finn, S.R. Pye, W.C. Cockerill, A.A. Ismail, D.K. Roy. Participants: D. Banzer, Berlin, Germany; L.I. Benevolenskaya, Moscow, Russia; A. Bhalla, Bath, U.K.; J. Bruges Armas, Azores, Portugal; J.B. Cannata, Oviedo, Spain; P. Delmas, Lyon, France; G. Dilsen, Istanbul, Turkey; J. Dequeker, Leuven, Belgium; J. Falch, Oslo, Norway; B. Felsch, Jena, Germany; D. Felsenberg, Berlin, Germany; C. Gennari, Siena, Italy; K. Hoszowski, Warsaw, Poland; I. Jajic, Zagreb, Croatia; J. Janot, Bochum, Germany; O. Johnell, Malmo, Sweden; G. Kragl, Erfurt, Germany; A. Lopez Vaz, Oporto, Portugal; R. Lorenc, Warsaw, Poland; G. Lyritis, Athens, Greece; F. Marchand, Lyon, France; P. Masaryk, Piestany, Slovakia; C. Matthis, Lubeck, Germany; T. Miazgowski, Szczecin, Poland; M. Navez Diaz, Oviedo, Spain; H.A.P. Pols, Rotterdam, Netherlands; G. Poor, Budapest, Hungary; A. Rapado, Madrid, Spain; H.H. Raspe, Lubeck, Germany; D.M. Reid, Aberdeen, U.K.; J. Reeve, Harrow, U.K.; W. Reisinger, Berlin, Germany; C. Scheidt-Nave, Heidelberg, Germany; J. Stepan, Prague, Czech Republic; C. Todd, Cambridge, U.K.; K. Weber, Graz, Austria; A.D. Woolf, Truro, U.K. This report was prepared on behalf of the group by: S.R. Pye, T.W. O'Neill, M. Lunt, J.A. Kanis, C. Cooper, O. Johnell, J. Reeve, and A.J. Silman. The study was financially supported by a European Union Concerted Action Grant under BIOMED 1 (BMH1CT920182), and also EU grants C1PDCT925102, ERBC1PDCT 930105 and 940229. The central coordination was also supported by the UK Arthritis Research Campaign, the Medical Research Council (G9321536) and the European Foundation for Osteoporosis and Bone Disease. The EU's PECO program linked to BIOMED 1 funded in part the participation of the Budapest, Warsaw, Prague, Piestany, Szczecin, and Moscow centers. Data collection from Croatia was supported by a grant from the Wellcome Trust.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/s00198-004-1706-2.
Rights and permissions
About this article
Cite this article
Silman, A.J. Risk factors for Colles' fracture in men and women: results from the European Prospective Osteoporosis Study. Osteoporos Int 14, 213–218 (2003). https://doi.org/10.1007/s00198-002-1364-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-002-1364-1