
Abstract
Introduction and hypothesis
Sexual well-being is an important aspect of women's life. The objective of this study was to validate the Portuguese-translated version of the short form of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire—PISQ-12.
Methods
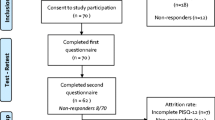
Sixty-four women were enrolled to participate in the process of validating the PISQ-12 (study group). A further 68 subjects were allocated to a control group for comparison between the group of women with pelvic organ prolapse/urinary incontinence and the asymptomatic group.
Results
The PISQ-12 presented good internal consistency (Cronbach's alpha of 0.79 for the study group and 0.80 for the control group). The test–retest reliability using the intraclass correlation coefficient was 0.77. Mean score on the PISQ-12 was significantly higher in the control group than in the study group (42.7 ± 3.9 vs 27.8 ± 9.3)
Conclusions
The Portuguese version of the PISQ-12 was reliable for the assessment of sexual function in women with pelvic organ prolapse/urinary incontinence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sexual well-being is an important aspect of women's health, and sexual dysfunction can lead to a poorer quality of life, affecting the relationship between partners. Although sexual dysfunction is a common problem, it has been the subject of scant investigations. Two types of questionnaires are used to evaluate sexual function: generic questionnaires which are applied to the general population but may not detect subtle changes in a specific population and disease-specific questionnaires used to assess patients presenting specific medical conditions.
Rogers et al. introduced a self-reporting questionnaire, the PISQ-31, to specifically evaluate sexual function in women with urinary incontinence (UI) and/or pelvic organ prolapse (POP) [1]. This questionnaire consists of 31 questions divided into three groups: emotional–behavioral, physical, and relationship with partner. A short form of the PISQ-31 questionnaire, called the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12), was then validated [2].
In the absence of a validated questionnaire in Portuguese to evaluate the impact of UI and POP on women's sexual function, this study was designed to validate and culturally adapt the PISQ-12 for use in Portuguese-speaking women. Although in Portuguese language there are several questionnaires to evaluate the quality of life in women with urinary incontinence and pelvic organ prolapse, there is not a specific one which evaluates the sexual function in women with these dysfunctions. The PISQ-12 questionnaire will help health professionals evaluate and determine the best treatment for these women. For scientific studies, it seems to be an instrument to measure sexual function in women with urinary incontinence and pelvic organ prolapse.
Material and methods
The PISQ-12 is a specific self-reporting questionnaire which evaluates sexual function in women with UI/POP. It consists of the following items: items 1–4 concern emotional and behavioral factors, items 5–9 deal with physical aspects, while items 10–12 address the relationship with partner. The scores are based on the sum of the individual questions. The Likert scale is used to grade responses which range from “never” to “always,” with a score of 0 to 4. For items 1–4, inverse scoring is used. The maximum score possible is 48: higher scores indicate better sexual function,
Two bilingual translators performed the translation into Portuguese. A third translator back-translated this version into English to check if the translated version accurately reflected the original. A committee comprising five health professionals and the two bilingual translators analyzed the results in order to resolve any discrepancies with the first translation. A pretest was carried out in 25 women from the vaginal surgery clinic of the Department of Obstetrics and Gynecology of the Santa Casa de São Paulo Hospital. After analysis and cultural adaptation of discrepant items, another pretest was administered to 11 women. Subsequently, the Portuguese version was considered ready for application.
One hundred women from the urogynecology center (NUG) of the Care Management Center of Jaú (NGA/25-Jaú) were evaluated for complaints of UI/POP, and of these, 64 were asked to join this study. All participants underwent a gynecological exam including a stress test (ST) and quantification of degree of pelvic organ prolapse (POP-Q). Another group of 68 women without UI/POP complaints served as the control group. This study was conducted between September and December of 2009. The research ethics committee of the Faculty of Medical Sciences of the Santa Casa de São Paulo Hospital—FCMSCSP—approved this study and all participants signed an informed consent form.
The questionnaire was self-administered; however, in cases when the interviewee is unable to read or write, the interviewer read out the questions aloud and filled out the replies given. This method was adopted in other validations such as that of King's Health [3]. Cam [4] also used an interview in the translation and evaluation of the PISQ-12 into Turkish, and this same method was also utilized by Espuña [5] to validate the Spanish version of the PISQ-12. Weinberger has recommended the use of this method [6].
To evaluate test–retest agreement, 51 women answered the same questionnaire 4 weeks after the initial interview. Women over 18 who had a heterosexual relationship and an active sexual life for at least 6 months were included in the study.
Scores on the PISQ-12 were calculated according to the author's instructions. The women in the study group answered the translated and adapted version of the PISQ-12 as well as two other previously validated questionnaires, the International Consultation on Incontinence Questionnaire—Short Form (ICIQ-SF) [7] and International Consultation on Incontinence Questionnaire—Vaginal Symptoms (ICIQ-VS) [8], considered as the “gold standard.”
Statistical analyses
Descriptive statistical analysis was done using measures of position and dispersion for continuous variables and frequency tables for categorical variables. Cronbach's alpha coefficient was used to measure internal consistency and accuracy based on the homogeneity of the items. In general, accuracy should not be below 0.80 if the scale was fully used, although values above 0.60 indicate consistency.
The intraclass correlation coefficient (ICC) was used to determine the test–retest reliability. ICC values above 0.70 indicate good reliability.
Pearson's coefficient of correlation was used to confirm a linear correlation between two variables. This coefficient ranges from −1 to +1. Values close to the extremes indicate strong negative or positive correlation, respectively, whereas values near zero indicate no correlation. Comparison of proportions was performed using the chi-squared test or Fisher's exact test, where applicable.
The Mann–Whitney test was used to compare continuous or ordinal variables between two groups, whereas the Kruskal–Wallis test was employed for three or more groups. The significance level was set at 5% for all statistical tests. The SAS System for Windows (Statistical Analysis System), version 9.2 (SAS Institute, INC, 2002–2008) was used for the statistical analysis.
Results
Of the 132 women assessed, 64 were considered symptomatic and were assigned to the study group, while the 68 asymptomatic women formed the control group. Twenty-seven (52.9%) subjects had a positive ST and 24 (39.2%) negative. Twenty-four patients had UI for approximately 1 year (38.1%), 18 (28.6%) between 1 and 5 years, and 21 (33.3%) for more than 4 years. The groups were similar with respect to educational level, age, and marital status as shown in Table 1.
Cronbach's alpha was 0.79 for the study group and 0.80 for the control group, which showed a good internal consistency. The intraclass correlation coefficient of 0.77 indicated test–retest reliability. The study group showed lower scores in comparison to the control group on the descriptive analysis and comparison of the scores of the two groups (Table 2).
Comparison of patients with and without UI was made using the stress test, while degree of POP was measured by the POP-Q. Correlations between the PISQ-12 and the previously validated tests (ICIQ-SF and ICIQ-VS) were also verified. The positive force test subjects showed lower scores (26.0 ± 8.9, p = 0.034). No significant correlation was found for the POP-Q or the ICIQ-SF. Comparison against the gold standard test, the ICIQ-VS, revealed a significant, albeit weak, correlation with the PISQ-12 (Table 3). ICIQ-VS scores were negatively correlated, given its inversely related scoring. Figure 1 depicts the validation of the Portuguese version vs other previously validated versions of the PISQ-12.

Comparison of PISQ-12 scores with previous validations
Discussion
The PISQ-12 is a specific questionnaire to evaluate sexual function in women with UI and POP, and yet, there was not any specific questionnaire in Portuguese. The present study showed that the Portuguese version of the PISQ-12 correlated well with the instruments validated for POP and UI, although the correlations among POP were weak. In general, the scores have shown the differences between groups study and control (Table 2). The scores comparison among stages of prolapse by the POP-Q did not find significant differences among the stages of POP, not being possible to discriminate the stage of POP with the score, which means that the more the stage of POP is, the worst the score is (Table 4). This might have happened due to the subjective nature that are the vaginal symptoms and topics related to sexuality such as dyspareunia, age, and emotional problems [9–11]. Weber et al. [9] and Ellerkman [10] did not find any correlation between sexual function and POP. In the Turkish and Spanish validation, no weak correlation was found. Although pelvic organ prolapse had an effect on some aspects of sexuality, it has no effect on certain aspects of sexual function such as orgasm and sexual satisfaction [12].
It is important to be aware that the Brazilian population is culturally and geographically different with some peculiarities. Although the sample size was determined correctly, following the previous questionnaire, perhaps with a larger sample, this weak correlation can be explained.
The objective of our study was to validate the Portuguese version of PISQ-12 questionnaire and not to determine whether POP is the reason for sexual dysfunction. Therefore, the global scores showed significant differences between groups.
Comprehension difficulties due to a low level of schooling were overcome with the assistance of the interviewer [6]. Our next objective is to determine if future studies could investigate the responsiveness of this test for evaluating sexual function in women after specific treatments for UI and POP.
Conclusion
The Portuguese-translated version of the PISQ-12 proved reliable and consistent for the assessment of sexual function in women with urinary incontinence and/or pelvic organ prolapse.
Abbreviations
- PISQ-12:
-
Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire
- IU:
-
Urinary incontinence
- POP:
-
Pelvic organ prolapse
- NUG:
-
Urogynecology center
- NGA:
-
Care management center
- ST:
-
Stress test
- POP-Q:
-
Pelvic Organ Prolapse Quantification
- ICC:
-
Intraclass correlation coefficient
- ICIQ-SF:
-
International Consultation on Incontinence Questionnaire—Short Form
- ICIQ-VS:
-
International Consultation on Incontinence Questionnaire—Vaginal Symptoms
References
Rogers RG, Krammerer-Doak D, Villarreal A, Coates K, Qualls C (2001) A new instrument to measure sexual function in women with urinary incontinence or pelvic organ prolapsed. Am J Obstet Gynecol 184(4):552–558
Rogers RG, Coates KW, Kammerer-Doak D, Khalsa S, Qualls C (2003) A short form of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12). Int Urogynecol J Pelvic Floor Dysfunct 14:164–168
Tammanini JTN, D'Áncoa CAL, Botega NJ, Netto NR Jr (2003) Validação do “King's Health Questionnaire” para o português em mulheres com incontinência urinária. Rev Saude Publica 37(2):1–13
Cam C, Sancak P, Karahan N, Sancak A, Celik C, Karateke A (2009) Validation of the short form of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12) in a Turkish population. Eur J Obstet Gynecol Reprod Biol 146:104–107
Espuña PM, Puig CM, Gonzáles AM, Zardain PC, Rebollo AP (2008) Cuestionário para evaluación de la función sexual em mujeres com prolapso genital y/o incontinência. Validación de La version española Del “Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12)”. Actas Urol Esp 32(2):211–219
Weinberger M, Oddone EZ, Samsa GP, Landsman PB (1996) Are health-related quality of life measures affected by the mode of administration? J Clin Epidemiol 49(2):135–140
Tamanini JTN, Dambros M, D'Ancona CAL, Palma PR, Netto NR Jr (2004) Validação para o português do “International Consultation on Incontinence Questionnaire- Short Form” (ICIQ-SF). Rev Saude Publica 38(3):438–444
Tamanini JTN, Almeida FG, Girotti ME, Riccetto CLZ, Palma PCR, Rios LAS (2008) The Portuguese validation of the International Consultation on Incontinence Questionnaire—Vaginal Symptoms (ICIQ-VS) for Brazilian women with pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct 19(10):1385–1391
Weber AM, Walters MD, Schover LR, Mitchinson A (1995) Sexual function in women with uterovaginal prolapse and urinary incontinence. Obstet Gynecol 85(4):483–487
Ellerkmann RM, Cundiff GW, Melick CF, Nihira MA, Leffler K, Bent AE (2001) Correlation of symptoms with location and severity of pelvic organ prolapse. Am J Obstet Gynecol 185(6):1332–1338
Novi JM, Jeronis S, Morgan MA, Arya LA (2005) Sexual function in women with pelvic organ prolapse compared to women without pelvic organ prolapse. J Urol 173:1669–1672
Tok EC, Yasa O, Ertunc D, Savas A, Durukan H, Kanik A (2010) The effect of pelvic organ prolapse on sexual function in a general cohort of women. J Sex Med 7:3957–3962
Acknowledgments
We would like to thank the Care Management Center (NGA-25) and the Urogynecology Center (NUG) of Jaú city, São Paulo state, for authorizing the interviews and the use of the questionnaire in patients from the “Unified Health System” (SUS). We also thank the nurse master Professor Renata Cristina de Oliveira Souza Castro of the NUG/NGA-25 for her care and patience in the collection of data for this study. We are also indebted to Dr. José Tadeu Nunes Tamanini, urologist from the NUG/NGA-25, for his professionalism and sense of ethical responsibility which guided the Portuguese validation of this questionnaire. Finally, our grateful thanks are extended to the Medical Sciences Faculty of the Santa Casa de São Paulo Hospital and Irmandade Casa de Misericórdia de São Paulo.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Santana, G.W.R.M., Aoki, T. & Auge, A.P.F. The Portuguese validation of the short form of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12). Int Urogynecol J 23, 117–121 (2012). https://doi.org/10.1007/s00192-011-1505-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-011-1505-1