
Abstract
Introduction and hypotheses
The aim was to evaluate the long-term (5 years) effect of performing a retropubic tension-free vaginal tape (TVT) operation after a prior failed mid-urethra sling procedure and try to identify reasons for failure of the primary operation.
Methods
We identified 26 women to whom a repeat mid-urethra sling procedure (using the TVT Gynecare device) had been performed. Both the primary and repeat operations were retropubic procedures. Four different tape materials had been utilized in the primary procedure.
Results
Twenty women (77%) of the identified 26 women participated in the study. Seventy-five percent of the women were cured or significantly improved after the repeat TVT procedure. Reasons for failure of the primary procedure were grouped as follows: inadequate tape material (four out of 20), inadequate surgical technique (six out of 20), patients' medical condition (four out of 20), and unrecognized reasons (six out of 20).
Conclusions
A retropubic mid-urethra sling operation can be considered after failed mid-urethra sling surgery.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
One of the challenges of incontinence surgery for the treatment of female stress incontinence is the degree of effectiveness achieved and the durability of cure. Traditional surgical procedures as colposuspension and bladder neck supporting slings have a long-term cure rate around 70% at most [1]. Many other less invasive methods have been associated with a rapid decline of cure by time. Needle suspensions are, for instance, effective only for a few years with a cure rate of only 23% after 4 years [2], and the same is true for periurethral bulking, only 30% cured after 4 years follow-up [3]. The dilemma has always been which surgical procedure to use once one has failed either from the start or by time. The first modern mid-urethral tape operation, the tension-free vaginal tape (TVT) procedure, has been shown to have cure rates between 80% and 90% [4]. Long-term prospective follow-up of the results of the TVT procedure confirms that there is no decline in cure rate by time during follow-up periods of more than 11 years [5]. It has also been shown that the TVT is effective as a secondary surgical procedure to cure stress incontinence after failed primary surgery performed with traditional methods [6, 7]. As demands for the use of minimally invasive incontinence procedures have become ever stronger, the need for assessing how a repeat mid-urethra sling procedure performs is evident. The aim of the present report was to evaluate the long-term effect of performing a retropubic TVT operation on women that have had a prior failed mid-urethra sling procedure and try to identify the reason for the failure of the primary operation.
Materials and methods
The Helsinki University Central Hospital is a tertiary referral center to which patients with a failed or complicated past incontinence operation are sent for considering reoperation. We identified 26 patients to whom a repeat mid-urethra sling procedure had been performed and for whom at least 3 years had passed since the repeat operation. Both the primary and the repeat mid-urethra sling operations were retropubic procedures with the policy of the hospital to perform the second operation using the retropubic TVT device (TVT, Gynecare, Johnson & Johnson, Sommerville, NJ, USA). The identified 26 women were invited to the clinic for evaluation of their continence status and overall well-being three or more years after the second operation. The study was approved by the Helsinki University Ethics Committee and a written consent was obtained from all the women.
The primary mid-urethra sling operations were performed during a time period between 1992 and 2002 and the repeat procedure between 1999 and 2004. The mean and median time between the first and repeat operation was 57 months (SD ±32 months, range 4–103 months). Four different tape materials had been used in the primary mid-urethra sling procedure (two polytetrafluoroethylene, five knitted polyester, one multifilament microporous polypropylene, and 12 monofilament macroporous polypropylene slings).
The repeat TVT procedure was performed after recurrent stress incontinence had been diagnosed urodynamically in 14 patients and by a cough stress test and by the detrusor instability score (DIS) [8], which is a validated questionnaire to identify mixed incontinence, in six patients. The TVT operation was performed according to Ulmsten et al. [9] in local anesthesia using 0.25 % prilocaine with adrenaline (epinephrine). Cystoscopy was performed twice during the operation after each retropubic pass of the TVT needle to detect possible bladder injury. Adjustment of the tape was performed by using the cough test allowing a few drops of saline to escape on vigorous coughing in order to avoid retention. The repeat TVT operations were performed by an experienced urogynecologist.
Evaluation during the follow-up visit after the repeat TVT operation included a 24-h pad weighing test, a cough stress test performed in a semilithotomy position with a comfortably filled bladder (200–300 mL), a careful gynecological examination to detect possible tape erosions or other adverse effects of the tape material, and a postvoid residual urine volume measurement. Subjective outcome of the repeat surgery was assessed by the following validated condition-specific quality of life questionnaires: the Incontinence Impact Questionnaire—Short Form (IIQ-7) [10], the urogenital distress inventory (UDI-6 )[10], the urinary incontinence severity score (UISS) [11], the DIS [8], and a visual analog score (VAS) [11] where 0 represents no urinary problems and 100 unbearable urinary complaints.
Overall cure was defined as a negative stress test and a negative pad test (≤8 g/24 h) and a VAS ≤15, women were regarded as significantly improved if either the stress test or the pad test was negative and the VAS was ≤30. All other women were regarded as failures. Patients with moderate or severe urinary symptoms in the UDI-6 questionnaire were also regarded as failures either because of urge or stress incontinence according to which questions were ticked for.
The Statistical Package for Social Sciences (SPSS for Windows 15.0, Chigaco, IL, USA) was used for statistical analysis. Descriptive statistics used for continuous variables were mean, median, and range, and for categorical variables, the frequencies. For analysis of continuous variables with non-normal distribution the Wilcoxon nonparametric two-related samples test was used. A p < 0.05 was considered statistically significant.
Results
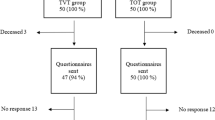
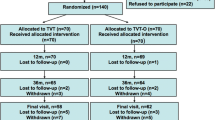
Twenty women of the identified 26 (77%) women participated in the study. Two patients had died from reasons unrelated to incontinence surgery, two women refused to participate in the study, and two women were lost to follow-up. The patient characteristics are shown in Table 1. The mean follow-up time since the repeat operation was 64 months (median 61 months, range 34–100 months), which is more than 5 years.
The primary operation was performed in several different hospitals throughout the country and, therefore, the data of these patients were not consistent and all desired information had not been obtained.
The tape placed during the primary operation was not especially identified if it was still in place. The primary tape had been partly or entirely removed between 2 and 72 months after the primary surgery in eight patients due to fistulation and infection. The tape had been cut before the repeat operation in one patient due to retention. There were no intraoperative complications during the repeat operation, although reasonable resistance in passing the TVT needle retropubically due to scar tissue was noted in some of the patients. One retropubic hematoma was found postoperatively, which resolved uneventfully without intervention. Tape exposure was seen in one patient after the repeat procedure at her last follow-up visit.
The stress test was negative in 15 patients (75%) and the pad test was negative in 13 patients (65%). Eleven patients had both a negative stress test and a negative pad test (55%) and fulfilled the criteria of objective cure. Four patients (20%) were significantly improved according to the criteria set, although one of these patients scored 0 on her VAS score and regarded herself as cured. One patient among the improved had urge predominant mixed incontinence and she also had had urge problems before the second operation. Five patients (25%) were failures both by objective and subjective criteria. Two of the failed patients were elderly frail patients with several medical conditions as obstructive pulmonary disease, diabetes mellitus, obesity, and preoperative mixed incontinence. These patients as all the others were offered conservative treatment of their recurrent incontinence but demanded surgical treatment.
There was a highly significant shift towards a normal continence condition from 60 to 5 in the UISS (p < 0.001) and a significant shift in the same direction in the VAS score from 69 to 5 (p = 0.021). The results of the condition-specific quality of life questionnaires are shown in Table 2.
All available clinical data was scrutinized in an attempt to identify the reasons of failure of the primary operation. According to available data, the most probable reasons of failure were grouped into the following categories: inadequate tape material (four patients), inadequate surgical technique (six patients), patients' medical condition (four patients), and unrecognized reasons (six patients). Table 3 shows the supposed reasons of failure of the primary mid-urethra retropubic sling procedure for each of the 20 patients and the 5-year follow-up results of the repeat TVT operation.
Eight patients were initially treated with tape materials other than monofilament macroporous polypropylene. Four of these tapes (50%) had been removed because of fistulation and infection and removal of the tape led to recurrent incontinence. One patient became incontinent after she had experienced a subarachnoidal hemorrhage with hydrocephalus formation 5 years after the first operation. In three cases, the reason for recurrence of incontinence between 3 and 24 months after the primary operation could not be identified.
Monofilament macroporous polypropylene tape was used in the primary operation of 12 patients; and in five of these cases (42%), a protrusion of the tape was seen. Inadequate surgical technique was regarded to be the reason for failure of the first operation in six cases. In three of these cases, protrusion of the tape was noticed at the first control visit, the women being continent but complaining of discomfort which led to resection or removal of the tape and recurrence of symptoms. In one case, a bladder perforation during the first operation led to the removal of the left arm of the tape and reinsertion of a new tape on the left side, which was then sutured to the right-sided tape in the midline. In this case, incontinence symptoms reoccurred 1 year after the first operation; and 5 years later, the tape erosion was noticed. In one case with postoperative retention problems, the tape was cut; and in one case of late detection of bladder perforation, the tape was removed and these operations led to recurrence of incontinence. Medical conditions as diabetes, obesity, obstructive pulmonary disease, and weight gain were identified as possible reasons for failure in three patients. In two patients, no clear reason for failure of the primary operation with polypropylene tape could be detected. In one case, the recurrence occurred 2 months postoperatively when the patient was carrying heavy weights; and in one case, after 6 years postoperatively without any explanation.
Discussion
The present study reveals that a 75% long-term objective cure or significant improvement rate after a repeat mid-urethra sling operation using the TVT procedure can be achieved. Petrou and Frank [12] reported a 57% short-term subjective cure or improvement rate after repeat traditional pubovaginal sling operations with a mean follow-up of 17 months. The TVT procedure has been shown to be effective in the treatment of recurrent stress urinary incontinence after traditional incontinence operations with objective cure rates between 70% and 90% [6, 7, 13]. The effectiveness of the repeat TVT procedure of the present study thus did not fully reach the rates seen in reports where TVT has been performed after traditional incontinence operations but the results seem to be superior to those achieved when performing traditional sling operations twice [12].
Reports on repeat mid-urethra sling operations are scarce. Most reports include small number of patients and with short follow-up times. Usually, both the primary and secondary operations include a variety of different mid-urethra tape procedures, mixing retropubic and transobturator approaches. Two reports with more than ten patients were identified from the literature [14, 15], the rest including five or less patients are all with short-term follow-up. In the report by Tsivian et al. [14], 12 patients were treated with repeat TVT, IVS, or TOT due to persistent or recurrent stress urinary incontinence after previous mid-urethra operations and the cure rate was 92% after a mean follow-up of 23 months. In a study by Lee et al. [15], 29 patients were followed up for at least 1 year after repeat TVT, TVT-O, or TOT operation and the cure rate was 76% where cure was defined as a negative stress test and absence of any involuntary urinary leakage during stressful activities. In the study of Lee et al., the retropubic TVT had a substantially higher cure rate of 92% than the transobturator approach with a cure rate of 63% as a repeat operation. A few reports with five or less patients having repeat mid-urethra tapes followed up for 6–12 months show good results [16–19].
A few reports have been published on complications caused by the sling material when used vaginally. Weinberger and Ostergard [20] reported that 22% of the polytetrafluoroethylene (Teflon) suburethral slings had to be removed because of complications. Sling surgery with knitted polyester/polyethylene terephtalate (Mersilene) has been associated with a tissue intolerance of 0–3% [21]. Multifilament microporous polypropylene has been associated with as much as 24% of erosion and sinus formation requiring sling removal [22]. The currently most commonly used tape material is macroporous monofilamental polypropylene which has very little adverse tissue reactions although erosion rates of between 0% and 2% have been reported [5, 21, 23].
In the early 1990s when the development of the TVT operation was ongoing, materials other than macroporous monofilament polypropylene were used and both fistulation and erosion of the tape was seen in these patients. In the present study, there were eight out of the total 20 patients who had other than a polypropylene sling at the primary operation. Four of these slings had to be removed because of complications and thus led to recurrence of incontinence. Another three patients developed recurrent incontinence with the tape in place and the reason for failure remained unidentified. It might be that the mechanical properties of these Mersilene slings are not as favorable as the polypropylene slings of the TVT procedure with its special knitting and elasticity.
Possible underlying reasons for failure of mid-urethra tape procedures have been identified. Such are prior incontinence operations [24], mixed incontinence [25, 26], age [27], low-pressure urethra [28], and obesity [27]. Reasons for failure are probably multifactorial also including inadequate surgical technique. In the present study, three patients (15%) had had incontinence surgery before the first mid-urethra operation and two of these failed also after the second operation. We know that when the number of incontinence operations increases, the risk of failures increases [12]. Inadequate surgical technique was regarded as the cause of failure in six patients. Either the tape was placed wrongly in the bladder and had to be removed or the tape perforated the vaginal mucosa causing protrusion of the tape, which caused discomfort to the patient or her partner and resulted in removal of the tape. These patients were continent before removal of the tape and understandably became incontinent after removal, the reason of which, however, was inadequate placement of the tape.
The mean body mass index before the repeat operation was 28 in the group of failed and 24 in the group of cured patients. Failed patients were also older than cured women (mean age 62 and 53, respectively) but the difference was not statistically significant due to the small number of patients. The repeat TVT procedure failed in five patients of the present study. Four of these five patients had symptoms of mixed incontinence already before the primary operation and were found to have stress predominant mixed incontinence before the repeat operation. As reports on 50–80% relief of urgency symptoms in women with mixed incontinence after TVT surgery have been published [4], we found it justified to perform the repeat operation on these women as they requested. Two of these patients were elderly with medical conditions as diabetes and obstructive pulmonary disease and two had low-pressure urethra. One patient gained weight after the primary operation and had recurrence of incontinence after 2 years. She underwent the repeat TVT, which resulted in dryness, but 2 years later when she lost 11 kg of weight, recurrence of incontinence appeared once again 2 years after the repeat procedure. Weight changes may have an influence on the results of surgery.
Because of the high cure rates after TVT surgery, it has been difficult to obtain greater number of failures to whom repeat mid-urethra sling procedures have been undertaken. Therefore, the knowledge of how repeat mid-urethra sling operations perform is unclear. When the reasons for failure of the primary procedure mostly have stayed unexplained and the repeat procedure has not necessarily been the same as the primary one, knowing that cure rates differ between different approaches [29, 30], it is difficult to assess the cause of a repeat failure.
The weakness of our study is the small number of patients, although it is the second biggest in the literature thus far. One of its strengths is that both the primary and secondary operations have been performed in the same way, with the repeat procedure always being the retropubic TVT operation. Another strength is the long-term 5 years follow-up after the repeat operation and that we made every effort to identify the causes of failure after both the primary and repeat operation. We found that complications associated with a repeat mid-urethra sling procedure are not a problem. Cure rates after a repeat TVT are comparable to or better than after any repeat incontinence surgery. Failures are multifactorial as many of the failed cases of our report had several of the recognized risk factors for failure of mid-urethra sling procedures.
In conclusion, we think that a minimally invasive retropubic mid-urethra sling operation can be recommended after failed incontinence surgery even if the primary operation has been a mid-urethra sling procedure.
References
Alcalay M, Monga A, Stanton SL (1995) Burch colposuspension: a 10–20 year follow up. Br J Obstet Gynecol 102:740–745
Elkabir JJ, Mee AD (1998) Long-term evaluation of the Gittes procedure for urinary stress incontinence. J Urol 159:1203–1205
Corcos J, Fournier C (1999) Periurethral collagen injection for the treatment of female stress urinary incontinence: 4-year follow-up results. Urology 54:815–818
Nilsson CG (2004) Latest advances in TVT tension-free support for urinary incontinence. Surg Technol Int 12:171–176
Nilsson CG, Palva K, Rezapour M, Falconer C (2008) Eleven years prospective follow-up of the tension-free vaginal tape procedure for treatment of stress urinary incontinence. Int Urogynecol J 19:1043–1047
Rezapour M, Ulmsten U (2001) Tension-free vaginal tape (TVT) in women with recurrent stress urinary incontinence--a long-term follow up. Int Urogynecol J Pelvic Floor Dysfunct 12(Suppl 2):9–11
Kuuva N, Nilsson CG (2003) Tension-free vaginal tape procedure: an effective minimally invasive operation for the treatment of recurrent stress urinary incontinence? Gynecol Obstet Invest 56:93–98
Kauppila A, Alavaikko P, Kujansuu E (1982) Detrusor instability score in the evaluation of stress urinary incontinence. Acta Obstet Gynecol Scand 61:137–141
Ulmsten U, Henriksson L, Johnson P, Varhos G (1996) An ambulatory surgical procedure under local anesthesia for treatment of female urinary incontinence. Int Urogynecol J 7:81–85
Ubersax JS, Wyman JF, Shumaker SA, McClish DK, Fantl JA (1995) Short forms to assess life quality and symptom distress for urinary incontinence in women: the incontinence impact questionnaire and urogenital distress inventory. Continence program for women research group. Neurourol Urodyn 14:131–139
Stach-Lempinen B, Kujansuu E, Laippala P, Metsanoja R (2001) Visual analogue scale, urinary incontinence severity score and 15 D-psychometric testing of three different health-related quality-of-life instruments for urinary incontinent women. Scand J Urol Nephrol 35:476–483
Petrou SP, Frank I (2001) Complications and initial continence rates after a repeat pubovaginal sling procedure for recurrent stress urinary incontinence. J Urol 165:1979–1981
Liapis A, Bakas P, Lazaris D, Creatsas G (2004) Tension-free vaginal tape in the management of recurrent stress incontinence. Arch Gynecol Obstet 269:205–207
Tsivian A, Neuman M, Yulish E, Shtricker A, Levin S, Cytron S et al (2007) Redo midurethral synthetic sling for female stress urinary incontinence. Int Urogynecol J 18:23–26
Lee KS, Doo CK, Han DH, Jung BJ, Han JY et al (2007) Outcomes following repeat mid urethral synthetic sling after failure of the initial sling procedure: Rediscovery of the tension-free vaginal tape procedure. J Urol 178:1370–1374
Riachi L, Kohli N, Miklos J (2002) Repeat tension-free transvaginal tape (TVT) sling for the treatment of recurrent stress urinary incontinence. Int Urogynecol J 13:133–135
Villet R, Ercoli A, Atallah D, Hoffmann P, Salet-Lizee D (2002) Second tension-free vaginal tape procedure and mesh retensioning: two possibilities of treatment of recurrent-persistent genuine stress urinary incontinence after a primary tension-free vaginal tape procedure. Int Urogynecol J 13:377–379
Moore RD, Gamble K, Miklos JR (2007) Tension-free vaginal tape sling for recurrent stress incontinence after transobturator tape sling failure. Int Urogynecol J 18:309–313
Lo TS, Lee SJ (2007) Simple sling resection and a second, intermediate polypropylene mesh for treatment of vaginal tape protrusion concurrent with recurrent urinary stress incontinence after TVT procedure. J Obstet Gynaecol Res 33:739–742
Weinberger MW, Ostergard DR (1995) Long-term clinical and urodynamic evaluation of the polytetrafluoroethylene suburethral sling for treatment of genuine stress incontinence. Obstet Gynecol 86:92–96
Cosson M, Debodinance P, Boukerrou M, Chauvet MP, Lobry P et al (2003) Mechanical properties of synthetic implants used in the repair of prolapse and urinary incontinence in women: which is the ideal material? Int Urogynecol J 14:169–178
Balakrishnan S, Lim YN, Barry C, Corstiaans A, Kannan K et al (2007) Sling distress: a subanalysis of the IVS tapes from the SUSPEND trial. Aust N Z J Obstet Gynaecol 47:496–498
Comiter CV (2006) Surgery insight: management of failed sling surgery for female stress urinary incontinence. Nat Clin Pract Urol 3:666–674
Meschia M, Pifarotti P, Gattei U, Bertozzi R (2007) Tension-free vaginal tape: analysis of risk factors for failures. Int Urogynecol J 18:419–422
Debodinance P, Delporte P, Engrand JB, Boulogne M (2002) Tension-free vaginal tape (TVT) in the treatment of urinary stress incontinence: 3 years experience involving 256 operations. Eur J Obstet Gynecol Reprod Biol 105:49–58
Kulseng-Hanssen S, Husby H, Schiotz HA (2008) Follow-up of TVT operations in 1, 113 women with mixed urinary incontinence at 7 and 38 months. Int Urogynecol J 19:391–396
Hellberg D, Holmgren C, Lanner L, Nilsson S (2007) The very obese woman and the very old woman: tension-free vaginal tape for the treatment of stress urinary incontinence. Int Urogynecol J 18:423–429
Rezapour M, Falconer C, Ulmsten U (2001) Tension-free vaginal tape (TVT) in stress incontinent women with intrinsic sphincter deficiency (ISD)—a long-term follow-up. Int Urogynecol J 12(Suppl2):12–14
Araco F, Gravante G, Sorge R, Overton J, De Vita D, Sesti F et al (2008) TVT-O vs TVT: a randomized trial in patients with different degrees of urinary stress incontinence. Int Urogynecol J 19:917–926
Novara G, Ficarra V, Boscolo-Berto R, Secco S, Cavalleri S, Ficarra V et al (2007) Tension-free midurethral slings in the treatment of female stress urinary incontinence: a systematic review and meta-analysis of randomized controlled trials of effectiveness. Eur Urol 52:663–678
Acknowledgements
This study has been supported by grants of the Finnish Medical Association.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Palva, K., Nilsson, C.G. Effectiveness of the TVT procedure as a repeat mid-urethra operation for treatment of stress incontinence. Int Urogynecol J 20, 769–774 (2009). https://doi.org/10.1007/s00192-009-0849-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-009-0849-2