
Abstract
The objective of this study is to assess the objective recurrence and complications of adjuvant materials in the treatment of anterior vaginal wall prolapse. The inclusion criteria were randomised controlled trials (RCTs) using adjuvant materials versus standard surgery for anterior vaginal wall prolapse. The main outcome measures were objective recurrence and complications. Ten RCTs (1,087 patients) were included in the systematic review. Meta-analysis showed a lower risk of objective recurrence after 1 year in the patients having an anterior repair with a biological adjuvant material (odds ratio 0.56; 95% confidence interval 0.34–0.92) and absorbable synthetic adjuvant material (odds ratio 0.44; 95% confidence interval 0.21–0.89). The evidence for the use of biological adjuvant materials in anterior vaginal wall prolapse surgery shows trends towards reduction of objective recurrence at 12 months.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It is estimated that the lifetime risk of having prolapse or incontinence surgery by age 80 is 11.1% and the risk of having a second operation is about 29.2% [1]. Implanted adjuvant materials (grafts) are being used with increasing frequency by pelvic reconstructive surgeons [2]. It seems logical that reinforcing with stronger material rather than re-using the same weak connective tissue that failed will strengthen the repair.
Outside the field of urogynaecology, the use of adjuvant materials in incisional hernia has been explored. In cases of small incisional hernias, the recurrence rates were 67% in suture repair compared to 17% with adjuvant material repair over an 81-month follow-up [3].
An ideal adjuvant material is one that is biocompatible, chemically and physically inert, non-carcinogenic, mechanically strong, non-allergenic, non-modified by body tissue, resistant to infection and inexpensive [4]. Adjuvant materials can be classified by material type, weave and pore size and may be biological or synthetic. Biological adjuvant materials (grafts) are in the form of allograft, autografts and xenografts. Autografts are taken from the patient themselves (e.g. fascia lata from the thigh). Allografts are taken from a similar species while xenografts are taken from another species (e.g. porcine dermis or small intestine submucosa). Synthetic adjuvant materials may be classified as absorbable and non-absorbable and the pore size classified as macro-porous (>75 μm) and micro-porous (<75 μm) [4]. The pore size and weave of mesh may be important in whether the body can mount an immune response against bacteria [1].
Currently, there is a dearth of robust data to support the use of adjuvant material in prolapse surgery and most of the data available are from the manufacturer, which can cause bias. In addition, the existent data that are published are in the form of case series; with its inherent biases, there may be little incentive for companies to produce randomised controlled data due to financial drive to get a product onto the market.
In vaginal surgery, the most common site for recurrence is in the anterior vaginal wall with reported failure rates ranging from 20% to 40% [5]. We can assume that the factors that cause a prolapse in the first instance are also the cause of the recurrence. However, factors such as grade of the prolapse, type of surgery, experience of the surgeon and age of the patient at first repair can also play a part [6].
The objectives of this review were to determine the efficacy of the use of adjuvant material in surgical treatment of anterior vaginal wall prolapse in randomised controlled trials (RCTs) and to explore the rates of adverse events. Because of the more recent RCT data included, this review is more up to date, when compared to the one in the Cochrane library [7]. Furthermore, this review looks at anterior repairs using biological and synthetic grafts as separate entities.
Materials and methods
A prospective peer-reviewed protocol for this review was prepared a priori as per published guidelines. The components of the protocol consisted of the following: identifying the review questions, the search strategy including search terms, the study selection criteria, study quality assessment checklist and data extraction and synthesis [8].
Sources
All reports which describe (or might describe) RCTs and quasi-randomised trials of the use of adjuvant materials in anterior vaginal wall prolapse surgery were obtained. The databases searched included Cochrane Incontinence Group Trials Register (September 2007), CENTRAL (The Cochrane Library, Issue 3, 2007), MEDLINE (1966 to September 2007), EMBASE (1980 to September 2007), CINAHL (1982 to September 2007) and the National Library of Health.
The following keywords were used for the search as text words or subject headings using OVID software: ‘pelvic organ prolapse AND cystocele AND anterior colporrhaphy AND mesh.’ We also hand-searched the bibliographies of all relevant reviews and primary studies to identify articles not captured by electronic searches. In addition, a hand search of conference proceedings of the International Continence Society and International Urogynaecological Association (2004–2007) was performed. In most cases, the first or corresponding authors of included trials were contacted for additional information. Attempts were made to contact the authors of seven abstracts [10, 12, 23, 24, 26, 28, 29]. Three authors responded and provided the complete transcripts of the study [10, 12, 24]. In cases where the same article has been published as an abstract, complete article or presented at a meeting, then reference would be made to the published completed article in this text [9–13].
Study selection
The inclusion criteria were prospective RCTs comparing anterior vaginal wall repair with and without adjuvant material. The main outcomes assessed were objective recurrence, dyspareunia, voiding difficulties, adjuvant material erosions and prolapse symptoms. Two authors (PL and RF) performed the selection of trials for inclusion after employing the search strategy described previously.
All assessments of the quality of trials and data extraction were performed independently by two authors (PL and RF) using forms designed according to Cochrane guidelines. Data on characteristics of the study participants including details of inclusion criteria, interventions, methods used to measure success (or definitions of cure/failure) and adverse events were extracted. Wherever there were two or more publications by the same author on same topic, we assessed the quality of data from both and used the most up-to-date or larger dataset for meta-analysis. The following quality criteria and methodological details were assessed: method of randomisation; quality of allocation concealment until randomisation, sample size, proportion of women lost to follow-up and whether an intention-to-treat analysis and a power calculation were done.
Statistical analyses were performed according to the statistical guidelines of the Cochrane Collaboration [14]. Data from intention-to-treat analyses were used where available. For the dichotomous data, results of each study were expressed as Peto odds ratio (OR) with 95% confidence intervals (CI) and combined for meta-analysis using the Peto-modified Mantel–Haenszel method [15]. The outcome of recurrence and other adverse events were a negative consequence; therefore, higher odds were considered to be detrimental. Conversely, lower odds ratio meant that risk of adverse event including recurrence was lower in the adjuvant material (experimental) group. Heterogeneity was assessed by P value and I 2 test [16].
Results
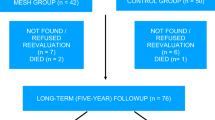
Figure 1 summarises the trial flow for identifying the potentially relevant RCTs involving the use of adjuvant material in the treatment for prolapse surgery. There were two studies that looked at the use of adjuvant material in both anterior and posterior vaginal prolapse and these studies were excluded as the data could not be teased out [20, 21]. Ten RCTs containing 1,087 women in total were included in the review (details given in Table 1) [9, 10, 12, 13, 17–29]. The surgical techniques in all the studies were described and performed using “standard or traditional techniques” and these were clarified in five studies [10, 13, 22, 25, 27]. The primary outcome in all trials was cure–recurrence. There was a wide variation in the method used to report cure. Outcomes were assessed at various time periods following surgery between 3 and 24 months. The studies also reported a range of other adverse events, the most common being erosions and dyspareunia reported in five and three studies, respectively [10, 13, 22–24, 29]. Biological adjuvant materials were used in four RCTs [10, 24–26] and synthetic adjuvant materials were used in the experimental group in six studies [13, 22, 23, 27–29]. Amongst the synthetic adjuvant materials used, two studies used absorbable material [22, 27]. The ten studies compared the use of adjuvant material in anterior repairs with standard anterior repairs [10, 13, 22–28]. All the studies included in the meta-analysis were primary repairs [10, 24, 25].

Study selection process for systematic review of the use of adjuvant material in anterior vaginal wall repair
As shown in Fig. 2, the included studies were of varying quality with some studies published as abstracts only. Three trials reported adequate concealment prior to allocation [10, 13, 22]. There was an adequate description of the method of randomisation in seven studies [10, 13, 22, 24, 25, 27, 28]. Intention-to-treat analysis was reported in seven studies while power calculation was done in five studies. In two trials, the follow-up was inadequate (more than 15% of randomised participants withdrew or were lost to follow-up) [22, 23].

Methodological quality of studies included in the systematic review of effectiveness and complications of adjuvant material in anterior vaginal wall prolapse surgery
Figure 3 provides a summary of the results of the meta-analyses.

Meta-analysis of recurrence of prolapse 1 year following surgery using adjuvant material versus a standard anterior repair
In this review, recurrence was defined as Ba greater than or equal to −1. The outcome measured in the meta-analysis was recurrence at 12 months and only three studies using biological adjuvant materials (450 patients) and one study using absorbable synthetic adjuvant material (143 patients) qualified. Three studies assessed recurrence in less than 12 months [23, 26, 29] while the other studies defined recurrence differently [13, 22, 28].
On meta-analyses, there was a lower recurrence in the group who had an anterior repair with a biological adjuvant material (odds ratio 0.56; 95% confidence interval 0.34–0.92) and polyglactin adjuvant material (OR 0.44; 95% CI 0.21–0.89). A meta-analysis of non-absorbable synthetic adjuvant material could not be performed.
Figure 4 quantifies the risks of various complications by the type of adjuvant material. We looked at studies reporting their erosion rates for patients undergoing anterior repairs only. The erosion rates amongst studies using non-absorbable and absorbable synthetic adjuvant material were 14% (21/150) and 2.9% (1/35), respectively, whilst amongst the studies with biological adjuvant material it was 0.67%(1/150). Only one study looked at re-operation rate for prolapse and this rate was 1% in both the adjuvant material and the control group [13]. The number needed to treat with biological adjuvant material to prevent recurrence at 12 months post-operatively was 13 (95% CI 6.5–85.3) and with absorbable synthetic adjuvant material was six (95% CI 3.0–33.8). As there were only three studies in the meta-analysis, the funnel plot or other tests for publication bias were not performed [30].

Risk of complications following the use of adjuvant material in anterior vaginal wall prolapse surgery
Discussion
Women who had anterior vaginal wall repair with adjuvant material had a lower risk of recurrence of prolapse at 1 year post-operatively compared to patients undergoing standard repair. The confidence intervals are wide and there was insufficient data to suggest any difference in the risk of dyspareunia, voiding difficulties and recurrent prolapse symptoms in the two groups.
There are several strengths of this review. The search was thorough and systematic. Two reviewers independently did the study selection and data extraction to minimise errors. We adhered to the QUOROM checklist while reporting the meta-analyses [31]. There were also no language restrictions in the literature search; however, all the articles and abstracts retrieved were in English. The data for biological and synthetic adjuvant material were sub-grouped to assess whether there was any significant difference in the recurrence rates.
There was no uniformity in reporting of the outcomes in the intervention studies of prolapse repairs. All studies used the endpoints of the recurrence of prolapse, dyspareunia post-operatively and the incidence of erosions but the method of assessing the outcomes varied as did the definitions of subjective and objective success of the operations. Some studies used reference point at Ba < −2 while others used Ba < −1 to define objective cure. The subjective cure rates are of prime importance to patients and clinicians [32]. Only two RCTs reported data on subjective improvement by means of validated questionnaires or visual analogue scales [22, 29].
Interestingly, despite the widespread interest in the use of adjuvant material in surgery, there has only been one RCT of synthetic adjuvant material in the published literature since 2001 [13]. There were however three studies that were published as abstracts for international meetings [23, 28, 29]. This might represent a greater inclination to use biological adjuvant material for trial purposes. Five of the RCTs were in the form of abstracts and not yet published as complete articles [23, 24, 26, 28, 29]. There was no significant difference in the complications such as voiding difficulties, dyspareunia and prolapse symptoms following the use of both synthetic and biological adjuvant material when compared to standard anterior repairs. This could be due to the small number of subjects included in these studies and therefore the need for larger studies. There have been reports of retrovesical haematoma, erosion into the bladder and vesicovaginal fistula after the use of anterior vaginal adjuvant material [33, 34]. There was also a wide range of adjuvant material used, from biological adjuvant material like Pelvicol and fascia lata to non-absorbable and absorbable synthetic adjuvant material such as polypropylene or polyglactin. This along with different definitions of recurrence might explain heterogeneity amongst the studies.
One must remember that it is a relatively new operation, so there should be appropriate clinical governance procedures in place. The reduced risk of recurrence may appear to make the use of adjuvant material in repair preferable in women with recurrent prolapse but needs to be investigated specifically in this subgroup of patients.
There were insufficient data to suggest any difference in re-operation rate for prolapse in the two groups. Patients suffering erosions may need to have second operation but some can be treated conservatively (for example with estrogen cream). With the erosion of 11.9% amongst adjuvant material, one has to take this into consideration when calculating the economic benefit of using adjuvant material. The publication bias could not be assessed meaningfully as there were only three studies included in the meta-analysis.
Patients should be counselled that long-term data on effectiveness and adverse events are still awaited. If clinicians are to perform adjuvant material procedures, then data should ideally be collected for audit purposes. In the UK, there is the British Society of Urogynaecology database (URL: www.rcog.org.uk/bsug) to enable the best chance of collection of robust observational data at a national level.
To help resolve the issue of medium- to long-term effectiveness and complications, clinicians may initiate good quality and adequately powered trials with long-term follow-up or participate in ongoing robustly designed multicentre trials. The main issues are sample size and trial methodology. An individual patient data meta-analysis may address the uncertainty by combining raw data from various studies included in this review as well as the data from ongoing studies.
This review shows the need for more methodologically sound and sufficiently powered RCTs with a longer follow-up before meshes can be introduced widely into clinical practice. The need also for more standardised outcomes to be measured cannot be over-emphasised.
References
Olsen AC, Smith VJ, Bergstrom JO et al (1997) Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 89:501–506
Davila GW (2006) Introduction to the 2005 IUGA grafts roundtable. Int Urogynaecol J 17(suppl 1):S4–S5
Burger JW, Luijendijk RW, Hop WC et al (2004) Long term follow up of a randomized controlled trial of suture versus mesh repair of incisional hernia. An Surg 240:578–583
Griffis K, Hale DS (2005) Grafts in pelvic reconstructive surgery. Clin Obstet Gynecol 48(3):713–723 Sept
Julian TM (1996) The efficacy of Marlex mesh in the repair of severe, recurrent vaginal prolapse of the anterior midvaginal wall. Am J Obstet Gynecol 175:1472–1475
Diez-Itza I, Aizpitarte I, Becerro A (2007) Risk factors for the recurrence of pelvic organ prolapse after vaginal surgery: a review at 5 years after surgery. Int Urogynecol J 18:1317–1324
Maher C, Baessler K, Glazener CMA, Adams EJ, Hagen S (2007) Surgical management of pelvic organ prolapse in women. Cochrane Database Syst Rev (3):CD004014. doi:10.1002/14651858.CD004014.pub3
Khan K, ter Riet G, Popay J, Nixon J, Kleijnen J (2001) Undertaking systematic reviews of research on effectiveness (CRD Report No 4). University of York, York
Meschia M, Pifarotti P, Riva D, Bernasconi F, Magatti F, Kocjancic E (2006) Pelvicol implant for anterior vaginal wall prolapse repair: a two years randomized follow-up study. Int Urogynecol J 17(Suppl 2):S64–S65
Meschia M, Pifarotti P, Riva D, Bernasconi F, Magatti F, Kocjancic E (2007) Porcine skin collagen implants (Pelvicol) to prevent vaginal wall prolapse recurrence. A multicentre randomized study. J Urol 177:192–195
Kocjancic E, Crivellaro S, Bernasconi F, Magatti F, Frea B, Meschia M (2007) A two years follow up, prospective randomized study on cystocele repair with or without Pelvicol implant. www.abstracts2view.com/aua/view.php?nu=AUA07L1_93519
Hiltunen R, Nieminen K, Takala T, Heiskanen E, Merikari M, Nieme K, Hienonen P (2006) Transvaginal mesh repair of the anterior compartment prolapse: a randomized comparing prospective study. Int Urogynecol J 17(Suppl 2):S142
Hiltunen R, Nieminen K, Takala T, Heiskanen E, Merikari M, Nieme K, Hienonen P (2007) Low-weight polypropylene mesh for anterior vaginal wall prolapse. Obstet Gynecol 110:455–462
Deeks J, Altman DG, Bradburn MJ (2001) Statistical methods for examining heterogeneity and combining results from several studies in meta-analysis. In: Egger M, Smith GD, Altman DG (eds) Systematic reviews in health care: meta-analysis in context, 1st edn. BMJ Books, London
Yusuf S, Peto R, Lewis J, Collins R, Sleight P (1985) Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis 27:335–371
Higgins JPT, Thompson SG (2002) Quantifying heterogeneity in meta-analysis. Stat Med 21:1539–1558
Higgs PJ, Carey MP, Goh JTW, Krause HG, Leong A, Cornish A (2006) Randomized controlled trial comparing vaginal prolapse repair with mesh augmentation to traditional vaginal repair: 6 month follow up. Int Urogynecol J 17(Suppl 2):S64
Meschia M, Pifarotti P, Gattei U, Magatti F, Kocjancic E, Bernasconi F, Riva D (2004) Multicentre randomized trial of PelvicolTM implant to prevent recurrence of anterior vaginal wall prolapse in women undergoing primary surgery for genital prolapse. http://www.icsoffice.org/publications/2004/PDF/0289.PDF
Meschia M, Pifarotti P, Magatti F, Bernasconi F, Riva D, Kocjancic E (2005) Porcine skin collagen implants (Pelvicol™) to prevent anterior vaginal wall prolapse recurrence: a randomised study. Neuro Urodynamics 24(5/6):587
Meschia M, Bacchichet R, Cervigni M, Guercio E, Maglioni Q et al (2007) A multicenter randomized trial on transvaginal mesh repair of severe genital prolapse with the Perigee–Apogee System: The PERAPO study. Int Urogynecol J 18(Suppl 1):S10
Lim JL, Carey MP, Higgs PJ, Goh J, Krause H, Leong A, Cornish A (2007) Vaginal colporrhaphy versus vaginal repair with mesh for pelvic organ prolapse: a randomised controlled trial. Int Urogynecol J 18(Suppl 1):S38
Weber M, Walter M, Marion R, Piedmonte MA, Ballard L (2001) Anterior colporrhaphy: a randomized trial of three surgical techniques. Am J Obstet Gynecol 185:1299–1306
Ali S, Han HC, Lee LC (2006) A prospective randomized trial using Gynemesh *PS for the repair of anterior vaginal wall prolapse. Int Urogynecol J 17(Suppl 2):S221
Guerette NL, Aguirre O, VanDrie DM, Biller DH, Davila GW (2006) A multi-center, randomized, prospective trial comparing anterior colporrhaphy alone to bovine pericardium collagen matrix graft reinforced anterior colporrhaphy: 12-month analysis. Int Urogynecol J 17(Suppl 2):S63–S64
Gandhi S, Goldberg R, Kwon C, Koduri S, Beaumont MS, Abramov Y, Sand P (2005) A prospective randomized trial using solvent dehydrated fascia lata for the prevention of recurrent anterior vaginal wall prolapse. Am J Obstet Gynecol 192:1649–1654
Hviid UH, Rudnicki M (2005) A randomised, controlled study of biomesh (Pelvicol) for vaginal anterior wall prolapse. Int Urogynecol J Pelvic Floor Dysfunct 16(suppl 2):S58
Sand PK, Koduri S, Lobel RW, Winkler HA, Tomezsko J, Culligan PJ et al (2001) Prospective randomized trial polyglactin 910 mesh to prevent recurrence of cystoceles and rectoceles. Am J Obstet Gynecol 184:1357–1362
Al-Nazer MA, Ismail WA, Gomaa IA (2007) Comparative study between anterior colporrhaphy versus vaginal wall repair with mesh for management of anterior vaginal wall prolapse. Int Urogynecol J 18(Suppl 1):S49–S50
Nguyen JN, Burchette RJ (2007) Anatomic support and visceral function following anterior colporrhaphy versus polypropylene mesh transobturator prolapse repair: a via trial. Int Urogynecol J 18(Suppl 1):S51
Begg CB (1994) Publication bias. In: Cooper H, Hedges LV (eds) The handbook of research synthesis. Russell Sage Foundation, New York, pp 399–409
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF (1999) Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Lancet 354:1896–1900
Tincello DG, Alfirevic Z (2002) Important clinical outcomes in urogynecology: views of patients, nurses and medical staff. Int Urogynecol J Pelvic Floor Dysfunct 13:96–98
Ignjatovic I, Stosic D (2007) Retrovesical haematoma after Prolift ((R)) procedure for cystocele correction. Int Urogynecol J 18:1495–1497
Yamada BS, Govier FE, Stefanovic KB, Kobashi KC (2006) Vesicovaginal fistula and mesh erosion after Perigee (transobturator polypropylene mesh anterior repair). Urology 68(5):1121.e 5–7 Epub 2006 Nov 7
Acknowledgements
The authors acknowledge contribution of Derek Yates, Librarian, who performed the systematic search.
Conflicts of interest
Mr. Toozs-Hobson has recruited for an RCT using SurgiSIS mesh in recurrent pelvic floor prolapse.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Foon, R., Toozs-Hobson, P. & Latthe, P.M. Adjuvant materials in anterior vaginal wall prolapse surgery: a systematic review of effectiveness and complications. Int Urogynecol J 19, 1697–1706 (2008). https://doi.org/10.1007/s00192-008-0668-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-008-0668-x