
Abstract
Purpose
Anterior cruciate ligament (ACL) graft failure is a complication that may require revision ACL reconstruction (ACL-R). Non-anatomic placement of the femoral tunnel is thought to be a frequent cause of graft failure; however, there is a lack of evidence to support this belief. The purpose of this study was to determine if non-anatomic femoral tunnel placement is associated with increased risk of revision ACL-R.
Methods
After screening all 315 consecutive patients who underwent primary single-bundle ACL-R by a single senior orthopedic surgeon between January 2012 and January 2017, 58 patients were found to have both strict lateral radiographs and a minimum of 24 months follow-up without revision. From a group of 456 consecutive revision ACL-R, patients were screened for strictly lateral radiographs and 59 patients were included in the revision group. Femoral tunnel placement for each patient was determined using a strict lateral radiograph taken after the primary ACL-R using the quadrant method. The center of the femoral tunnel was measured in both the posterior–anterior (PA) and proximal–distal (PD) dimensions and represented as a percentage of the total distance (normal center of anatomic footprint: PA 25% and PD 29%).
Results
In the PA dimension, the revision group had significantly more anterior femoral tunnel placement compared with the primary group (38% ± 11% vs. 28% ± 6%, p < 0.01). Among patients who underwent revision; those with non-traumatic chronic failure had statistically significant more anterior femoral tunnel placement than those who experienced traumatic failure (41% ± 13% vs. 35% ± 8%, p < 0.03). In the PD dimension, the revision group had significantly more proximal femoral tunnel placement compared with the primary group (30% ± 9% vs 38% ± 9%, p < 0.01).
Conclusion
In this retrospective study of 58 patients with successful primary ACL-R compared with 59 patients with failed ACL-R, anterior and proximal (high) femoral tunnels for ACL-R were shown to be independent risk factors for ACL revision surgery. As revision ACL-R is associated with patient- and economic burden, particular attention should be given to achieving an individualized, anatomic primary ACL-R. Surgeons may reduce the risk of revision ACL-R by placing the center of the femoral tunnel within the anatomic ACL footprint.
Level of evidence
Level III.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Anterior cruciate ligament reconstruction (ACL-R) failure rates have been reported between 3 and 17% after primary ACL-R [25, 28]. ACL-R failure is a severe complication, as patients who undergo revision ACL-R undergo another period of rehabilitation and may have worse clinical outcomes and lower rates of return to play [10, 13, 15]
Numerous reasons for ACL-R failure exist, including technical, traumatic, and biologic mechanisms. The Multicenter ACL Revision Study’s (MARS) analysis of 460 patients undergoing revision ACL-R found that technical error was responsible for failure 60% of the time, with non-anatomic femoral tunnel position being cited in 80% of these cases [13, 16]. Among patients where femoral tunnel malposition was cited as the only cause for failure, the tunnels were judged to be too anterior 30% of the time, and too vertical 36% of the time [16]. Placement of the ACL graft within the native femoral footprint, as opposed to outside of it, has been shown to reproduce kinematics more similar to that of the intact knee [17, 31]. The location of the tibial tunnel may also affect knee kinematics, as knees with tunnels placed in the posterior portion of the tibial footprint have been found to have increased anterior tibial translation compared with the intact knee [24].
The ACL’s native femoral insertion site may be evaluated on lateral radiographs, and has been measured in a cadaveric study by Bernard et al. as 25% of the distance from the posterior condyle along Blumensaat’s line and 29% of the height of the condyle measured orthogonally from Blumensaat’s line [1]. While anatomic ACL reconstruction may be considered a concept more so than a specific technique, it has been defined as the functional restoration of the ACL to its native dimensions, collagen orientation, and insertion sites [27]. In addition to biomechanical studies that demonstrated the advantage of anatomic ACL-R over non-anatomic techniques, a randomized control trial demonstrated small, but significantly improved anteroposterior and rotational stability of anatomic ACL-R compared with trans-tibial ACL-R [3, 7, 12, 17]. Despite improved biomechanics of anatomic ACL-R, conventional trans-tibial ACL-R may be sufficient for some patients due to participation in activities which are less demanding or at lower activity levels, as well as variation in individual anatomy [5, 14, 20]. However, objective data on femoral tunnel placement through radiologic measurement and its relationship to revision ACL-R has not been well established in the literature. Understanding the risks for revision surgery may help surgeons perform a more value-based ACL-R. “Value,” generally speaking, may be considered to be the ratio of benefits to costs. Therefore, a “value-based” ACL-R may be considered as one which aims to maximize the benefits of the surgery, as measured by patient reported outcomes, through evidence-based practice while minimizing the costs of additional procedures [2].
The purpose of this study was to assess the femoral tunnel position on routine post-operative plain films in patients who required revision ACL-R compared with those who did not. Moreover, to the best of the author’s knowledge, this is the first study to investigate femoral tunnel position and mechanism of failure in the context of revision ACL-R. It was hypothesized that patients who underwent revision ACL had femoral tunnels placed more anteriorly, more proximally, or both, when compared to patients who did not require ACL revision.
Materials and methods
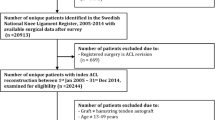
Following approval by the Institutional Review Board at University of Pittsburgh (STUDY1903019), a database search was performed for all primary, isolated single-bundle ACL-R performed by a single senior orthopedic surgeon (V.M.) between January 2012 and January 2017; a total of 315 patients were identified. Given the relative infrequency of revision ACL-R surgery, the database search was expanded to include all revision ACL-R at a single academic institution between January 2009 and January 2019, resulting in 456 individuals. Inclusion criteria included “strict” post-operative lateral knee radiographs, ACL-R without multi-ligamentous injury at time of index surgery, and minimum 2-year follow-up for primary ACL-R. Postoperative lateral knee radiographs were deemed “strict” if there was less than 6 mm of offset between the posterior halves of the medial and lateral condyles, as this has been shown to maximize inter-observer reliability (ICC = 0.77 for condylar offset of 0–6 mm) (Fig. 1) [18]. To minimize inclusion of patients in the primary group who eventually required revision, patients in the primary group required a minimum follow-up of 24 months. Exclusion criteria included concomitant ligament reconstruction procedures performed at the time of index surgery and two-tunnel femoral ACL-R. Of the 315 patients who underwent primary single-bundle ACL-R, 172 were excluded due to lack of a strict lateral radiogram, 67 were excluded due to insufficient follow-up, and 18 were excluded due to having undergone revision ACL-R within the follow-up period, leaving 58 patients in the primary group who met the inclusion criteria. Patients from the revision group were screened consecutively until 59 patients who met inclusion criteria and had strict lateral radiographs were included. To evaluate ACL-R failures by any potential mechanism, no time cut-off was used when screening cases of revision. One-hundred-and-seventeen patients were included in the final analysis.

Strict lateral knee radiograph. Examples of lateral knee radiographs. a demonstrates a “strict” lateral radiograph, determined when there was less than 6 mm of offset between the posterior walls of the medial and lateral femoral condyles, when measured perpendicular to the tangent of the curves. b Demonstrates an example of a lateral radiograph that does not meet criteria to be considered “strict,” as it was measured to have more than 6 mm of offset
Demographic data including age, sex, laterality, BMI, graft choice, length of follow-up, and time to failure (if applicable) were collected for all patients in each group and are shown in Table 1. For each patient, who underwent revision, the mechanism of failure was recorded as either chronic non-traumatic failure or traumatic failure.
Two blinded independent observers measured the center of the femoral tunnel on lateral radiographs according to the quadrant method described by Bernard et al. [1]. The quadrant method has been independently validated in a study investigating ACL insertion sites location based on two-dimensional analysis [26]. The authors repeated the quadrant method in 36 cadaveric knees and found the location of the ACL femoral footprint to not be significantly different from previously reported data using the same method [26]. The posterior–anterior (PA) dimension was defined as the total sagittal diameter of the lateral femoral condyle measured along the Blumensaat’s line, and the proximal–distal (PD) dimension was the height of the intercondylar notch defined as the distance between the Blumensaat’s line and a tangent to the distal subchondral bone contour of the condyle parallel to the Blumensaat’s line. The center of the femoral tunnel was reported as a percentage of each dimension. The center of the normal anatomic footprint of the ACL was 25% of the PA dimension and 29% of the PD dimension [1]. Both of the two blinded independent observer measured femoral tunnel position on 10 randomly selected lateral radiographs and an intraclass correlation coefficient (ICC) for absolute agreement between raters was calculated to ensure inter-observer reliability. Both observers repeated the same measurements a minimum of 3 months later to calculate intra-observer reliability (Table 2). The inter-rater reliability (ICC: 0.87–0.88) and intra-rater reliability (ICC: 0.60–0.90) were found to be consistent with previous studies [18]. Following this, the femoral tunnel position for all 117 patients was measured and recorded.
Statistical analysis
A student’s t test was performed to compare femoral tunnel position in each dimension, age, and BMI between individuals with intact ACL-R and those undergoing revision ACL-R. Fisher’s exact test was used to compare differences in gender, laterality, and autograft frequency. A multivariable logistic regression was calculated to predict revision status based on femoral tunnel placement in the PA and PD dimensions. Additionally, the interaction between the PA and PD dimension of each femoral tunnel was analyzed using the product of the deviation from the mean for each data point. Being in the primary group was coded as 0 and being in the revision group was coded as 1. A multivariate logistic regression was also performed on demographic and graft usage data on predictive ability for revision. Hamstring graft usage was the reference, against which all other grafts were compared. Sample size calculation was performed for independent study groups with continuous endpoints, using an alpha of 0.05 and a power of 80%. Using the exact mean and standard deviation of tunnel positions reported by Bernard et al., it was calculated that a sample of at least 32 patients was required to detect a difference between the primary and revised groups of at least one standard deviation (2.2% in PA dimension, 2.5% in PD dimension) in either dimension. Significance was set at p < 0.05. A post hoc means-based two-tailed power analysis using the final sample size and alpha set to 0.05 was performed. Post hoc power analysis demonstrated a power of 0.99 achieved for the PA dimension, as well as a power of 0.99 achieved for the PD dimension.
Results
Female patients who underwent revision were found to be significantly younger than females who did not (p < 0.05). There was no significant difference between autograft and allograft usage between the two groups. In the revision group, revision surgery ranged from 4 to 204 months after primary surgery, with a mean of 60.2 ± 50.5 months (median: 42 months). In the primary group, the minimum follow-up period was 24 months with a mean of 37.8 ± 15.6 months. Mechanism of failure data for those in the revision ACL-R group may be found in Table 3.
In the PA dimension, femoral tunnels were significantly more anterior in those patients who underwent revision compared to those who did not (38% ± 11% vs. 28% ± 6%, p < 0.01). Among patients who underwent revision, femoral tunnels were significantly more anterior in those who experienced non-traumatic chronic failure than those who experienced traumatic failure (41% ± 13% vs. 35% ± 8%, p = 0.03). Femoral tunnel position between just those who experienced traumatic failure and those with intact ACL-R was significantly different (35% ± 8% vs. 28% ± 6%, p < 0.01). Femoral tunnels that were 30% or more anterior, had an odds ratio for revision of 6 (95% CI 3–12, p < 0.01), and tunnels that were 40% or more anterior had an odds ratio for revision of 39 (95% CI 5–301, p < 0.01). Among those who underwent revision, femoral tunnels that were 37% or more anterior had an odds ratio for experiencing chronic non-traumatic failure of 3 (95% CI 1–9, p = 0.04). The average length of the femoral condyle in the PA dimension was found to be 48 ± 5 mm. As the native footprint of the ACL is considered to be 25% in the PA dimension, a tunnel located 30% or more anterior corresponds to a tunnel placed approximately 3 mm or more anterior to the native ACL footprint.
In the PD dimension, femoral tunnels were significantly more proximal (high) in those patients who underwent revision compared with those who did not (30% ± 9% vs 38% ± 9%, p < 0.01). Among those who underwent revision, there was no significant difference in PD dimension tunnel position between those who experienced non-traumatic chronic failure and those who experienced traumatic failure. Femoral tunnel PD position of 25% or less had an odds ratio for revision of 13 (95% CI 3–60, p < 0.01). The average height of the condyle in the PD dimension was 27 ± 3 mm. As the native footprint of the ACL is considered to be 29% in the PD dimension, a tunnel placed 25% or less corresponds to a tunnel that is placed approximately 1 mm higher than the native ACL footprint.
A multivariable logistic regression (Table 4) found that quadriceps tendon usage had an odds ratio for revision of 0.11 (95% CI 0.03–0.46, p < 0.05). The other graft choices, as well as age, gender, and BMI, were not predictive of revision status. A multivariable logistic regression also revealed that for each 1% decrease in PA dimension, there was a 0.84 decrease in odds of having a revision (Table 5). A decrease in the PA dimension correlates to less anterior, and therefore closer to anatomic, tunnel placement. For each 1% decrease in PD dimension, there was a 1.10 increase in odds of having a revision. A decrease in the PD dimension correlates to a more proximal (high), and therefore more vertically oriented graft, in the intercondylar notch. The two coordinates were found to significantly predict the revision status independently.
Discussion
This study demonstrated that having undergone revision ACL-R was associated with significantly more anterior and proximal (high) femoral tunnel placement during primary ACL-R (Fig. 2). Patients who experienced non-traumatic failure were found to have significantly more anterior femoral tunnel placement than those who experienced traumatic failure. Moreover, revision status was predicted by the tunnel placement in each dimension (PA and PD) independently. Based on the present data, surgeons less familiar with anatomic ACL-R technique might consider intra-operative use of fluoroscopy to guide femoral tunnel placement.

Comparing primary femoral tunnel position between patients with intact primary and revised ACL reconstructions. A lateral radiograph of the knee. The overlaid grid represents the quadrant method established by Bernard et al. with the PA dimension measured along Blumensaat’s line and the PD dimension at a line perpendicular to Blumensaat’s line. Green circles represent femoral tunnel placement of patients in the primary group (n = 58), with the outlined green diamond representing their average (28% of PA dimension, 38% of PD dimension). The red circles represent femoral tunnel placement of patients in the revision group (n = 59), with the outlined red diamond representing their average (38% of PA dimension, 30% of PD dimension)
The differences in tunnel position between the groups were significant. These data may therefore help surgeons understand how to reduce a patient’s odds of revision ACL-R. In addition to increased risk of repeat graft failure, increased risk of failed meniscal repair, and increased incidence of chondral lesions, patients who undergo revision generally have significantly worse outcomes [15, 16, 29, 30]. While some patients are able to return to sport, the return to sport is typically at a lower level than before the injury [10]. International Knee Documentation Committee (IKDC) objective scores also tend to be lower after revision ACL-R than after primary ACL-R [15].
ACL rupture in general is a risk factor for early development of OA, and ACL-R reduces but does not eliminate the risk [8, 23]. A systematic review of post-traumatic OA following ACL injury found that anatomic ACL-R was associated with less radiographic OA than non-anatomic ACL-R at long-term follow-up [23]. The data presented in this study may demonstrate that patients are at reduced odds of undergoing revision ACL-R when the femoral tunnels are placed less anteriorly and less proximally (high), which may also contribute to a decreased risk of post-traumatic OA.
Understanding why ACL reconstructions fail is a multifaceted issue, of which femoral tunnel position is but one variable. The MARS group broadly defined three modes of failure; traumatic, technical error, and biologic, with some failures overlapping between modes [13]. Of those failures with technical error, femoral tunnel malposition was reported in 80% of cases [16]. For an anatomic ACL-R, which has been described as the functional restoration of the ACL to its native dimensions, collagen orientation, and insertion sites, proper femoral tunnel position involves placement within the native ACL’s femoral insertion site [27]. Evaluation of the native femoral insertion site in routine post-operative plain films is possible, albeit complicated by individually variable bony morphology as well as the potential for radiographs to be captured off-axis [1]. The present study required lateral radiographs to have less than 6 mm of condylar offset, which may limit general clinical application of these results. The radiographic analysis suggests that femoral tunnels placed more than 30% of the PA dimension may have increased odds of failure from any modality. There was also, however, a significant difference in femoral tunnel position between those who experienced traumatic failure and those who experienced chronic non-traumatic failure. Patients who experienced non-traumatic failure had the most anterior tunnels centered at an average of 41% of the PA dimension. In comparison, patients who experienced traumatic failure had tunnels centered at average of 35% of the PA dimension (Fig. 3). These data suggest that there may potentially be a difference between anatomic tunnel placement, non-anatomic placement, and semi-anatomic placement. Patients with femoral tunnels placed less than 30% of the PA dimension were found to have the lowest odds of requiring revision and may be considered “anatomic”. Patients with femoral tunnels more than 37% of the PA dimension have increased odds of experiencing chronic instability and non-traumatic failure and may be deemed “non-anatomic.” Patients with femoral tunnels placed between 30 and 37% are less likely to experience chronic instability, while statistically speaking are at increased odds of experiencing traumatic failure with return to sport. Such tunnels may be defined as “semi-anatomic.” It should be noted that while these differences were found to be statistically significant, it may be difficult to translate these results into surgical decision making. Given the average length of the condyle in the PA dimension, the difference between the proposed semi- and non-anatomic positions is only approximately 3 mm.

Comparing primary femoral tunnel position between patients with intact primary ACL reconstruction, patients with traumatic failure, and patients with non-traumatic Failure. A lateral radiograph of the knee. The overlaid grid represents the quadrant method established by Bernard et al. with the PA dimension measured along Blumensaat’s line and the PD dimension at a line perpendicular to Blumensaat’s line. The outlined green diamond represents the average location of those patients with intact primary ACL-R (28% of PA dimension, 38% of PD dimension). The outlined orange diamond represents the average location of those patients who underwent revision ACL-R after traumatic failure (35% of PA dimension, 32% of PD dimension). The outlined red diamond represents the average location of those patients who underwent revision ACL-R after non-traumatic failure (41% of PA dimension, 28% PD dimension)
The results of the present study may reflect findings that has been shown in previous biomechanical studies in cadaveric knees. Knees with grafts placed anterior to the anatomic femoral footprint experienced more anterior tibial translation in response to both anterior tibial and combined rotatory loads than knees with anatomic reconstructions, particularly in lower levels of knee flexion [17]. Knees with grafts placed in a more proximal (high) femoral position experienced less rotational stability at lower levels of knee flexion than knees with less proximal femoral graft placement [21]. Clinically, these results have been demonstrated in a variety of studies [3, 7, 9]. Patients with residual pivot shift have also been found to have more proximal graft placement in addition to lower patient reported outcomes [9]. Moreover, a prospective randomized control trial of 281 patients demonstrated improved anteroposterior and rotational stability in anatomic reconstruction compared with conventional reconstruction at mid-term follow-up [3, 7].
Restoration of native knee kinematics, stability, and return to sport is a goal for many patients, and simple decision rules during ACL-R rehabilitation can significantly decrease rates of re-injury among these patients [4]. The data in this study also suggest that placement of the femoral tunnel less than 30% of the PA dimension may have some protective effect from traumatic re-injury. In the event of revision ACL-R, patients would not only be at risk for worse clinical outcomes and progression of knee OA, but also increased economic burden [10, 23]. Healthcare utilization costs for ACL-R have been steadily increasing, with total healthcare utilization costs for revision ACL-R costing more than primary ACL-R ($16,238 vs $15,000 USD, respectively) [6]. There is evidence to suggest that patients may be less likely to require revision when primary ACL-R is performed at high-volume institutions [11, 12]. Moreover, patients of high-volume surgeons may be less likely to require subsequent knee surgeries of any kind in the year after ACL-R [12]. Several studies have demonstrated similar improved outcomes with total hip and total knee arthroplasties from high-volume surgeons and hospitals [12, 22]. Given the significant functional and economic burdens associated with revision ACL-R, every effort should be made to achieve an anatomic reconstruction the first time.
There are several limitations to this study. The femoral tunnel position was the only technical aspect of the ACL-R considered in this study, and it was only evaluated on two-dimensional plain films. Other technical factors such as tibial tunnel position and meniscal procedures were not considered. While one dimension of the tibial tunnel position may be evaluated on lateral plain films, computed tomography would have been needed for a more accurate assessment of tibial tunnel position, which was not available in this study. The retrospective nature of this study may introduce confounding factors and biases that may be easier to minimize in a prospective study. Due to screening methods, only individuals who underwent revision ACL-R were included, which may have missed those who experienced graft failure but did not undergo revision surgery. Additionally, quadriceps tendon usage was significantly associated with not having undergone revision, indicating that the use of multiple graft types may have confounded the results. Moreover, allograft tissue was not used significantly more often in the revision group than in the primary group, despite the fact that allograft tissue has been shown to be associated with revision in the past [19]. The differences in graft usage between the primary and revision groups may be due to the fact that all primary patients came from the same surgeon, while the revised patients were pooled from multiple surgeons. Including multiple surgeons in the revision group allowed for a larger sample size, but introduced additional confounding variables. Variables such as reconstruction technique, surgeon experience and volume, and rehabilitation protocols have been shown to significantly impact the rates of ACL-R failure [4, 7, 11, 12]. Clinically, the results of the present study demonstrate that there may be a relationship between femoral tunnel position and mechanism of failure in patients who required revision ACL-R.
Conclusion
In this retrospective study of 58 patients with successful primary ACL-R, who were compared to 59 patients who had failed ACL-R, anterior and proximal (high) femoral tunnels for ACL-R were shown to be independent risk factors for ACL revision surgery. Moreover, patients who experienced non-traumatic failure had statistically significantly more anterior femoral tunnel placement than those who experienced traumatic failure. In other words, placement of an ACL graft into the anatomic footprint of the ACL may reduce the odds of revision ACL-R. As revision ACL-R is associated with patient- and economic burden, particular attention should be given to achieving an individualized, anatomic, and value-based primary ACL-R.
References
Bernard M, Hertel P, Hornung H, Cierpinski T (1997) Femoral insertion of the ACL radiographic quadrant method. Am J Knee Surg 10(1):14–21
Crowley R, Daniel H, Cooney TG, Engel LS, Health and Public Policy Committee of the American College of Physicians (2020) Envisioning a better U.S. Health care system for all: coverage and cost of care. Ann Intern Med 172:S7–S32
Eliya Y, Nawar K, Rothrauff BB, Lesniak BP, Musahl V, De Sa D (2020) Anatomical anterior cruciate ligament reconstruction (ACLR) results in fewer rates of atraumatic graft rupture, and higher rates of rotatory knee stability: a meta-analysis. JISAKOS 5(6):359–370
Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA (2016) Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med 50(13):804–808
HamrinSenorski E, Sundemo D, Murawski CD, Alentorn-Geli E, Musahl V, Fu F, Desai N, Stålman A, Samuelsson K (2017) No differences in subjective knee function between surgical techniques of anterior cruciate ligament reconstruction at 2-year follow-up: a cohort study from the Swedish national knee ligament register. Knee Surg Sports Traumatol 25(12):3945–3954
Herzog MM, Marshall SW, Lund JL, Pate V, Spang JT (2017) Cost of outpatient arthroscopic anterior cruciate ligament reconstruction among commercially insured patients in the united states, 2005–2013. Orthop J Sports Med. https://doi.org/10.1177/2325967116684776
Hussein M, van Eck CF, Cretnik A, Dinevski D, Fu FH (2012) Prospective randomized clinical evaluation of conventional single-bundle, anatomic single-bundle, and anatomic double-bundle anterior cruciate ligament reconstruction: 281 cases with 3- to 5-year follow-up. Am J Sports Med 40(3):512–520
Kvist J, Filbay S, Andersson C, Ardern CL, Gauffin H (2020) Radiographic and symptomatic knee osteoarthritis 32 to 37 years after acute anterior cruciate ligament rupture. Am J Sports Med 48(10):2387–2394
Lee MC, Seong SC, Lee S et al (2007) Vertical femoral tunnel placement results in rotational knee laxity after anterior cruciate ligament reconstruction. Arthroscopy 23(7):771–778
Lefevre N, Klouche S, Mirouse G, Herman S, Gerometta A, Bohu Y (2017) Return to sport after primary and revision anterior cruciate ligament reconstruction: a prospective comparative study of 552 patients from the FAST cohort. Am J Sports Med 45(1):34–41
Lind M, Strauss MJ, Nielsen T, Engebretsen L (2020) Low surgical routine increases revision rates after quadriceps tendon autograft for anterior cruciate ligament reconstruction: results from the danish knee ligament reconstruction registry. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06220-0
Lyman S, Koulouvaris P, Sherman S, Do H, Mandl LA, Marx RG (2009) Epidemiology of anterior cruciate ligament reconstruction: trends, readmissions, and subsequent knee surgery. J Bone Joint Surg Am 91(10):2321–2328
Wright RW, Huston LJ, MARS Group et al (2010) Descriptive epidemiology of the multicenter ACL revision study (MARS) cohort. Am J Sports Med. 38(10):1979–1986
Middleton KK, Muller B, Araujo PH et al (2015) Is the native ACL insertion site “completely restored” using an individualized approach to single-bundle ACL-R? Knee Surg Sports Traumatol Arthrosc 23(8):2145–2150
Mohan R, Webster KE, Johnson NR, Stuart MJ, Hewett TE, Krych AJ (2018) Clinical outcomes in revision anterior cruciate ligament reconstruction: a meta-analysis. Arthroscopy 34(1):289–300
Morgan JA, Dahm D, Levy B, Stuart MJ, MARS Study Group (2012) Femoral tunnel malposition in ACL revision reconstruction. J Knee Surg 25(5):361–368
Musahl V, Plakseychuk A, VanScyoc A et al (2005) Varying femoral tunnels between the anatomical footprint and isometric positions: effect on kinematics of the anterior cruciate ligament-reconstructed knee. Am J Sports Med 33(5):712–718
Pfeiffer TR, Burnham JM, Hughes JD et al (2018) An increased lateral femoral condyle ratio is a risk factor for anterior cruciate ligament injury. J Bone Joint Surg Am 100(10):857–864
Rahardja R, Zhu M, Love H, Clatworthy MG, Monk AP, Young SW (2020) Factors associated with revision following anterior cruciate ligament reconstruction: a systematic review of registry data. Knee 27(2):287–299
Rahardja R, Zhu M, Love H, Clatworthy MG, Monk AP, Young SW (2020) No difference in revision rates between anteromedial portal and transtibial drilling of the femoral graft tunnel in primary anterior cruciate ligament reconstruction: early results from the new zealand ACL registry. Knee Surg Sports Traumatol Arthrosc 28(11):3631–3638
Rayan F, Nanjayan SK, Quah C, Ramoutar D, Konan S, Haddad FS (2015) Review of evolution of tunnel position in anterior cruciate ligament reconstruction. World J Orthop 6(2):252–262
Ricciardi BF, Liu AY, Qiu B, Myers TG, Thirukumaran CP (2019) What is the association between hospital volume and complications after revision total joint arthroplasty: a large-database study. Clin Orthop Relat Res 477(5):1221–1231
Rothrauff BB, Jorge A, de Sa D, Kay J, Fu FH, Musahl V (2020) Anatomic ACL reconstruction reduces risk of post-traumatic osteoarthritis: a systematic review with minimum 10-year follow-up. Knee Surg Sports Traumatol Arthrosc 28(4):1072–1084
Sakamoto Y, Tsukada H, Sasaki S, Kimura Y, Yamamoto Y, Tsuda E, Ishibashi Y (2020) Effects of the tibial tunnel position on knee joint stability and meniscal contact pressure after double-bundle anterior cruciate ligament reconstruction. J Orthop Sci 25(6):1040–1046
Sonnery-Cottet B, Saithna A, Cavalier M et al (2017) Anterolateral ligament reconstruction is associated with significantly reduced ACL graft rupture rates at a minimum follow-up of 2 years: a prospective comparative study of 502 patients from the SANTI study group. Am J Sports Med 45(7):1547–1557
Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S (2008) Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci 13(2):122–129
van Eck CF, Gravare-Silbernagel K, Samuelsson K et al (2013) Evidence to support the interpretation and use of the anatomic anterior cruciate ligament reconstruction checklist. J Bone Joint Surg Am 95(20):e1531–e1539
Vap AR, Persson A, Fenstad AM, Moatshe G, LaPrade RF, Engebretsen L (2019) Re-revision anterior cruciate ligament reconstruction: an evaluation from the Norwegian knee ligament registry. Arthroscopy 35(6):1695–1701
Wright RW, Huston LJ, Haas AK, Nwosu SK, Allen CR, Anderson AF, MARS Group (2020) Meniscal repair in the setting of revision anterior cruciate ligament reconstruction: Results from the MARS cohort. Am J Sports Med. https://doi.org/10.1177/0363546520948850
Wyatt RWB, Inacio MCS, Liddle KD, Maletis GB (2014) Prevalence and incidence of cartilage injuries and meniscus tears in patients who underwent both primary and revision anterior cruciate ligament reconstructions. Am J Sports Med 42(8):1841–1846
Yamamoto Y, Hsu W-H, Woo SL-Y, Van Scyoc AH, Takakura Y, Debski RE (2004) Knee stability and graft function after anterior cruciate ligament reconstruction: a comparison of a lateral and an anatomical femoral tunnel placement. Am J Sports Med 32(8):1825–1832
Funding
No outside funding was used during this study.
Author information
Authors and Affiliations
Contributions
All listed authors have contributed substantially to this work: KB, JH, CG, and RV were involved with drafting and revising the manuscript, tables and figures, as well as data analysis. AP was involved with data analysis, statistics, and data interpretation. BL, JI, and VM were involved in the study design. BL, JK, JI, and VM were involved in the clinical analysis, editing, and revision of the manuscript, tables, and figures.
Corresponding author
Ethics declarations
Conflict of interest
VM reports educational grants, consulting fees, and speaking fees from Smith & Nephew plc, educational grants from Arthrex, is a board member of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS), and deputy editor-in-chief of Knee Surgery, Sports Traumatology, Arthroscopy (KSSTA). In addition, VM has a patent Quantifed injury diagnostics-US Patent No. 9,949,684, Issued on April 24, 2018, issued to University of Pittsburgh.
Ethical approval
Approved by the Institutional Review Board at University of Pittsburgh (STUDY1903019).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Byrne, K.J., Hughes, J.D., Gibbs, C. et al. Non-anatomic tunnel position increases the risk of revision anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 30, 1388–1395 (2022). https://doi.org/10.1007/s00167-021-06607-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06607-7