
Abstract
Purpose
The use of an accessory anteromedial portal to drill the femoral graft tunnel in primary anterior cruciate ligament (ACL) reconstruction was introduced in the 2000s in an effort to achieve a more anatomic femoral tunnel position. However, some early studies reported an increase in revision ACL reconstruction compared to the traditional transtibial technique. The aim of this study was to analyse recent data recorded by the New Zealand ACL Registry to compare outcomes of ACL reconstruction performed using the anteromedial portal and transtibial techniques.
Methods
Analysis was performed on primary isolated single-bundle ACL reconstructions recorded between 2014 and 2018 by the New Zealand ACL Registry. Patients were categorised into two groups according to whether an anteromedial portal or transtibial technique was used to drill the femoral graft tunnel. The primary outcome was revision ACL reconstruction and was compared between both groups through univariate and multivariate survival analyses. The secondary outcomes that were analysed included subscales of the Knee Injury and Osteoarthritis Outcome Score (KOOS) and Marx activity score.
Results
Six thousand one hundred and eighty-eight primary single-bundle ACL reconstructions were performed using either the anteromedial portal or transtibial drilling techniques. The mean time of follow-up was 23.3 (SD ± 14.0) months. Similar patient characteristics such as mean age (29 years, SD ± 11), sex (males = 58% versus 57%) and time to surgery (median 4 months, IQR 5) were observed between both groups. The rate of revision ACL reconstruction was 2.6% in the anteromedial portal group and 2.2% in the transtibial group (n.s.). The adjusted risk of revision ACL reconstruction was 1.07 (95% CI 0.62–1.84, n.s.). Patients in the anteromedial portal group reported improved scores for subscales of the KOOS and higher Marx activity scores at 1-year post-reconstruction.
Conclusion
There was no difference in the risk of revision ACL reconstruction between the two femoral tunnel drilling techniques at short-term follow-up. We observed minor differences in patient-reported outcomes at 1-year follow-up favouring the anteromedial portal technique, which may not be clinically relevant. Surgeons can achieve good clinical outcomes with either drilling technique.
Level of evidence
III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anterior cruciate ligament (ACL) reconstruction is a procedure that has undergone significant changes to surgical technique over many decades that have improved the success of treatment and prolonged the careers of athletes [1,2,3,4,5]. Since becoming an arthroscopic procedure, there has been interest in more “anatomical” reconstruction to restore the ACL to its native location and structure to enhance the stability of the knee [6,7,8,9,10,11,12,13,14]. In particular, attention has been focused on the technique for drilling the femoral graft tunnel. Surgeons traditionally used a “transtibial” technique, where the femoral tunnel is drilled via and in line with the tibial tunnel [15, 16]. Some authors argue the transtibial technique can lead to a “non-anatomical” ACL reconstruction, as it tends to place the graft in a more vertical orientation compared to the native ACL [17,18,19,20].
The native femoral footprint of the ACL is well described, situated posterior to the lateral intercondylar ridge [14, 21, 22]. A number of studies have demonstrated that the use of an accessory anteromedial portal may have a higher success rate of placing the femoral tunnel within this native footprint, as the surgeon has greater flexibility since femoral tunnel positioning is independent of the tibial tunnel [21, 23,24,25,26,27,28,29]. Furthermore, biomechanical studies associate “anatomically” reconstructing the ACL at the native femoral footprint with increased objective knee stability [30,31,32,33].
Despite an increase in the popularity of the anteromedial portal drilling technique, early studies associate its use with an increased risk of revision compared to the transtibial technique [34,35,36,37]. It was theorised that the increased risk was due to a learning curve faced by surgeons who transitioned from using the transtibial technique to the use of an accessory anteromedial portal to drill the tunnel [35]. This reason may be supported by Eysturoy et al. who found an increased risk of revision during the earlier use of the anteromedial portal technique, but found no difference in revision risk using more recent data when compared to the transtibial technique [38].
This study aimed to clarify the risk of revision ACL reconstruction between anteromedial portal and transtibial drilling of the femoral graft tunnel using data from the New Zealand ACL Registry. It is hypothesised that the effect of any learning curve will be minimised as the registry began capturing data in 2014, well after anteromedial portal drilling was introduced. Additionally, post-operative patient-reported outcome measures (PROMs) at 1 year will be compared between the two drilling techniques.
This study was performed to analyse whether there remains a higher rate of failure with the anteromedial portal technique and to provide feedback to surgeons who practise either drilling technique.
Materials and methods
Following exemption from the Health and Disability Ethics Committee (HDEC), a retrospective review was performed on prospectively captured data by the New Zealand ACL Registry. The operation of the registry has been declared as a protected quality assurance activity by the New Zealand Ministry of Health and all patients recorded in the registry have signed consent forms to participate.
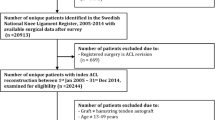
Between 2014 and 2018, 7612 primary ACL reconstructions have been recorded. This study reviewed all primary isolated single-bundle ACL reconstructions performed using either the anteromedial portal or transtibial techniques when drilling the femoral graft tunnel (n = 6353). We excluded patients who underwent multi-ligament reconstruction, contralateral ACL reconstruction or any concurrent surgery such as osteotomy or unicompartmental knee replacement (n = 165).
The New Zealand ACL Registry
The New Zealand ACL Registry is a nationwide registry that began in 2014 and prospectively captures data on patient, surgical and follow-up variables. Since 2017, it is mandatory for all orthopaedic surgeons who perform ACL reconstructions to actively participate in the registry to achieve recertification [39]. As of 2018, based on comparisons to government healthcare data, it is estimated that approximately 85% of all ACL reconstructions performed in New Zealand are captured by the registry [40]. Patient demographic data are collected through a pre-operative form, while an intra-operative data form detailing each reconstruction procedure is completed by the surgeon. In addition, surgeons can fill out a post-operative complication form that details any early and late complications relating to the procedure. Patient-reported complications are confirmed with the treating surgeon. Patient-reported outcome measures (PROMs) including the Knee Injury and Osteoarthritis Outcome Score (KOOS) and Marx questionnaires are captured pre-operatively and post-operatively at 6 months, 1, 2 and 5 years.
Outcome of interest and predictor variables
The main predictor variable was femoral graft tunnel drilling technique (anteromedial portal versus transtibial) as recorded by the surgeon using the intra-operative data form. The primary outcome was revision ACL reconstruction occurring during the study period.
The secondary outcomes were patient-reported outcome measures (PROMs) captured by the registry at 1 year after reconstruction. All five subscales of the KOOS including symptoms, pain, activities of daily living (ADL), sport and recreation (Sport/Rec) and quality of life (QoL), and Marx activity score were analysed. Subscales of the KOOS are scored independently on a scale of 0–100 with 0 representing “extreme knee problems” and 100 representing “no knee problems” [41]. The Marx questionnaire is designed to ask patients how often they performed four activities including running, cutting, deceleration and pivoting when they were in their most active state [42]. The maximum activity score is 16, indicating a patient who has performed all four activities more than four times a week.
Statistical analyses
Descriptive statistics were provided as mean values with standard deviation (SD) or median values with interquartile ranges (IQR). Univariate analysis of the rate of revision ACL reconstruction was performed using Chi-Square test. Kaplan–Meier survival analysis was performed to produce a survival plot with the associated number at risk and cumulative survival probabilities of revision. Incidence densities were calculated per 100 observed person-years. Hazard ratios (HR) with 95% confidence intervals (CI) were computed to compare the risk of revision between drilling techniques using a Cox proportional hazards regression model adjusting for patient and surgical covariates (age, sex, time from injury-to-surgery, graft choice, concomitant meniscal or cartilage injury, previous knee surgery, cause of injury and pre-operative Marx activity score). The assumption of proportional hazards was assessed via log(-log) plots and found suitable. KOOS and Marx scores were assessed for normality through visualization of Q–Q plots and histograms, before being analysed through Student’s t test or Mann–Whitney U test. Results were considered statistically significant at p < 0.05. All analyses were performed using IBM SPSS Statistics version 25.
Results
Six thousand one hundred and eighty-eight primary isolated single-bundle ACL reconstructions were performed using either the anteromedial portal or transtibial femoral tunnel drilling techniques between 2014 and 2018 (Table 1). The mean time of follow-up was 23.3 (SD ± 14.0) months. The anteromedial portal technique was used in 5285 reconstructions (85.4%), while the transtibial technique was used in 903 reconstructions (14.6%). The mean age of patients in this study was 28.9 years and 3597 patients were male (58%). The median time from injury-to-surgery was 4.2 months with the hamstring tendon as the most popular choice of graft (n = 4616, 74.6%), followed by the patellar tendon (n = 1414, 22.9%) and quadriceps tendon (n = 50, 0.8%). The majority of index ACL injuries were caused while playing a sport (n = 5147, 83.2%). Overall, 3728 patients had a concomitant meniscal injury (60%), while 2502 patients had a concomitant cartilage injury (40%). 232 patients had previous knee surgery prior to their primary ACL reconstruction (4%). Patient demographics were similar between the two drilling techniques, however, 38% of patients in the transtibial group had a patellar tendon autograft compared to 20% of patients in the anteromedial portal group.
Patients in the anteromedial portal group reported higher pre-operative Marx activity scores compared to patients in the transtibial group (mean scores 11.4 vs 11.2, p = 0.04) (Table 2). There was no difference in pre-operative KOOS scores between the two groups.
Revision in ACL reconstruction
There were 135 revisions in the anteromedial portal group (2.6%) compared with 20 in the transtibial group (2.2%, n.s.) (Table 3).
The number of revisions per 100 observed person-years was 1.3 (95% CI 1.1–1.6) in the anteromedial portal group, comparable to 1.1 (95% CI 0.7–1.8) in the transtibial group (Table 3).
The number at risk at 2 years in the anteromedial portal group was 2484 with a cumulative survival probability of 97.1% (95% CI 96.5–97.6) (Fig. 1). The number at risk at 2 years in the transtibial group was 474 with a cumulative survival probability of 97.9% (95% CI 96.4–98.8).

Cumulative survival probability of revision following primary ACL reconstruction
After adjusting for patient and surgical variables on multivariate analysis, there was no difference in the risk of revision between the anteromedial portal and transtibial drilling techniques (HR 1.07, 95% CI 0.62–1.84, n.s.).
In 3045 patients who had a minimum follow-up of 2 years, the revision rate was 4.3% in the anteromedial portal group and 3.7% in the transtibial group (adjusted HR 1.09, n.s.) (Table 5 in “Appendix”).
When analysing the registry’s post-operative complications data, there were 197 surgeon-reported graft failures in the anteromedial portal group (3.7%) and 32 in the transtibial group (3.5%, n.s.). On multivariate analysis, there was no difference in the risk of graft failure (adjusted HR 0.93, 95% CI 0.62–1.40, n.s.).
Patient-reported outcome measures
At 1-year post-reconstruction, the mean response rate was 45.9% for both the KOOS and Marx activity questionnaire (Table 4).
Patients in the anteromedial portal group reported higher scores for the pain, ADL, Sport/Rec, QoL and Marx scores. No difference was reported for the symptoms score.
Discussion
The most important finding of this study was that there was no difference in the rate and risk of revision between the anteromedial portal and transtibial femoral graft tunnel drilling techniques. However, patients in the anteromedial portal group reported higher scores for subscales of the KOOS and Marx activity score at 1-year post-reconstruction.
The use of an accessory anteromedial portal has increased when drilling the femoral graft tunnel in primary ACL reconstruction, as it provides the surgeon with greater flexibility when deciding where to place the femoral graft tunnel [43, 44]. Despite this potential advantage, Tejwani et al. from the Kaiser Permanente ACL Registry found a 1.3 times higher risk of revision when using the anteromedial portal technique [37]. Similarly, Desai et al. from the Swedish National Knee Ligament Register reported a 1.4 times higher risk of revision and theorised that a learning curve associated with the anteromedial portal technique may explain this observation [34]. Although the anteromedial portal allows surgeons to “anatomically” reconstruct the ACL, it does not always result in accurate graft tunnel placement at the native footprint [45]. Variation in tunnel positioning targets especially during the early use of this technique may have contributed to a tunnel placed too anteriorly, reduced tunnel length and other technical difficulties that may have increased the rate of failure, but could have been prevented with experience and refinement [20, 27, 45,46,47]. Clatworthy et al. and Williams et al. found a higher rate of failure when first switching to an anteromedial portal technique, but noted they concurrently altered tunnel positioning to the “central” femoral footprint, in contrast to the “anteromedial bundle” position they used with the transtibial technique [48, 49]. They reported their failure rate reduced when they changed the femoral tunnel position back to the “anteromedial bundle” position while still using an anteromedial portal technique.
In contrast to the referenced registry studies, the New Zealand ACL Registry began capturing data in April 2014, providing surgeons with adequate time to adjust to a different technique and allowing for a fairer comparison between techniques. The lack of association between revision and drilling technique in this study may support the existence of a previous learning curve that has now been overcome by surgeons. Results from the Danish Knee Ligament Reconstruction Register may also support this theory. Rahr-Wagner et al. found a 2.04 times higher revision risk with the anteromedial portal technique compared to the transtibial technique during the period January 2007 to December 2010 [35], whereas Eysturoy et al. found no difference in revision risk between the two techniques (HR 0.99, p = 0.96) during the later time period of January 2012 to December 2015 [38].
This study found that patients in the anteromedial portal group reported improved pain, ADL, Sport/Rec, QoL and Marx activity scores at 1-year post-reconstruction when compared to patients in the transtibial group. Despite the association with improved KOOS, the difference in mean scores was small, ranging from as low as a 1.6-point difference to as high as a 5-point difference when compared to the transtibial technique. Furthermore, the mean pre-operative activity levels were higher in the anteromedial portal group and may explain the similar observation at 1-year post-reconstruction. This suggests that the difference in post-operative scores is unlikely to be clinically significant.
The strengths of this study include the analysis of data recorded in a more recent time period to previous studies that have analysed data recorded during the early use of the anteromedial portal technique. Furthermore, the availability of a large patient population allows for greater certainty when attempting to identify any meaningful statistical associations. However, this study is not without limitations. Although the New Zealand ACL Registry captures the drilling technique used by the surgeon, it does not evaluate tunnel positioning or “anatomical reconstruction” using a tool such as the Anatomic Anterior Cruciate Ligament Reconstruction Scoring Checklist (AARSC) [50]. As a result, this study is a comparison between the anteromedial portal and transtibial drilling techniques, rather than the effectiveness of anatomically reconstructing the ACL. While it provides reassurance that good clinical outcomes can be obtained with both drilling methods, further work incorporating such data would be needed to identify whether the accuracy of tunnel placement between techniques influences the outcome of treatment. In addition, revision ACL reconstruction may underestimate the true rate of repeat ACL injury as not all patients who suffer a graft rupture may proceed to undergo a revision. Despite this, revision is a robust and well-defined outcome that is easily captured by a national registry. Furthermore, there is no reason to suggest patients would be less likely to undergo revision depending on the drilling techniques used. In this study, the average response rate for PROMs was approximately 46% at 1-year post-reconstruction. This is comparable to the Danish Knee Ligament Reconstruction Register which reported a 31% response rate at 1-year post-reconstruction [35]. The low post-operative response rate could potentially introduce bias into the analysis. However, as the operative data are prospectively collected, the response rate at 1 year is not expected to be greatly influenced by the drilling technique. The New Zealand ACL Registry is actively in contact with patients to achieve a more complete capture of PROMs. It is expected that these response rates will improve with time and maturation of the registry, allowing for a more in-depth analysis in the future. To mitigate against the variable follow-up durations of each patient, the Cox regression model was utilised and an analysis on only patients with a minimum follow-up of 2 years was performed, which demonstrated consistent results (“Appendix”).
The clinical relevance of this study is that surgeons can achieve good clinical outcomes with either drilling technique.
Conclusion
At a mean follow-up of 23 months, no difference in the risk of revision ACL reconstruction was observed between the anteromedial portal and transtibial techniques when drilling the femoral graft tunnel. Minor differences in patient-reported outcomes were observed. Good clinical outcomes can be achieved with the use of either drilling technique.
References
Davarinos N, O’Neill BJ, Curtin W (2014) A brief history of anterior cruciate ligament reconstruction. Adv Orthop Surg 2014:1–6
Ellman MB, Sherman SL, Forsythe B, LaPrade RF, Cole BJ, Bach BR Jr (2015) Return to play following anterior cruciate ligament reconstruction. J Am Acad Orthop Surg 23(5):283–296
Fu FH, Bennett CH, Lattermann C, Ma CB (1999) Current concepts current trends in anterior cruciate ligament reconstruction part 1: biology and biomechanics of reconstruction. Am J Sports Med 27(6):821–830
McCulloch PC, Lattermann C, Boland AL, Bach BR (2007) An illustrated history of anterior cruciate ligament surgery. J Knee Surg 20(2):95–104
Morris RC, Hulstyn MJ, Fleming BC, Owens BD, Fadale PD (2016) Return to play following anterior cruciate ligament reconstruction. Clin Sports Med 35(4):655–668
Aga C, Kartus JT, Lind M, Lygre SHL, Granan LP, Engebretsen L (2017) Risk of revision was not reduced by a double-bundle ACL reconstruction technique: results from the Scandinavian Registers. Clin Orthop Relat Res 475(10):2503–2512
Andernord D, Björnsson H, Petzold M, Eriksson BI, Forssblad M, Karlsson J et al (2014) Surgical predictors of early revision surgery after anterior cruciate ligament reconstruction: results from the Swedish National Knee Ligament Register on 13,102 patients. Am J Sports Med 42(7):1574–1582
Björnsson H, Andernord D, Desai N, Norrby O, Forssblad M, Petzold M et al (2015) No Difference in revision rates between single- and double-bundle anterior cruciate ligament reconstruction: a comparative study of 16,791 patients from the Swedish national knee ligament register. Arthroscopy 31(4):659–664
Middleton KK, Hamilton T, Irrgang JJ, Karlsson J, Harner CD, Fu FH (2014) Anatomic anterior cruciate ligament (ACL) reconstruction: a global perspective. Part 1. Knee Surg Sports Traumatol Arthrosc 22(7):1467–1482
Murawski CD, Wolf MR, Araki D, Muller B, Tashman S, Fu FH (2013) Anatomic anterior cruciate ligament reconstruction: current concepts and future perspective. Cartilage 4(3):27–37
Shino K, Suzuki T, Iwahashi T, Mae T, Nakamura N, Nakata K et al (2010) The resident’s ridge as an arthroscopic landmark for anatomical femoral tunnel drilling in ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 18(9):1164–1168
Steckel H, Starman JS, Baums MH, Klinger HM, Schultz W, Fu FH (2007) Anatomy of the anterior cruciate ligament double bundle structure: a macroscopic evaluation. Scand J Med Sci Sport 17(4):387–392
Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL-Y (2002) Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med 30(5):660–666
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH (2006) Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc 14(10):982–992
Arnold MP, Kooloos J, Van Kampen A (2001) Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc 9(4):194–199
Heming JF, Rand J, Steiner ME (2007) Anatomical limitations of transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med 35(10):1708–1715
Kaseta MK, DeFrate LE, Charnock BL, Sullivan RT, Garrett WE (2008) Reconstruction technique affects femoral tunnel placement in ACL reconstruction. Clin Orthop Relat Res 466(6):1467–1474
Lee DH, Kim HJ, Ahn HS, Il BS (2016) Comparison of femur tunnel aperture location in patients undergoing transtibial and anatomical single-bundle anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 24(12):3713–3721
Marchant BG, Noyes FR, Barber-Westin SD, Fleckenstein C (2010) Prevalence of nonanatomical graft placement in a series of failed anterior cruciate ligament reconstructions. Am J Sports Med 38(10):1987–1996
Mulcahey MK, David TS, Epstein DM, Alaia MJ, Montgomery KD (2014) Transtibial versus anteromedial portal anterior cruciate ligament reconstruction using soft-tissue graft and expandable fixation. Arthroscopy 30(11):1461–1467
Burnham JM, Malempati CS, Carpiaux A, Ireland ML, Johnson DL (2017) Anatomic femoral and tibial tunnel placement during anterior cruciate ligament reconstruction: anteromedial portal all-inside and outside-in techniques. Arthrosc Tech 6(2):e275–e282
Farrow LD, Chen MR, Cooperman DR, Victoroff BN, Goodfellow DB (2007) Morphology of the femoral intercondylar notch. J Bone Jt Surg 89-A 89(10):2150–2155
Abebe ES, Moorman CT, Dziedzic TS, Spritzer CE, Cothran RL, Taylor DC et al (2009) Femoral tunnel placement during anterior cruciate ligament reconstruction: an in vivo imaging analysis comparing transtibial and 2-incision tibial tunnel-independent techniques. Am J Sports Med 37(10):1904–1911
Dargel J, Schmidt-Wiethoff R, Fischer S, Mader K, Koebke J, Schneider T (2009) Femoral bone tunnel placement using the transtibial tunnel or the anteromedial portal in ACL reconstruction: a radiographic evaluation. Knee Surg Sports Traumatol Arthrosc 17(3):220–227
Gavriilidis I, Motsis EK, Pakos EE, Georgoulis AD, Mitsionis G, Xenakis TA (2008) Transtibial versus anteromedial portal of the femoral tunnel in ACL reconstruction: a cadaveric study. Knee 15(5):364–367
Kopf S, Forsythe B, Wong AK, Tashman S, Irrgang JJ, Fu FH (2012) Transtibial ACL reconstruction technique fails to position drill tunnels anatomically in vivo 3D CT study. Knee Surg Sports Traumatol Arthrosc 20(11):2200–2207
Kopf S, Pombo MW, Shen W, Irrgang JJ, Fu FH (2011) The ability of 3 different approaches to restore the anatomic anteromedial bundle femoral insertion site during anatomic anterior cruciate ligament reconstruction. Arthroscopy 27(2):200–206
Lee KW, Hwang YS, Chi YJ, Yang DS, Kim HY, Choy WS (2014) Anatomic single bundle anterior cruciate ligament reconstruction by low accessory anteromedial portal technique: an in vivo 3D CT study. Knee Surg Relat Res 26(2):97–105
Tompkins M, Milewski MD, Brockmeier SF, Gaskin CM, Hart JM, Miller MD (2012) Anatomic femoral tunnel drilling in anterior cruciate ligament reconstruction. Am J Sports Med 40(6):1313–1321
Alentorn-Geli E, Samitier G, Álvarez P, Steinbacher G, Cugat R (2010) Anteromedial portal versus transtibial drilling techniques in ACL reconstruction: a blinded cross-sectional study at two- to five-year follow-up. Int Orthop 34(5):747–754
Bedi A, Musahl V, Steuber V, Kendoff D, Choi D, Allen AA et al (2011) Transtibial versus anteromedial portal reaming in anterior cruciate ligament reconstruction: an anatomic and biomechanical evaluation of surgical technique. Arthroscopy 27(3):380–390
Chen H, Tie K, Qi Y, Li B, Chen B, Chen L (2017) Anteromedial versus transtibial technique in single-bundle autologous hamstring ACL reconstruction: a meta-analysis of prospective randomized controlled trials. J Orthop Surg Res 12(1):167
Steiner ME, Battaglia TC, Heming JF, Rand JD, Festa A, Baria M (2009) Independent drilling outperforms conventional transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med 37(10):1912–1919
Desai N, Andernord D, Sundemo D, Alentorn-Geli E, Musahl V, Fu F et al (2017) Revision surgery in anterior cruciate ligament reconstruction: a cohort study of 17,682 patients from the Swedish National Knee Ligament Register. Knee Surg Sports Traumatol Arthrosc 25(5):1542–1554
Rahr-Wagner L, Thillemann TM, Pedersen AB, Lind MC (2013) Increased risk of revision after anteromedial compared with transtibial drilling of the femoral tunnel during primary anterior cruciate ligament reconstruction: results from the danish knee ligament reconstruction register. Arthroscopy 29(1):98–104
Svantesson E, Sundemo D, Hamrin Senorski E, Alentorn-Geli E, Musahl V, Fu FH et al (2017) Double-bundle anterior cruciate ligament reconstruction is superior to single-bundle reconstruction in terms of revision frequency: a study of 22,460 patients from the Swedish National Knee Ligament Register. Knee Surg Sports Traumatol Arthrosc 25(12):3884–3891
Tejwani SG, Prentice HA, Wyatt RWB, Maletis GB (2018) Femoral tunnel drilling method: risk of reoperation and revision after anterior cruciate ligament reconstruction. Am J Sports Med 46(14):3378–3384
Eysturoy NH, Nielsen TG, Lind MC (2019) Anteromedial portal drilling yielded better survivorship of anterior cruciate ligament reconstructions when comparing recent versus early surgeries with this technique. Arthroscopy 35(1):182–189
New Zealand ACL Registry Annual Report 2017
New Zealand ACL Registry Annual Report 2018
Roos EM, Lohmander LS (2003) The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis The Knee injury and Osteoarthritis Outcome Score (KOOS). Health Qual Life Outcomes 1:64
Marx RG, Stump TJ, Jones EC, Wickiewicz TL, Warren RF (2001) Development and evaluation of an activity rating scale for disorders of the knee. Am J Sports Med 29(2):213–218
Harner CD, Honkamp NJ, Ranawat AS (2008) Anteromedial portal technique for creating the anterior cruciate ligament femoral tunnel. Arthroscopy 24(1):113–115
Tibor L, Chan PH, Funahashi TT, Wyatt R, Maletis GB, Inacio MCS (2016) Surgical technique trends in primary ACL reconstruction from 2007 to 2014. J Bone Jt Surg 98(13):1079–1089
Jaecker V, Zapf T, Naendrup JH, Pfeiffer T, Kanakamedala AC, Wafaisade A et al (2017) High non-anatomic tunnel position rates in ACL reconstruction failure using both transtibial and anteromedial tunnel drilling techniques. Arch Orthop Trauma Surg 137(9):1293–1299
Basdekis G, Abisafi C, Christel P (2008) Influence of knee flexion angle on femoral tunnel characteristics when drilled through the anteromedial portal during anterior cruciate ligament reconstruction. Arthroscopy 24(4):459–464
Robin BN, Jani SS, Marvil SC, Reid JB, Schillhammer CK, Lubowitz JH (2015) Advantages and disadvantages of transtibial, anteromedial portal, and outside-in femoral tunnel drilling in single-bundle anterior cruciate ligament reconstruction: a systematic review. Arthroscopy 31(7):1412–1417
Clatworthy M, Sauer S, Roberts T (2019) Transportal central femoral tunnel placement has a significantly higher revision rate than transtibial AM femoral tunnel placement in hamstring ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 27(1):124–129
Śmigielski R, Zdanowicz U, Drwięga M, Ciszek B, Williams A (2015) The anatomy of the anterior cruciate ligament and its relevance to the technique of reconstruction. Bone Jt J 98-B(8):1020–1026
Van Eck CF, Gravare-Silbernagel K, Samuelsson K, Musahl V, Van Dijk CN, Karlsson J et al (2013) Evidence to support the interpretation and use of the anatomic anterior cruciate ligament reconstruction checklist. J Bone Jt Surg 95-A 95(20):e153
Acknowledgements
The authors would like to acknowledge Charlotte Smith from the New Zealand ACL Registry for her ongoing support and assistance with data administration. RR would to like to acknowledge the Maurice and Phyllis Paykel Trust for providing student support.
Funding
No funding for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
We, the authors, declare that we have no conflicts of interest with relation to this study. MGC reports that he does consulting for Johnson & Johnson, receives fellowship funding from Johnson & Johnson and Arthrex, and receives royalties from Arthrex, none of which are related to this study.
Ethical approval
Health and Disability Ethics Committee exemption as an audit activity.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
See Table 5
.
Rights and permissions
About this article

Cite this article
Rahardja, R., Zhu, M., Love, H. et al. No difference in revision rates between anteromedial portal and transtibial drilling of the femoral graft tunnel in primary anterior cruciate ligament reconstruction: early results from the New Zealand ACL Registry. Knee Surg Sports Traumatol Arthrosc 28, 3631–3638 (2020). https://doi.org/10.1007/s00167-020-05959-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-020-05959-w