
Abstract
Purpose
Total Knee Arthroplasty (TKA) procedures incorporate technology in an attempt to improve outcomes. The Active Robot (ARo) performs a TKA with automated resections of the tibia and femur in efforts to optimize bone cuts. Evaluating the Learning Curve (LC) is essential with a novel tool. The purpose of this study was to assess the associated LC of ARo for TKA.
Methods
A multi-center prospective FDA cohort study was conducted from 2017 to 2018 including 115 patients that underwent ARo. Surgical time of the ARo was defined as Operative time (OT), segmented as surgeon-dependent time (patient preparation and registration) and surgeon-independent time (autonomous bone resection by the ARo). An average LC for all surgeons was computed. Complication rates and patient-reported outcome (PRO) scores were recorded and examined to evaluate for any LC trends in these patient related factors.
Results
The OT for the cases 10–12 were significantly quicker than the OT time of cases 1–3 (p < 0.028), at 36.5 ± 7.4 down from 49.1 ± 17 min. CUSUM and confidence interval analysis of the surgeon-dependent time showed different LCs for each surgeon, ranging from 12 to 19 cases. There was no difference in device related complications or PRO scores over the study timeframe.
Conclusion
Active Robotic total knee arthroplasty is associated with a short learning curve of 10–20 cases. The learning curve was associated with the surgical time dedicated to the robotic specific portion of the case. There was no learning curve-associated device-related complications, three-dimensional component position, or patient-reported outcome scores.
Level of evidence
Level II.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Primary TKA is a cost-effective treatment for patients with symptomatic end-stage knee osteoarthritis (OA). Robotics for TKA streamline the procedure, reduce instrumentation, and enhance bone cuts and component alignment—ultimately striving to improve clinical results and implant durability [19, 22]. Ingress of robotic technology in the operating room challenges surgeons to adopt new technology into their customized surgical techniques, learn system controls, adjust to automated processes, and methodically plan surgical treatment. The juncture of implementing novel devices raises concerns for operative time, surgical complications, and associated patient-related outcome (PRO) scores [12, 15].
Current robotic technology allows for variations in methodologies of execution resulting in three unique platforms: passive, semi-active, and active [12]. Jacofsky et al. discussed the limitations of robotic systems: they require a significant amount of education for surgeons to optimize safety and usefulness [12]. Learning curve (LC) studies on new technology revealed a range of 10–20 cases to achieve proficiency. The robotic-arm assisted technology, MAKO, revealed a learning curve of seven cases [14, 15, 17]. However, literature is scarce regarding the integration of active robotic systems for the modern surgeon. It is necessary to discuss the pioneer of active robotic surgical systems, the TSolution One Total Knee Application (THINK Surgical Inc., Fremont, CA). Designed as computed tomography (CT) based open-implant platform capable of performing automated femoral and tibial resections with its Active Robotic TKA (ARo) component under surgeon supervision [12, 18]. Early results of the technology revealed radiological outcomes to have a statistically significant reduction of malalignment compared to conventional instruments, 43–32%, respectively [23]. Encouraging results regarding safety and effectiveness require discussion of the associated LC. The purpose of the study was to assess operative times, evaluation of complication rates, and effects on PRO scores. No specific hypothesis is necessary to assess the LC of ARo.
Methods
Institutional review board (IRB) approval was obtained to conduct a multi-center, prospective, non-randomized US investigational device exemption clinical trial to evaluate the safety and effectiveness of robotic-assisted TKA using the TSolution One Total Knee Application (THINK Surgical).
This prospective FDA cohort study included 115 patients with symptomatic osteoarthritis undergoing primary TKA between 2017 and 2018. Appropriate sample size determination was done for safety and effectiveness outcomes, it was determined to be unnecessary for assessment of the LC. All patients who underwent ARo within the context of learning curve assessments had their TKA performed by four different fellowship-trained adult reconstruction surgeons (YDK, BNS, SK, WJL). All four surgeons had at least 10 years of experience in adult reconstructive surgery. A total of nine patients had their ARo performed by four other surgeons—but given the limited amount of cases performed by each surgeon, these cases were not included in this study. Inclusion criteria included the following: patients above 21 years of age, radiographic osteoarthritis diagnosed as Kellgren–Lawrence Grade of 3 or higher. Exclusion criteria included the following: previous open knee surgery in the operative knee, BMI > 40 kg/m2, candidate for bilateral TKA, active or prior history of joint infection, presence of hardware in the ipsilateral lower extremity. To provide adequate stability for femoral and tibial fixation, there was an exclusion criteria for patients with osteoporosis, and no patients enrolled in the study met this exclusion criteria. There was no upper age limit.
The open-implant platform of the device was able to accommodate three different implants in the study. Sixty-nine patients were implanted with Zimmer-Biomet Persona PS (69), while Forty-six patients were implanted with Corin Unity CR (43) or PS (3) implants. The patella was resurfaced in all patients.
ARo surgical times were collected at different stages of the surgery when the autonomous robot was present in the surgical field. The ARo operative time (OT) was defined as the time from patient preparation to the end of bone resection, further segemented to a surgeon-dependent time (i.e. from patient positioning, fixation of device, installation of pins, registration with probes) and a surgeon-independent time (i.e. automated bone resection performed by the ARo).
To determine the LC of the ARo, OT data from all surgeons were combined sequentially in groups of three surgeries. Student’s t-test was used to assess if there was statistically significant difference between the first three surgeries and the following groups of three surgeries. Statistical significance was set at p ≤ 0.05 for all statistical tests. Next, the LC for each individual surgeon was computed for the surgeon-dependent time. Since a variety of analysis have been used in literature to determine the LC for robotic systems in orthopedics, two alternative analyses were used to compute the LC for individual surgeons. First, cumulative summation (CUSUM) sequential analysis was used to assess the initial and proficiency phases of the LC for each individual surgeon. CUSUM plots were calculated as a running total of the difference between the case time at each point and the overall average case time for each surgeon. Second, the LC was determined as the number of surgeries required to have two consecutive surgeries completed within 95% confidence interval of the steady-state surgical time. The steady-state surgical time was computed as the average time of the last five cases of each surgeon.
Complications were recorded and evaluated as related to the active robot and/or the general TKA procedure. Preoperative, 6-week, 3-month, 6-month and 1-year, patient-reported outcome (PRO) scores available for the study included the following: Knee Society Score (KSS) Functional Score, Objective Score, Patient Expectations and Satisfaction Score and Short-Form 12 (SF-12) Mental and Physical Composite Scores. Statistical analyses were performed using nqueryAdvisor 7.0 (Los Angeles, CA).
Results
115 patients were enrolled in the study with a mean age of 65.9 years (± 8.3). Demographics of patients can be found in Table 1. Complete surgical data along with baseline KSS and SF-12 scores were only available for 107/115 (93%)—and thus results from our analysis only included this cohort of 107 patients.
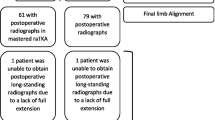
Figure 1 reveals the mean OT for entire cohort was 37.9 ± 11.3 min. Results from our analysis demonstrated a statistically significant decrease in OT from first three cases to cases 10–12 (49.1 ± 17 min vs 36.5 ± 7.4 min; p < 0.028). Figure 2 demonstrates the surgeon-dependent time to have a statistically significant (p < 0.014) decrease of 10 min between cases 1–3 and cases 13–15. Automated robotic cutting time did not demonstrate any associated LC throughout the study. Complete surgical data, including skin-to-skin surgical time, can be found in Table 2. No learning curve was observed regarding coronal alignment in patients. Cases 1–3 and 16–18 had a mean and standard deviation error of 0.3 ± 2.2° and 0.3 ± 2.7°, respectively (p = 0.999). Malalignment was defined as ± 3° difference in varus-valgus from the planned HKA. Radiological outcomes revealed a 43% reduction of malalignment compared to the 32% malalignment rate for conventional instruments.

Operative time over course of study

Surgeon-dependent time over course of study
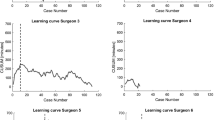
CUSUM analysis for the surgeon-dependent surgical time showed a different LC for each surgeon (Fig. 3). Phase 1 is the initial learning phase, then progressing to Phase 2 as the proficiency phase. Specifically, Surgeon 1 is noted to have no clear LC. A t-test did not find any significant difference between cases. CUSUM for Surgeon 2 and 3 revealed an initial learning phase of 12 cases (p = 0.035) and 16 cases (p < 0.001). Surgeon 4 revealed an initial learning phase of 19 cases. (p = 0.0081). Analysis based on confidence intervals for surgeon-dependent surgical time confirmed the findings from the CUSUM analysis, with LC of 12, 16, and 19 cases, respectively, for Surgeon 2, Surgeon 3, and Surgeon 4, with no discernable LC for Surgeon 1.


a–d CUSUM plots for each of the four surgeons. The orange dotted line indicates the end of the learning phase (i.e. phase 1) and the start of the proficiency phase (i.e. phase 2). a Surgeon 1. b Surgeon 2. c Surgeon 3. d Surgeon 4
Complete analysis of PRO scores at all time-points can be found in Fig. 4. Analysis of PRO scores demonstrated significant improvements from preoperative values. The 12-month follow-up KSS scores for Functional, Objective, Patient Expectations and Satisfaction revealed a significant difference (p < 0.001) from their respective preoperative scores. SF-12 Physical Composite scores also revealed a significant difference between the preoperative and 12-month follow-up (p < 0.0001). The PRO scores for each surgeon during and after their individual LC revealed no significant difference—indicating that patient outcomes were not affected by surgeon learning curve. For surgeons 2, 3. and 4, unpaired t-tests were performed comparing within LC and post-LC PROM deltas (postoperative score minus preoperative score) at each follow-up period. Surgeon 1 was excluded because they did not have a discernible LC. Table 3 shows the t-test p values, as well as the mean and confidence interval values. All t-test p values were above 0.05, indicating that there were no significant difference between PROMs within and post-LC. Some patients did not have PRO values, due to lost to follow-up or patient did not reconsent.

Patient Reported Outcome (PRO) scores over period of study
Analysis of complications demonstrated only one definitive device-related complication (metallic tack left within the distal femur) that occurred in a single patient. Otherwise, no traditional TKA device-related complications such as medial or lateral collateral ligament injuries, extensor mechanism disruptions, neurologic or vascular deficits, periprosthetic fractures, patellofemoral or tibiofemoral dislocations occurred. Additionally, no patients underwent revision surgery. Similar to PRO score analysis, we also found that there was no statistically significant association between complication rate and individual surgeon LC: despite surgeons adapting to technology during their initial cases, no significant increase in adverse events was sustained by patients. A complete list of TKA-related complications can be found in Table 4. with the most common being excessive/unexpected postoperative swelling and pain.
Of the 115 patients enrolled into the study, eight patients were switched to conventional instrumentation: three prior to any cutting, three after the femur had been cut but prior to any tibia cuts, and two after the femur had been cut and the tibia was partially cut. Patients were switched to conventional instrumentation by surgeon’s discretion, as well did not sustain injury during the shift.
Discussion
The most important finding from our FDA case series demonstrate ease of implementation of ARo technology amongst surgeons and excellent safety profile with only one definitive device-related complication. The patient with the metallic tack retained in distal femur was immediately made aware and elected not to return to operating room due to being asymptomatic and otherwise satisfied with their Aro TKA. The first important finding of this study is that OT of ARo significantly decreases after ten cases and that this LC was including the surgeon-dependent and surgeon-independent portions of the case involving exposure, pin placement, robot fixation and bone registration, and bone cutting. A second important finding is that the CUSUM analysis for the surgeon-dependent surgical time showed variable results with LC for each surgeon ranging from 12 to 20 cases. A final important finding is that there was no LC associated with PRO scores or device-related complications, thus highlighting an excellent safety profile that can be applied almost immediately to patients.
The importance of determining a learning curve for a particular surgery, implant, or technique is of paramount importance [10]. Learning curves indicate ease of adoptability of a new technology or surgery and suggest the number of repetitions it may require for a surgeon to become facile with that particular aspect of a procedure. Additionally, and perhaps more importantly, they can provide a quantitative and qualitative analysis of complications that may be incurred upon patients during the learning period [7, 9]. Surgeons can use the data provided from learning curve studies and perform their own risks vs benefit analysis to determine whether implementation of a particular method/technology is appropriate in their practice.
As surgical technology available to surgeons continues to be developed and marketed, orthopaedic surgeons have trended towards increased rates of adoption [5]. Analysis of data suggested a nearly threefold increase in implementation of technology in TKA between 2008 and 2015 (4.3–11.6%; p < 0.001) [2]. Proponents of computer-assisted TKA cite the ability to “provide real time intraoperative information on limb alignment and exact flexion/extension gap measurements.”[21] Other authors have reported that robotic-assisted TKA results in greater patient satisfaction and higher KSS scores at 6 weeks and 1 year postoperatively [21]. Similar to these prior literature reports, results from our series also demonstrated that PRO scores significantly improved postoperatively as compared to preoperative scores. Mean improvement of KSS score for our cohort was 42.8 at 1 year, with final KSS score of 82.7, similar to previously published values for robotic-assisted TKA cohorts (KSS 85 at 1 year) [21]. Our 1-year improvements in SF-12 Mental and Physical composite scores of 57.8 and 48.6, respectively, are in line with previously published data on robotic-assisted TKA reported long-term SF-12 Mental and Physical composite scores of 56.5 and 47.5, respectively [13]. In addition to demonstrating this improvement during sequential patient follow-ups, an important finding in our data was that LC was not associated with differences in PRO scores or device-related complications as the trial progressed, suggesting that although surgeons may have taken longer to complete initial cases during their LC, this did not negatively affect patients. These data may allow surgeons to feel confident that their individual LCs will not have an adverse effect on their patients, and these data can be used during pre-operative counseling to reassure patients of the safety profile of ARo. This LC is also distinctly different from the adoption of other techniques in joint replacements such as the anterior approach to total hip arthroplasty, where patients should be counselled on complications during the surgeon’s LC such as intraoperative fractures, dislocations, and lateral femoral cutaneous nerve palsies [1, 6, 11]. To our knowledge, there is a paucity of data on robotic TKA systems such as ARo which perform autonomous cuts, and at present the literature is limited to series describing surgeon-directed cuts within a robotic assisted platform [15, 16].
Results from our data demonstrate a short learning curve of less than 20 cases with only the robot-specific (surgeon-dependent) aspects of TKA, but not with the remainder of the procedure. We believe that the learning curve likely depends on each surgeon’s previous experience and expertise level in general related to navigation/robotics in surgery. Indeed – results from our analysis demonstrate that Surgeon One did not demonstrate a clear LC—and it is worth noting that this surgeon reported prior use of robot for THA and also utilization of navigation-assisted TKA for 15 years prior to this study. Besides the experience of the surgeon with computer-assisted technology, another possible explanation for the absence of a learning curve for surgeon 1 is that the level of training on the study and on the technology improved from the first initiated site to the following sites, as reasonably expected with an emerging technology. Indeed, the surgeon with no clear learning curve was the first site started in the study. Increased popularity and greater surgeon training with ARo will likely result in an even shorter LC and further advancement of current technology. Furthermore—we believe that the current landscape of ***orthopaedic surgical education is exposing future surgeons to greater rates of technology [3, 4, 20], which could result in even shorter learning curves for junior surgeons wishing to adopt ARo. Learning curve studies of surgical guidance systems have shown encouraging results for technological innovation into the surgical field. Other papers have found learning curves of 7, 7, and 40 cases for skin to skin times using Mako, OMNIBotics, and NAVIO robotic systems respectively for TKA [14, 15, 17]. Another paper on the NAVIO system found a learning curve of 12 cases for the steps of registration of bony surfaces, the digital reconstruction, intraoperative planning and bone resection [8]. A comparable study on MAKO revealed a wider LC range of 11–43 cases for operative time. The study revealed similar results of no LC associated with the component alignment [24].
However, learning curves of guidance systems cannot be directly compared to the results of an autonomous robotic system. The present study has ARO surgical times measured differently and show that robotic TKA has a somewhat variable learning curve which probably is surgeon-dependent and for the most part within 20 cases.
Limitations of our study at this time was that we did not have a control group. Focus of the study was on the learning curve associated with the adoption of an active robotic system, rather than outcomes. Unbiased multicenter outcome studies are necessary and should be performed in the future to evaluate clinical results. Another weakness in the study is the limited number of surgeons that participated in the FDA case series. Due to this limitation, wide variations in LC could be seen.
We feel that our findings are particularly relevant with the advent of widely available technologies available to surgeons in the operating room and provides a baseline with which to determine a safe, efficacious learning curve.
Conclusion
Active Robotic total knee arthroplasty is associated with a short learning curve of 10–20 cases. The learning curve was associated with the surgical time dedicated to the robotic specific portion of the case. There was no learning curve associated device-related complications, three dimensional component position, or patient reported outcome scores.
References
Berndt K, Rahm S, Dora C, Zingg PO (2019) Total hip arthroplasty with accolade/trident through the direct minimally invasive anterior approach without traction table: learning curve and results after a minimum of 5 years. Orthop Traumatol Surg Res 105:931–936
Boylan M, Suchman K, Vigdorchik J, Slover J, Bosco J (2018) Technology-assisted hip and knee arthroplasties: an analysis of utilization trends. J Arthroplasty 33:1019–1023
Camp CL, Krych AJ, Stuart MJ, Regnier TD, Mills KM, Turner NS (2016) Improving resident performance in knee arthroscopy: a prospective value assessment of simulators and cadaveric skills laboratories. J Bone Joint Surg Am 98:220–225
Cannon WD, Garrett WE Jr, Hunter RE, Sweeney HJ, Eckhoff DG, Nicandri GT et al (2014) Improving residency training in arthroscopic knee surgery with use of a virtual-reality simulator. A randomized blinded study. J Bone Joint Surg Am 96:1798–1806
Christ AB, Pearle AD, Mayman DJ, Haas SB (2018) Robotic-assisted unicompartmental knee arthroplasty: state-of-the art and review of the literature. J Arthroplasty 33:1994–2001
de Steiger RN, Lorimer M, Solomon M (2015) What is the learning curve for the anterior approach for total hip arthroplasty? Clin Orthop Relat Res 473:3860–3866
Ezzibdeh RM, Barrett AA, Arora P, Amanatullah DF (2020) Learning curve for the direct superior approach to total hip arthroplasty. Orthopedics. https://doi.org/10.3928/01477447-20200404-051-7
Geller JA, Rossington A, Mitra R, Jaramaz B, Khare R, Netravali NA. Rate of learning curve and alignment accuracy of an image-free handheld robot for total knee arthroplasty. Abstract number O44 presented at: European Knee Society; May 2–3, 2019; Valencia, Spain
Gofton WT, Papp SR, Gofton T, Beaule PE (2016) Understanding and taking control of surgical learning curves. Instr Course Lect 65:623–631
Gofton WT, Solomon M, Gofton T, Page A, Kim PR, Netting C et al (2016) What do reported learning curves mean for orthopaedic surgeons? Instr Course Lect 65:633–643
Hartford JM, Bellino MJ (2017) The learning curve for the direct anterior approach for total hip arthroplasty: a single surgeon’s first 500 cases. Hip Int 27:483–488
Jacofsky DJ, Allen M (2016) Robotics in arthroplasty: a comprehensive review. J Arthroplasty 31:2353–2363
Jeon SW, Kim KI, Song SJ (2019) Robot-assisted total knee arthroplasty does not improve long-term clinical and radiologic outcomes. J Arthroplasty 34:1656–1661
Kaper B (2020) Learning curve and time commitment assessment in the adoption of NAVIO robotic-assisted total knee arthroplasty. Orthopaedic proceedings. J Bone Joint Surg Br 102(Suppl 1):59
Kayani B, Konan S, Huq SS, Tahmassebi J, Haddad FS (2019) Robotic-arm assisted total knee arthroplasty has a learning curve of seven cases for integration into the surgical workflow but no learning curve effect for accuracy of implant positioning. Knee Surg Sports Traumatol Arthrosc 27:1132–1141
Kayani B, Konan S, Pietrzak JRT, Huq SS, Tahmassebi J, Haddad FS (2018) The learning curve associated with robotic-arm assisted unicompartmental knee arthroplasty: a prospective cohort study. Bone Joint J 100-B:1033–1042
Keggi J, Plaskos C (2017) Learning curve and early patient satisfaction of robotic-assisted total knee arthroplasty. Orthopaedic proceedings. J Bone Joint Surg Br 99(Suppl 4):59–59
Liow MHL, Chin PL, Pang HN, Tay DK, Yeo SJ (2017) THINK surgical TSolution-One((R)) (Robodoc) total knee arthroplasty. SICOT J 3:63
Lonner JH, Fillingham YA (2018) Pros and cons: a balanced view of robotics in knee arthroplasty. J Arthroplasty 33:2007–2013
Mabrey JD, Reinig KD, Cannon WD (2010) Virtual reality in orthopaedics: is it a reality? Clin Orthop Relat Res 468:2586–2591
Smith AF, Eccles CJ, Bhimani SJ, Denehy KM, Bhimani RB, Smith LS et al (2019) Improved patient satisfaction following robotic-assisted total knee arthroplasty. J Knee Surg. https://doi.org/10.1055/s-0039-1700837
Sodhi N, Khlopas A, Piuzzi NS, Sultan AA, Marchand RC, Malkani AL et al (2018) The learning curve associated with robotic total knee arthroplasty. J Knee Surg 31:17–21
Stulberg B, Zadzilka J, Kreuzer SW, Long W, Kissin Y, Liebelt RA, Zuhars J (2020) Results of an active robotic total knee arthroplasty us trial. Orthopaedic proceedings. J Bone Joint Surg Br 102(Suppl 2):9
Vermue H, Luyckx T, Winnock de Grave P, Ryckaert A, Cools AS, Himpe N, Victor J (2020) Robot-assisted total knee arthroplasty is associated with a learning curve for surgical time but not for component alignment, limb alignment and gap balancing. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06341-6
Funding
No funding was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors that they have no conflict of interest.
Ethics approval
Institutional review board (IRB) approval was obtained to conduct a multi-center, prospective, non-randomized US investigational device exemption clinical trial to evaluate the safety and effectiveness of robotic-assisted TKA using the TSolution One Total Knee Application (THINK Surgical).
Informed consent
Written informed consent was obtained from all study participants after IRB approval for the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mahure, S.A., Teo, G.M., Kissin, Y.D. et al. Learning curve for active robotic total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 30, 2666–2676 (2022). https://doi.org/10.1007/s00167-021-06452-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06452-8