
Abstract
Purpose
Autologous osteochondral transplantation is an established treatment for large-sized osteochondral lesions of the talus (OLT) with excellent short term outcomes. However, few studies assess the outcomes of autologous osteochondral transplantation at mid-term follow-up. The purpose of the current systematic review was to evaluate the clinical outcomes of the autologous osteochondral transplantation procedure in the treatment of OLT at mid-term and long-term follow-up.
Methods
A systematic search of the MEDLINE, EMBASE and Cochrane Library databases was performed in October 2017 based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Included studies were evaluated with regard to level of evidence (LOE) and quality of evidence (QOE) using the Coleman Methodology Score. Clinical outcomes, and complications were also evaluated.
Results
Eleven studies, with 500 ankles were included at a mean 62.8 months follow-up. Seven studies used the American Orthopaedic Foot and Ankle Society (AOFAS) score. The weighted mean preoperative AOFAS score was 55.1 ± 6.1, and the postoperative score was 86.2 ± 4.5, with 87.4% of patients (132 of 151) being reported as excellent or good results. In total, 53 of the 500 patients (10.6%) had complications. The most common complication was donor site morbidity with 18 patients (3.6%) at final follow-up. Thirty-one patients (6.2%) underwent reoperations, and 5 ankles (1.0%) were regarded as failed autologous osteochondral transplantation.
Conclusion
The current systematic review demonstrated that good clinical and functional outcomes can be expected following autologous osteochondral transplantation for the treatment of OLT, with a low failure rate. The results from this study show patients can be reasonably counselled to expect good clinical outcomes in the mid-term. MRI and radiographs showed restoration of articular surface as well as a minimal presence of osteoarthritis at mid-term follow-up. However, as low level and quality of evidence and the variability of the data may confound the data, further well-designed studies are necessary to determine the effectiveness of autologous osteochondral transplantation in the treatment for OLT.
Level of evidence
IV.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The operative treatment of osteochondral lesions of the talus (OLT) can be broadly divided into two categories: reparative procedures, including bone marrow stimulation (BMS), and replacement procedures, including autologous osteochondral transplantation (AOT). AOT is an established treatment for large-sized OLT, typically greater than 107 mm2 [22]. AOT can substitute the talar lesion with viable hyaline cartilage and subchondral bone by insertion of an autologous osteochondral graft.
Several clinical studies have demonstrated favourable outcomes following AOT in the treatment of OLT at short-term follow-up [5, 13, 25]. However, little evidence exists on the mid-term and longer-term follow-up. Additionally, few studies include a large number of patients or have a high level of evidence, limiting the ability to draw broad and meaningful conclusions about the effectiveness of the AOT procedure for the treatment of OLT beyond short-term follow-up.
Currently no systematic review exists of mid-term outcome following AOT for OLT, as such there is uncertainty regarding the mid-term outcome due to the low number of studies reporting this. Therefore, the purpose of the current systematic review was to evaluate the clinical outcomes analysing level and quality of evidence of the AOT procedure in the treatment of OLT at greater than 4 years following surgery. Our hypothesis was that the AOT procedure would produce good clinical outcomes at the mid- and long-term follow-up, with a high survivorship rate.
Materials and methods
Search strategy
A systematic review of the MEDLINE, EMBASE and Cochrane Library databases during October 2017 was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [15]. The search terms were: (osteochondral OR osteochondritis dissecans OR cartilage OR chondral OR transchondral) AND (talus OR talar OR ankle) AND (transplantation OR autograft OR transfer OR transplant OR mosaicplasty). References of all articles identified by this search were also screened for possible inclusion. The inclusion and exclusion criteria are shown in Table 1.
Two independent reviewers screened the titles, abstracts and full-text articles of all searched studies by applying the aforementioned criteria. Any disagreements were resolved by consensus and if disagreement persisted, a senior author was consulted.
Assessment of level of evidence and methodological quality
The level of evidence (LOE) was assessed using the criteria published by The Journal of Bone and Joint Surgery and the methodological quality of evidence (QOE) was assessed using the Modified Coleman Methodology Score [1, 17]. Two independent reviewers determined the MCMS for each study. If any discrepancy existed, the senior author evaluated the available data and a consensus was reached. Studies were considered excellent when they scored 85–100 points, good studies when they scored 70–84 points, fair studies when they scored 55–69 points and poor studies when they scored less than 55 points.
Data extraction and evaluation
Two reviewers independently extracted data from each study and assessed variable reporting of outcome data using parameters of previously published criteria for the treatment of OLT [11]. The authors also collected surgical procedure characteristics, including lesion size, donor-site for the grafts, diameter and number of the grafts required. Finally, objective and subjective outcomes, postoperative imaging, donor-site morbidity, complications, and additional surgeries were extracted and evaluated.
Statistical analysis
All statistical analyses were performed using SAS software version 9.3 (SAS Institute, Inc., Cary NC). Descriptive statistics were calculated for all continuous and categorical variables. Continuous variables were reported as weighted mean and estimated standard deviation, whereas categorical variables were reported as frequencies with percentages. A value of p < 0.05 was considered statistically significant.
Results
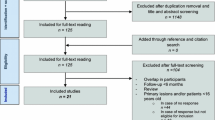
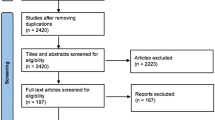
The search yielded 1096 studies, of these 11 studies met the inclusion and exclusion criteria for the current review (Fig. 1). The 11 included studies were published between 2001 and 2016.

PRISMA flow diagram
Patients demographics
A total of 500 patients, with a weighted mean age of 33.8 ± 4.8 years (range 27.0–43.7), underwent AOT procedure for the treatment of OLT [3, 5, 7, 8, 10, 12, 14, 20, 23, 27, 28]. The weighted mean postoperative follow-up time was 62.8 ± 13.3 months (range 48–85). The weighted mean lesion size was 110.5 ± 24.1 mm2 (range 85.0–152.9) (Table 2).
LOE and QOE
There were three studies of LOE III, and eight studies of LOE IV. The mean MCMS of all included studies was 55.9 ± 6.3 of 100 points. No studies were classified as good or excellent quality using the MCMS. There were three studies (27.3%) of fair quality and eight studies (72.7%) of poor quality. There were just two studies investigating a large numbers of patients (n > 60).
Surgery characteristics
The donor-sites used for harvesting osteochondral grafts were reported in all included studies, and nine studies were from the ipsilateral knee and two studies utilized ipsilateral talar articular facet. The donor-sites of the knee included the lateral femoral condyle, lateral edge (border) of the trochlea or medial femoral condyle. Ten studies reported the graft sizes and the number of grafts, with a weighted mean number of 1.7 ± 0.7 (range 1–3). The characteristics of the included studies are shown in Table 2.
Variable reporting of outcome data
The defined data that were reported in the studies included in this review are shown in Table 3. Demographic information including age and gender were reported in 100% of the included studies. While the study design, and imaging data were relatively well-reported variables with 86.4 and 81.8%, respectively, patient history were reported with only 54.5%, and clinical variables and patient-reported outcomes were the least reported variable in only 48.5 and 45.5% of the included studies.
Clinical and functional outcomes are listed in Table 4. Eight different outcome measures were recorded in 11 studies. The American Orthopaedic Foot and Ankle Society (AOFAS) score was the most frequently utilized in seven studies of the included. Of the seven studies that used AOFAS score, six studies reported both pre- and postoperative scores. The weighted mean preoperative AOFAS score was 55.1 ± 6.1 (range 45.9–65.5), and the postoperative score was 86.2 ± 4.5 (range 78–90), with 87.4% of patients (132 of 151) being reported as excellent or good results. The visual analogue scale (VAS) score was utilized in five studies, and all studies investigated both pre- and postoperative scores. The weighted mean preoperative VAS score was 6.8 ± 1.0 (range 5.9–8.5), and the postoperative score was 2.4 ± 0.9 (range 1.5–3.9). Two studies reported the Foot and Ankle Outcome Score (FAOS), with a weighted mean preoperative score of 51.0 ± 0.1 (range 50.9–51.1) and postoperative score of 80.5 ± 5.6 (range 75.6–86.8). One study reported Lysholm score as a donor site outcome measure, with a score of 88 points. Other outcomes were reported in 1 study, including SF-12, Hannover score, and Tegner activity score.
Of 11 studies, 9 studies (81.2%) reported the results of postoperative imaging. However, only five studies (45.5%) used MRI for follow-up evaluation. Of the studies reporting MRI results, two studies investigated a scoring system including magnetic resonance observation of cartilage repair tissue (MOCART) score, and the weighted mean MOCART score was 80.8 ± 6.8 (range 73.1–86.7). Four studies evaluated the occurrence rate of postoperative subchondral bone cysts using MRI, with a weighted mean occurrence rate of 50.0% (range 33.3–66.7%). Four studies utilized plain radiographs (36.4%) as a follow-up evaluation. On the radiographs, 6 of 154 patients (3.9%) demonstrated some degree of decrease of ankle joint space at a mean of 60.3 months follow-up. Postoperative CT was reported in only 1 study (9.1%).
Complications and reoperations
Complication rates ranged from 0 to 50.0%. In total, 54 of the 500 patients (10.8%) had complications. Complications included donor-site morbidity, infection, symptomatic hardware, nerve injury, anterior ankle impingement and non-union of the graft or osteotomy site. The most common complication was donor site morbidity with 26 patients (5.2%), but those with donor site morbidity decreased to 18 patients (3.6%) at final follow-up. A total of 31 patients (6.2%) underwent reoperations, including 11 arthroscopic debridements, 5 hardware removals, 3 ankle fusions, 2 revision surgeries (ACI and second AOT), and 10 unclear procedures. The authors deemed a total of five ankles (1.0%) failures, three required ankle fusions and two required revision surgeries.
Discussion
The most important finding in the current study was that the AOT procedure has been shown to result in good–excellent outcomes in 87.4% of patients at mid-term follow-up. Additionally, the rate of reoperation was relatively low at 6.1%, with only a small portion of these patients requiring a revision procedure or an ankle fusion (1.0%). However, the current literature consists of low LOE with poor MQOE, and this is consistent with the literature on cartilage repair in the talus as a whole [21]. Therefore, careful attention should be paid when evaluating the outcomes of the studies following AOT in the treatment of OLT, because low LOE and QOE studies may show overestimated outcomes compared to higher LOE and QOE studies [18]. Regarding the overall reporting of outcome data, the results from the current review were similar to those on microfracture for OLT [11]. The categories of demographic information and study design were well reported, while patient history, clinical variables, and patient-reported outcome data were reported less frequently. A higher percentage of reporting of imaging data has been shown in the current review than that of microfracture reported by Hannon et al. [11], but only 46% of studies utilized MRI follow-up evaluation, despite MRI assessment being crucial in the treatment of cartilage pathology. These results remind investigators to implement data collection according to the previously recommended list of variables for studies on OLT, as adequate reporting of data should be necessary to perform high-quality studies and establish further clinical evidence [11].
There has been significant growth in the literature regarding the clinical outcomes of AOT for the treatment of OLT. However, the majority of studies have reported outcomes with short-term follow-up. The current systematic review represents a comprehensive assessment of the studies with mid-term follow-up of patients who underwent AOT for the treatment of OLT. The AOT procedure provided excellent clinical results with significant improvement of clinical outcomes scores at a mean of 62.8 months follow-up time, and 87.4% of patients were reported to have excellent and good clinical results. This is an important finding as outcomes following BMS procedure have been shown to deteriorate in the mid-term [4, 26]. These findings, therefore, indicate that AOT results remain stable over time as previous systematic reviews have found similar results with the AOT procedure in the short-term [2, 4, 29]. This may be due to viable normal cartilage and subchondral bone of the autografts that have the potential to survive in the longer term compared to fibrous cartilage repair tissue following BMS.
Overall, additional surgeries, including arthroscopic debridement, removal of symptomatic hardware, ankle fusion and revision AOT, were required in 6.2% of patients. However, the clinical failure rate was only 1.0% at the mid-term. The current study has found that there is good integration of the graft with surrounding tissues, and good quality cartilage remained on MRI findings at mid-term follow-up. However, there is still a concern that the current study has shown that a high rate of postoperative cyst formation after AOT for OLT in the mid-term follow-up. Although the clinical impact of postoperative subchondral cyst formation was not found to be significant in the short-term, the long-term outcomes of these cyst formations are not yet known [24]. Subchondral cysts have the potential to contribute to the graft failure or poorer outcomes in the long-term. Further research is required to investigate the long-term consequences of these cyst formations as well as the longevity of cartilage and subchondral bone of the grafts following AOT.
Donor-site morbidity was the most commonly reported complication in 5.2% of patients. However, knee donor-site morbidity can improve over time from the short- to mid-term follow-up. Fraser et al. [6] showed that the overall incidence of DSM was 12.5% at 2 years after surgery and it decreased to 5% at the final follow-up of 41 months. Additionally, Paul et al. [19] found significant clinical improvement in the Lysholm score over time at 6-month intervals up to 30 months. Furthermore, none of the included studies showed an increase in donor-site morbidity over the course of the follow-up, suggesting that knee donor-site morbidity may decrease over time. Further studies of longer follow-up are required to support the current study findings.
The most common donor site utilized was the non-weightbearing portion of the lateral femoral condyle. The advantage of harvesting from the lateral femoral condyle is that the topography of the lateral femoral condyle closely matches the joint surface of the talar dome [16]. Two studies utilized anterior articular talar facet medially or laterally as a donor site. While they did not report any donor-site morbidity, it is difficult to assess and diagnose donor-site morbidity accurately as both the donor and recipient site are the same joint. In addition, few studies reported AOT procedure using articular talar facet as a donor site. As the ankle joint is a highly congruent small joint, the anterior articular talar facet may not be an optimal donor site for larger lesions. However, scant evidence of the AOT procedure using talar facet graft still exists, and further longer follow-up studies investigating the outcomes of the harvest site of the talus and its influence on the ankle joint is necessary.
Despite the encouraging clinical and functional outcomes reported, only four studies reported plain radiographic outcomes at mid-term follow-up. In the current review, the rate of ankle joint narrowing was low, with only 3.9% of ankles showing reduced joint space on radiography at final follow-up. While following BMS, Ferkel et al. [4] evaluated 50 patients at a mean of 71 months follow-up and found that 34% of patients demonstrated advancement by at least one grade of arthritis on radiography. The current review also demonstrated that only two studies evaluated the postoperative MRI using qualitative outcome measures, despite postoperative MRI follow-up is crucial to evaluate the graft/host integration, chondral wear, and subchondral bone condition following AOT procedure [8, 23]. However, their results were encouraging with a mean MOCART score of 80.8, suggesting the cartilage of the graft is maintained with good quality over mid-term. Although very few studies reported on the postoperative imaging results, these findings have suggested that the AOT procedure may afford the ankle joint increase longevity with hyaline character of the grafts. In contrast, BMS fills the defect site with fibrous cartilage repair tissue that is a less durable alternative will inevitably deteriorate over time [4]. This finding is supported by the low rate of failure in the included studies. Additionally, Hangody et al. [9] have reported that biopsy specimens following the AOT procedure were similar to native cartilage in both type II collagen and proteoglycan content.
The most commonly reported scoring system was the AOFAS score. However, the current review found that the reported outcome measures were heterogeneous, with eight different scoring systems. Currently there is a lack of a validated scoring system for OLT. To provide more accurate analysis, a novel validated scoring system for the clinical evaluation in the treatment of OLT is warranted. Despite this, the results from this study show patients can be reasonably counselled to expect good clinical outcomes in the mid-term.
This systematic review has several limitations and sources of potential bias. The search criterion was limited to MEDLINE, EMBASE and The Cochrane Library, with articles exclusively published in English. The QOE of the included studies was poor, and the LOE was also low with no Level I or II study. However, this is consistent with the literature on cartilage repair as a whole and is not exclusive to this treatment [21]. The majority of the studies were retrospective and did not have a control, preventing us from having a true reference point to compare the results against. The data extraction was not performed in a blinded fashion, but rather was performed by two independent reviewers and later confirmed by the lead author.
Conclusion
The current systematic review demonstrated that good clinical and functional outcomes at mid-term can be expected following AOT procedure for the treatment of OLT, with a low failure rate. In addition, MRI and radiographs showed restoration of articular surface as well as a minimal presence of osteoarthritis at mid-term follow-up. However, as low level and quality of evidence and the variability of the data may confound the data, further well-designed studies are necessary to determine the effectiveness of AOT procedure in the treatment for OLT.
References
Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD (2000) Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 10:2–11
Dahmen J, Lambers KTA, Reilingh ML, van Bergen CJA, Stufkens SAS, Kerkhoffs GMMJ. (2017) No superior treatment for primary osteochondral defects of the talus. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-017-4616-5
de l’Escalopier N, Barbier O, Mainard D, Mayer J, Ollat D, Versier G (2015) Outcomes of talar dome osteochondral defect repair using osteocartilaginous autografts: 37 cases of Mosaicplasty®. Orthop Traumatol Surg Res 101:97–102
Ferkel RD, Zanotti RM, Komenda GA, Sgaglione NA, Cheng MS, Applegate GR et al (2008) Arthroscopic treatment of chronic osteochondral lesions of the talus: long-term results. Am J Sports Med 36:1750–1762
Fraser EJ, Harris MC, Prado MP, Kennedy JG (2016) Autologous osteochondral transplantation for osteochondral lesions of the talus in an athletic population. Knee Surg Sports Traumatol Arthrosc 24:1272–1279
Fraser EJ, Savage-Elliott I, Yasui Y, Ackermann J, Watson G, Ross KA et al (2016) Clinical and MRI donor site outcomes following autologous osteochondral transplantation for talar osteochondral lesions. Foot Ankle Int 37:968–976
Georgiannos D, Bisbinas I, Badekas A (2016) Osteochondral transplantation of autologous graft for the treatment of osteochondral lesions of talus: 5- to 7-year follow-up. Knee Surg Sports Traumatol Arthrosc 24:3722–3729
Haleem AM, Ross KA, Smyth NA, Duke GL, Deyer TW, Do HT et al (2014) Double-plug autologous osteochondral transplantation shows equal functional outcomes compared with single-plug procedures in lesions of the talar dome: a minimum 5-year clinical follow-up. Am J Sports Med 42:1888–1895
Hangody L, Dobos J, Baló E, Pánics G, Hangody LR, Berkes I (2010) Clinical experiences with autologous osteochondral mosaicplasty in an athletic population: a 17-year prospective multicenter study. Am J Sports Med 38:1125–1133
Hangody L, Kish G, Módis L, Szerb I, Gáspár L, Diószegi Z et al (2001) Mosaicplasty for the treatment of osteochondritis dissecans of the talus: two to seven year results in 36 patients. Foot Ankle Int 22:552–558
Hannon CP, Murawski CD, Fansa AM, Smyth NA, Do H, Kennedy JG (2013) Microfracture for osteochondral lesions of the talus: a systematic review of reporting of outcome data. Am J Sports Med 41:689–695
Imhoff AB, Paul J, Ottinger B, Wörtler K, Lämmle L, Spang J et al (2011) Osteochondral transplantation of the talus: long-term clinical and magnetic resonance imaging evaluation. Am J Sports Med 39:1487–1493
Kennedy JG, Murawski CD (2011) The treatment of osteochondral lesions of the talus with autologous osteochondral transplantation and bone marrow aspirate concentrate: surgical technique. Cartilage 2:327–336
Kreuz PC, Steinwachs M, Erggelet C, Lahm A, Henle P, Niemeyer P (2006) Mosaicplasty with autogenous talar autograft for osteochondral lesions of the talus after failed primary arthroscopic management: a prospective study with a 4-year follow-up. Am J Sports Med 34:55–63
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med 151:W65-94
Marymont JV, Shute G, Zhu H, Varner KE, Paravic V, Haddad JL et al (2005) Computerized matching of autologous femoral grafts for the treatment of medial talar osteochondral defects. Foot Ankle Int 26:708–712
Marx RG, Wilson SM, Swiontkowski MF (2015) Updating the assignment of levels of evidence. J Bone Jt Surg Am 97:1–2
Moher D, Cook DJ, Jadad AR, Tugwell P, Moher M, Jones A et al (1999) Assessing the quality of reports of randomised trials: implications for the conduct of meta-analyses. Health Technol Assess 3:1–98
Paul J, Sagstetter A, Kriner M, Imhoff AB, Spang J, Hinterwimmer S (2009) Donor-site morbidity after osteochondral autologous transplantation for lesions of the talus. J Bone Jt Surg Am 91:1683–1688
Paul J, Sagstetter M, Lämmle L, Spang J, El-Azab H, Imhoff AB et al (2012) Sports activity after osteochondral transplantation of the talus. Am J Sports Med 40:870–874
Pinski JM, Boakye LA, Murawski CD, Hannon CP, Ross KA, Kennedy JG (2016) Low level of evidence and methodologic quality of clinical outcome studies on cartilage repair of the ankle. Arthroscopy 32:214–222
Ramponi L, Yasui Y, Murawski CD, Ferkel RD, DiGiovanni CW, Kerkhoffs GMMJ. et al (2016) Lesion size is a predictor of clinical outcomes after bone marrow stimulation for osteochondral lesions of the talus: a systematic review. Am J Sports Med 45:1698–1705
Ross AW, Murawski CD, Fraser EJ, Ross KA, Do HT, Deyer TW et al (2016) Autologous osteochondral transplantation for osteochondral lesions of the talus: does previous bone marrow stimulation negatively affect clinical outcome? Arthroscopy 32:1377–1383
Savage-Elliott I, Smyth NA, Deyer TW, Murawski CD, Ross KA, Hannon CP et al (2016) Magnetic resonance imaging evidence of postoperative cyst formation does not appear to affect clinical outcomes after autologous osteochondral transplantation of the talus. Arthroscopy 32:1846–1856
Scranton PE Jr, Frey CC, Feder KS (2006) Outcome of osteochondral autograft transplantation for type-V cystic osteochondral lesions of the talus. J Bone Jt Surg Br 88:614–619
Shimozono Y, Coale M, Yasui Y, O’Halloran A, Deyer TW, Kennedy JG (2017) Subchondral bone degradation following microfracture for osteochondral lesions of the talus. Am J Sports Med. https://doi.org/10.1177/0363546517739606
Valderrabano V, Leumann A, Rasch H, Egelhof T, Hintermann B, Pagenstert G (2009) Knee-to-ankle mosaicplasty for the treatment of osteochondral lesions of the ankle joint. Am J Sports Med 37(Suppl 1):105S-111S
Yoon HS, Park YJ, Lee M, Choi WJ, Lee JW (2014) Osteochondral autologous transplantation is superior to repeat arthroscopy for the treatment of osteochondral lesions of the talus after failed primary arthroscopic treatment. Am J Sports Med 42:1896–1903
Zengerink M, Struijs PA, Tol JL, van Dijk CN (2010) Treatment of osteochondral lesions of the talus: a systematic review. Knee Surg Sports Traumatol Arthrosc 18:238–246
Funding
No funding was received by any of the authors related to this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This manuscript is a systematic review and does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Shimozono, Y., Hurley, E.T., Myerson, C.L. et al. Good clinical and functional outcomes at mid-term following autologous osteochondral transplantation for osteochondral lesions of the talus. Knee Surg Sports Traumatol Arthrosc 26, 3055–3062 (2018). https://doi.org/10.1007/s00167-018-4917-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-018-4917-3