
Abstract
Purpose
Recently, the functional flexion axis has been considered to provide a proper rotational alignment of the femoral component in total knee arthroplasty. Several factors could influence the identification of the functional flexion axis. The purpose of this study was to analyse the estimation of the functional flexion axis by separately focusing on passive flexion and extension movements and specifically assessing its orientation compared to the transepicondylar axis, in both the axial plane and the frontal plane.
Methods
Anatomical and kinematic acquisitions were performed using a commercial navigation system on 79 patients undergoing total knee arthroplasty with cruciate substituting prosthesis design. The functional flexion axis was estimated from passive movements, between 0° and 120° of flexion and back. Intra-observer agreement and reliability, internal–external rotation and the angle with the surgical transepicondylar axis, in axial and frontal planes, were separately analysed for flexion and extension, in pre- and post-implant conditions.
Results
The analysis of reliability and agreement showed good results. The identification of the functional flexion axis showed statistically significant differences both in relation to flexion and extension and to pre- and post-implant conditions, both in frontal plane and in axial plane. The analysis of internal–external rotation confirmed these differences in kinematics (p < 0.05, between 25° and 35° of flexion).
Conclusions
The identification of the functional flexion axis changed in relation to passive flexion and extension movements, above all in frontal plane, while it resulted more stable and reliable in axial plane. These findings supported the possible clinical application of the functional flexion axis in the surgical practice by implementing navigated procedures. However, further analyses are required to better understand the factors affecting the identification of the functional flexion axis.
Level of evidence
IV.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In total knee arthroplasty (TKA), the rotational alignment of the femoral component has been reported to influence both tibiofemoral and patellofemoral kinematics [28, 30]. The femoral component malpositioning is indeed a critical aspect in TKA since it may lead to altered joint kinematics, instability stiffness and excessive wear of the polyethylene component [1, 16, 19, 25, 32].
Literature reported several methods, which can be considered as gold standards and that are currently used to identify the optimal placement of the femoral component. These methods are generally based on the acquisition of specific anatomical landmarks—i.e. the transepicondylar axis (TEA) [1], the axis tangent to the posterior condyles (PCA) [24] or the Whiteside line, which is defined as the anteroposterior axis of the distal femur [29]. However, the accuracy in identifying these anatomical landmarks has been reported to be strictly correlated with the surgeon’s experience [27, 28], and therefore, their use could lead to implant malpositioning.
Recently, several functional methods have been proposed to overcome these issues. In particular, a method called functional flexion axis (FFA) has been introduced to reduce the problem related to inter-surgeon variability. This method is inherently joint- and patient-specific, and it is based on the identification of a functional reference estimated through the knee joint mean helical axis (MHA) [33].
Supported by the literature [5, 9, 26, 32, 33], the FFA can be hypothesised to properly represent the main axis of rotation of the knee during joint flexion–extension movements. Several studies reported the benefits of using the FFA both from a biomechanical perspective, to describe the tibiofemoral kinematics during flexion–extension movements [5, 9, 26, 32, 33], and from a clinical point of view, to assess the rotational alignment of the femoral component during TKA [8, 10, 11, 25, 28].
On the other hand, the literature highlighted the necessity of additional analyses to better verify the suitability of the FFA in the daily clinical practice and its reliability with respect to the anatomical references [8, 10, 25, 28]. In particular, several works analysed the differences introduced by the surgery [25, 32], but—at present—there is no study focused on the influence that the intra-operative passive kinematics could have on the FFA identification.
For instance, as highlighted by Amis et al. [2] in a deep analysis of the patellofemoral joint and by a recent work published by Feng et al. [13] on the tibiofemoral joint, the joint kinematics can differ when considering hypothetically “specular” or “symmetrical” actions or movements, like knee joint flexion and extension.
Therefore, since the FFA is inherently defined on the basis of joint kinematics, the main hypothesis of this work was that differences in joint kinematics during passive movements usually considered “symmetrical” (like flexion and extension) could influence the identification of the FFA orientation.
The main purpose of the present study was therefore to acquire knee joint passive range of motion (PROM) during navigated TKA and analyse the knee joint kinematics and the reliability in the identification of FFA orientation both before and after the implant placement, specifically focusing on the assessment of flexion and extension movements, separately. This kind of analysis applied to navigated TKA procedure represented the main novelty of the work.
Materials and methods
A cohort of 111 patients presenting knee osteoarthritis (OA) and consecutively undergoing primary cemented TKA with posterior-stabilised cruciate substituting rotating-platform prostheses (Gemini, Waldemar Link GmbH & Co, Hamburg, Germany) including patellar resurfacing was prospectively enrolled in this study between September 2008 and September 2010. Inclusion criteria consisted in primary OA and body mass index (BMI) <40 kg/m2. All patients with knee OA were screened regardless from radiographic severity of the disease (Kellgren–Lawrence score up to 4). Exclusion criteria included all with post-traumatic and rheumatoid arthritis, anterior cruciate ligament (AC) and/or posterior cruciate ligament (PCL) instability (which could lead to an internal derangement of knee kinematics), previous surgeries on the ipsilateral limb and limited range of motion (ROM) with active flexion <90°. Finally, thirty-two patients were excluded and seventy-nine patients were thus included in this analysis (Table 1).
The study was approved by the institutional review board (protocol number 11551/CE/US/mL, 5 May 2006).
Navigation set-up
All the surgeries were performed by using a commercial image-free navigation system (BLU-IGS, Orthokey LLC, Delaware, USA) that neither altered the original surgical technique nor affected knee kinematics. This system was reported by the producer to have a 3D RMS volumetric accuracy of 0.350 mm and a 3D RMS volumetric repeatability of 0.200 mm [31], whereas the navigated protocol and the intra-tester repeatability of the method were reported to be about 1 mm for translations and 1° for rotations [20, 21]. The navigation system was used both to guide the surgery and to intra-operatively acquire the anatomical data and the passive joint kinematics. TKA planning was intra-operatively performed using several anatomical landmarks including the TEA, PCA and Whiteside line [6]. Moreover, a software specifically designed for kinematic analysis (KLEE, Orthokey LLC, Lewes, Delaware, USA) allowed to acquire kinematic data in both pre-implant and post-implant conditions [20, 21]. The joint coordinate reference system (JCS) was specifically defined by means of additional anatomical landmarks acquisitions, as described in [8], proposed by Cole et al. [6] and widespread by Grood and Suntay [14].
Surgical procedure
All the surgeries were performed under spinal anaesthesia. After subcutaneous dissection, the capsule was opened to register patients’ anatomy, while maintaining intact cruciate ligaments and menisci. After skin incision and before meniscal and anterior cruciate ligament (ACL) removal, femoral and tibial trackers were fixed, with patella reduction, and anatomical and pre-implant kinematic data were acquired, while post-implant kinematic data were collected after definitive prosthesis implantation. Cemented TKA was then performed by using the navigation system and following the suggested standard planning and surgical procedure.
Kinematic acquisition protocol
Passive flexion and extension movements, from full extension to full flexion, were separately acquired three times for each patient, both before and after implant positioning. Both the PROMs were performed by the expert operating surgeon (M.M.) maintaining the foot in neutral position, without any additional rotation respect to the tibial axis to not constrain the knee joint. During the whole sets of acquisition, the patella was maintained reduced in the anatomical position by using a temporary suture repair.
Data analysis
All the information acquired by the navigation system were offline processed with proprietary routines (Matlab, MathWorks, Natick, MA, USA).
In order to highlight any difference in kinematics that could influence the FFA estimation, the relative motion of tibia with respect to femur was first analysed with Grood and Suntay algorithm [14]. Rotations during the passive range of motion (PROM) were computed and described in terms of instantaneous flexion–extension (FE) and internal–external (IE) rotations. For statistical comparison of kinematic behaviour, continuous data obtained from passive movements were re-sampled each 5° of knee flexion, extrapolating the values from 0° to 120° of knee flexion. Internal–external rotation values of flexion and extension were then averaged on the three repetitions, at every re-sampled angle, for both pre- and post-operative conditions for each patient. The mean values obtained for each patient were then averaged for the whole set of patients, thus obtaining one mean curve for both flexion and extension separately before and after the implant positioning.
The MHA computational method was used to estimate the FFA; in particular, the finite helical axis (FHA) was evaluated for each time step starting from full extension and for each PROM, and then, with a least square approach, the corresponding mean FFA was estimated [33]. An average FFA obtained from the three performed repetitions was computed separately for flexion (0°–120°) and extension (120°–0°) PROMs in both pre- and post-implant conditions. Since the FFA aimed to be used in TKA femoral component orientation, the only FFA orientation with respect to the TEA was studied in two different anatomical planes (specifically axial and frontal) in order to easily compare the obtained results from a clinical point of view using a common anatomical reference (i.e. TEA), as a gold standard (Fig. 1).

Graphical representation of the angle between the FFA and the TEA in frontal and axial planes (Frontal plane: negative angle value for varus rotation and positive angle value for valgus rotation. Axial plane: negative angle value for external rotation and positive angle value for internal rotation)
Variability in the identification of the TEA was reduced by considering only one expert operator (M.M.)—an orthopaedic surgeon with more than 30 years of experience—who performed also all the surgeries.
Statistical analysis
Starting from the available literature [8], the minimum sample size was prospectively estimated for a two-tailed independent Student’s t test with a power of 95 %, hypothesising for the estimated FFA–TEA angle, a mean of difference of 1.5° ± 1.5° between flexion and extension PROM in both the frontal plane and the axial plane. Considering the most restrictive factor, at least 27 patients should have been enrolled.
First, the analysis of the FFA reliability and agreement was performed to evaluate the robustness of the proposed method. The repeatability coefficient [4] and the intra-class correlation coefficient (ICC) [22] were used for the analysis of the FFA reliability and agreement, respectively, evaluated from within-subject replicated measurements obtained with the same method. Confidence intervals (CIs) for every analysed parameter were evaluated at 95 % level. Afterwards, the difference in internal–external rotations during flexion and extension PROM paths in pre- and post-operative conditions was tested with independent and two-tailed paired Student’s t test, respectively, thus evaluating any statistical difference between flexion and extension at each frame of PROM. Moreover, a descriptive statistical analysis was performed on the FFA–TEA angles in both axial and frontal planes, on both pre- and post-implant values to check the data distribution, and a Shapiro–Wilk test of normality was also performed in order to evaluate the null hypothesis of the population, which is normally distributed. Independent Student’s t test was performed on the angles identified by the FFA with respect to the TEA in both the planes, to evaluate any statistical difference in the estimation of the FFA between flexion and extension PROMs. These inferential statistics were also individually performed on both pre- and post-implant data. Finally, a paired Student’s t test was executed between pre-operative and post-operative estimation of the FFA analysing the corresponding angles between the FFA and the TEA, in order to identify the differences introduced by the implant in the FFA estimation.
Statistical significance was set to 95 % (p = 0.05) for all the tests, performed with Analyse-it software (Analyse-it Software, Ltd., The Tannery 91 Kirkstall Road, Leeds, LS3 1HS, UK.
Results
The analysis of the intra-observer reliability (i.e. ICC values) and agreement (i.e. repeatability coefficient) of the FFA–TEA angle considered both in frontal and axial views and in pre- and post-implant conditions is reported in Table 2.
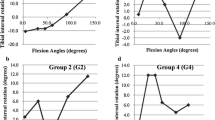
The analysis of the amount of IE rotation during flexion and extension PROMs in both pre- and post-implant conditions is reported in Fig. 2, showing a statistically significant difference between the two PROMs in pre-implant condition, between 25° and 35° of flexion (p < 0.05).

Internal–external (IE) rotation (°) of the tibia on the femur during PROM, in pre- and post-implant conditions, for flexion and extension paths of movement (negative value for internal rotation and positive value for external rotation)
The normality test reported that all the data presented normal distribution (Shapiro–Wilk test, n.s.).
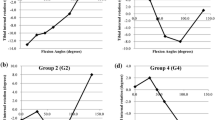
Independent Student’s t test highlighted statistically significant differences between flexion and extension PROMs in both frontal (−8.5° ± 7.0° vs −1.7° ± 5.1° in pre-operative conditions and −3.2° ± 5.4° vs 0.7° ± 5.2° in post-operative conditions) and axial planes (−0.9° ± 4.4° vs −4.0° ± 4.7° in pre-operative conditions and 1.3° ± 3.8° vs −0.6° ± 4.5° in post-operative conditions, Fig. 3). Analogously, several statistically significant differences were found comparing pre- and post-operative conditions (Fig. 4).

Histogram plot corresponding of FFA–TEA angles, as mean ± SD, grouped to compare flexion and extension movements in both planes and conditions (Frontal plane: negative angle value for varus rotation and positive angle value for valgus rotation. Axial plane: negative angle value for external rotation and positive angle value for internal rotation). *p < 0.05

Histogram plot corresponding of FFA–TEA angles, as mean ± SD, grouped to compare pre- and post-operative conditions in both planes and movements (Frontal plane: negative angle value for varus rotation and positive angle value for valgus rotation. Axial plane: negative angle value for external rotation and positive angle value for internal rotation). *p < 0.05
Discussion
The most important finding of the present study was that the estimation of the FFA orientation changed in the frontal plane in relation to flexion and extension PROMs, above all considering pre-operative conditions. Specifically, pre-implant FFA orientation—computed during flexion PROM—significantly differed from the TEA, whereas the FFA–TEA angle resulting from extension PROM was found to be close to zero. Moreover, the orientation of the FFA changed significantly after TKA in both flexion and extension—mostly in the frontal plane—while the correspondence between the FFA and the TEA was almost maintained in the axial plane.
The role of the FFA in TKA component positioning has been widely analysed in the literature [3, 8, 10, 11, 25, 28], due to its inherently patient- and joint-specific characteristics. These features indeed pretend to make the FFA less influenced by the variability typically related to the manual identification of anatomical landmarks [12, 18]. Several authors evaluated the usefulness of FFA in both assessing knee kinematics [10, 25, 26, 32] and, more recently, defining the rotational alignment of the femoral component in TKA [8, 10, 25, 28]. Furthermore, literature analysed both the FFA reliability with respect to defined anatomical landmarks and also the correspondence between the FFA and the TEA, thus investigating the hypothesis of a functional–anatomical relationship [1, 3, 7, 17].
While literature agreed on the fact that the FFA requires further analyses in order to achieve the possibility of being used in the daily clinical practice [8, 11, 15, 25], at present no studies have been focused on analysing the influence of the performed movements on the reliability of the functional procedure itself. Most of the reported studies were in fact based on the hypothesis that passive flexion and extension movements were exactly “symmetrical”, thus giving no importance to the influence of the specific movement on the FFA estimation.
Arguing on this issue, we looked at scientific literature thus to find some references that could support the hypothesis of a “hysteretic” behaviour of the knee joint. Although focused on the patellofemoral joint, the first work, which underlined the differences between flexion and extension movements, was authored by Amis et al. [2]. They specifically underlined the importance of considering the joint movement as not “mirrored”. More recently, riding on this concept, Feng et al. in an in vivo experimental study analysed the motion of the femoral condyles during continuous lunge, finding that the pattern of the internal–external rotation was different in the middle part of knee joint flexion, when considering flexion and extension movements, separately.
Concerning the FFA definition, several authors decided to analyse the only flexion PROMs [3, 11, 25] on defined different ranges of motion. Out of these, Asano et al. [3] analysed the knee PROM from 0° to 90° of flexion, reporting a good correspondence between the FFA and the surgical TEA in axial plane (with an external rotation angle with respect to the posterior condylar axis ranging from −1.0° to 5.5° and from 1.0° to 6.0°, respectively). Our results are also in agreement with Eckhoff et al. [11], who assessed the FFA by passively flexing the joint from 15° to 115° and comparing the FFA and the TEA in frontal and axial plane and specifically reported differences in the coronal view (average 1.8°; range 0.1°–3.9°) and in the transverse view (average 2.3°; range 0.2°–5.2°). Oussedik et al. [25] estimated the FFA in axial plane performing a PROM from 20° to 80° of flexion and comparing it to the TEA. They reported that the mean pre-incision FFA was similar to the intra-operative FFA and observed no differences in variability between surgical TEA and pre-incision FFA, showing an average angular deviation of the FFA with respect to the TEA congruent with our findings. Further, several authors estimated the FFA by performing complete flexion–extension cycles (from 0° to 120° and back to 0°), but without analysing the contribution of flexion and extension, separately. Doro et al. [10], for instance, assessed the reproducibility and reliability of the FFA in the axial plane under different testing conditions. They specifically reported that the variance of the FFA axis determined under neutral loading conditions was smaller than the variance of the TEA when the kinematics were measured in the closed surgical condition. This finding gave consistency to the possibility of using the FFA during navigated procedure. However, varus, valgus and internal loading of the leg were reported to increase the variability in identifying the FFA from about 2° up to about 6°. These values of variability are, however, consistent with our reliability analysis. Finally, Colle et al. [7, 8], performing two different in vivo studies on the FFA, reported good reliability of the FFA estimation during TKA, even compared to ACL reconstructions (whose patients could be considered providing a “normal” kinematics). Compared to our reliability analysis, they specifically reported lower repeatability coefficients ranging between 2.9° and 4.9° and lower ICC ranging between 0.83 and 0.95.
Summarising our findings, the present study reported that the FFA computed in pre-operative conditions in the frontal plane by using the flexion PROMs showed a greater deviation from the TEA and a higher variability. In the axial plane, the bigger deviation derived instead from the analysis of the extension PROMs. These values were reduced in post-operative conditions due to the insertion of the prosthesis, whose design and position contributed to define the new knee movement. Both pre-operative and post-operative FFA–TEA angles were in agreement with the values previously reported by Colle et al. [8].
Compared to literature, the present study highlighted specific differences introduced by flexion and extension PROMs in identifying the FFA. These differences could be attributed to different factors. First, the presence of the screw-home mechanism occurs in the first degrees of knee flexion, as highlighted in Fig. 2. Due to the inherent limitation of the method used to estimate the FFA (i.e. the MHA), an internal rotation contributed to angularly shift the FFA orientation above all in the frontal plane. For this reason, the effect of the screw home was more evident in the frontal plane during passive flexion, reporting higher value of angular difference with respect to the TEA. On the contrary, during passive extension, the tibia maintained a constant external rotation while flexed and the FFA estimation resulted less stable only in the axial plane probably due to secondary rotations involuntarily introduced by the surgeon. During flexion, the articular surfaces were supposed in fact to be in contact thus to lead the movement, whereas possible abnormal rotations could be introduced during extension (especially during the first 30° of knee flexion). These induced rotations can be hypothesised to be a result of the joint opening—as under varus/valgus stress—caused by temporary loss of contact between the articular surfaces. The absence of the screw-home mechanism and this lack of articular congruence could lead to this unusual FFA variation in the axial plane during extension. The analysis of IE rotation during flexion and extension confirmed the influence of screw home in estimating FFA, by showing a statistically significant difference between 25° and 35° of knee flexion (Fig. 2). Although in different conditions, these analyses are coherent with the findings reported by Feng et al. [13], who specifically identified differences in tibial internal–external rotation between flexion and extension in the middle range of flexion. This fact underlined the possibility that in this range of flexion the knee joint could be considered, somehow, activity-dependent and thus presented an “hysteretic” behaviour. The OA was supposed to be the second factor introducing the differences in the FFA orientation between flexion and extension movements. The OA mainly affected the distal condyles and less the posterior ones, thus showing a more evident effect on the physiological limb alignment (varus/valgus) on the frontal plane. Moreover, the OA, in general, influences the limb deformity in a not constant way throughout the flexion arc [23], but it results to be more evident in the first 30° of flexion, exactly during the screw-home mechanism [7].
The obtained results were in general supported by good values of the repeatability coefficient and the ICC in both pre- and post-implant conditions, for both flexion and extension PROMs. Compared to previous similar analysis [7, 8], a slightly greater variability was, however, identified for the extension PROM.
This study presented some limitations. The intra-operative registration was performed by manually identify some specific landmarks with the risk of introducing possible bias. At present, this procedure could be considered the gold standard for image-free navigation systems [17]. However, this bias was minimised by involving only one skilled expert surgeon, thus limiting the variability during the acquisition. Furthermore, as previously discussed, the flexion and extension PROMs were performed without control on applied torques, but with the only visual feedback. This limitation was, however, calmed by performing the PROMs three times and checking whether the corresponding variability was out of pre-defined thresholds. Finally, the passive joint kinematics was acquired in both pre- and post-implant conditions with the capsule maintained vented. However, also this approach was reported not to have a significant effect on the FFA estimation [25]. Moreover, this study could not claim to have wider biomechanical perspectives since, due to inherent limitation of an in vivo intra-operative study, all the patients were analysed under anaesthesia. It was possible to estimate the FFA by using only passive movements, thereby artificially eliminating the influence of the muscular tone.
However, these limitations did not make this study lose generality for the specific navigated application, and the here-reported findings continue to support the possible clinical application of FFA to the daily surgical practice by implementing ad hoc navigated procedures.
Conclusions
The malpositioning of the femoral component is a critical aspect in TKA. Several methods, based on both anatomical and kinematic features, have been introduced and used in computer-assisted surgery to guide the surgeon during the implant placement, like FFA. This paper demonstrated that passive flexion and extension movements influenced in a different way the estimation of the FFA orientation. Although the FFA showed good stability and reliability in axial plane, the use of the FFA in the daily surgical practice still need further and deeper analyses to better understand the relationship between the FFA orientation, the performed PROM and the presence of different levels of OA. However, due to the inherent importance of defining operator-independent and patient-specific references, the presented findings remain particularly important when considering the FFA as a possible functional landmark during navigated TKA.
References
Aglietti P, Sensi L, Cuomo P, Ciardullo A (2008) Rotational position of femoral and tibial components in TKA using the femoral transepicondylar axis. Clin Orthop Relat Res 466:2751–2755
Amis AA, Senavongse W, Bull AMJ (2006) Patellofemoral kinematics during knee flexion–extension: an in vitro study. J Orthop Res 24:2201–2211
Asano T, Akagi M, Nakamura T (2005) The functional flexion–extension axis of the knee corresponds to the surgical epicondylar axis: in vivo analysis using a biplanar image-matching technique. J Arthroplasty 20:1060–1067
Bartlett JW, Frost C (2008) Reliability, repeatability and reproducibility: analysis of measurement errors in continuous variables. Ultrasound Obstet Gynecol Off J Int Soc Ultrasound Obstet Gynecol 31:466–475
Blankevoort L, Huiskes R, De Lange A (1990) Helical axes of passive knee joint motions. J Biomech 23:1219–1229
Cole GK, Nigg BM, Ronsky JL, Yeadon MR (1993) Application of the joint coordinate system to three-dimensional joint attitude and movement representation: a standardization proposal. J Biomech Eng 115:344–349
Colle F, Bignozzi S, Lopomo N, Zaffagnini S, Sun L, Marcacci M (2012) Knee functional flexion axis in osteoarthritic patients: comparison in vivo with transepicondylar axis using a navigation system. Knee Surg Sports Traumatol Arthrosc 20:552–558
Colle F, Lopomo N, Bruni D, Visani A, Iacono F, Zaffagnini S, Marcacci M (2014) Analysis of knee functional flexion axis in navigated TKA: identification and repeatability before and after implant positioning. Knee Surg Sports Traumatol Arthrosc 22:694–702
Dennis DA, Mahfouz MR, Komistek RD, Hoff W (2005) In vivo determination of normal and anterior cruciate ligament-deficient knee kinematics. J Biomech 38:241–253
Doro LC, Hughes RE, Miller JD, Schultz KF, Hallstrom B, Urquhart AG (2008) The reproducibility of a kinematically-derived axis of the knee versus digitized anatomical landmarks using a knee navigation system. Open Biomed Eng J 2:52–56
Eckhoff D, Hogan C, Di Matteo L, Robinson M, Bach J (2007) Difference between the epicondylar and cylindrical axis of the knee. Clin Orthop Relat Res 461:238–244
Ehrig RM, Taylor WR, Duda GN, Heller MO (2007) A survey of formal methods for determining functional joint axes. J Biomech 40:2150–2157
Feng Y, Tsai TY, Li JS, Wang S, Hu H, Zhang C, Rubash HE, Li G (2015) Motion of the femoral condyles in flexion and extension during a continuous lunge. J Orthop Res 33(4):591–597
Grood ES, Suntay WJ (1983) A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng 105:136–144
Iacono F, Bruni D, Bignozzi S, Colle F, Marcacci M (2014) Does total knee arthroplasty modify flexion axis of the knee? Knee Surg Sports Traumatol Arthrosc 22(8):1728–1735
Ishida K, Shibanuma N, Matsumoto T, Sasaki H, Takayama K, Toda A, Kuroda R, Kurosaka M (2015) Factors affecting intraoperative kinematic patterns and flexion angles in navigated total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 23(6):1741–1747
Jenny J-Y, Boeri C (2004) Low reproducibility of the intra-operative measurement of the transepicondylar axis during total knee replacement. Acta Orthop Scand 75:74–77
MacWilliams BA (2008) A comparison of four functional methods to determine centers and axes of rotations. Gait Posture 28:673–679
Maderbacher G, Schaumburger J, Baier C, Zeman F, Springorum HR, Birkenbach AM, Grifka J, Keshmiri A (2015) Appropriate sagittal femoral component alignment cannot be ensured by intramedullary alignment rods. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-015-3541-8
Martelli S, Zaffagnini S, Bignozzi S, Bontempi M, Marcacci M (2006) Validation of a new protocol for computer-assisted evaluation of kinematics of double-bundle ACL reconstruction. Clin Biomech (Bristol Avon) 21:279–287
Martelli S, Zaffagnini S, Bignozzi S, Lopomo N, Marcacci M (2007) Description and validation of a navigation system for intra-operative evaluation of knee laxity. Comput Aided Surg 12(3):181–188
McGraw KO, Wong SP (1996) Forming inferences about some intraclass correlation coefficients. Psychol Methods 1:30–46
Mihalko WM, Ali M, Phillips MJ, Bayers-Thering M, Krackow KA (2008) Passive knee kinematics before and after total knee arthroplasty: are we correcting pathologic motion? J Arthroplasty 23:57–60
Moon YW, Seo JG, Lim SJ, Yang JH (2010) Variability in femoral component rotation reference axes measured during navigation-assisted total knee arthroplasty using gap technique. J Arthroplasty 25:238–243
Oussedik S, Scholes C, Ferguson D, Roe J, Parker D (2012) Is femoral component rotation in a TKA reliably guided by the functional flexion axis? Clin Orthop Relat Res 470(11):3227–3232
Reichl I, Leichtle U, Lorenz A (2014) Functionally computed flexion axis reduces kinematic interspecimen variation in in vitro experiments. Comput Methods Biomech Biomed Eng 17(Suppl 1):126–127
Siston RA, Patel JJ, Goodman SB, Delp SL, Giori NJ (2005) The variability of femoral rotational alignment in total knee arthroplasty. J Bone Joint Surg Am 87:2276–2280
Siston RA, Cromie MJ, Gold GE, Goodman SB, Delp SL, Maloney WJ, Giori NJ (2008) Averaging different alignment axes improves femoral rotational alignment in computer-navigated total knee arthroplasty. J Bone Joint Surg Am 90:2098–2104
Vanin N, Panzica M, Dikos G, Krettek C, Hankemeier S (2011) Rotational alignment in total knee arthroplasty: intraoperative inter- and intraobserver reliability of Whiteside’s line. Arch Orthop Trauma Surg 131:1477–1480
Victor J (2009) Rotational alignment of the distal femur: a literature review. Orthop Traumatol Surg Res 95:365–372
Wiles AD, Thompson DG, Frantz DD (2004) Accuracy assessment and interpretation for optical tracking systems. In: Proceedings of SPIE Medical Imaging 2004: visualization image-guided procedures, and display, vol 5367, pp 421–432
Wilson DA, Astephen Wilson JL, Richardson G, Dunbar MJ (2014) Changes in the functional flexion axis of the knee before and after total knee arthroplasty using a navigation system. J Arthroplasty 29(7):1388–1393
Woltring HJ, Huiskes R, de Lange A, Veldpaus FE (1985) Finite centroid and helical axis estimation from noisy landmark measurements in the study of human joint kinematics. J Biomech 18:379–389
Acknowledgments
This work was partially supported by the “5×1000” (2012) funding, provided by Istituto Ortopedico Rizzoli, Bologna (Italy). The authors would like to thank Mr. Emil J. “Systemystic” Ferretti for his contribution to the laboratory IT management and the precious Mrs. Silvia Bassini for the graphical support.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Colle, F., Bruni, D., Iacono, F. et al. Changes in the orientation of knee functional flexion axis during passive flexion and extension movements in navigated total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 24, 2461–2469 (2016). https://doi.org/10.1007/s00167-015-3816-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3816-0