
Abstract
Purpose
The aim of this paper was to determine whether the change in the position of the patient’s leg as well as the use of flexible reamers may help in obtaining a longer femoral tunnel with minimal risk of perforating the posterior cortex.
Methods
One hundred and twenty-five patients who had undergone anatomic ACL reconstruction between 2010 and 2013 were included in this prospective cohort study. The first group was composed of patients whose femoral tunnel had been drilled with rigid reamers, while the leg being operated on was positioned on an arthroscopic leg holder (82 patients). In the second group of patients, the femoral tunnel was also drilled with rigid reamers, but the leg was positioned on the table (25 patients), while the third group was composed of patients whose femoral tunnel was drilled with flexible reamers, and the leg was positioned on a leg holder (18 patients). The length of the femoral tunnel was measured intraoperationally, while the site of femoral insertion and the position of the tunnel were read from native radiographic images.
Results
When the femoral tunnel was drilled on the medial aspect of the lateral condyle, the centre of the tunnel was located at 31.4 % from the most proximal point of the femoral condyle and 34.7 % from the Blumensaat line. The length of the tunnel drilled with rigid reamers on the operating table (36.1 mm) was statistically significantly greater (p < 0.05) than the length of the tunnel drilled with the same reamers, but with the leg positioned on the leg holder (32.5 mm). The length of the tunnel drilled with flexible reamers with the leg positioned on the leg holder (42.5 mm) was highly statistically significantly greater than the length of the tunnel drilled with rigid reamers (p < 0.01), and it was statistically significantly greater than the length of the tunnel drilled with rigid reamers with the leg placed on the operating table (p < 0.05).
Conclusion
The drilling of the femoral tunnel during anatomic ACL reconstruction with the use of flexible reamers provides a longer femoral tunnel than when it is drilled with rigid reamers, without any danger of perforation of the posterior cortex.
Level of evidence
III.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
When drilling the femoral tunnel during anatomic reconstruction of the ACL, the surgeon is faced with at least two problems: adequate length of the tunnel and perforation of the posterior femoral cortex [9, 19]. These two issues are at the opposite ends of the lever called the selection of the femoral graft insertion site. The fixation of the graft on the femur where the tunnel is shorter than 25 mm cannot provide adequate incorporation of the graft into the bone [2, 7]. This length varies with different authors from 15 [18] to 30 mm [11]. When the use of suspensory devices is also added in as a factor, this length is increased by at least 15 mm (the length of the loop). Perforation of the posterior femoral cortex during tunnel drilling not only increases the duration of the procedure, but also prevents fixation and leads to a new, most frequently non-anatomic, position of the femoral graft fixation. This type of complication is not very frequent, but it does occur in a certain number of cases [9].
The proper femoral insertion site should be within the anatomic femoral footprint [15], and it should provide an adequate tunnel length and should not jeopardize the success of proximal graft fixation by causing damage to the posterior femoral cortex. Although the site of femoral anatomic ACL insertion has been the topic of many studies [3, 6, 8, 15, 17, 20], which have, in various ways, visually described the precise insertion site of the ACL and its bundles, this theoretical knowledge meets with numerous obstacles in practice, when the surgeon needs to choose, in the very confined space of the intercondylar notch, with 30° or 70° optics, the centre of graft insertion on the medial aspect of the lateral femoral condyle. This segment of a seemingly simple task decides the fate of the reconstruction and makes the difference between successful and poorly performed reconstructions.
In order to provide for an adequate tunnel length, many surgeons decrease the angle between the drill and the medial aspect of the lateral femoral condyle, but then they face the problem of possible posterior femoral cortex perforation, which is why they move the insertion site distally and anteriorly, thereby missing the area of the anatomic footprint on the femur. Such a position of femoral insertion can be seen on radiographic images of properly performed yet insufficient ACL reconstructions.
The aim of this paper is to determine whether the change in the position of the patient’s leg as well as the use of flexible reamers may help in obtaining a longer femoral tunnel with minimal risk of perforating the posterior cortex.
Materials and methods
This prospective cohort study included 125 patients of the Clinic for Orthopedic Surgery and Traumatology, of the Clinical Center of Serbia, who had undergone anatomicl ACL reconstruction between June 2010 and June 2013. The patients were divided into three groups. The first group was composed of patients who had the femoral tunnel drilled with rigid reamers with the leg positioned on an arthroscopic leg holder (82 patients). The femoral tunnel of the second group of patients was also drilled with rigid reamers, but their lower limb was positioned on the operating table (25 patients). The third group of patients was composed of subjects whose femoral tunnel was drilled with flexible reamers with the lower limb positioned on an arthroscopic leg holder (18 patients). Patients operated on in the period between June 2010 and June 2012 belonged to the first group, patients operated on in the period between June 2012 and December 2012 belonged to the second group, while those operated on in the period between December 2012 and June 2013 belonged to the third group. The average age of the patients did not significantly differ between the groups (ANOVA p = n.s.; Table 1).
Surgical technique
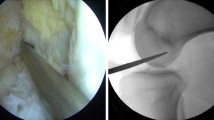
The reconstruction included direct arthroscopy whereby ACL lesion was verified. The leg being operated on was, in the first and second group of patients, placed on an arthroscopic leg holder, which enabled lower leg flexion from 110° to 115°. In the second group of patients, the leg was positioned on the operating table, which enabled 125°–130° flexion during the operation. After graft material was taken (STG or BPTB graft), the femoral graft insertion site was selected in all patients. After the medial aspect of the lateral condyle was cleared of the ruptured ACL remains, the surgeon, with the aid of the bifurcation ridge and the resident ridge, determined the centre of insertion, located at the point of meeting between the superior and the middle third of the height of the bifurcation ridge. In some cases, when the surgeon could not establish the aforementioned markers, a guide for establishing the centre of femoral insertion was employed (depending on the thickness of the graft), whose precise position the surgeon modified based on personal experience.
After that, in the first two patient groups (leg positioned on a leg holder and leg placed on the operating table), maximal flexion was performed and a canal was drilled through the anteromedial portal with a guide (2.5 mm). At the same time, the optics was located in the accessory medial portal positioned above and laterally to the medial portal, while the angle between the guide and the medial aspect of the lateral condyle was maximal (leaning on the medial femoral condyle). The canal was dilated with a rigid reamer of appropriate thickness (the thickness was graft dependent).
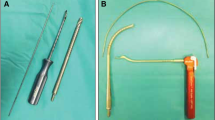
In the third group of patients, after the centre of insertion was determined, the guide for drilling the femoral tunnel was positioned, with the aid of an instrument for flexible guide placement, and the femoral tunnel was drilled with the leg flexed at an angle of around 100°–110° (Fig. 1). The tunnel was then dilated with the aid of flexible reamers to an appropriate width (dependent on the thickness of the graft). After tunnel dilation, arthroscopic testing of the tunnel walls integrity was performed.

Measuring the femoral tunnel length with the aid of the femoral tunnel length measurement device
Measurements
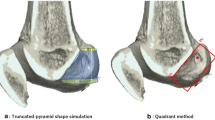
The length of the tunnel was measured directly, intraoperationally with the aid of the femoral tunnel length measurement device. Upon inserting the guide through the lateral femoral condyle, the marker on the guide was aligned with the medial aspect of the lateral condyle, which was controlled with the aid of an optic device. After that, the femoral tunnel length measurement device was positioned over the lateral end of the guide, reaching as far as the lateral aspect of the lateral femoral condyle, and the length of the tunnel was read (Fig. 1). The accuracy of tunnel measurement was 1 mm. The position of the femoral insertion of the graft was determined indirectly, on native radiographic images, with the aid of a net by Bernard et al. [3]. The centre of the tunnel on the medial aspect of the lateral condyle was determined on sagittal radiographic images after which a square was positioned on this segment. The anterior margin of this square was, in fact, the line of the roof of the intercondylar notch. The posterior margin lay parallel to the anterior one passing through the convexity of the condyle. The proximal margin was at a right angle to the previous two, passing through the most proximal point of the lateral condyle, while the distal margin lay parallel to the proximal margin, passing through the point of intersection between the anterior margin and the convexity of the condyle (Fig. 2). The distance between the first two margins was named the height of the condyle, while the distance between the second two margins was named the length of the condyle. The centre of the insertion is expressed as the percentage of the distance from the proximal margin in relation to the height (y-axis) and as the percentage of the distance from the roof of the intercondylar notch in relation to the length of the condyle (x-axis).

Grid method used to determine the insertion of the graft
The position of the femoral tunnel in the frontal and sagittal plane was measured indirectly, on frontal and sagittal radiographic images, as the angle between the line running along the middle of the tunnel and the distal femoral axis (Fig. 3). The distal femoral axis represents the line passing through the two central points of the diaphysis breadth, located at the distance of 10 and 20 cm from the tip of the medial femoral condyle. After the distal femoral axis was positioned on the X-ray image, a line was drawn through the central portion of the femoral tunnel. At the intersection of these two lines, the angle of the femoral tunnel in the sagittal and frontal planes was measured with the aid of a goniometer, with a one-degree accuracy.

Method of measuring the angle of the femoral tunnel in frontal (α) and sagittal (β) plane
This study was approved by the Ethical Committee of the Faculty of Medicine, University of Belgrade, ID number of approval: 29/3-14.
Statistical analysis
An a priori power analysis was performed to determine the sample size using the two-sided hypothesis test at an α level of 0.05. The calculations involving our sample size of 125 patients indicated the power of 0.60–0.99 to detect a significant difference in measurement outcomes in the present study. All data were processed with the aid of the SPSS 11.0 program. Differences between all three groups were tested by the one-way ANOVA test. Gender distribution in the groups was tested with the aid of the Chi-square test. The differences between the groups were tested with the Student’s t test for independent samples. The correlation was tested with the Pearson correlation coefficient. The statistical significance was set at 0.05.
Results
All three groups of patients had approximately the same site of insertion on the x-axis (proximally–distally) which did not show a statistically significant difference (n.s.); this also applies to the y-axis (n.s.; Fig. 4).

Visual image of the centre of the femoral tunnel on the medial aspect of the lateral femoral condyle
The length of the femoral tunnel (Table 2) drilled with a flexible reamer was statistically significantly greater than the length of the same tunnel drilled with a rigid reamer both with the leg positioned on the leg holder (p = 0.000; p < 0.01) and when it was positioned on the operating table (p = 0.012; p < 0.05). Also, the tunnel drilled on the operating table with the lower leg flexed at an angle of 125°–130° was statistically significantly longer (p = 0.017; p < 0.05) than the tunnel drilled on the leg holder with the lower leg flexed at an angle of 110°–115°.
The angle of the femoral tunnel in the frontal plane (Table 1) drilled with flexible reamers was highly statistically significantly smaller than the same tunnel drilled with rigid reamers, both with the leg placed on the leg holder and with the leg placed on the operating table (p = 0.000; p < 0.01 in both cases). The angle of the femoral tunnel in the frontal plane drilled on the operating table with the lower leg flexed at an angle of 125°–130° was statistically significantly greater (p = 0.033; p < 0.05) than the corresponding tunnel drilled on the leg holder with the lower leg flexed at an angle of 110°–115°.
The angle of the femoral tunnel in the sagittal plane did not statistically significantly differ between the three groups of patients (n.s.).
By monitoring the increase in the length of the tunnel in relation to the angle of the tunnel in the frontal and sagittal planes in all subjects, it is possible to establish a statistically significant indirect correlation between the length and the angle of the tunnel in the frontal (r = −0.295; p < 0.05; Fig. 5) but not in the sagittal plane (n.s.).

Correlation between the length of the femoral tunnel and the angle of the tunnel in the frontal plane
Discussion
The most significant contribution of this study to the anatomic reconstruction of the anterior cruciate ligament is reflected in the fact that with the assistance of flexible reamers, it is possible to increase the length of the femoral tunnel without excess flexion of the lower leg. Greater lengths of the femoral tunnel are achieved primarily due to the decrease in the tunnel angle in the frontal plane, which becomes more vertical, forming a more acute angle with the femoral diaphysis and possesses an outer opening above the lateral epicondyle, nearer to or on the very diaphysis of the femur. The length of the femoral tunnel obtained in this study is somewhat greater than the values for tunnel lengths published by Kim et al. [10] in their study on 80 patients, where they compared the transportal and outside-in techniques of femoral tunnel drilling.
Also, a moderately longer tunnel can be obtained by forced, maximal flexion of the lower leg which cannot be performed when the leg is positioned on the arthroscopic leg holder, but only when the leg is lying freely on the operating table. In this case, the outer opening of the tunnel remains in the domain of the epicondyle, and it does not significantly change the angle, either in the frontal or in the sagittal plane, while the increase in the length of the tunnel by around 4 mm can be attributed to a difference in the configuration of the lateral condyle and to the avoidance of the popliteal notch. However, such a procedure decreases the space in the knee joint due to the femoral condyle resting against the tibia, and as a result of the increase in the flexion angle, the reamer head may come in contact with the condylar cartilage and damage it.
The breadth of the lateral femoral condyle at the level of the popliteal notch amounts to 27 mm, and at the level of the lateral epicondyle, it is 33.5 mm [14]. These results, obtained by direct measurement on macerated thigh bones speak in favour of the fact that by drilling the femoral tunnel perpendicularly to the medial aspect of the lateral condyle, a length of the tunnel which is somewhat greater than the breadth of the condyle at the level of the popliteal notch can be achieved. Forced flexion of the lower leg (130° or more) enables the reamer to be positioned in the direction of the lateral epicondyle, thereby making the tunnels somewhat longer. The use of flexible reamers reduces the angle of the tunnel in the frontal plane; the tunnel extends along the lateral condyle and enters into the inferior segment of the femoral diaphysis, thereby becoming longer.
Just as there are differing opinions as to the minimal tunnel length necessary for successful incorporation of the graft into the bone, it is also difficult to determine how often tunnels are made to be too short. Tunnels shorter than 30 mm were present in 18.3 % of the cases in the first group and 8 % of the cases in the second group, while the third group registered no cases of tunnels shorter than 30 mm. However, practically speaking, none of the tunnels were, in fact, too short, as all the grafts incorporated successfully into the bone.
Similar data on the site of femoral graft insertion were published by Ahn et al. [1] in their study on 69 patients, 35 of whom had undergone anatomic ACL reconstruction. With the aid of 3D CT reconstruction, they established that the centre of femoral insertion was positioned at a distance from the most proximal point of the lateral condyle that amounted to 24.7 % of its length and 27.1 % of the intercondylar notch roof. Also, Colombet et al. [5] stated in their study that the centre of femoral graft insertion for single-bundle reconstruction was located at a distance that was 29 % from the most proximal point and 37.5 % from the roof of the intercondylar notch.
The results of the present study are supported by the study published by Lee et al. [8] which was carried out on 104 patients whose ACL reconstructions were performed with the application of two different techniques: the transtibial technique and through the anteromedial portal. The length of the femoral tunnel obtained with the use of the transtibial technique completely coincides with the femoral tunnel length of the group of patients in the present study, whose tunnel was drilled with flexible reamers. The length of the femoral tunnel obtained by drilling through the anteromedial portal is somewhat greater (34.4 mm) than the tunnel length of the group in the present study whose femoral tunnel was drilled in a similar fashion.
The results of the present study completely support the results published by Steiner et al. [12]. Their femoral tunnel drilled with flexible reamers (42 mm) was longer than the tunnel drilled with rigid reamers (32.5) with the lower leg flexed at 110°. In their study on 106 patients, whose femoral tunnels were drilled with rigid reamers through the anteromedial portal, Tompkins et al. [16] noted the length of the femoral tunnel of 37 mm with the knee flexed at 134°. This tunnel length does not significantly differ from the length of the tunnel found in the present study (36.5 mm), which was drilled with the lower leg flexed at 130°–135°.
In the present study, the angle of the femoral tunnel in the frontal plane in both of the groups where drilling was performed with rigid reamers was approximately equal to the angle published by other authors [4] who had also drilled with rigid reamers through the anteromedial portal (56.6°). However, the angle of the femoral tunnel drilled with flexible reamers in the present study (43°) significantly differs from the angle of the other tunnels. It can be noted that the direction of the tunnel is more perpendicular, so that it forms a more acute angle with the diaphysis of the femur and is closer to the angle of the native ACL in the frontal plane amounting to 76° [13]. Therefore, the graft itself is less angulated at the point of entry into the femur and has better biomechanical features.
For achieving the necessary hyperflexion of the knee, hip flexion of the leg being operated on is necessary. Application of standard leg holders without freeing the lower leg and elevating the leg from the leg holder does not make a satisfactory degree of hyperflexion possible. The position in which the patient is lying down on the operating table without a leg holder, provides for a greater length of the femoral tunnel and is, in fact, the recommended position for the application of the anteromedial portal and rigid reamers. The application of flexible reamers provides for an adequate length of the graft femoral tunnel without hyperflexion of the knee, thereby making the task of the surgeon significantly easier. Also, the application of flexible reamers reduces the significance of the choice of the patient’s position as to its influence on the graft femoral tunnel length.
Patients who had undergone primary ACL reconstruction with an STG or BPTB graft were included in the study. Patients with multiligament injuries were excluded from the study, as well as patients with osteal damage to the femur, tibia or patella. Sagittal radiographic images which were used for measurement had to be images of overlapping femoral condyles with a tolerance of up to 5 mm. Frontal radiographic images had to clearly and visibly show the medial and lateral femoral epicondyles. There was not a single perforation of the posterior femoral cortex in any of the subjects during femoral tunnel drilling.
Conclusion
The drilling of the femoral tunnel during anatomic ACL reconstruction with the use of flexible reamers provides a longer femoral tunnel than when it is drilled with rigid reamers, without any danger of perforation of the posterior cortex. In order to obtain an adequate length of the femoral tunnel for fixation with the aid of suspensory devices, it is not necessary to “push” the lower leg into excess flexion, rather adequate length can be achieved with the use of flexible reamers with a lesser degree of lower leg flexion.
References
Ahn JH, Jeong HJ, Ko CS, Ko TS, Kim JH (2014) Three-dimensional reconstruction computed tomography evaluation of tunnel location during single-bundle anterior cruciate ligament reconstruction: a comparison of transtibial and 2-incision tibial tunnel-independent techniques. Clin Orthop Surg 5:26–35
Bedi A, Raphael B, Maderazo A, Pavlov H, Williams RJ III (2010) Transtibial versus anteromedial portal drilling for anterior cruciate ligament reconstruction: a cadaveric study of femoral tunnel length and obliquity. Arthroscopy 26(3):342–350
Bernard M, Hertel P, Hornung H, Cierpinski T (1997) Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg 10(1):14–21
Chang MJ, Chang CB, Won HH, Je MS, Kim TK (2013) Anteromedial portal versus outside-in technique for creating femoral tunnels in anatomic anterior cruciate ligament reconstructions. Arthroscopy 29(9):1533–1539
Colombet P, Robinson J, Christel P, Franceschi JP, Djian P, Bellier G, Sbihi A (2006) Morphology of anterior cruciate ligament attachments for anatomic reconstruction: a cadaveric dissection and radiographic study. Arthroscopy 22(9):984–992
Ferretti M, Doca D, Ingham SM, Cohen M, Fu FH (2012) Bony and soft tissue landmarks of the ACL tibial insertion site: an anatomical study. Knee Surg Sports Traumatol Arthrosc 20(1):62–68
Golish SR, Baumfeld JA, Schoderbek RJ, Miller MD (2007) The effect of femoral tunnel starting position on tunnel length in anterior cruciate ligament reconstruction: a cadaveric study. Arthroscopy 23(11):1187–1192
Lee JK, Lee S, Seong SC, Lee MC (2014) Anatomic single-bundle ACL reconstruction is possible with use of the modified transtibial technique. J Bone Joint Surg Am 96:664–672
Kadija M, Bumbaširević M, Blagojević Z, Dubljanin-Raspopović E (2006) Posterior femoral cortex perforation unrecognised during arthroscopic LCA reconstructive surgery. Acta Chir Iugosl 53(4):73–78
Kim JG, Wang JH, Ahn JH, Kim HJ, Lim HC (2013) Comparasion of femoral tunnel length between transportal and retrograde reaming outside-in techniques in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 21:830–838
Moon DK, Yoon CH, Park JS, Kang BJ, Cho SH, Jo HS, Hwang SC (2014) Effect of anteromedial portal entrance drilling angle during anterior cruciate ligament reconstruction: a three-dimensional computer simulation. Yonsei Med J 55(6):1584–1591
Steiner ME, Smart LR (2012) Flexible instruments outperform rigid instruments to place anatomic anterior cruciate ligament femoral tunnels without hyperflexion. Arthroscopy 28(6):835–843
Stijak L, Radonjić V, Nikolić V, Blagojević Z, Herzog RF (2009) The position of anterior cruciate ligament in frontal and sagittal plane and its relation to the inner side of the lateral femoral condyle. Knee Surg Sports Traumatol Arthrosc 17(8):887–894
Stijak L, Radonjić V, Aksić M, Filipović B, Sladojević M, Santrac-Stijak G (2009) Correlation between femur’s length and morphometric parameters of distal femur important in rupture anterior cruciate ligament. Acta Chir Iugosl 56(2):61–66
Takahashi M, Matsubara T, Doi M, Suzuki D, Nagano A (2006) Anatomical study of the femoral and tibial insertions of the anterolateral and posteromedial bundles of human posterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 14(11):1055–1059
Tompkins M, Milewski MD, Carson EW, Brockmeier SF, Hamann JC, Hart JM, Miller MD (2013) Femoral tunnel length in primary anterior cruciate ligament reconstruction using an accessory medial portal. Arthroscopy 29(2):238–243
Tsukada H, Ishibashi Y, Tsuda E, Fukuda A, Toh S (2008) Anatomical analysis of the anterior cruciate ligament femoral and tibial footprints. J Orthop Sci 13(2):122–129
Yasuda K, Kondo E, Ichiyama H, Kitamura N, Tanabe Y, Tohya-ma H et al (2004) Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using ham-string tendon grafts. Arthroscopy 20:1015–1025
Yasuda K, van Eck CF, Hoshino Y, Fu FH, Tashman S (2011) Anatomic single- and double-bundle anterior cruciate ligament reconstruction, part 1: basic science. Am J Sports Med 39(8):1789–1799
Zauleck MK, Gabriel S, Fischmeister MF, Hirtler L (2014) Origin of the anterior cruciate ligament and the surrounding osseous landmarks of the femur. Clin Anat 27(7):1103–1110
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kadija, M., Milovanović, D., Bumbaširević, M. et al. Length of the femoral tunnel in anatomic ACL reconstruction: comparison of three techniques. Knee Surg Sports Traumatol Arthrosc 25, 1606–1612 (2017). https://doi.org/10.1007/s00167-015-3670-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3670-0