
Abstract
Purpose
To investigate the effect on hip-flexion strength of a 6-week hip-flexor training programme using elastic bands as resistance. We hypothesized that the training group, compared to a control group, would increase their hip-flexion strength more.
Methods
Thirty-three healthy subjects (45 % females), 24(5) years of age, were included in a randomized controlled trial and allocated to heavy strength training of the hip-flexor muscles or to control (no strength training). Strength training of the hip-flexors (dominant leg) was performed three times 10 min per week for 6 weeks. The strength training group progressed from 15 repetition maximum (RM) (week 1) to 8 RM (week 6). Isometric hip-flexion strength (primary outcome) was measured by a blinded assessor using a reliable test procedure.
Results
In the strength training group, the isometric hip-flexion strength of the trained leg increased by 17 %, (p < 0.001). The between-group difference in hip-flexion strength change in the trained leg (dominant leg, training group) versus the non-trained leg (dominant leg, control group) was significantly different from baseline to follow-up, corresponding to a mean change of 0.34 (95 % CI 0.17–0.52) Nm/kg, in favour of the strength training group (p < 0.001).
Conclusion
Simple hip-flexor strength training using elastic bands as external loading, for only 6 weeks, substantially improves hip-flexor muscle strength. This simple exercise programme seems promising for future prevention and treatment of acute and longstanding hip-flexor injuries, such as acute rectus femoris injuries and longstanding iliopsoas-related pain and impingement.
Level of evidence
I.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Specific ways of strengthening the hip-flexors in injury prevention or post-surgical rehabilitation have not previously been well described in the sports medicine literature. This is surprising, as both acute and overuse injuries of the hip-flexors are very common [10, 14] during sports and recreational activity, and a frequent source of longstanding pain in young-aged to middle-aged individuals [14].
Acute injuries to the rectus femoris are often experienced in kicking sports, such as in the different football codes, whereas longstanding iliopsoas-related pain is common in football players, runners and dancers [10, 14, 22, 27, 28, 38]. Furthermore, femoroacetabular impingement (FAI) is increasingly recognized as an important differential diagnosis in athletes with hip and groin pain [38], that if not settled by conservative treatment, may need surgical correction. In patients with FAI, substantial hip-flexor weakness, with decreased sagittal kinematics and range of motion both prior to and following FAI surgery have been documented [9]. Furthermore, recent evidence suggests that the iliopsoas tendon may cause impingement as it is placed in close proximity to the anterior capsule and labrum, just distal to the iliopectineal eminence [7, 26]. This condition can produce anterior hip pain that may mimic FAI symptoms or even coexist with FAI, as the iliopsoas makes an obtuse angle on the femoral head, resulting in possible compression and friction exerting on the femoral head and anterior labrum, around the three o’ clock hip joint position, during hip motion [7, 26]. Hence, simple ways of improving hip-flexor strength and function are needed in injury prevention and post-surgical rehabilitation.
Strength training including concentric, isometric and eccentric contractions has also proved to be an effective approach in prevention and treatment of acute and overuse muscle tendon injuries [24, 32, 34]. By introducing a hip-flexor strength training programme, where the only equipment needed is a strong elastic exercise band, the implementation of a strength training programme for injury prevention and/or post-operative rehabilitation in athletes with everything from acute hip-flexor injury, to more longstanding iliopsoas symptoms from overuse, or in combination with intra-articular hip joint-related problems, is expected to be much easier than compared to referring to conventional and much more impractical hip-flexor strength training machines. The clinical advantage of the elastic band is that it is portable and inexpensive, takes up very little space and can be used everywhere, indoor as well as outdoor, wherever solid attachment of the elastic band is possible.
The purpose of the present study was therefore to investigate the feasibility and effect of a novel simple hip-flexor strength training programme in healthy subjects, using elastic bands as external loading. We hypothesized that hip-flexion strength would increase more in the heavy strength training group (HST group) compared with the control group (CON).
Materials and methods
The present randomized controlled superiority trial with assessor blinding aimed to investigate the effect of a simple hip-flexor strength training programme in healthy subjects, using elastic bands as external loading. The participants were stratified for gender, and then randomly assigned to two parallel groups: hip-flexor training or control (Fig. 1), after the (baseline) pretesting, Table 1. The allocation process was blinded, and randomization was performed, by drawing lots in a one-to-one allocation ratio. The study followed CONsolidated Standards of Reporting Trials (CONSORT).

Flow chart of study profile
Subjects
Thirty-three healthy, physically active women (n = 15) and men (n = 18) gave their informed consent in accordance with the Declaration of Helsinki and participated in the study, which was conducted between October and December 2010. Included participants had to have been physically active prior to the initiation of the study for at least 2.5 h a week. They were excluded if they had performed systematic strength training of the hip-flexors more than once a week prior to the initiation of the study, if they had an injury and/or pain in the lower back, the hips and/or lower extremities within the last 6 months. Ethical approval was obtained from The Danish Ethics Committee of the Capital Region, and the Danish Data Protection Agency (ID: H-3-2010-062). The trial was registered at ClinicalTrials.gov (NCT01319175).
Training programme
All training sessions in the training group were performed at the Metropolitan University College, Copenhagen. A physiotherapist, who ensured that the exercises were performed correctly and according to the protocol, supervised all training sessions. The training leg for the participants was their dominant leg, defined as the preferred leg when kicking a ball. The hip-flexor exercise programme, constituting the training intervention, and its mechano-biological descriptors are documented below as suggested by Toigo and Boutellier [37]. Participants in the training group were instructed not to perform additional strength training of the hip-flexors during the study and to continue daily living and sporting activity as usual.
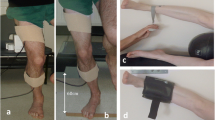
The exercise programme consisted of a single hip-flexor exercise performed in the standing position with an elastic band tied above the knee, 5 cm proximal to the patella of the training leg. The elastic band was tied to a fixed point, and the participant held on to a chair with both hands to increase body stability. During the training sessions, the supervising physiotherapist instructed the participants to reach full active range of motion in hip-flexion and extension (Fig. 2).

Hip-flexor exercise. Starting position, full active hip extension
The elastic bands (Thera-band©) used in the study were in various colours—gold, silver, black and blue—ranging from strongest type to weakest. Participants performed three training sessions of three sets per week for 6 weeks. The relative load was 15 repetition maximum (RM) during week 1, 10 RM during week 2–4 and 8 RM during week 5 and 6. The supervising physiotherapist monitored the intensity (relative load) during the exercise session. The number of repetitions had to be within ±2 repetitions of the prescribed relative load (intensity) and was adjusted one level up or down until the prescribed relative load was achieved. The physiotherapist, ensuring a 3-s concentric contraction, a 2-s isometric contraction, a 3-s eccentric contraction, a 2-s rest before the next repetition and a 2-min rest before the next set, supervised time under tension. Each training session lasted 10 min, including rest between sets.
Control group
Participants in the control group were instructed not to perform systematic strength training of the hip-flexors during the study, but otherwise to continue daily living and sporting activity as usual.
Outcome measures
The primary outcome was the change in maximal isomeric hip-flexion strength in the dominant leg from baseline to follow-up. The secondary outcome was the change in maximal isometric hip-flexion strength in the non-dominant leg. Isometric hip-flexion strength in 90° of hip-flexion in the sitting position was chosen as the only strength measurement, as this is a highly reliable hip-flexion strength test (ICC = 0.91, SEM % <5 %), with no systematic test–retest variation [35]. The measurements were taken 1 week pre- and 3–5 days post-intervention by an assessor blinded to group allocation and leg dominance, using a hand-held dynamometer (Powertrack II Commander, JTECH Medical, Salt Lake City, UT, USA). The participants were carefully instructed not to reveal to the assessor which group they were allocated to. The testing order of legs (dominant versus non-dominant) was randomized before testing by a third person. For the isometric hip-flexion strength test, four maximal trials separated by 30-s pauses were performed [35]. The highest value of the four trials was used for the statistical analysis. If the last trial elicited the highest value, an additional measurement was taken until no further increase was observed. Between testing of each leg, a 2-min break was introduced to avoid fatigue caused by the testing. Hip-flexion strength is expressed as maximal hip-flexion torque per kilo body weight (Nm/kg) using the external lever arm (from the anterior iliac spine to 5 cm proximal to patella, measured in the supine position) and the body weight of each participant, measured at pre- and post-intervention.
During all training sessions, delayed onset muscle soreness (DOMS) since the last training session was quantified using a numerical rating scale (NRS) measuring pain from 0 to 10, and perceived loading was quantified using the BorgCR10 scale [1].
Statistical analyses
A 15 % hip-flexion strength difference between groups was chosen as the minimal real difference (MIREDIF). It was considered a realistic strength increase after 6 weeks of strength training of a muscle group, which is rarely systematically strength trained. Based on pilot data, it was estimated that to achieve 80 % power with a significance level of 5 %, 12 participants were required for each group to be able to show a MIREDIF of 15 %.
If nothing else is stated, variability around mean values is presented as ±1 SD. The dependent variables showed a normal distribution (Shapiro–Wilk W test), and parametric statistics were applied. Paired and unpaired Student’s t tests were used to determine statistically significant (p < 0.05) within- or between-group differences, respectively. Intention-to-treat analysis was not performed, as we were interested in the potential efficacy of the strength training programme. Therefore, only participants who complied with the specific strength training programme and test setup exactly as planned and predefined were included in the analyses [13]. Specifically, only data from participants in the HST group with a compliance of at least 70 % were analysed. Furthermore, participants in both the HST group and the control group were excluded from the analysis, if they sustained an injury to their back, hip or groin, or any other situation causing periods of immobilisation during the study period, as previous research has shown that hip and groin pain/injury, and injury-related inactivity affects hip muscle strength [11, 36]. A person blinded to name and group allocation excluded participants from the analyses following the criteria mentioned above (Fig. 1).
Results
The total compliance for participants in the HST group was 17 (±1) sessions (94 % compliance). DOMS (Fig. 3a), and average perceived training load (Fig. 3b) during the strength training, was reported throughout the intervention period. No complications or adverse effects related to the strength training programme were reported during the intervention period.

a Delayed onset muscle soreness (DOMS) registered for the HST group. b Perceived loading registered for the HST group. RM repetition maximum
Effects of the hip-flexor strength training are visualized in Fig. 4. Six weeks of hip-flexor strength training using elastic bands as external loading increased isometric hip-flexion strength of the trained leg (dominant leg, training group), corresponding to a mean within-group change of 0.32 (95 % CI 0.19–0.45) Nm/kg (p < 0.001). There was no significant within-group change in isometric hip-flexion strength in the non-trained leg (dominant leg, control group), corresponding to a mean change of −0.02 (95 % CI−0.15 to 0.10) Nm/kg (n.s.)

Primary outcome. Within- and between-group differences for maximal isometric hip-flexion strength in the HST group (dominant leg, HST) and the control group (dominant leg, CON). * Statistically significant (p < 0.001) within-group difference. ** Statistically significant (p < 0.001) between-group difference
The between-group difference (primary outcome) of hip-flexion strength change in the trained leg (dominant leg, training group) versus the non-trained leg (dominant leg, control group) was significantly different from baseline to follow-up, corresponding to a mean change of 0.34 (95 % CI 0.17–0.52) Nm/kg, in favour of the HST group (p < 0.001).
No within-group changes in hip muscle strength occurred in the standing leg (non-dominant leg, training group), corresponding to a mean difference of 0.11 (CI 95 % −0.08 to 0.29) Nm/kg (n.s.), and in the non-trained leg (non-dominant leg, control group), corresponding to a mean difference of 0.03 (CI 95 % −0.09 to 0.16) (n.s.).
No between-group changes in hip muscle strength occurred in the standing leg (non-dominant leg, training group) versus the non-trained leg (non-dominant leg, control group), corresponding to a mean difference of 0.07 (CI 95 % −0.14 to 0.21) Nm/kg (n.s.).
Discussion
The most important finding of the present study was that the hip-flexor strength training programme using elastic bands as external loading effectively improved hip-flexor muscle strength by 17 % on average. The isometric hip-flexion strength increase was substantial and reached the hypothesized magnitude of at least 15 %, in only 6 weeks with three training sessions per week.
The hip-flexor strength training programme in the present study potentially involves all hip-flexors including sartorius, rectus femoris, tensor fascia lata and the iliopsoas muscle [5, 6, 15, 16, 39]. As the iliopsoas muscle has been shown to be most active during isometric contraction in 90° of hip-flexion, as opposed to lesser degrees of hip-flexion [21], it seems reasonable to assume that the strength capacity of the iliopsoas was certainly improved. This simple hip strengthening programme using an elastic band for resistance and by only including one exercise therefore seems ideal for prevention and rehabilitation of acute injuries to the rectus femoris are often experienced in kicking sports, such as in the different football codes, as well as longstanding iliopsoas-related pain which is commonly experienced in football players, runners and dancers [10, 14, 22, 27, 28, 38]. Athletes and patients with the increasingly recognized condition of iliopsoas impingement which is now considered an important differential diagnosis in athletes with hip and longstanding groin pain [9, 26] may also benefit from simple hip-flexor strengthening [30]. This approach can be performed addressing the substantial hip-flexor weakness and decreased sagital kinematics and range of movement that have been documented both prior and after FAI surgery [9]. In patients with a suspected antero-medially located labral injury and/or iliopsoas impingement, it is suggested not to perform the elastic band exercise in full range of motion when commencing the exercise programme, as this may cause increased compression of the labrum and iliopsoas tendon [7, 26]. However, exercise from 0° of hip-flexion/extension, instead of 10°–20° of hip extension, should still provide sufficient range and time under tension so that muscle strength gains similar to training in full range of motion can be achieved [37].
The present study supports recent studies showing that strength training using elastic bands may induce sufficient levels of muscle activity to induce a substantial strength gain and seems to be comparable to more traditional types of strength training, such as free weights or strength training machines [1, 18, 19, 31]. Moreover, the 17 % isometric strength improvement, which is almost similar to what has previously been shown from 12 weeks of progressive strength training (~20 % increase) of this load magnitude but with a bigger total exercise volume by Hubal et al. [17], was obtained in only 6 weeks of training. This is consistent with results of more recent studies on strengthening programmes, where only 4–6 weeks of strength training can improve muscle strength, including hip muscle strength, in the magnitude of 10–15 % [4, 20, 29, 33]. Future RCT studies are, however, needed to investigate the effect of this strength training programme in relation to prevention and treatment of hip/groin pathology, such as acute rectus femoris injuries and longstanding iliopsoas-related pain and impingement [10, 14, 22, 27, 28, 38], using elastic bands as external loading.
Hand-held dynamometry (HHD) has been shown to provide highly reliable hip strength measurements [35], whereas isokinetic hip strength testing seems more difficult to conduct in a reliable manner [8]. In the present study, hip-flexion strength gains were obtained in the training leg only. On the basis of the sample size (powered to be able to show a 15 % strength difference), a minor effect cannot be excluded to exist in the other leg (the standing leg). Theoretically, achieving an effect in the standing leg would be possible by different physiological pathways [23]. Firstly, a neural crossover effect can occur when training the contralateral side. However, this effect may be of such small magnitude that it is not possible to detect with the present sample size [23]. Secondly, it has been documented that some EMG activity on the contralateral side exists during active hip-flexion in the supine position, i.e. the standing leg is not completely passive [15, 16]. The iliopsoas muscle on the contralateral side is primarily working isometrically during the standing hip-flexor exercise, providing muscular stabilization of the hip, pelvic and lumbar region [2, 3, 5, 6], while hip-flexion occurs on the opposite side. These contralateral contractions may, however, not be of sufficient intensity to induce a substantial effect, such as a 15 % strength increase [15, 16, 21].
Evaluation of specific exercises and their likely effect on strength capacity is most often indicated by analyses of surface electromyograms (EMG), recorded during the execution of these specific exercises [1, 15, 16, 21, 25, 31]. However, actual strength gains over time will also depend on other training variables than the level of muscle activity, such as the total training volume and intensity [37]. Therefore, it is of great importance to conduct studies that investigate the effect of single exercises in a prospective design, such as the present study, before new strength training programmes are introduced as prevention or treatment in a clinical practice.
The hip-flexors are stressed in many different sporting activities requiring high-velocity hip-flexion such as sprint running, football and dancing [10, 22, 27, 28, 38], where great forces are transmitted via the trunk to the upper and/or lower extremities [3, 12]. At present, this novel hip-flexor strength training programme is therefore suggested as a simple approach for improving hip muscle strength and function in athletes, which may be particularly relevant in prevention or post-injury/surgical treatment of hip-flexor injuries such as acute injuries to the rectus femoris muscle and longstanding iliopsoas-related pain and/or impingement [10, 14, 22, 27, 28, 38].
Conclusion
Simple hip-flexor strength training using elastic bands as external loading, for only 6 weeks, improves hip-flexor muscle strength by an average of 17 %. This substantial strength gain is comparable to what is commonly achievable using strength training machines. Thus, this simple hip-flexor exercise seems a promising prevention and treatment approach for acute and longstanding hip-flexor injuries, such as acute rectus femoris injuries and longstanding iliopsoas-related pain and impingement.
References
Andersen LL, Andersen HC, Mortensen OS (2010) Muscle activation and perceived loading during rehabilitation exercises: comparison of dumbbells and elastic resistance. Phys Ther 90(4):538–549
Andersson E, Oddsson L, Grundström H, Thorstensson A (1995) The role of the psoas and iliacus muscles for stability and movement of the lumbar spine, pelvis and hip. Scand J Med Sci Sports 5(1):10–16
Andersson EA, Nilsson J, Thorstensson A (1997) Intramuscular EMG from the hip-flexor muscles during human locomotion. Acta Physiol Scand 161(3):361–370
Baroni BM, Rodrigues R, Franke RA (2013) Time course of neuromuscular adaptations to knee extensor eccentric training. Int J Sports Med. doi:10.1055/s-0032-1333263
Basmajian JV (1958) Electromyography of iliopsoas. Anat Rec 132(2):127–132
Bogduk N, Pearcy M, Hadfield G (1992) Anatomy and biomechanics of psoas major. Clini Biomech 7(2):109–119
Blankenbaker DG, Tuite MJ, Keene JS, del Rio AM (2012) Labral injuries due to iliopsoas impingement: can they be diagnosed on MR arthrography? AJR Am J Roentgenol 199(4):894–900
Claiborne TL, Timmons MK, Pincivero DM (2009) Test-retest reliability of cardinal plane isokinetic hip torque and EMG. J Electromyogr Kinesiol 19(5):345–352
Diamond LE, Dobson FL, Bennell KL, Wrigley TV, Hodges PW, Hinman RS (2014) Physical impairments and activity limitations in people with femoroacetabular impingement: a systematic review. Br J Sports Med. doi:10.1136/bjsports-2013-093340
Ekstrand J, Hägglund M, Waldén M (2011) Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med 39(6):1226–1232
Friel K, McLean N, Myers C, Caceres M (2006) Ipsilateral hip abductor weakness after inversion ankle sprain. J Athl Train 41(1):74–78
Hides JA, Fan T, Stanton WR (2010) Psoas and quadratuslumborum muscle asymmetry among elite Australian football league players. Br J Sports Med 44(8):563–567
Hollis S, Campbell F (1999) What is meant by intention to treat analysis? Survey of published randomized controlled trials. BMJ 319(7211):670–674
Hölmich P (2007) Long-standing groin pain in sportspeople falls into three primary patterns, a “clinical entity” approach: a prospective study of 207 patients. Br J Sports Med 41(4):247–252
Hu H, Meijer OG, van Dieën JH, Hodges PW, Bruijn SM, Strijers RL, Nanayakkara PW, van Royen BJ, Wu W, Xia C (2010) Muscle activity during the active straight leg raise (ASLR), and the effects of a pelvic belt on the ASLR and on treadmill walking. J Biomech 43(3):532–539
Hu H, Meijer OG, van Dieën JH, Hodges PW, Bruijn SM, Strijers RL, Nanayakkara PW, van Royen BJ, Wu WH, Xia C (2011) Is the psoas a hip flexor in the active straight leg raise? Eur Spine J 20(5):759–765
Hubal MJ, Gordish-Dressman H, Thompson PD, Price TB, Hoffman EP, Angelopoulos TJ, Gordon PM, Moyna NM, Pescatello LS, Visich PS, Zoeller RF, Seip RL, Clarkson PM (2005) Variability in muscle size and strength gain after unilateral resistance training. Med Sci Sports Exerc 37(6):964–972
Jakobsen MD, Sundstrup E, Andersen CH, Bandholm T, Thorborg K, Zebis MK, Andersen LL (2012) Muscle activity during knee-extension strengthening exercise performed with elastic tubing and isotonic resistance. Int J Sports Phys Ther 7:606–616
Jakobsen MD, Sundstrup E, Andersen CH, Aagaard P, Andersen LL (2013) Muscle activity during leg strengthening exercise using free weights and elastic resistance effects of ballistic vs. controlled contractions. Hum Mov Sci 32(1):65–78
Jensen J, Hölmich P, Bandholm T, Zebis MK, Andersen LL, Thorborg K (2014) Eccentric strengthening effect of hip-adductor training with elastic bands in soccer players: a randomized controlled trial. Br J Sports Med 48(4):332–338
Juker D, McGill S, Kropf P, Steffen T (1998) Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during a wide variety of tasks. Med Sci Sports Exerc 30(2):301–310
Khan K, Brown J, Way S, Vass N, Crichton K, Alexander R, Baxter A, Butler M, Wark J (1995) Overuse injuries in classical ballet. Sports Med 19(5):341–357
Lee M, Gandevia SC, Carroll TJ (2009) Unilateral strength training increases voluntary activation of the opposite untrained limb. Clinic Neurophysiol 120(4):802–808
Malliaras P, Barton CJ, Reeves ND, Langberg H (2013) Achilles and patellar tendinopathy loading programmes: a systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness. Sports Med 43(4):267–286
Nachemson A (1966) Electromyographic studies on the vertebral portion of the psoas muscle; with special reference to its stabilizing function of the lumbar spine. Acta Orthop Scand 37(2):177–190
Nelson IR, Keene JS (2014) Results of labral-level arthroscopic iliopsoas tenotomies for the treatment of labral impingement. Arthroscopy 30(6):688–694
Quirk R (1983) Ballet injuries: the Australian experience. Clin Sports Med 2(3):507–514
Reid DC (1988) Prevention of hip and knee injuries in ballet dancers. Sports Med 6(5):295–307
Snyder KR, Earl JE, O’Connor KM, Ebersole KT (2009) Resistance training is accompanied by increases in hip strength and changes in lower extremity biomechanics during running. Clin Biomech 24(1):26–34
Stalzer S, Wahoff M, Scanlan M (2006) Rehabilitation following hip arthroscopy. Clin Sports Med 25(2):337–357
Sundstrup E, Jakobsen MD, Andersen CH, Jay K, Andersen LL (2012) Swiss ball abdominal crunch with added elastic resistance is an effective alternative to training machines. Int J Sports Phys Ther 7(4):372–380
Thorborg K (2012) Why hamstring eccentrics are hamstring essentials. Br J Sports Med 46(7):463–465
Thorborg K, Bandholm T, Petersen J, Weeke KM, Weinold C, Andersen B, Serner A, Magnusson SP, Hölmich P (2010) Hip abduction strength training in the clinical setting: with or without external loading? Scand J Med Sci Sports 20(Suppl 2):70–77
Thorborg K, Hölmich P (2013) Advancing hip and groin injury management: from eminence to evidence. Br J Sports Med 47(10):602–652
Thorborg K, Petersen J, Magnusson SP, Hölmich P (2010) Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand J Med Sci Sports 20(3):493–501
Thorborg K, Serner A, Petersen J, Madsen TM, Magnusson P, Hölmich P (2011) Hip adduction and abduction strength profiles in elite soccer players: implications for clinical evaluation of hip adductor muscle recovery after injury. Am J Sports Med 39(1):121–126
Toigo M, Boutellier U (2006) New fundamental resistance exercise determinants of molecular and cellular muscle adaptations. Eur J Appl Physiol 97(6):643–663
Werner J, Hägglund M, Walden M, Ekstrand J (2009) UEFA injury study: a prospective study of hip and groin injuries in professional football over seven consecutive seasons. Br J Sports Med 43(13):1036–1040
Yoshio M, Murakami G, Sato T, Sato S, Noriyasa S (2002) The function of the psoas major muscle: passive kinetics and morphological studies using donated cadavers. J Orthop Sci 7(2):199–207
Acknowledgments
External funding was received from Danish Regions for the current study. Thanks to Birk Mygind Grønfeldt, Stig Midtiby and Silje Marie Midtun for assisting with subject recruitment, training intervention and data collection. Also, thanks to the School of Physiotherapy, Metropolitan University College, Copenhagen, for providing training and testing facilities.
Conflict of interest
There is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Thorborg, K., Bandholm, T., Zebis, M. et al. Large strengthening effect of a hip-flexor training programme: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc 24, 2346–2352 (2016). https://doi.org/10.1007/s00167-015-3583-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3583-y