
Abstract
Purpose
Anterior cruciate ligament (ACL) injuries in siblings are commonly observed in the clinic. One, possibly genetic, factor contributing to the pathogenesis of sibling injuries may be narrow intercondylar notches, which are well recognized as predisposing to ACL injury. This study aimed primarily to: (1) assess the incidence of ACL injuries in siblings within an existing study cohort, (2) compare intercondylar notch width size in injured compared to matched uninjured control siblings and (3) compare the number of injured versus control sibling pairs sharing a narrow notch.
Methods
Twenty-four ACL-injured siblings from 10 families were matched for age, gender, family composition and sports activity, with 24 uninjured siblings from another 10 families. Intercondylar radiographs were taken to calculate anterior and posterior notch width indices (NWI). Notch size and the number of narrow notches in sibling pairs were compared between groups.
Results
Thirteen of 72 ACL-study participants had siblings with torn ACLs. Mean anterior NWI was 0.18 and 0.24 (p < 0.001), and mean posterior NWI was 0.26 and 0.3 (p = 0.006) for injured and uninjured siblings, respectively. Sixty percent of injured sibling pairs shared a narrow notch, while no uninjured sibling pairs did so (p = 0.003).
Conclusion
This study showed that siblings (and often sibling pairs) with injuries do have significantly narrower notches than those without. This could partly explain the prevalence of ACL injuries in siblings. To reduce ACL-injury rates, we advise that siblings of ACL-injured athletes with narrow notches, be radiologically screened, and if necessary, cautioned and counselled regarding preventative training.
Level of evidence
Case–control study, Level III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
An anterior cruciate ligament (ACL) rupture incurs a heavy physical, emotional and financial burden on the athlete. The high prevalence and cost of this injury have prompted researchers to search for predictive factors and to identify at-risk populations for ACL injury, with the long-term goal of reducing the rate of injury. Many extrinsic [27] and intrinsic factors [12, 19, 20, 23] have been explored including femoral intercondylar notch width size [2, 10, 14, 29]. It is well established that a narrow intercondylar notch is a predisposing factor for ACL injury [3, 25, 26, 28, 36]. Athletes with a narrow notch are 26 times more likely to incur a non-contact ACL injury then those with a normal notch [28]. However, the incidence and extent of narrowing have not been investigated in family groups, who may be at risk, if a genetic underpinning exists.
Palmer in 1938 [29], first noted the pathologic relationship between the intercondylar notch and ACL injury. In 1987, Houseworth et al. [14] reported a significant difference in the posterior notch area in subjects with and without an ACL injury and concluded that a narrowed posterior notch predisposed to ACL injury. Using computerized tomography (CT), Anderson et al. [3] found anterior notch stenosis in ACL injured compared to control subjects. Souryal et al. [29] devised the notch width index (NWI) which measured radiographically the narrowest portion of the intercondylar notch as a ratio of the width of the femur, at the level of the popliteal groove. These researchers found a significantly narrowed notch in patients with bilateral injuries compared to those with unilateral injuries. More recent research [7, 13, 15, 32, 36] has confirmed the presence of narrow intercondylar notches in ACL-injured subjects, and several authors [6, 9, 22] have described the mechanism by which a narrow notch contributes to ACL injury.
Very few studies have addressed ACL injuries in families, and only one was found that investigated notch width size in one pair of siblings [12]. Earlier studies by Anderson et al. [3] and Souryal et al. [29] found no difference in family history between subjects with injured or healthy knees. In contrast, however, Harner et al. [10] found a significant difference in the incident rate of immediate family member having an ACL injury compared to a control group. In their study, Hewitt et al. [12] compared notch width size in two ACL-injured female fraternal twins with a larger group of female players from the same sport. They found that these siblings had a significantly smaller notch suggesting that there may be a congenital component at play.
Despite the frequent clinical reporting of ACL injuries occurring in siblings, to date no study was found that compared the notch width size in a cohort of ACL-injured siblings with a matched group of siblings with healthy knees. This knowledge would provide professionals with a guide for counselling ACL-injured athletes regarding radiographic prescreening for their uninjured siblings and participation in a preventative neuromuscular training programme if required. It is currently known that such training programmes [12, 20] minimize the risk of incurring this life-changing injury, which commonly leads to early osteoarthritis. Unknown is how we determine the high-risk population that could benefit from such programmes [12].
This study aimed to better understand the anatomic and possible genetic factors involved in ACL injuries. Firstly, this study aimed to determine the incidence of ACL injuries in siblings within an existing study cohort. Secondly, it aimed to determine the size of femoral notch width indices in siblings who have ruptured their ACL and in a matched control group of siblings with uninjured knees. Thirdly, it aimed to compare the number of injured versus control sibling pairs who shared a narrow notch. In addition, this study aimed to assess the notch width shape in injured compared to uninjured siblings. It was hypothesized that there would be a significant difference in the size of the NWI between injured and control subjects, that shared narrow notches would be more common in the injured compared to the control sibling pairs, and that there would be more injured than control siblings with a steep A-shaped intercondylar notch.
Materials and methods
Subjects for this study were selected from a cohort of 72 patients with unilateral ACL ruptures taking part in a clinical study. All patients had a unilateral rupture confirmed by an orthopaedic surgeon. They did not have any collateral or posterolateral instability or radiological osteoarthritis. A detailed history included a specific question regarding family members including parent, child or sibling with a confirmed diagnosis of an ACL rupture. Both ACL-deficient and ACL-reconstructed family members were included. Where study participants indicated that they had a sibling with an ACL rupture, the siblings were contacted and requested to attend a knee examination including a radiograph. The injured sibling groups were then matched for age, gender, sports activity and family composition with uninjured sibling controls. Control participants were required to have played at least one cutting sport and to have played sport three times a week or more for longer than 5 years. Control participants were recruited in response to notifications placed in local hockey, cricket, basketball and University sports clubs as well as from hospital staff, family and friends. All participants signed consent to take part in this study.
Radiographic assessment
The method used to view the intercondylar notch was that described by LaPrade et al. [17]. This method is considered to use the most reproducible radiographic parameters [17] although the Holmbach 70° view may be more accurate [2]. A posterior–anterior view was taken of each knee separately with the knee at 45° of flexion and the patient in prone kneeling. The perpendicular distance from the housing to the film was 1.12 m, and the femur was in neutral rotation. Attention was paid to all details regarding the precise angle, correct distance from beam and avoidance of femoral adduction or rotation. One of the authors (SLK) was present at each radiographic assessment to ensure the correct positioning of the patient and accuracy of the measures. Once taken, bilateral intercondylar radiographs for each sibling were stored, in a large radiograph envelope. Once all radiographs were completed, one of the authors (SLK) selected the radiograph of the uninjured knee from the envelopes of the injured siblings and randomly selected either the left or the right knee radiograph from the envelopes of the control siblings. The selected injured and control intercondylar radiographs were then organized in random order so that the assessor (RCK) was blind to the grouping of the siblings.
Notch measurement
In this current study, both the anterior and posterior notch width indices were calculated. In each case, the width of the notch measured at the level of the popliteal groove was divided by the width of the femoral condyles measured at the same level, to give the NWI as shown in Fig. 1. The notch width was measured precisely as described by Souryal et al. [29] using a translucent ruler, which has a precision of 0.1 cm. For each subject, the size of both anterior and posterior NWI was recorded. For anterior notches, a ratio of <0.2 was considered narrow, [29] and for posterior, a ratio of <0.24 was considered narrow. As stated the radiograph of the uninjured side was used to calculate the NWI since 17 of the injured siblings had undergone surgery, which had involved a notchplasty to increase the notch size in all bar three cases. The assessor also described the notches as round (inverted U), rounded A-shaped or steep A-shaped based on the description by Anderson et al. [3]. International review board approval for taking radiographs was granted by the Ethics Committee of The University of Queensland, Australia. Because the assessment involved radiography of healthy subjects, a report from a medical physicist was required.

Photograph showing the anterior and posterior femoral notches. The notch width index was calculated as the anterior (A) or the posterior (P) notch width distance divided by the femoral bicondylar width (C–C) measured at the level of the popliteal groove (B). The femoral bicondylar width is measured along a line parallel to the most inferior points of both condyles (D–D)
Statistical analysis
A power analysis under the parameters of an expected medium effect size difference between injured and matched control sibling pairs, α = 0.05, and power = 0.08 was conducted. Based on these parameters, a full sample size of 34 (that is 17 pairs in each group) would be required to maintain Type I error at 0.05.
In order to assess the incidence of ACL injuries in siblings, the number of ACL-injured patients, from the cohort of 72, who had indicated that they had a sibling with an ACL injury, was tallied and their sibling composition was recorded.
A mixed-model ANOVA was performed in order to uncover whether there were any significant differences in NWI size between the siblings with ACL injuries and those with healthy knees. Within-family pairing was considered the unit of analysis leading to a 2 (Sibling Pair) × 2 (group: injured vs. matched controls) mixed-model ANOVAs with sibling pair a within-subject factor and group as a between-subjects factor. The dependent variables were anterior and posterior NWI, which were analysed separately.
The number of sibling pairs with and without narrow notches was compared using Chi-squared analyses. These latter two analyses involved 10 sibling pairs from each family that is two of the siblings from each of the three sibling families.
Finally, the number of injured and uninjured siblings with round, rounded A-shaped or steep A-shaped notches was compared.
Results
It was revealed that 13 out of the 72 patients had a sibling with a ruptured ACL. The additional siblings who were contacted and were able to take part in the study totalled 24 siblings from 10 of the families. The details of recruitment and sibling configurations are shown in Fig. 2. In each of the injured sibling and control group, there were nine females and 15 males. The mean age was 27 (±5.4) years old for the injured siblings and 30.2 (±7.6) years old for the control siblings.

Recruitment and family demographic of the injured and uninjured siblings
Mixed-model ANOVAs revealed only significant effects for group main effect for both anterior NWI, p < 0.001, η 2 = 0.55, and posterior NWI, p = 0.006, η 2 = 0.36. The average anterior NWI in the injured sibling group was 0.18 (SD = 0.03) compared to 0.24 (SD = 0.02) in the control group. For the posterior NWI, the injured sibling group average was 0.26 (SD = 0.03) and in the control sibling group was 0.30 (SD = 0.02).
The total number of injured siblings considered to have a narrow or stenotic anterior NWI (<0.2) was 16 out of the 24 (66 %) compared to one out of 24 (4 %) in the control group. The number of injured siblings considered to have a narrow posterior NWI (<0.24) was eight out of the 24 (33 %) compared to 0 % in the control group. Not all injured siblings had a narrow notch (Table 1).
However, when comparing injured to uninjured sibling pairs, six of the injured sibling pairs presented with narrow notches compared to no uninjured sibling pairs. Conversely, narrow notches were not present in four injured sibling pairs and in all 10 uninjured sibling pairs. This finding of a difference in the number of sibling pairs with a narrow notch in the injured (6) compared to the uninjured (0) groups was statistically significant, p = 0.003 (Table 2).
In the injured group, 12 of 24 injured siblings the notch shapes were steep A shaped. In the control group, none of the notches were steep A-shaped (Table 3).
Discussion
The most important finding of this present study was that as hypothesized, the NWI of ACL-injured siblings was significantly narrower than that of uninjured siblings for both anterior (p < 0.001) and posterior notches (p = 0.006). In addition, there were significantly more sibling pairs sharing narrow notches in the injured compared to the control group (p = 0.003), and there were more injured than uninjured siblings with a steep A-shaped notch. Furthermore, this study was also able to confirm the observed frequency of ACL ruptures occurring in siblings, finding that 13 of a cohort of 72 or almost one in five of injured ACL patients have at least one sibling with an injured ACL. Narrow intercondylar notches have for decades been considered to be a risk factor for ACL rupture [3, 25, 28] and could explain the relatively high incidence of ACL injuries in families.
Although described frequently in ACL-injured patients, the presence of narrow intercondylar notches has, until now, not been investigated in sibling groups. The mean anterior NWI in ACL-injured siblings was 0.18, and in uninjured siblings was 0.24. This is similar to the findings by Le Prade et al. [17] and more recently Uhorchak et al. [32] who reported anterior NWI of 0.193 and 243 [17] and of 0.18 and 0.21 [32] in injured and uninjured athletes, respectively. Our finding of a significant difference in posterior NWI measuring 0.26 in injured and 0.3 in control siblings is similar to those reported by Chung et al. [5] who, (as illustrated in their photos), measured the posterior NWI to be 0.26 and 0.29 for injured and uninjured athletes.
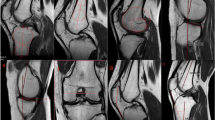
In addition, 12 out of the 24 injured siblings had a steep A-shaped notch, while none of the control siblings did. This compares similarly to studies by Al-Saeed et al. [1] and Anderson et al. [3]. The latter reported that 35 % of unilateral ACL-injuries patients had a steep ‘wave-shaped’ notch compared to 6 % of uninjured subjects. Figure 3 shows the intercondylar notches of the two injured identical male twins who demonstrate a narrowed and steep A-shaped notch. In contrast, Fig. 4 shows the much larger round notches of the uninjured sibling identical twins. Not all studies have reported A-shaped notches [15] or smaller notches in patients with ACL injuries [11, 18, 24, 31, 34]. Some authors believe other measures are more relevant than notch width index or notch shape as a predictive factor for ACL injury. These include width of the lateral femoral condyle [10], the posterior tibial slope of the lateral condyle [30], a small ACL [4], anteromedial ridging of the anterior notch [9] and notch width rather than notch width index [25]. However, Simon et al. [26] in an important recent MRI study found that the intercondylar notch width at the inlet was the best predictor of ACL injury, with a sensitivity of 74 % and a specificity of 67 % and a positive predictive value of 69 %.

Narrow notches in identical 15-year-old male twins who ruptured their ACLs 3 months apart. The anterior notches are clearly narrower than the posterior, which are less distinct in this example. The anterior notch width indices measure <0.2 in both cases. The shape of the anterior notches is steep A-shaped

Broader notches in uninjured identical female twins. The anterior notch is not clearly narrower than the posterior. The notch width indices measure >2. The shape of the notch is round and contrasts markedly to that of the injured twins
This study may have been limited by the use of radiology rather than MRI or CT [28]. Van Eck et al. [34] found no correlation between three radiographic views of the intercondylar notch and notch volume on CT scans and have suggested that radiographic views be interpreted with caution. Anderson et al. [2] have highlighted the difficulty in identifying the anterior outlet on planer radiography. Furthermore, there is no standardized method when using radiology. Either posterior–anterior (PA) [17, 25] or anterior–posterior (AP) [33, 35] views are used. Participants may be positioned in standing [25] or in prone kneeling [28, 29]. The angle of the knee may be positioned at 45° [17, 25], 60° [5], 70° [28, 29]. The distance from the camera to the knee may also vary. Although considered reliable [34] and reproducible [28], the accuracy of measurement using radiography has been questioned [2]. To ensure maximum possible accuracy of measurement, detailed attention was paid to the consistent and exact positioning of the patient avoiding adduction or rotation of the femur as this affects the view of the notch. A 45° knee flexion angle was measured using a goniometer and kept constant for each patient since Ireland et al. [15] have shown that a 10° difference in flexion alters the NWI. A PA view at 45° was selected as both the posterior and anterior notches are visible. Because of the uncertainty in the literature regarding the measurement of either anterior [12, 21, 25, 28, 29] or posterior [5, 13, 33, 35] notch outlets, we measured both, although, as mentioned, the anterior outlet can, at times, be difficult to define [2]. We found radiology to be a convenient and inexpensive means whereby valuable information with regard to notch size was provided. However, we acknowledge the possibility that the size of the anterior notch may have been narrower in the injured participants than assessed on radiograph. Out of eight, ACL-injured siblings who were measured as having normal size notches on radiograph, four required a notchplasties to broaden the notch during surgery, as the surgeon considered that the notches were narrowed.
Another limitation of this study includes the small sample size. The accuracy of ruler measures may be a further limitation. Ruler measures are considered to have a precision of 0.1 cm. Zooker et al. [37] found that measures of the width of the patellar tendon using a ruler were accurate to 1.2 mm in assessing surgical width. Measurement accuracy may have been increased by the use of digital calipers, which have a precision of 0.1 mm [32]. On the other hand, one of the strengths of this study was the blinding of the NWI assessor who assessed the contralateral knee of the injured siblings in order to avoid identification of the injured group from the surgical screws. Recent studies have shown that there is no side-to-side difference in notch width indices in cadaveric non-arthritic knees [8] or in ACL-deficient patients [5]. Teitz et al. [31] found no side-to-side difference in notch width size in ACL or uninjured subjects.
Recognizing at-risk groups is an essential part of preventing ACL injuries. This exploratory study has created awareness that siblings of ACL-injured subjects may be a high-risk population for ACL injuries, as a result of possibly genetic, narrow femoral intercondylar notches. This study suggests that in day-to-day practice professionals should educate and caution ACL-injured athletes known to have a stenotic intercondylar notch that their siblings may be at risk. It would be appropriate to recommend that notch width indices be assessed on radiograph as a screening tool prior to CT or MRI, to determine whether siblings should avoid vigorous cutting sports or undergo special training to reduce the chances of an ACL rupture [12, 20]. Some authors have even suggested prophylactic notchplasty be performed [29]. Identifying athletes at risk should lead to the long-term goal of reducing the rate of ACL injuries which have become a critical healthcare issue, very costly to the young athletic population in terms of pain, suffering, unfulfilled sporting potential and early osteoarthritis.
Conclusion
This study has highlighted the frequency of ACL injuries occurring in siblings. It has provided evidence that NWI are narrower in siblings with ACL injuries compared to control siblings and has shown that a narrow NWI is a significantly more frequently shared feature in siblings with ACL injuries than those without. This suggests that narrow notches may be a genetically predisposing factor contributing to ACL injuries in siblings. A steep A-shaped notch may also be a contributing factor to the pathogenesis of ACL injuries in siblings. However, not all sibling groups had narrow notches, and it appears that there may be other, possibly combined, predisposing factors contributing to ACL injuries in siblings.
References
Al-Saeed O, Brown M, Athyal R, Sheikh M (2013) Association of femoral intercondylar notch morphology, width index and the risk of anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 21:678–682
Anderson AF, Anderson CN, Gorman TM, Cross MB, Spindler KP (2007) Radiographic measurements of the intercondylar notch: are they accurate? Arthroscopy 23:261–268
Anderson AF, Lipscomb AB, Liudahl KJ, Addlestone RB (1987) Analysis of the intercondylar notch by computed tomography. Am J Sports Med 15:547–552
Chaudhari AM, Zelman EA, Flanigan DC, Kaeding CC, Nagaraja HN (2009) Anterior cruciate ligament-injured subjects have smaller anterior cruciate ligaments than matched controls: a magnetic resonance imaging study. Am J Sports Med 37:1282–1287
Chung SCY, Chan WL, Wong SH (2011) Lower limb alignment in anterior cruciate ligament-deficient versus–intact knees. J Orthop Surg Hong Kong 19:303–308
Davis TJ, Shelbourne KD, Klootwyk TE (1999) Correlation of the intercondylar notch width of the femur to the width of the anterior and posterior cruciate ligaments. Knee Surg Sports Traumatol Arthrosc 7:209–214
Domzalski M, Grzelak P, Gabos P (2010) Risk factors for anterior cruciate ligament injury in skeletally immature patients: analysis of intercondylar notch width using magnetic resonance imaging. Int Orthop 34:703–707
Everhart JS, Flanigan DC, Chaudhari AM (2014) Anteromedial ridging of the femoral intercondylar notch: an anatomic study of 170 archival skeletal specimens. Knee Surg Sports Traumatol Arthrosc 22:80–87
Everhart JS, Flanigan DC, Simon RA, Chaudhari AM (2010) Association of noncontact anterior cruciate ligament injury with presence and thickness of a bony ridge on the anteromedial aspect of the femoral intercondylar notch. Am J Sports Med 38:1667–1673
Harner CD, Paulos LE, Greenwald AE, Rosenberg TD, Cooley VC (1994) Detailed analysis of patients with bilateral anterior cruciate ligament injuries. Am J Sports Med 22:37–43
Herzog RJ, Silliman JF, Hutton K, Rodkey WG, Steadman JR (1994) Measurements of the intercondylar notch by plain film radiography and magnetic resonance imaging. Am J Sports Med 22:204–210
Hewett TE, Lynch TR, Myer GD, Ford KR, Gwin RC, Heidt RS (2010) Multiple risk factors related to familial predisposition to anterior cruciate ligament injury: fraternal twin sisters with ACL ruptures. Br J Sports Med 44:848–855
Hoteya K, Kato Y, Motojima S, Ingham SJ, Horaguchi T, Saito A, Tokuhashi Y (2011) Association between intercondylar notch narrowing and bilateral anterior cruciate ligament injuries in athletes. Arch Orthop Traumatol Surg 131:371–376
Houseworth SW, Mauro VJ, Mellon BA, Kieffer DA (1987) The intercondylar notch in acute tears of the anterior cruciate ligament: a computer graphics study. Am J Sports Med 15:221–224
Ireland ML, Ballantyne BT, Little K, McClay IS (2001) A radiographic analysis of the relationship between the size and shape of the intercondylar notch and anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 9:200–205
Keays SL, Bullock-Saxton J, Keays AC, Newcombe P, Bullock M (2007) A 6-year follow-up of the effect of graft site on strength, stability, range of motion, function, and joint degeneration after anterior cruciate ligament reconstruction: patellar tendon versus semitendinosus and gracilis tendon graft. Am J Sports Med 35:729–739
LaPrade RF, Burnett QM 2nd (1994) Femoral intercondylar notch stenosis and correlation to anterior cruciate ligament injuries. A prospective study. Am J Sports Med 22:198–202
Lombardo S, Sethi PM, Starkey C (2005) Intercondylar notch stenosis is not a risk factor for anterior cruciate ligament tears in professional male basketball players an 11-year. Prospective study. Am J Sports Med 33:29–34
Loudon JK, Jenkins W, Loudon KL (1996) The relationship between static posture and ACL injury in female athletes. J Orthop Sports Phys Ther 24:91–97
Myer GD, Ford KR, Paterno MV, Nick TG, Hewett TE (2008) The effects of generalized joint laxity on risk of anterior cruciate ligament injury in young female athletes. Am J Sports Med 36:1073–1080
Mohamed EE, Useh U, Mtshali BF (2012) Q-angle, pelvic width, and intercondylar notch width as predictors of knee injuries in women soccer players in South Africa. Afr Health Sci 12:174–180
Norwood L, Cross M (1977) The intercondylar shelf and the anterior cruciate Ligament. Am J Sports Med 5:171–176
Ramesh R, Von Arx O, Azzopardi T, Schranz PJ (2005) The risk of anterior cruciate ligament rupture with generalised joint laxity. J Bone Jt Surg Br 87:800–803
Schickendantz MS, Weiker GG (1993) The predictive value of radiographs in the evaluation of unilateral and bilateral anterior cruciate ligament injuries. Am J Sports Med 21:110–113
Shelbourne KD, Davis TJ, Klootwyk TE (1998) The relationship between intercondylar notch width of the femur and the incidence of anterior cruciate ligament tears. A prospective study. Am J Sports Med 26:402–408
Simon RA, Everhart JS, Nagaraja HN, Chaudhari AM (2010) A case-control study of anterior cruciate ligament volume, tibial plateau slopes and intercondylar notch dimensions in ACL-injured knees. J Biomech 43:1702–1707
Smith HC, Vacek P, Johnson RJ, Slauterbeck JR, Hashemi J, Shultz S, Beynnon BD (2012) Risk factors for anterior cruciate ligament injury a review of the literature—Part 1: neuromuscular and anatomic risk. Sports health: a multidisciplinary approach. Sports Health 4:69–78
Souryal TO, Freeman TR (1993) Intercondylar notch size and anterior cruciate ligament injuries in athletes. A prospective study. Am J Sports Med 21:535–539
Souryal TO, Moore HA, Evans JP (1988) Bilaterality in anterior cruciate ligament injuries: associated intercondylar notch stenosis. Am J Sports Med 16:449–454
Stijak L, Herzog RF, Schai P (2008) Is there an influence of the tibial slope of the lateral condyle on the ACL lesion? A case-control study. Knee Surg Sports Traumatol Arthrosc 16:112–117
Teitz CC, Lind BK, Sacks BM (1997) Symmetry of the femoral notch width index. Am J Sports Med 25:687–690
Uhorchak JM, Scoville CR, Williams GN, Arciero RA, Pierre PS, Taylor DC (2003) Risk factors associated with noncontact injury of the anterior cruciate ligament a prospective four-year evaluation of 859 west point cadets. Am J Sports Med 31:831–842
Van Eck CF, Kopf S, van Dijk CN, Fu FH, Tashman S (2011) Comparison of 3-dimensional notch volume between subjects with and subjects without anterior cruciate ligament rupture. Arthroscopy 27:1235–1241
van Eck CF, Martins CA, Lorenz SG, Fu FH, Smolinski P (2010) Assessment of correlation between knee notch width index and the three-dimensional notch volume. Knee Surg Sports Traumatol Arthrosc 18:1239–1244
Vyas S, Van Eck CF, Vyas N, Fu FH, Otsuka NY (2011) Increased medial tibial slope in teenage pediatric population with open physes and anterior cruciate ligament injuries. Knee Surg Sports Traumatol Arthrosc 19:372–377
Zeng C, Gao SG, Wei J, Yang TB, Cheng L, Luo W, Lei GH (2013) The influence of the intercondylar notch dimensions on injury of the anterior cruciate ligament: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 21:804–815
Zooker C, Pandarinath R, Kraeutler MJ, Ciccotti MG, Cohen SB, DeLuca RF (2013) Clinical measurement of patellar tendon: accuracy and relationship to surgical tendon dimensions. Am J Orthop 42:317–320
Acknowledgments
The authors would like to thank the Private Practitioners fund at the Nambour General Hospital, Nambour, Queensland, Australia, for funding the radiographs. Thank you also to David Ward, Christopher Bates and Dr Nigel Sommerfeld.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Keays, S.L., Keays, R. & Newcombe, P.A. Femoral intercondylar notch width size: a comparison between siblings with and without anterior cruciate ligament injuries. Knee Surg Sports Traumatol Arthrosc 24, 672–679 (2016). https://doi.org/10.1007/s00167-014-3491-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-014-3491-6