
Abstract
This study examines the effect of the tibial slope on the anterior cruciate ligament lesion (separately on the lateral and medial tibial condyle). The study consisted of 33 matched pairs of patients divided into two groups: an examined group with a diagnosed ACL lesion, and a control group with diagnosed patellofemoral pain. The patients were matched on the basis of four attributes: age, sex, type of lesion (whether it was profession-related), and whether the lesion was left- or right-sided. Measurements were carried out by radiography and MRI. In the examined group, the lateral tibial plateau was significantly greater than in the control group (P < 0.001), and the medial tibial plateau had lower tibial slope values than the control group; however, the difference was not statistically significant (P = 0.066). In both groups, the difference between the slopes on the lateral and medial plateaus was statistically significant (P < 0.001). In relation to ACL intact patients, population with ACL rupture have greater tibial slope of the lateral condyle. The greater tibial slope of the lateral tibial plateau may be the factor that leads to the injury of the anterior cruciate ligament. Compared to the medial plateau, the population with ACL rupture have a greater tibial slope on the lateral plateau, while the population of the intact ACL have greater tibial slope on the medial plateau. The tibial slope of the medial and lateral condyle should be compared separately because the values obtained from the two sets of data were different, revealing apparently opposing effects on the ACL lesion.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Many factors can bring about an anterior cruciate ligament (ACL) lesion. After the Hunt Valley Consensus Conference, held in Maryland in 1999, an information sheet identifying a number of factors that can assist in defining the appearance of non-contact lesions of the ACL was published [3, 14, 15]. Apart from the intercondylar notch, the tibial slope is one of the most often stated anatomic structures that may cause ACL injury [2]. Although, in many studies, this factor has been presented as an important one, results often do not provide direct effect of the tibial slope on the ACL lesion [11, 15, 23].
The tibial slope is defined as the angle between the line perpendicular to the tibial axis and the posterior inclination of the tibial plateau. Giffin et al. [13] reported that a small increase in the tibial slope did not influence the anterior tibial translation and that it assumed a protective role in ACL deficiency. Dejour et al. [12], in a study covering 281 knees, established a significant correlation between the tibial slope and the anterior tibial translation during standing in both cases, normal and cases with ACL-deficient knees. A large tibial slope can lead to a larger anterior tibial translation via stress to the knee joint and consequently induce stretching and rupture of the anterior cruciate ligament.
Dejour and Bonnin [11] compared the monopodal stance test with Lachman’s radiological test. They showed that a 10° increase in the tibial slope was combined with increases in the anterior tibial translation by 6 and 3 mm, as judged by the monopodal stance test and Lachman’s radiological test, respectively. In contrast, Meister et al. [23] did not establish statistically significant differences in tibial slopes in their control case study (50 patients with ACL-deficient knees and 50 patients with patellofemoral pain).
In their study of weight-bearing in the knee, Bonin et al. [4] examined the anterior tibial translation after an ACL rupture. They showed that the anterior tibial translation increased significantly after an ACL rupture, in particular in the position of flexion (60°) when hamstring muscles cannot compensate for the rupture.
In their study of knee kinematics, Mahfouz et al. [21] showed that the anterior tibial translation was much larger on the lateral than on the medial condyle in the normal knee in 120° flexion. During complete flexion, the medial femoral condyle touches the medial tibial plateau at approximately the same point while the lateral femoral condyle slowly moves in the posterior direction. Thus, during flexion, the lower leg makes one more motion that describes an internal rotation.
In their examination of tensions of different parts of the ACL, Branthigan and Woshel [6] showed that the antero-medial (AM) part was stretched by flexion and the postero-lateral (PL) by extension. They suggested that the ACL served as the main knee stabilizer in tibiofemoral translation, with specific tension being produced in the course of internal rotation [1, 17], which partly explained the lesion mechanism. When an anterior force is applied to the tibia of the knee with intact ligaments, the internal rotation that occurs [20] imparts considerable stress on the ACL.
One of the most frequent mechanisms of non-contact ACL lesions is hyperextension with internal rotation. Physiological internal rotation is possible during flexion of the knee joint. Tibial slope on lateral tibial plateau undertakes an important role during extension motion because it favors internal rotation, which, in turn, imparts considerable stress on the extended ACL.
In this paper, we have tried to establish the fact whether the patients with ACL rupture have greater tibial slope to the lateral and minor tibial slope to the medial condyle, compared to the ACL intact patients.
Patients and methods
A large group from the Kantonal Hospital in the Sursee–Wolhusen region was followed from 1 September 2001 to 1 September 2006. The patients were accepted for knee interventions; none were diagnosed with gonarthrosis. Two groups of patients were established. The examined group consisted of 205 patients with isolated ruptures of the ACL, and with no reported lesions of collateral ligaments, posterior cruciate ligaments or other bone elements. The control group consisted of 258 patients whose major complaint was patellofemoral pain. After matching 33 pairs from the two groups, a total of 66 patients were considered. The patients were matched by their age at the time of the accident (a difference of up to 5 years was tolerated), sex, type of lesion (whether it was profession-related), and whether the lesion affected the left or right side of the knee. There were 21 male and 12 female pairs, 9 pairs of soccer-, 4 pairs of ski-, 3 pairs of gymnastics-, and 16 pairs of patients with other sports-related lesions as well as one involved in a motorbike accident. Twenty pairs had the lesion on their right knee and 13 pairs on the left knee. The average age of the patients was 29.88 ± 9.78 years (from 15 to 48 years of age) in the examined group, and 30.06 ± 11.06 years (from15 to 48 years of age) in the control group. Measurements were done by radiography and MRI.
In order to establish the tibial slope, we used the proximal tibial anatomic axis (PTAA), which demonstrates the best correlation with the tibial shaft anatomic axis (TSAA) [7, 10].
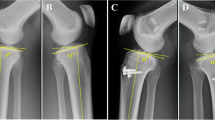
Using lateral X-rays, the PTAA was examined with the help of two medial points (midpoints between anterior and posterior tibial cortex) defined by 5 and 15 cm distances below the tibial tuberosity. The next plotted line followed the slope of the anterior intercondylar area. The angle between these two lines was defined as the “angle of the anterior tibial plateau.” The value of the said angle was used as the reference in establishing PTAA on the MRIs. (Fig. 1).

Determination of the tibial slope. The angle of the anterior tibial slope (α) was established on the X-ray using the TPAA and a line projecting from the anterior tibial plateau (line a). By transferring “α” to the line that follows the anterior tibial plateau on the sagittal MRI (line a), a line running parallel to the TPAA was obtained (line b). The obtained line was transferred to the sagittal MRI section of the medial (M) and lateral (L) tibial condyle. Using a line perpendicular to the tibial axis and a line running along the tibial slope of the medial (line c) and lateral (line d) condyle, the angle of the tibial slope (β and γ) on the tibial condyle was obtained

Distribution of values of the tibial slope on the lateral tibial plateau in the examined and control group
All MRIs were made using 1.5 T magnets. All measurements were performed at three sagittal sections of the knee joint. The first sagittal section was through the middle of the anterior tibial plateau at a point equidistant from both the intercondylar tubercles. The other two sections, which measured the medial and lateral tibial plateaus, were at the point of the shortest femorotibial distance on the medial and lateral plateaus.
On the MRI, at the sagittal plane between the two intercondylar tubercles, a line traversing the anterior tibial plateau was drawn. The value of the angle of the anterior tibial plateau (α––measurement obtained by X-rays) was used to obtain a line parallel with the TPAA. Four angle points were marked using tracing foil to assist correct transfer. A line parallel to the TPAA was transferred on the MRI section of the medial and lateral tibial plateau.
The angle of the tibial slope on the medial and lateral tibial condyle was measured between two lines, one of the tibial slope (on the medial and lateral condyle) and the other perpendicular to the line parallel to the TPAA.
The data was analyzed with the SPSS 11.0 programme. The differences between the two groups were tested using the Student’s t test for linked pairs. The two groups were tested for the following differences:
-
The difference between the tibial slope on the lateral tibial plateau
-
The difference between the tibial slope on the medial tibial plateau
-
The difference between the average tibial slopes
-
The difference between the tibial slope on medial and lateral tibial plateau in each group, and
-
The difference between the differences of the tibial slope on the lateral and medial plateau in the two groups.
All differences were sex-matched. The significance level was set at 5% (P < 0.05).
Results
Comparison of the tibial slope on lateral tibial plateau in both the groups led us to conclude that the difference was significant (P < 0.01; Table 1.). The tibial slope on the medial tibial plateau in the two groups was not significant (P > 0.05, P = 0.066).
The average tibial slope on lateral tibial plateau in the examined group was 7.52° (from 0 to 13°; Fig.2), and the medial was slightly lower at 5.24° (from −1 to 12°). The value of the tibial slope on lateral tibial plateau in the control group was 4.36° (from −2 to 9°), whereas the tibial slope on the medial tibial plateau had a value of 6.58° (from 0 to 13°).
During examination of the differences between the tibial slope on the lateral and medial tibial plateaus, a statistically significant difference (P < 0.01) between the two groups was observed. A larger slope on the lateral tibial condyle than on the medial (2.28°) was observed in the examined group compared to the control group where the slope on the medial condyle was larger than on the lateral one (2.22°).
In both groups, the differences between the tibial plateau slopes on both lateral and medial condyles were tested. The lateral and medial tibial plateaus of the same group had significantly different values (P < 0.01 in both groups).
Although the mean of the tibial slope in the examined group was slightly higher than in the control group, there was no statistically significant difference (P > 0.05) between the examined and control groups (we tested the arithmetic mean of the tibial slope on the medial and lateral plateau––the whole tibial slope).
When the groups were split according to sex, similar results were obtained. The data are presented in Table 2. The largest tibial slope was observed on the lateral tibial plateau in females from the examined group (9.00 ± 3.25°). The smallest slope was observed on the lateral plateau in males from the control group (4.00 ± 2.56°).
Discussion
The problem inherent to the measurement of the tibial slope on the short sagittal MRI sections of the knee is the impossibility to adequately determine the proximal tibial anatomic axis (PTAA). To determine the PTAA, a section covering a minimum of 150 mm below the joint gap of the knee is necessary [7, 10]. Kuwano et al. [19] determined the posterior tibial slope on the medial and lateral condyles by means of a 3D CT scanner, with an image capturing 150 mm of the proximal end of the tibia. We had no MR images with the adequate proximal tibia length at our disposal. We tried to offset this shortcoming by determining the proximal tibial anatomic axis and the angle of the anterior tibial slope by means of sagittal X-rays. Using the angle of the “anterior tibial slope” obtained by means of X-rays and the line following the anterior tibial slope on the sagittal images, a line parallel to the PTAA was defined.
Dejour and Bonnin [11] established that the anterior tibial translation was bigger on the lateral than on the medial tibial compartment in both normal and deficient knees. Bull et al. [8] showed that in the ACL-deficient knees, tibial subluxation and internal rotation at the very beginning of flexion occurred primarily as a result of excessive anterior motion of the lateral tibial plateau. In our study, the tibial slope on the lateral plateau had a significantly higher value in the examined group than in the control group. The anterior tibial translation during flexion was greater on the lateral tibial plateau [8, 11, 21]. We believe that this can explain why the additional increase in the tibial slope imparted stress on the ACL that could result in its rupture. A similar, statistically significant, sex-linked difference was observed in the two groups.
Matsuda et al. [22], in their study on MRIs, quote slightly higher values of the tibial slope for normal (lateral 7.2°; medial 10.7°) as well as for the varus knees (lateral 6.0°; medial 9.9°), what is probably the consequence of using a different way of determining the tibial anatomic axis as a starting point. But the above-mentioned study, as well as our control group (both cases of the ACL intact patients), registers higher values of the tibial slope on the medial than to the lateral tibial plateau.
Chiu et al. [9] used the line of the anterior tibial cortex in determining the tibial slope on the previously photographed tibias and obtained the value of 14.8° for medial and 11.8° for lateral plateau. This study, as well as ours, is in favor of greater tibial slope on medial than on the lateral plateau, with the ACL intact patients. On the other hand, the reasons of extremely high values of the tibial slope on both medial and lateral plateau together, are multiple. One of the reasons is in using the line of the anterior tibial cortex as an axis in taking measurements (we used PTAA). The other reason refers to the authors’ statement that aging brings an increase in the tibial slope plateau. In that context, our population of the tested group was younger, 30 years of age on an average, while at the Chiu study the average age of the tested population was 68. The third reason may consider the difference between the two populations: Chinese and European.
Giffin et al. [13] in their study performed on ten cadaverous knees estimated a slightly higher value of the tibial slope at 8.8 ± 1.8°. In distinction from our study, this measurment was based on the X-rays only, with the examined material belonging to the older population (60–78 years of age), and without examining the separate values of the tibial slope on medial and lateral plateau.
The higher values of the tibial slope on the medial condyle in the control group suggested that the larger tibial slope of the medial condyle could be protective. However, we did not observe a statistically significant difference between the examined and control groups, although the test result had a borderline value (P = 0.066). A hypothetical increase by one value (in one case by 2°) in the tibial slope on the medial tibial plateau in the control group was statistically significant. To determine the effect of the medial tibial plateau on an ACL lesion, further studies using state-of-the-art equipment and including more patients are necessary.
Neither the examined nor the control groups revealed any statistically significant differences when the whole tibial slope was considered (the arithmetic mean of the medial and lateral tibial slopes), although the examined group displayed a slightly larger tibial slope. Meister et al. [23], in their age-matched study, did not observe a statistically significant difference either. They found a slightly greater tibial slope in the control group than in the examined group, as well as one that was probably the consequence of considering only one attribute (age) in patient matching, whereas we considered four (age, sex, type of lesion (whether it was profession-related), and whether the lesion was left- or right-sided).
Dejour et al. [12] measured the minimum and maximum tibial slopes of 0 and 19°, respectively. In our study, the minimum tibial slope of −2° was measured in the lateral condyle of the control group, whereas the maximum slope in the lateral condyle in the examined group was 13°.
Brandon et al. [5], in their study of the relationship between the tibial slope and ACL insufficiency and in a comparison of the Pivot-shift level, discovered a statistically significant difference between the tibial slope in ACL insufficiency and the control (in both males and females). Contrary to our study, this study is done only on the X-rays. In this study, the knee lesion factor was also not observed.
Different relationships between the tibial slope and ACL lesions have been reported in different studies [9, 13, 16, 18, 22]. We found that the tibial slopes on the lateral and medial tibial plateau were significantly different (P < 0.01) in both the examined and control groups. The arithmetical means in both groups should not be compared.
When only differences between the lateral and medial condyles in the examined group were compared with same differences in the control group, a significant difference (P < 0.01) was arrived at. This finding confirmed the effect of the tibial slope on the lateral tibial plateau in an ACL lesion.
Conclusion
Comparing the tibial slope of the 33 matched pairs, we may say that in relation to the ACL intact patients, the population with ACL rupture has the greater tibial slope on the lateral condyle. The increased tibial slope of the lateral tibial plateau may be the factor which causes the injury of the anterior cruciate ligament. The population with ACL rupture has got a greater tibial slope on the lateral plateau in comparison to the medial one, while the population with the ACL intact has the greater tibial slope on the medial plateau. The tibial slope of the medial and lateral condyle should be compared separately because the values obtained from the two sets of data were different, revealing apparently opposing effects on the ACL lesion.
References
Amis AA, Dawkins GP (1991) Functional anatomy of the anterior cruciate ligament. Fibre bundle actions related to ligament replacements and injuries. J Bone Joint Surg Br 73(2):260–267
Arendt EA (2001) Anterior cruciate ligament injuries. Curr Womens Health Rep 1(3):211–217
Boden BP, Dean GS, Feagin JA Jr, Garrett WE Jr (2000) Mechanisms of anterior cruciate ligament injury. Orthopedics 23(6):573–578
Bonnin M, Carret JP, Dimnet J, Dejour H (1996) The weight-bearing knee after anterior cruciate ligament rupture. An in vitro biomechanical study. Knee Surg Sports Traumatol Arthrosc 3(4):245–251
Brandon ML, Haynes PT, Bonamo JR, Flynn MI, Barrett GR, Sherman MF (2006) The association between posterior-inferior tibial slope and anterior cruciate ligament insufficiency. Arthroscopy 22(8):894–899
Branthingan OC, Woshel AF (1941) The mechanics of the ligaments and menisci of the knee joint. J Bone Joint Surg 23:44–46
Brazier J, Miguad H, Gougeon F, Cotten A, Fontaine C, Duquennoy A (1996) Evaluation of methods for radiographic measurement of the tibial slope. A study of 83 healthy knees. Rev Chir Orthop Reparatrice Appar Mot 82(3):195–200
Bull AMJ, Earnshaw PH, Smith A, Katchburian MV, Hassan ANA, Amis AA (2002) Intraoperative measurement of knee kinematics in reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br 84(7):1075–1081
Chiu KY, Zhang SD, Zhang GH (2000) Posterior slope of tibial plateau in Chinese. J Arthroplasty 15:224–227
Çullu E, Özkan İ, Şavk ŞÖ, Alparslan B (1999) Tibial slope. Joint Dis Relat Surg 10(2):174–178
Dejour H, Bonnin M (1994) Tibial translation after anterior cruciate ligament rupture. Two radiological test compared. J Bone Joint Surg Br 76(5):745–749
Dejour H, Neyret P, Bonnin M (1992) Monopodal weight-bearing radiography of the chronically unstable knee. In: Jakob R, Staubli H-U (eds) Knee and the cruciate ligaments: anatomy, biomechanics, clinical aspect, reconstruction, complications, rehabilitation. Springer, Berlin, pp 568–576
Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD (2004) Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med 32(2):376–382
Griffin LY, Angel J, Albohm MJ, Arendt EA et al. (2000) Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg 8(3):141–150
Ireland ML (2002) The female ACL: why is it more prone to injury? Orthop Clin North Am 33(4):637–651
Jackowski DM, Kirkley A, Spechley M (2001) A prospective cohort study to determine risk factors for anterior cruciate ligament injury in varsity athletes. University of Western Ontario, London
Kennedy JC, Weinberg HW, Wilson AS (1974) The anatomy and function of the anterior cruciate ligament. As determined by clinical and morphological studies. J Bone Joint Surg 56(2):223–235
Kessler MA, Burkart A, Martinek V, Beer A, Imhoff AB (2003) Development of a 3-dimensional method to determine the tibial slope with multislice-CT. Z Orthop Ihre Grenzgeb 141(2):143–147
Kuwano T, Urabe K, Miura H, Nagamine R, Matsuda S, Satomura M, Sasaki T, Sakai S, Honda H, Iwamoto Y (2005) Importance of the lateral anatomic tibial slope as a guide to the tibial cut in the total knee arthroplasty in Japanese patients. J Orthop Sci 10(1):42–47
Lerat JL, Moyen BL, Cladiere F, Besse JL, Abidi H (2000) Knee instability after injury to the anterior cruciate ligament. J Bone Joint Surg Br 82(1):42–47
Mahfouz MR, Komistek RD, Dennis DA, Hoff WA (2004) In vivo assessment of the kinematics in normal and anterior cruciate ligament-deficient knees. J Bone Joint Surg Am 86A(2):56–61
Matsuda S, Miura H, Nagamine R, Urabe K, Ikenoue T, Okazaki K, Iwamoto Y (1999) Posterior tibial slope in the normal and varus knee. Am J Knee Surg 12(3):165–168
Meister K, Talley MC, Horodyski MB, Indelicato PA, Hartzel JS, Batts J (1998) Caudal slope of the tibia and its relationship to noncontact injuries to the ACL. Am J Knee Surg 11(4):217–219
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stijak, L., Herzog, R.F. & Schai, P. Is there an influence of the tibial slope of the lateral condyle on the ACL lesion?. Knee Surg Sports Traumatol Arthr 16, 112–117 (2008). https://doi.org/10.1007/s00167-007-0438-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-007-0438-1