
Abstract
Purpose
In the treatment of medial osteoarthritis secondary to anterior cruciate ligament (ACL) injury there is no consensus about optimum treatment, with both high tibial osteotomy (HTO) and unicompartmental knee arthroplasty (UKA) being viable options. The aim of this review was to compare the outcomes of these treatments, both with or without ACL reconstruction.
Methods
EMBASE, MEDLINE and the Clinical Trials Registers were searched to identify relevant studies. Studies meeting pre-defined inclusion criteria were assessed independently by two researchers for methodological quality and data extracted.
Results
Twenty-six studies involving 771 patients were identified for inclusion. No randomized controlled trials were identified. Seventeen studies reported outcomes following HTO and nine studies reported outcomes following UKA. HTO patients were significantly younger than those receiving UKA, and ACL reconstruction patients were younger than non-reconstructed patients. Treatment with HTO ACL reconstruction had the lowest revision rate (0.62/100 observed component years) but the highest rate of complications (4.61/100 observed component years). Too little data were available to test for differences in outcome between different surgical techniques or prosthesis designs.
Conclusions
Limited conclusions about the optimum treatment can be made due to the absence of controlled trials. In patients treated with HTO ACL reconstruction, the high complication rate likely outweighs its minimally superior survival. Outcomes following UKA ACL reconstruction are similar to outcomes for UKA in the ACL intact knee without any increase in complications. As such in patients meeting indications for UKA, UKA ACL reconstruction should be performed with further work required to identify the optimum treatment in other patient groups.
Level of evidence
IV.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Anterior cruciate ligament (ACL) injury is an established risk factor for the development of secondary osteoarthritis (OA) of the knee with the relative risk of developing radiological disease, grade II or greater, by 10 years almost fivefold that of an un-injured knee [2, 33]. Patients with a primary ACL injury who develop secondary OA are typically young and active, and in these patients the disease pattern in the medial tibial plateau is typically more posterior than the antero-medial OA seen in patients with an intact ACL, [19, 36, 45]. Conversely, patients with primary OA who develop secondary ACL instability tend to be comparatively older and less active with a more extensive pattern of disease across both the medial and lateral compartments. In this latter group with ACL deficiency secondary to OA, a total knee arthroplasty (TKA) is considered the treatment of choice [34, 37, 44]; however, there is no consensus on the treatment of medial knee OA in ACL deficiency patients where ACL deficiency is the primary pathology.
For patients with ACL deficiency who develop secondary OA that does not respond to non-operative modalities the surgical treatment options are as follows: (1) high tibial osteotomy (HTO) with or without ACL reconstruction, (2) unicompartmental knee arthroplasty (UKA) with or without ACL reconstruction, or (3) TKA or (4) ACL reconstruction alone. Due to younger age and higher activity levels seen in patients with primary ACL deficiency who develop secondary OA, bone conserving options are preferred with TKA not being recommended as the primary treatment option in this cohort [37, 44]. At the other end of the spectrum ACL reconstruction alone, with the exception of those patient who report instability as their primary complaint, is not a definitive treatment option but can be used as a reasonable, low co-morbidity treatment option to improve symptoms prior to subsequent HTO or UKA [47].
Whilst both HTO and UKA have been demonstrated to be valid treatment options for the treatment of medial OA secondary to ACL deficiency, the philosophy behind each technique is markedly different, and there continues to be lack of consensus in the literature as to which technique provides optimum outcomes for specific patient subgroups. Additionally, whilst HTO can be performed either with or without ACL reconstruction in UKA simultaneous or sequential ACL reconstruction is advised due to the higher risk of tibial loosening; however, in certain cases, upon patient request, UKA has been performed alone [5].
The primary aim of this review is to assess the surgical treatment options for medial OA in ACL deficiency patients in terms of risk of revision, complications and clinical outcomes. The secondary aim is to assimilate the outcomes of surgery in specific patient groups to provide an evidence-based approach to patient management as well as to identify areas for further research.
Materials and methods
EMBASE, MEDLINE and the Cochrane Central Register of Controlled Trials (CENTRAL) were searched for randomized clinical trials (RCTs), quasi-randomized and controlled clinical trials (CCTs) and case series (CS) investigating the surgical treatment options for medial OA in adult patients (>18 years) with ACL deficiency published between 1 January 1974 and 27 January 2014. Specifically, we included studies that assessed: HTO with ACL deficiency, HTO with ACL reconstruction, UKA with ACL deficiency and UKA with ACL reconstruction. The search strategy was based on that reported by the Cochrane Collaboration. Studies published in English, German and French were considered. In EMBASE, the following search strategy comprising of MESH terms as well as a free text search was used to identify relevant studies.
-
1.
OA [MESH] OR Knee [MESH] OR ‘medial knee arthritis’
-
2.
ACL [MESH] or ‘anterior cruciate ligament’ AND ‘insufficient*’ OR ‘rupture’ OR ‘instability’ OR ‘deficient’ OR ‘injury’
-
3.
AND 2.
-
4.
Tibia osteotomy [MESH] OR Tibia proximal osteotomy [MESH] or Osteotomy [MESH]
-
5.
‘unicondylar’ OR ‘unicompartmental’ OR ‘partial’ AND ‘knee arthroplasty’
-
6.
‘unicondylar’ OR ‘unicompartmental’ OR ‘partial’ AND ‘knee replacement’
-
7.
4. OR 5. OR 6.
-
8.
AND 7.
The reference lists of relevant studies were searched to identify further papers. The systematic review was performed in accordance with the PRISMA guidelines. Two review authors (FM and TH) identified trials to establish whether the study met the inclusion criteria regarding diagnosis, design and intervention. For each selected study, the full article was retrieved for final assessment. For studies meeting inclusion criteria, quality was assessed according to the Methodological index for non-randomized studies (MINORS) score, which is an instrument designed to assess the methodological quality of non-randomized observational surgical studies, both comparative and non-comparative [38].
Data were extracted independently in duplicate using a pre-tested, standardized form. Data relating to patient demographics, surgical procedure, follow-up period, number of complications, re-operations and revision surgeries as well as functional outcome using a validated scoring system were recorded. Disagreements were resolved by discussion, if disagreement persisted after discussion, the final decision was taken by a third review author (HP). We considered complications as any deviation from the expected post-operative course, both operative and non-operative. Failures were defined as any event resulting in further surgery in which a component was changed, a new component was added or where bearing dislocation had occurred in the case of UKA [28]; any patient requiring revision or replacement surgery for HTOs [20] and/or any traumatic graft rupture for ACL reconstructions [41]. Revision was defined as any operation where the patient underwent further surgery requiring the removal and/or exchange of any material implanted during the index operation.
Raw survival rates were calculated by dividing the number of not-failed patients at the last follow-up by the total number of patients followed up. The rate of failures, revisions, complications and re-operations per 100 observed component years was calculated using the method of calculation introduced by the Australian Arthroplasty Register, which allows the datasets with different numbers of cases and follow-up periods to be compared directly with each other [25].
Results
Descriptions of study
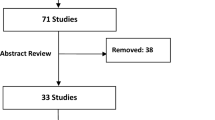
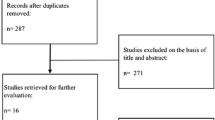
The search results are outlined in Fig. 1. Search revealed 131 papers. Among these, 26 studies involving 771 patients were suitable for inclusion in this review. Seventeen studies were retrospective in nature whilst nine were prospective. There were no randomized or quasi-randomized controlled trials. There were 22 CS of HTO with (n = 12) or without (n = 1) ACL reconstruction or UKA with (n = 5) or without (n = 4) ACL reconstruction. In addition, there were four cohort studies comparing HTO with or without ACL reconstruction [1, 3–7, 10–13, 16, 17, 21, 23, 24, 26, 27, 29–32, 42–44, 46, 48]. The assessment of methodological quality is outlined in Table 1. The median MINORS score was 8 (range 5–12) out of a maximum score of 16 for cases series and 12.5 (range 10–15) out of 24 for comparative studies. Patient demographics are reported in Table 2. All patients were diagnosed with medial OA however, the severity of OA was not clearly defined. In patients undergoing HTO various degrees of varus mal-alignment were reported, however, pre-operative alignment was not reported for patients undergoing UKA. Pre-operative symptoms of pain and instability were not clearly reported; however, instability tended to be reported in patients undergoing ACL reconstruction. For ACL reconstruction, mainly hamstring and bone-patellar tendon-bone (BPTB) autografts were used, but the use of allografts and synthetic implants was also described. For UKA, cemented implants were used in all patients.

Search results flowchart
Survival, revisions and complications
Raw survival rates, failures, revisions, complications and re-operations per 100 observed component years are reported in Table 3. In HTO ACL deficiency group, in addition to 1 revision due to a non-union (0.8 %), 5 complications (3.9 %) were reported in 127 patients. One of these required operative management [0.8 %; 1 manipulation under anaesthesia (MUA)] and 4 were managed non-operatively (3.1 %; data non-specified).
In HTO ACL reconstruction group, in addition to 9 revisions (2.6 %) due to 3 delayed consolidation, 1 non-union, 1 loss of fixation and 4 unknown reasons, 12 ACL re-ruptures were reported and counted as failures, but these patients did not undergo a new ACL reconstruction. Further, 74 complications [21.1 %; 23 deep venous thrombosis (DVT)], 13 stiffness, 1 hardware intolerance, 2 infections, 1 patellar tendon shortening, 8 haematomas, 2 delays in wound healing, 5 algodystrophy, 1 fixation instability, 1 neurovascular lesion, 1 patella fracture, 1 fibular pseudo-arthrosis and 14 not specified) were reported in 350 patients. Thirty of these required operative management (8.6 %; 1 hardware removal, 1 patellar lengthening, 1 stiffness, 1 re-fixation, 2 fibular resections, 3 ACL graft re-fixations, 7 scopes, 6 MUA, 2 arthrolysis, 1 fasciotomy and 2 haematoma drainages) whilst the others were managed non-operatively (12.6 %).
In UKA ACL deficiency group, 19 failures were reported (12.3 %; 4 progression of lateral OA, 1 painful joint replacement, 12 tibia loosening, 1 bearing instability, 1 not specified) which all required revision (12.3 %; 10 conversions to TKA, 1 arthrodesis, 1 conversion to bi-unicompartmental arthroplasty, 7 not specified). No complications were reported in 154 patients.
In UKA ACL reconstruction group, in addition to 3 failures (2.8 %; 1 each of progression of lateral OA, periprosthetic infection and bearing dislocation) which all required revision (2.8 %; 1 conversions to TKA, 1 two-stage revision to TKA, 1 bearing substitution), 3 complications (2.8 %; 1 lateral meniscal tear, 2 stiffness), managed with a re-operation (2.8 %; 2 scope, 1 MUA) were reported in 106 patients.
Survival rates of UKA by bearing type are reported in Table 4.
Other outcomes
Different clinical score were used in the various studies and their pooling was not possible. Clinical scores data are reported in Table 5.
The mean mal-alignment correction, reported in 10 out of 14 studies in HTO ACL reconstruction group, was 8° (range 2.8°–11.9°) from the pre-operative evaluation. It was reported in 5 out of 13 studies among the other 3 groups. In HTO ACL deficiency group, the mean correction was 11.5° (range 11°–11.6° reported in 2 studies). In UKA ACL deficiency group, it was reported only in one paper and it was 6.4°. Posterior slope was reported only in 7 studies out of 23, with post-operative values included between 2.5° and 11.7°, but with no clear description of benchmarks used so comparison was not possible.
Discussion
The most important finding of the present study is that the revision rate following both HTO and UKA is significantly lower when ACL reconstruction is performed, compared to when it is not. Where ACL reconstruction is performed in patients who undergo HTO have a marginal, yet significant, lower revision rate, but a significantly higher re-operation and complication rate, compared with patients undergoing UKA. Patient-specific factors that may favour one operation over the other may well exist but these have yet to be clearly defined, and in the existing studies the indications for performing one operation over another were poorly documented. The management of OA secondary to ACL deficiency remains a clinical challenge and there is no clear consensus as to the optimum treatment with this review highlighting that currently there is wide variation in practice with both HTO and UKA with or without ACL reconstruction being used to treat this population.
Important confounding factors that limit the direct comparison of outcomes of one technique over another include: age, disease severity and the presence of extra-articular deformity. Whilst across the published CS, the indications for the use of one technique over another were not clearly documented and several differences were noted in patient populations between different techniques. Patients undergoing HTO were significantly younger, with a mean age of 37 years compared to a mean age of 60 years in patients being treated with UKA. This observed difference in age may be due to differences in surgical practice, for example, surgeons are often reluctant to perform joint arthroplasty in the young but may instead prefer HTO as this strategy does not rule out subsequent joint replacement in case of failure. An equally valid potential reason for the differences in age may be that the studies are reporting on different populations with different stages of disease. Whilst stage of OA and indication for surgery was poorly reported across all case studies, HTO is indicated in early stage disease (partial thick cartilage loss), in contrast to UKA which is indicated in the presence of bone-on-bone arthritis [35]. As such whilst UKA can be seen as a definitive treatment for medial OA, HTO may also have a role also in changing the natural history of the disease and as a consequence it may be being performed at an earlier stage to halt the disease progression.
In addition, age may also influence the decision to perform ACL reconstruction. In the published studies patients with ACL reconstruction, both in HTO and UKA groups, were significantly younger than patients in whom reconstruction was not performed (mean age 38 vs 58 years) with pain and instability being more likely to be the presenting complaint than pain alone. The reasons for this are not clear from the published literature, but may be due to differences in the presenting complaint as older, lower demand, patients may be able to cope better with instability, or indeed it may be due to differences in the stability seen at different stages in the arthritis process with stiffness and osteophytes seen in more advanced disease, more prevalent in an older population, contributing to stability [9].
The results of HTO performed in the absence of ACL reconstruction demonstrate that the survival of HTO alone is higher than UKA alone, but lower than HTO with ACL reconstruction but with neither difference reaching statistical significance. Whilst acknowledging the different patient populations in the studies, these results suggest that in UKA it is more important to reconstruct the ACL compared with HTO. Given the high complication rate following combined HTO ACL reconstruction (21.1 %), there is a pressing need to identify which patients will benefit most from combined HTO ACL reconstruction and which may be treated by HTO alone. Lattermann et al. [26] suggest that where patients report pain and instability, a combined, simultaneous, procedure should be used, whereas in patients reporting pain alone a two-stage approach of HTO followed by ACL reconstruction in those who subsequently report instability may be more beneficial. Alternatively, multi planar reconstruction, correcting the frontal plane deformity, whilst simultaneously reducing the posterior tibial slope may be used to improve stability within the knee with Dejour et al. [10] have reporting a correlation between posterior tibial slope and anterior tibial translation in both ACL intact and ACL deficiency knees.
Overall, UKA with ACL reconstruction performed well with a revision rate of 0.72 % per 100 observed component years, which is comparable to outcomes in patients with intact ACL. Outcomes in ACL reconstruction patients receiving fixed-bearing designs compared with mobile bearing were similar but the sample size and follow-up period, were too small to allow appropriate statistical analysis. The results reported in the CS of ACL reconstruction knees are comparable with a meta-analysis of fixed compared mobile bearings in the treatment of medial OA in ACL intact patients who reported no significant difference in clinical outcome and complication rate at a mean follow-up of 5.8 years Smith et al. [39]. The long term outcomes of fixed versus mobile bearing UKA in the setting of ACL deficiency still need to be established to give guidance as to the optimum implant in this patient group.
Whilst ACL deficiency is considered as a contra-indication to UKA, several studies have reported on the outcomes of UKA without ACL reconstruction. Compared to UKA with ACL reconstruction, this cohort of patients has a significantly higher failure rate (by a factor of two), with tibial component loosening being the most frequent reason of failure. An important factor if performing UKA in ACL deficiency knees is the tibial slope. Hernigou et al. [21] reported an increase in aseptic loosening associated with increased posterior tibial slope and recommended that the tibia slope should not exceed 7°. A cadaveric study by Suero et al. [15, 40] has reported that reducing tibial slope decreases anterior tibial translation in fixed bearing UKA which may play a role in aseptic loosening, particularly in ACL deficiency knees. Although this is relevant for fixed bearing UKAs, change of tibial slope is not advocated for mobile bearing UKAs. Only 7 studies out of 23 reported data on tibial slope so it is not possible to come to a definite conclusion on the correlation between tibial slope and survival rate. The revision rate of mobile-bearing designs was marginally higher in ACL deficiency knees compared to fixed-bearing designs; however, there was insufficient data, both in terms of numbers of patients and follow-up period to perform a robust analysis.
In the published CS, the degree of correction of alignment was reported in five studies investigating HTO with a mean correction of 8° in the ACL reconstruction group and 11.5° in the ACL deficiency group, whereas none of the studies reporting on UKR reported alignment data. In HTO, mechanical axis correction can be considered the primary consideration, with the main indication being correction of frontal varus mal-alignment caused by an extra-articular, usually metaphyseal, deformity (tibia vara) [22]. In contrast, UKA’s main aim is to correct intra-articular varus deformity, which is primarily caused by loss of articular cartilage loss, rather than to correct limb alignment [18]. In tibia vara, HTO corrects the lower limb axis shifting the load towards the lateral compartment, thus reducing pressures on cartilage defects. Whilst the literature outlines multiple definitions of the optimal alignment following HTO, an important consideration is whether the procedure is likely to be a definitive one, where the joint may be over corrected, or a temporizing procedure, aiming for neutral alignment, prior to subsequent joint arthroplasty [8]. The results of our study did find a lower degree of correction seen in the ACL reconstruction group, who were significantly younger, compared to the ACL deficiency group; however, it is unclear if this was to facilitate future arthroplasty or whether the different groups had different levels of disease severity with greater correction required in ACL deficiency group who potentially had more advanced disease.
In patients treated with HTO, a closing wedge lateral osteotomy was performed in 92 % of cases in both ACL deficiency and ACL reconstruction knees. It is not clear if it this was due to surgeon preference or experience or if closing wedge osteotomy was, particularly in ACL deficiency patients, used to reduce the posterior tibial slope as a secondary effect [22]. Compared with an opening wedge technique closing wedge osteotomy has several further advantages. With a closing wedge compression on the osteotomy site removes the need for bone graft, morbidity associated with its harvest and in theory this compression should decrease the rate of non-union. However, one of the disadvantages of closing wedge osteotomies is the risk of persistent laxity in the medial collateral ligament (MCL) with Gaasbeek et al. reporting a lower degree of laxity following an open wedge technique. As a consequence with an opening wedge technique, there is a risk of excessive tightening of the MCL with large corrections which will increase pressure in the medial compartment, which go against the primary aim of the operation, and in addition there is a risk of increasing the posterior tibial slope [14].
The complications seen in the following surgery differed between patients receiving HTO and UKA. In HTO, groups complications were mainly related to ACL graft re-rupture, loss of fixation or bony union at the osteotomy site, whereas in UKA failures were related mainly to lateral OA progression or tibial component loosening. Overall, the rate of complications following HTO, in particular HTO with ACL reconstruction, was around threefold higher than the rate seen in patients receiving UKA. Following HTO with ACL reconstruction, the incidence of ACL re-rupture was around 3.4 %, whereas ACL re-rupture was not reported in any of the UKA studies. The majority of ACL ruptures in the HTO group were treated non-operatively, providing further evidence that HTO alone may be able to restore stability in some patient groups. Closing wedge osteotomies are said to reduce the posterior tibial slope, and consequently, ACL strain thus protecting it; however, the sample size was too small to test for differences in ACL rupture rate between patients undergoing closing and opening wedge osteotomies. Data pertaining to patient characteristics, graft positioning and other potential contributing factors were not provided, and as such further analysis, this finding was not possible. Further research is required to better understand the mechanism of graft rupture and identify any patient or operative factors that predict this. In addition, consensus over the optimum method of pre- and intra-operative assessment of the ACL needs to be achieved to allow accurate comparisons of the disease state of the ACL in future studies.
The clinical relevance of these findings is that in patients with ACL deficiency and secondary OA the primary question should be, is this patient suitable for UKA? As if a patient is suitable for UKA, then, due to the high complication rate seen HTO with ACL reconstruction, UKA with ACL reconstruction should be performed. In patients unsuitable for UKA, particularly those with partial thickness disease, then, HTO ± ACL reconstruction may be indicated, however, which patients may benefit from ACL reconstruction still needs to be defined.
Limitations of this review are that the current data are restricted to cases series as no randomized controlled trials have been published. The lack of homogeneity in each treatment group and lack of provision of data regarding disease severity and indication for the index operation limit the conclusions that can be drawn. Data regarding the experience of the surgeons with each particular technique, which is known to effect both the outcomes of HTO and UKA, was also not published and it is known that, in particular with UKA, some of the series may represent the learning curve of individual surgeons or the development curve of the implant. Finally, it must be acknowledged that the calculated outcome measure of analyzing revisions per 100 observed component years, whilst it allows a comparison across studies with different follow-up periods, assumes that revisions distribution is linear over time, which is indeed not the case.
Conclusions
The lack of high quality studies, and the absence of randomized or matched trials, suitable for this review makes it difficult to draw definite conclusions about the best treatment for treating patients with primary ACL deficiency and secondary medial OA. The demographic differences that were detected between treatment groups indicated that different indications may be being used for each procedure and that age, or a confounding factor related to age such as disease state, may influence the choice of surgical management. Important findings from this study are that HTO with ACL reconstruction, whilst having a comparable survival to UKA ACL reconstruction, has a high complication rate of around 21 %. As such from the results of this study, we would conclude that if a patient meets indications for UKA then UKA ACL reconstruction should be performed to achieve clinical outcomes similar to UKA in ACL intact patients with no increase in complications. However, further trials are required to directly compare UKA ACL reconstruction with HTO ± ACL reconstruction in a matched population to establish which patient factors, namely: age, disease severity and presence, location and severity of extra-articular deformity favour one treatment option over another, and as a secondary goal to establish in which patients undergoing HTO is ACL reconstruction indicated.
References
Agneskirchner JD, Burkart A, Imhoff AB (2002) Axis deviation, cartilage damage and cruciate ligament rupture-concomitant interventions in replacement of the anterior cruciate ligament. Unfallchirurg 105:237–245
Ajuied A, Wong F, Smith C, Norris M, Earnshaw P, Back D, Davies A (2014) Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med 42:2242–2252
Akamatsu Y, Mitsugi N, Taki N, Takeuchi R, Saito T (2010) Simultaneous anterior cruciate ligament reconstruction and opening wedge high tibial osteotomy: report of four cases. Knee 17:114–118
Badhe NP, Forster IW (2002) High tibial osteotomy in knee instability: the rationale of treatment and early results. Knee Surg Sports Traumatol Arthrosc 10:38–43
Boissonneault A, Pandit H, Pegg E, Jenkins C, Gill HS, Dodd CA, Gibbons CL, Murray DW (2013) No difference in survivorship after unicompartmental knee arthroplasty with or without an intact anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 21:2480–2486
Bonin N, Ait Si Selmi T, Donell ST, Dejour H, Neyret P (2004) Anterior cruciate reconstruction combined with valgus upper tibial osteotomy: 12 years follow-up. Knee 11:431–437
Boss A, Stutz G, Oursin C, Gachter A (1995) Anterior cruciate ligament reconstruction combined with valgus tibial osteotomy (combined procedure). Knee Surg Sports Traumatol Arthrosc 3:187–191
Briem K, Ramsey DK, Newcomb W, Rudolph KS, Snyder-Mackler L (2007) Effects of the amount of valgus correction for medial compartment knee osteoarthritis on clinical outcome, knee kinetics and muscle co-contraction after opening wedge high tibial osteotomy. J Orthop Res 25:311–318
Christensen NO (1991) Unicompartmental prosthesis for gonarthrosis. A nine-year series of 575 knees from a Swedish hospital. Clin Orthop Relat Res 273:165–169
Dejour H, Neyret P, Boileau P, Donell ST (1994) Anterior cruciate reconstruction combined with valgus tibial osteotomy. Clin Orthop Relat Res 299:220–228
Demange MK, Camanho GL, Pecora JR, Gobbi RG, Tirico LE, da Mota e Albuquerque RF (2011) Simultaneous anterior cruciate ligament reconstruction and computer-assisted open-wedge high tibial osteotomy: a report of eight cases. Knee 18:387–391
Dervin GF, Conway AF, Thurston P (2007) Combined anterior cruciate ligament reconstruction and unicompartmental knee arthroplasty: surgical technique. Orthopedics 30:39–41
Engh GA, Ammeen DJ (2014) Unicondylar arthroplasty in knees with deficient anterior cruciate ligaments. Clin Orthop Relat Res 472:73–77
Gaasbeek RD, Nicolaas L, Rijnberg WJ, van Loon CJ, van Kampen A (2010) Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomy. A one-year randomized controlled study. Int Orthop 34:201–207
Garg A, Walker PS (1990) Prediction of total knee motion using a three-dimensional computer-graphics model. J Biomech 23:45–58
Giger P, Bereiter H, Gachter A (1987) Replacement of the anterior cruciate ligament combined with valgization osteotomy of the tibia in incipient medial gonarthrosis with anterior cruciate ligament insufficiency. Z Orthop Ihre Grenzgeb 125:68–72
Goodfellow JW, Kershaw CJ, Benson MK, O’Connor JJ (1988) The Oxford Knee for unicompartmental osteoarthritis. The first 103 cases. J Bone Joint Surg Br 70:692–701
Gulati A, Pandit H, Jenkins C, Chau R, Dodd CA, Murray DW (2009) The effect of leg alignment on the outcome of unicompartmental knee replacement. J Bone Joint Surg Br 91:469–474
Harman MK, Markovich GD, Banks SA, Hodge WA (1998) Wear patterns on tibial plateaus from varus and valgus osteoarthritic knees. Clin Orthop Relat Res 352:149–158
Haviv B, Bronak S, Thein R, Kidron A (2012) Mid-term outcome of opening-wedge high tibial osteotomy for varus arthritic knees. Orthopedics 35:192–196
Hernigou P, Deschamps G (2004) Posterior slope of the tibial implant and the outcome of unicompartmental knee arthroplasty. J Bone Joint Surg Am 86:506–511
Hohmann E, Bryant A, Imhoff AB (2006) The effect of closed wedge high tibial osteotomy on tibial slope: a radiographic study. Knee Surg Sports Traumatol Arthrosc 14:454–459
Hui C, Salmon LJ, Kok A, Williams HA, Hockers N, van der Tempel WM, Chana R, Pinczewski LA (2011) Long-term survival of high tibial osteotomy for medial compartment osteoarthritis of the knee. Am J Sports Med 39:64–70
Krishnan SR, Randle R (2009) ACL reconstruction with unicondylar replacement in knee with functional instability and osteoarthritis. J Orthop Surg Res 4:43
Labek G, Thaler M, Janda W, Agreiter M, Stockl B (2011) Revision rates after total joint replacement: cumulative results from worldwide joint register datasets. J Bone Joint Surg Br 93:293–297
Lattermann C, Jakob RP (1996) High tibial osteotomy alone or combined with ligament reconstruction in anterior cruciate ligament-deficient knees. Knee Surg Sports Traumatol Arthrosc 4:32–38
Lerat JL, Moyen B, Garin C, Mandrino A, Besse JL, Brunet-Guedj E (1993) Anterior laxity and internal arthritis of the knee. Results of the reconstruction of the anterior cruciate ligament associated with tibial osteotomy. Rev Chir Orthop Reparatrice Appar Mot 79:365–374
Murray DW, Pandit H, Weston-Simons JS, Jenkins C, Gill HS, Lombardi AV, Dodd CA, Berend KR (2013) Does body mass index affect the outcome of unicompartmental knee replacement? Knee 20:461–465
Neuschwander DC, Drez D Jr, Paine RM (1993) Simultaneous high tibial osteotomy and ACL reconstruction for combined genu varum and symptomatic ACL tear. Orthopedics 16:679–684
Noyes FR, Barber-Westin SD, Hewett TE (2000) High tibial osteotomy and ligament reconstruction for varus angulated anterior cruciate ligament-deficient knees. Am J Sports Med 28:282–296
Noyes FR, Barber SD, Simon R (1993) High tibial osteotomy and ligament reconstruction in varus angulated, anterior cruciate ligament-deficient knees. A two- to seven-year follow-up study. Am J Sports Med 21:2–12
O’Neill DF, James SL (1992) Valgus osteotomy with anterior cruciate ligament laxity. Clin Orthop Relat Res 278:153–159
Oiestad BE, Engebretsen L, Storheim K, Risberg MA (2009) Knee osteoarthritis after anterior cruciate ligament injury: a systematic review. Am J Sports Med 37:1434–1443
Pandit H, Beard DJ, Jenkins C, Kimstra Y, Thomas NP, Dodd CA, Murray DW (2006) Combined anterior cruciate reconstruction and Oxford unicompartmental knee arthroplasty. J Bone Joint Surg Br 88:887–892
Pandit H, Jenkins C, Gill HS, Smith G, Price AJ, Dodd CA, Murray DW (2011) Unnecessary contraindications for mobile-bearing unicompartmental knee replacement. J Bone Joint Surg Br 93:622–628
Rout R, McDonnell S, Hulley P, Jayadev C, Khan T, Carr A, Murray D, Gill H, Price A (2013) The pattern of cartilage damage in antero-medial osteoarthritis of the knee and its relationship to the anterior cruciate ligament. J Orthop Res 31:908–913
Shelbourne KD, Benner RW (2007) Isolated anterior cruciate ligament reconstruction in the chronic ACL-deficient knee with degenerative medial arthrosis. J Knee Surg 20:216–222
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73:712–716
Smith TO, Hing CB, Davies L, Donell ST (2009) Fixed versus mobile bearing unicompartmental knee replacement: a meta-analysis. Orthop Traumatol Surg Res 95:599–605
Suero EM, Citak M, Cross MB, Bosscher MR, Ranawat AS, Pearle AD (2012) Effects of tibial slope changes in the stability of fixed bearing medial unicompartmental arthroplasty in anterior cruciate ligament deficient knees. Knee 19:365–369
Suomalainen P, Jarvela T, Paakkala A, Kannus P, Jarvinen M (2012) Double-bundle versus single-bundle anterior cruciate ligament reconstruction: a prospective randomized study with 5-year results. Am J Sports Med 40:1511–1518
Terzaghi C, Ferrari V, Legnani C, Albisetti W, Ventura A (2011) Combined anterior cruciate ligament reconstruction and unicompartmental knee arthroplasty. J Orthop Traumatol 12:1
Tinius M, Hepp P, Becker R (2012) Combined unicompartmental knee arthroplasty and anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 20:81–87
Weston-Simons JS, Pandit H, Jenkins C, Jackson WF, Price AJ, Gill HS, Dodd CA, Murray DW (2012) Outcome of combined unicompartmental knee replacement and combined or sequential anterior cruciate ligament reconstruction: a study of 52 cases with mean follow-up of five years. J Bone Joint Surg Br 94:1216–1220
White SH, Ludkowski PF, Goodfellow JW (1991) Anteromedial osteoarthritis of the knee. J Bone Joint Surg Br 73:582–586
Williams RJ 3rd, Kelly BT, Wickiewicz TL, Altchek DW, Warren RF (2003) The short-term outcome of surgical treatment for painful varus arthritis in association with chronic ACL deficiency. J Knee Surg 16:9–16
Williams RJ 3rd, Wickiewicz TL, Warren RF (2000) Management of unicompartmental arthritis in the anterior cruciate ligament-deficient knee. Am J Sports Med 28:749–760
Zaffagnini S, Bonanzinga T, Grassi A, Muccioli GMM, Musiani C, Raggi F, Iacono F, Vaccari V, Marcacci M (2013) Combined ACL reconstruction and closing-wedge HTO for varus angulated ACL-deficient knees. Knee Surg Sports Traumatol Arthrosc 21:934–941
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mancuso, F., Hamilton, T.W., Kumar, V. et al. Clinical outcome after UKA and HTO in ACL deficiency: a systematic review. Knee Surg Sports Traumatol Arthrosc 24, 112–122 (2016). https://doi.org/10.1007/s00167-014-3346-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-014-3346-1