
Abstract
Purpose
In total knee arthroplasty, surgical navigation systems provide tibio-femoral joint (TFJ) tracking for relevant bone preparation, disregarding the patello-femoral joint (PFJ). Therefore, the important intra-operative assessment of the effect of component positioning, including the patella, on the kinematics of these two joints is not available. The objective of this study is to explore in vivo whether accurate tracking of the patella can result in a more physiological TFJ and PFJ kinematics during surgery.
Methods
Ten patients underwent navigated knee replacement with patellar resurfacing. A secondary system was used to track patellar motion and PFJ kinematics using a special tracker. Patellar resection plane position and orientation were recorded using an instrumented probe. During all surgical steps, PFJ kinematics was measured in addition to TFJ kinematics.
Results
Abnormal PFJ motion patterns were observed pre-operatively at the impaired knee. Patellar resection plane orientation on sagittal and transverse planes of 3.9° ± 9.0° and 0.4° ± 4.1° was found. A good restoration of both TFJ and PFJ kinematics was observed in all replaced knees after resurfacing, in particular the rotations in the three anatomical planes and medio-lateral patellar translation.
Conclusions
Patella tracking results in nearly physiological TFJ and PFJ kinematics in navigated knee arthroplasty with resurfacing. The intra-operative availability also of PFJ kinematics can support the positioning not only of the patellar component in case of resurfacing, but also of femoral and tibial components.
Level of evidence
II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The complete comprehension of the natural function of the human knee joint depends on three-dimensional analysis of motion of both the tibio-femoral (TFJ) and the patello-femoral (PFJ) joints. The latter plays a fundamental role in the knee extensor mechanism [7, 10, 32], and a good patellar motion is important also for the success of total knee arthroplasty (TKA), since complications at the PFJ represent one of the main causes of surgical failure [30, 31, 33, 35]. In this surgery, patellar tracking is only visually inspected, and possible mal-tracking is realised at the end of the implantation, when only little final adjustments are possible [6, 16]. It is known that abnormal PFJ kinematics can result in anterior knee pain [33, 35]. The knowledge of this tracking throughout surgery therefore is important not only in the case of resurfacing, but also in non-resurfacing TKA, because the femoral and tibial components can be implanted to cope with initial mal-tracking or deformed conditions such as patella alta/baja or its dysplasia [22, 39]. The thickness of the patella before and after resurfacing is also important, and the current calliper-based measure is not artefact free [6, 16]. Instrumental intra-operative analysis of PFJ is therefore sought for successful operations and relevant prosthesis design [3, 7, 13].
Patellar motion has been investigated using several different methods and measuring devices [7, 10]. A number of studies have addressed PFJ kinematics in vitro [1, 7, 8, 10, 19, 25, 28, 38, 41], and a few mathematical models have been proposed [5, 17, 29, 37], but the most valuable measurements would be in vivo [4, 12, 21, 23, 24, 27, 34, 36, 40]. Mechanical and mathematical conventions, however, have been established [7, 10], based on recognised anatomical landmarks. Important progresses have been achieved in TKA with the introduction of knee surgical navigation systems, developed to optimise components positioning via intra-operative tracking of the bone segments and instrumentation [14, 15], but only femur and tibia are currently dealt with.
A few recent studies have analysed patellar tracking during TKA in vitro [2, 7, 19], one reported data in vivo before and after surgery [4], but not a single in vivo throughout the surgical steps. An original methodology for full assessment of PFJ kinematics during surgery, based on a standard navigation system with the addition of a separate tracker for the patella, has recently been developed and tested in vitro by these authors [6, 7]. This allows the determination of three-dimensional position and orientation (altogether pose) of the patella via calibration of anatomical landmarks.
The general aim of the present study is to explore the value of the knowledge of motion and of exact bone preparation parameters of the patella during navigated TKA surgery with patellar resurfacing. From initial experience obtained in in vitro experiments [6–8], a suitable surgical ad hoc protocol was developed, together with relevant dedicated software and surgical instrumentation. For the first time, both TFJ and PFJ are tracked simultaneously intra-operatively and patellar bone preparation was monitored, in terms of resection plane pose and location of the peg holes. The final scope of the present study is to assess whether this accurate patella resurfacing technique can result in a more physiological kinematics at these two joints.
Materials and methods
Ten patients affected by primary or inflammatory arthritis underwent primary TKA (Table 1) with a fixed bearing posterior-stabilised prosthesis (NRG, Stryker®-Orthopaedics, Mahwah, NJ-USA) and patellar resurfacing. Particularly, the size of the patient population analysed in this study meets the criteria for achieving differences in measurements with 80 % statistical power and α-level of 0.05. Clinical assessments were performed pre-operatively using the International Knee Society (IKS) scoring system [20] (Insall modification—1993), together with the assessment of the frontal mechanical axis on radiographs of the affected lower limb (Table 1). In addition, PFJ deformity was assessed immediately pre-operatively and at the end of operation via Merchant view radiographs; pre-operatively, no signs of dysplasia, subluxation or severe tilt were found.
Measurement equipment
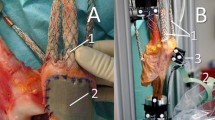
The bone preparation for femoral and tibial component implantation was performed according to a standard navigation system, traditionally utilised for TFJ navigation (Stryker®-Leibinger, Freiburg, Germany) [14, 15], with nominal and tested accuracy [7] of 0.5° and 0.5 mm. In addition, an original procedure for patellar tracking was performed by using a second experimental navigation system from the same company (Fig. 1), identical to the former system but with dedicated software for the collection and reporting (Fig. 2) of patellar references and motion . The entire procedure was approved by the local ethical committee and applied to all these patients after informed consent. Each of the two systems consists of a workstation equipped with a laptop for data processing and displaying, a localiser compound of three camera sensors, and a number of trackers, which communicate with the localiser via active light-emitting diodes. To avoid conflicts between the two navigation systems, each localiser had a camera shutter (Fig. 1), whose lowering/rising enabled tracker visibility when required. The two systems shared the standard femoral and tibial trackers, pinned into the bones, and the pointer-like tracker handled for system control and landmark digitisation. The experimental navigator is further equipped with a specially designed patellar tracker (Fig. 1), lighter and smaller than the femoral and tibial trackers and rigidly fixed by four 4-mm-long mono-cortical screws on the patellar anterior aspect, after bone exposure. The tracker is made of a thin titanium grid, folded to form a cylindrical sector, with a portion of a mask for cranial surgery (Stryker®-Leibinger, Freiburg, Germany) attached to the superior flatter area by sterile drape. This enabled standard patellar clamping for the surgical resurfacing procedure. It also provided a cluster of three active light-emitting diodes with a separate power supply to be seen with the patella both when it is in its natural location on the femoral trochlea and when it is partially everted to access its internal surface for anatomical landmarking.

Measurement set-up: the two navigation systems are positioned on the contralateral side (left) of the knee undergoing the TKA (right). Alternate lowering/rising of shutters disables/enables the localiser in corresponding tracker detection, this being marked in the figure by dashed/solid lines

Snapshots from the screen of the experimental navigator from a well-representative case. PFJ rotations (a left, in °) and translations (b right, in mm) assessed intra-operatively in the TRIAL step superimposed on those of the IMPAIR step
Acquisition procedure
Before surgery, both navigation systems were initialised, and the patellar tracker was assembled with a sterile procedure. On the experimental navigator, the template for drilling the patellar peg holes was instrumented with a standard tracker, and in the corresponding reference frame, the relevant geometry was characterised by suitable digitisation. The standard procedures for TKA navigation were performed on the standard navigator, starting from the anatomical survey, and immediately after, TFJ kinematics under passive conditions were collected [15]. At this step, i.e. with the knee still in its original impaired status (step IMPAIR), this process was repeated on the experimental navigator, for TFJ and PFJ kinematics (Fig. 2) by absolute pose registration of relevant trackers. For an exact replication of the survey, femoral and tibial anatomical landmarks were identified initially with a dermographic pen. In the experimental navigator, the most distal apex and the most medial and lateral prominences of the patellar articular surface were digitised.
Standard navigation-based procedures were then performed on the standard navigator for femur and tibia bone preparation, until corresponding trial prosthesis components were implanted. The procedures for patellar resection then followed [6, 7], these being tracked by the experimental navigator. Before that, the anterior, i.e. external, and posterior, i.e. internal, aspects of the patella were digitised to calculate the original patellar thickness. Still using the experimental navigator, both joint kinematics were recorded with the non-resurfaced patella and trial components in femur and tibia (step TRIAL). The patellar resection was performed and the pose of the corresponding component was recorded by the instrumented hole-drilling template. After patellar resection and final patellar component implantation, its posterior aspect was digitised to calculate the thickness also of the resurfaced patella.
Final components were implanted in the three bones and cemented, and the final joints kinematics (step FINAL) were recorded. In each of these three steps, two repetitions of a full cycle of passive flexion and extension were collected. In the experimental navigator, the kinematics at the three steps, i.e. IMPAIR, TRIAL (Fig. 2a, b) and FINAL, was superimposed for both joints. A sterile calliper was also used for an additional measurement of the patellar thickness before and after patellar resurfacing.
Anatomical and kinematics conventions
The anatomical coordinate systems for the femur and the tibia were defined using standard recommendations [11]. The patellar anatomical coordinate system was established and tested previously [7]. PFJ flexion–extension, medio-lateral rotation, tilt and translations along the three femur anatomical axes were calculated according to recent proposals [7, 10] together with TFJ rotations [18] and tibial translations along the three femur anatomical axes [9]. According to these conventions, both joint kinematics variables were calculated and shown at each surgical step on the experimental navigator. Post-operatively, these variables were also compared with in vitro control data from corresponding normal knees [8, 9].
This study was approved by the review board of the Istituto Ortopedico Rizzoli, Bologna, Italy (Identification Number 15/08); accordingly, all patients signed informed consent prior to surgery.
Statistical analysis
One-way analysis of variance was used to derive possible differences in kinematic variables between the surgical steps over the ten patients. Corresponding p values were calculated for assessing significance, this being accepted at p < 0.05. All calculations were made in MatLab® software package (The MathWorks, Inc., Natick, MA-USA).
Results
General results
The new overall technique was performed successfully in all surgeries without complications, resulting only in about 30-min-longer operation time on average. Patellar resection plane orientation on sagittal and transverse planes was 3.9° ± 9.0° and 0.4° ± 4.1°, respectively. At the end of operation, a good mechanical axis was achieved (Table 2), and no radiographic signs of patellar subluxation or tilt were found. The difference in patellar thickness before and after resurfacing (FINAL-IMPAIR), i.e. PFJ stuffing, was as small as −2.5, 0.5, 0.0, 0.7, 0.3, 0.6, −0.5, 0.6, 1.1, 2.0 mm in the ten knees.
TFJ kinematics
At the TFJ, the three rotations and translations after surgery were found to be within standard joint motion ranges (Table 2), both at the TRIAL and FINAL steps. Significant differences were found between the IMPAIR and FINAL surgical steps, i.e. before and after resurfaced TKA, over the ten patients for tibia-to-femur antero-posterior and proximo-distal translations.
In particular, the largely unphysiological ad-abduction patterns observed pre-operatively (IMPAIR) were all corrected. This can be realised also by the corresponding values in full extension (Table 2) at the IMPAIR and FINAL steps, these being −5.7° and 0.3°, respectively, in a typical case shown in Fig. 3.

TFJ and PFJ rotations (in mm) and translations (in °) over the TFJ flexion reported from patient #5, this being well representative for the entire cohort. For each variable, the IMPAIR (line with empty circle), TRIAL (dashed line) and FINAL (dotted line) patterns are plotted all together versus TFJ flexion and superimposed to corresponding control data from normal knees [8, 9] (solid line for the mean values centred on the band for one standard deviation)
PFJ kinematics
Physiological kinematics was observed also for the PFJ both at the TRIAL and FINAL steps. A nearly linear increase in flexion was observed over the flexion arc (Fig. 3). In particular, normal ranges were obtained for the patellar medio-lateral rotation and translation, and for tilt rotation (Table 2; Fig. 3). Significant differences were found between the IMPAIR and FINAL surgical steps over the ten patients for PFJ flexion–extension and proximo-distal translation.
This was true also in the presence of a particularly abnormal kinematics. At the IMPAIR step, abnormal lateral tilt in case A (range −15.1 to −3.9, Table 3) and abnormal medial translation in case B were observed (range −1.1 to 4.6, Table 3). At the FINAL step, these were recovered into more physiological ranges, respectively, −1.4 to −0.7 and −1.2 to 0.8 (Table 3). Abnormal patterns of motion were identified also at the intermediate TRIAL step, as for example, the lateral translation in case A and C (ranges −7.8 to −6.9 and −8.8 to −8.5, respectively, Table 3); this was addressed intra-operatively and resolved by a lateral retinacular release, which resulted in the FINAL step to the more physiological ranges of −3.6 to −1.2 and −3.5 to −3.9, respectively.
Discussion
The most important finding of the present study was that abnormal patterns also of the patello-femoral joint kinematics can be detected by looking intra-operatively at the patellar motion throughout the surgical steps (Table 2; Fig. 3). From these abnormalities, corresponding inaccuracies in bone preparation can be deduced, for the surgeon to make appropriate corrective actions during operation. In fact, the effect of patellar tracking, here originally introduced throughout navigated TKA with patellar resurfacing, on the kinematics of both knee joints was explored in vivo in real cases. The present very encouraging results demonstrate the value of this novel technique in the context of the modern surgical navigation systems. The tracking of the resection plane and the position of the prosthetic component at the patella resulted in an orientation error smaller than 4° and in a final patello-femoral stuffing smaller than about 2 mm. With the present technique, very satisfactory knee joint kinematics were obtained, particularly tilt rotation and medio-lateral translation of the latter.
This technique, which follows a protocol devised in previous in vitro studies [7, 8] and implies at the moment an additional navigator utilised in parallel to the standard one, has demonstrated to be feasible, i.e. able to reliably deliver additional measurements intra-operatively. The data collection performed by the additional experimental navigator did not affect the procedures of the standard navigator, and no surgical or post-surgical complications were registered. Particularly, the usual femoral and tibial trackers were complemented with a novel tracker for the patella, manufactured especially to ensure a rigid technical reference frame for the necessary digitisation of anatomical landmarks and articulating surfaces and to track patellar pose throughout knee motion. The report of patellar motion in clinical terms was met by successful calibration of these landmarks and by the adoption of standard joint conventions. The patellar tracker was designed to have negligible inertial effects and to be compatible with standard TKA procedures, including also those for patellar resurfacing, which was performed in all patients. Femoral, tibial and patellar pose data were successfully collected from the patients during all surgical steps, i.e. at the original impaired knee, with trial components but without patellar resurfacing, and with final components and resurfacing. The present technique also revealed that a relevant thorough three-dimensional calculation of the thickness of the original patella (at step IMPAIR) can be very different from the traditional measurements by the calliper, with a maximum over knees as large as 5 mm (2.2 ± 1.6 mm on average).
From the literature, only one previous study [4] reported PFJ kinematics intra-operatively, immediately before and after implantation. A different navigation system was used (Praxim®, Grenoble, France), and the reference frame for the patella was not defined based on relevant anatomical landmarks. Nevertheless, similar to the present study, significant changes between pre- and post-operative PFJ kinematics were observed, particularly in medio-lateral translation and tilt.
The technique reported in the present study has a number of limitations. The usage of a parallel navigation system for ad hoc measurements may have resulted in possible, however, small inconsistencies between the measurements from the two systems, though all the data here reported are from the experimental navigator. The number of cases performed so far is small, but additional cases will be reported. Other potential technical limitations, such as accuracy of the instruments, intra- and inter-surgeon repeatability of the anatomical coordinate system definitions, were discussed previously by the authors [7]. Control patterns for the kinematics variables (in yellow in Fig. 3) were here taken from normal knees, though obtained from equivalent in vitro measurements performed exactly with the same technique and in very similar conditions [8, 9]. Furthermore, the comparison was only in qualitative terms, just to figure out in which direction these patterns shall proceed over the successive surgical steps, for a good final replication of the natural joint motion. Finally, the additional surgical time could represent an issue for the new technique. However, this includes also operations outside the tourniquet-related time, and it is mainly due to the present preliminary instrumentation. Considering also the learning curve, the initial additional time is now shorter, and this could be further shortened, up to about 10 min, with the final instrumentation.
The present study first has explored in vivo patellar motion throughout TKA-navigated surgery, previous work being restricted on Sawbones® or specimen material [6, 16], or in vivo, but only before and after operation [4]. It has been demonstrated that an accurate patella resurfacing technique can result in a more physiological kinematics at both the tibio-femoral and patello-femoral joints. This is expected to results in limiting current complications at the latter, which represent one of the main causes of failure in TKA. The present intra-operative motion-tracking technique can support not only the patellar resurfacing, but also the positioning of the tibial and particularly the femoral components [25, 26], also in case of no resurfacing.
Conclusion
The extension to PFJ of the current standard navigation systems for TKA results in very encouraging kinematics at both joints of the knee and therefore lays the foundation for the design of future surgical patellar navigation systems, for the surgeon to perform a most possible comprehensive knee arthroplasty.
References
Amis AA, Senavongse W, Bull AM (2006) Patellofemoral kinematics during knee flexion–extension: an in vitro study. J Orthop Res 24:2201–2211
Anglin C, Brimacombe JM, Hodgson AJ, Masri BA, Greidanus NV, Tonetti J, Wilson DR (2008) Determinants of patellar tracking in total knee arthroplasty. Clin Biomech (Bristol, Avon) 23:900–910
Anglin C, Brimacombe JM, Wilson DR, Masri BA, Greidanus NV, Tonetti J, Hodgson AJ (2010) Biomechanical consequences of patellar component medialization in total knee arthroplasty. J Arthroplast 25:793–802
Anglin C, Ho KC, Briard JL, de Lambilly C, Plaskos C, Nodwell E, Stindel E (2008) In vivo patellar kinematics during total knee arthroplasty. Comput Aided Surg 13:377–391
Ateshian GA, Hung CT (2005) Patellofemoral joint biomechanics and tissue engineering. Clin Orthop Relat Res 436:81–90
Belvedere C, Ensini A, Leardini A, Feliciangeli A, Giannini S (2013) Patellar tracking in computer-assisted surgery. In: Catani F, Zaffagnini S (eds) Knee surgery using computer assisted surgery and robotics, 1st edn. Springer, Heidelberg, pp 187–201
Belvedere C, Catani F, Ensini A, de la Barrera JM, Leardini A (2007) Patellar tracking during total knee arthroplasty: an in vitro feasibility study. Knee Surg Sports Traumatol Arthrosc 15:985–993
Belvedere C, Leardini A, Ensini A, Bianchi L, Catani F, Giannini S (2009) Three-dimensional patellar motion at the natural knee during passive flexion/extension. An in vitro study. J Orthop Res 27:1426–1431
Belvedere C, Leardini A, Giannini S, Ensini A, Bianchi L, Catani F (2011) Does medio-lateral motion occur in the normal knee? An in vitro study in passive motion. J Biomech 44:877–884
Bull AM, Katchburian MV, Shih YF, Amis AA (2002) Standardisation of the description of patellofemoral motion and comparison between different techniques. Knee Surg Sports Traumatol Arthrosc 10:184–193
Cappozzo A, Catani F, Croce UD, Leardini A (1995) Position and orientation in space of bones during movement: anatomical frame definition and determination. Clin Biomech (Bristol, Avon) 10:171–178
Carpenter RD, Brilhault J, Majumdar S, Ries MD (2009) Magnetic resonance imaging of in vivo patellofemoral kinematics after total knee arthroplasty. Knee 16:332–336
Chew JT, Stewart NJ, Hanssen AD, Luo ZP, Rand JA, An KN (1997) Differences in patellar tracking and knee kinematics among three different total knee designs. Clin Orthop Relat Res 345:87–98
Ensini A, Catani F, Biasca N, Belvedere C, Giannini S, Leardini A (2011) Joint line is well restored when navigation surgery is performed for total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 20(3):495–502
Ensini A, Catani F, Leardini A, Romagnoli M, Giannini S (2007) Alignments and clinical results in conventional and navigated total knee arthroplasty. Clin Orthop Relat Res 457:156–162
Fu CK, Wai J, Lee E, Hutchison C, Myden C, Batuyong E, Anglin C (2012) Computer-assisted patellar resection system: development and insights. J Orthop Res 30:535–540
Gill HS, O’Connor JJ (1996) Biarticulating two-dimensional computer model of the human patellofemoral joint. Clin Biomech (Bristol, Avon) 11:81–89
Grood ES, Suntay WJ (1983) A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng 105:136–144
Heinert G, Kendoff D, Preiss S, Gehrke T, Sussmann P (2011) Patellofemoral kinematics in mobile-bearing and fixed-bearing posterior stabilised total knee replacements: a cadaveric study. Knee Surg Sports Traumatol Arthrosc 19:967–972
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res 248:13–14
Laprade J, Lee R (2005) Real-time measurement of patellofemoral kinematics in asymptomatic subjects. Knee 12:63–72
Lee PP, Chalian M, Carrino JA, Eng J, Chhabra A (2012) Multimodality correlations of patellar height measurement on X-ray, CT, and MRI. Skeletal Radiol 41(10):1309–1314
Leszko F, Sharma A, Komistek RD, Mahfouz MR, Cates HE, Scuderi GR (2010) Comparison of in vivo patellofemoral kinematics for subjects having high-flexion total knee arthroplasty implant with patients having normal knees. J Arthroplast 25:398–404
Lin F, Makhsous M, Chang AH, Hendrix RW, Zhang LQ (2003) In vivo and noninvasive six degrees of freedom patellar tracking during voluntary knee movement. Clin Biomech (Bristol, Avon) 18:401–409
Merican AM, Ghosh KM, Iranpour F, Deehan DJ, Amis AA (2011) The effect of femoral component rotation on the kinematics of the tibiofemoral and patellofemoral joints after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 19:1479–1487
Moon YW, Seo JG, Yang JH, Shon MS (2008) Analysis of the patellofemoral congruence angle according to the rotational alignment of the femoral component in navigation-guided TKA. Orthopedics 31(10 Suppl 1):62–67
Nha KW, Papannagari R, Gill TJ, Van de Velde SK, Freiberg AA, Rubash HE, Li G (2008) In vivo patellar tracking: clinical motions and patellofemoral indices. J Orthop Res 26(8):1067–1074
Philippot R, Chouteau J, Testa R, Moyen B (2010) In vitro analysis of patellar kinematics: validation of an opto-electronic cinematic analysis protocol. Knee Surg Sports Traumatol Arthrosc 18:161–166
Powers CM, Chen YJ, Scher I, Lee TQ (2006) The influence of patellofemoral joint contact geometry on the modeling of three dimensional patellofemoral joint forces. J Biomech 39:2783–2791
Schindler OS (2012) Basic kinematics and biomechanics of the patellofemoral joint. Part 2: the patella in total knee arthroplasty. Acta Orthop Belg 78:11–29
Schindler OS (2012) The controversy of patellar resurfacing in total knee arthroplasty: ibisne in medio tutissimus? Knee Surg Sports Traumatol Arthrosc 20:1227–1244
Schindler OS, Scott WN (2011) Basic kinematics and biomechanics of the patello-femoral joint. Part 1: the native patella. Acta Orthop Belg 77:421–431
Scuderi GR, Insall JN, Scott NW (1994) Patellofemoral pain after total knee arthroplasty. J Am Acad Orthop Surg 2:239–246
Stagni R, Fantozzi S, Catani F, Leardini A (2010) Can patellar tendon angle reveal sagittal kinematics in total knee arthroplasty? Knee Surg Sports Traumatol Arthrosc 18:949–954
Stiehl JB (2005) A clinical overview patellofemoral joint and application to total knee arthroplasty. J Biomech 38:209–214
Tang TS, MacIntyre NJ, Gill HS, Fellows RA, Hill NA, Wilson DR, Ellis RE (2004) Accurate assessment of patellar tracking using fiducial and intensity-based fluoroscopic techniques. Med Image Anal 8:343–351
van Eijden TM, Kouwenhoven E, Verburg J, Weijs WA (1986) A mathematical model of the patellofemoral joint. J Biomech 19:219–229
Van Kampen A, Huiskes R (1990) The three-dimensional tracking pattern of the human patella. J Orthop Res 8:372–382
Ward SR, Terk MR, Powers CM (2007) Patella alta: association with patellofemoral alignment and changes in contact area during weight-bearing. J Bone Joint Surg Am 89:1749–1755
Wilson NA, Press JM, Koh JL, Hendrix RW, Zhang LQ (2009) In vivo noninvasive evaluation of abnormal patellar tracking during squatting in patients with patellofemoral pain. J Bone Joint Surg Am 91:558–566
Zavatsky AB, Oppold PT, Price AJ (2004) Simultaneous in vitro measurement of patellofemoral kinematics and forces. J Biomech Eng 126:351–356
Acknowledgments
The authors thank Stryker®, Kalamazoo, USA-MI, for its technical and economical support and prof. Fabio Catani, Modena University Hospital, Italy, for the initial discussions on the topic. This work was supported also by the Italian Ministry of Economy and Finance, programme “5 per mille.”
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Belvedere, C., Ensini, A., Leardini, A. et al. Tibio-femoral and patello-femoral joint kinematics during navigated total knee arthroplasty with patellar resurfacing. Knee Surg Sports Traumatol Arthrosc 22, 1719–1727 (2014). https://doi.org/10.1007/s00167-013-2825-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-013-2825-0