
Abstract
Purpose
To study the efficacy of arthroscopic ganglionectomy in the management of ganglia of the foot and ankle.
Methods
From 2006 to 2010, arthroscopic ganglionectomy was performed for 89 ganglia in the foot and ankle of 88 patients. Clinical and intra-operative details were reviewed retrospectively.
Result
Ganglion stalk was identified in 6 % of the cases. The overall rate of presence of pathology was 26 %. The overall rate of recurrence or residual lesion was 12 % with high recurrent rate for extensor tendon ganglia and toe pulp ganglia.
Conclusions
Arthroscopic ganglionectomy of the foot and ankle ganglion by either internal drainage or complete resection is a feasible approach. Good results can be achieved in case of adequate internal drainage of the ganglion to the joints or fibrous tendon sheath.
Level of evidence
Therapeutic, Level IV.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ganglion cysts affect a wide variety of joints of the body, including those of the foot and ankle. Many ganglions are asymptomatic, but pain occurs in 50 % of cases [5]. Compression neuropathy of adjacent nerves has been reported. Initial conservative management of ganglia may entail observation and padding for comfort, aspiration of the cyst contents and injection of steroid or sclerosing agent into the cyst [11, 12, 23, 32]. Surgical resection is the most effective treatment. However, reported rates of recurrence of foot and ankle ganglion cysts range from 7 to 43 % [25, 28, 30]. Moreover, it can be associated with painful or unsightly scar [30]. Arthroscopic ganglionectomy is a well-described technique in wrist ganglion resection [4, 6, 9, 24]. It is a less-invasive surgical alternative with the benefit of visualizing and treating other intra-articular pathology, faster recovery, lower complication and recurrence rates and more satisfying cosmetic results [4, 36].
With the advances in the foot and ankle arthroscopy, arthroscopic ganglionectomy of the foot and ankle become technically feasible [14]. The purpose of this study was to review retrospectively the results of cases with arthroscopic ganglionectomy of ganglia of the foot and ankle in our hospital. It was hypothesized that arthroscopic ganglionectomy is an effective approach in management of ganglia of the foot and ankle.
Materials and methods
From August 2006 to August 2010, arthroscopic ganglionectomy was performed for 89 ganglia in the foot and ankle of 88 patients. The series consisted of 66 female patients and 22 male patients with an average age at operation of 44 years (ranged 16–73 years). The mean follow-up was 31 months (ranged 12–60 months). Six cases were recurrent ganglia after open ganglionectomy, and the remaining 83 cases were primary ganglia without previous surgery. The ganglia were divided into 3 groups of site of origins of the ganglia: joints (Group 1); tendons with fibrous tendon sheath (Group 2) and tendons without fibrous tendon sheath (Group 3). These were further subdivided according to the types of arthroscopy or tendoscopy performed (Table 1). The symptomatology, intra-operative findings, relationship between the origin of the tarsal tunnel ganglia and the tarsal tunnel syndrome, clinical result and complication of each group were studied.
Surgical technique
The approach can be either an endoscopic internal drainage of the ganglion cyst to the adjacent joint or tendon sheath or endoscopic resection of the ganglion cyst. In general, two portals are needed for endoscopic internal drainage. The visualization portal should be close to but not directly over the ganglion [15–20, 24, 33]. The ganglion portal is the portal directly through the ganglion cyst to the planned internal drainage site (Table 1; Fig. 1). For those huge ganglions, the cyst can be outlined by the cable of the diathermy to define how many joints are spanned by the ganglion in order to choose the proper joint for the internal drainage. Sometimes, the optimal location of the ganglion portal should be guided by preoperative MRI study. After the determination of the site of drainage, the visualization portal is made first; ganglion can be lightened by the arthroscope, and the planned ganglion portal site can be located with a needle before skin incision to avoid damage to the nerve and veins. After the establishment of the visualization and ganglion portals, the internal drainage site can be examined for any pathology and treated accordingly. The joint capsule or the tendon sheath adjacent to the ganglion sac is resected to allow adequate internal drainage of the ganglion.

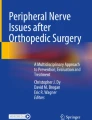
a A lateral tarsometatarsal ganglion was treated by arthroscopic ganglionectomy with P45 as the visualization portal and P34 as the ganglion portal. b Postoperative clinical photos showed good cosmetic results
Endoscopic resection of the ganglion cyst is applicable for ganglia in the retrocalcaneal space that can arise from posterior ankle, posterior subtalar or the flexor hallucis longus tendon. The posterolateral and posteromedial portals at the lateral and medial side of the Achilles tendon, respectively, were used for endoscopic resection of the cyst [34] (Fig. 2).

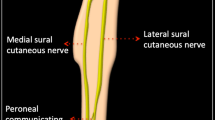
a A case of posteromedial ankle ganglion (a) compressed the posterior tibial nerve causing tarsal tunnel syndrome. b After the resection of the ganglion, the flexor hallucis tendon (b) and the posterior tibial nerve (c) can be seen
For those ganglions arising from the extensor tendons at the foot dorsum or the anterior ankle, which do not have a fibrous tendon sheath, the deep part of the ganglion sac can be resected with an arthroscopic shaver, and the mucinous ganglion fluid is drained to the potential space deep to the extensor tendons [14, 15].
Postoperatively, compression dressing with crepe bandage of the operative site is applied for 4 weeks.
Results
There were 62 Group 1 ganglia, 18 Group 2 ganglia and 9 Group 3 ganglia. The single most common site of origin was the lateral column of the Lisfranc joint (Table 1). Nine tarsal tunnel ganglia were identified, and six of them present with tarsal tunnel syndrome (Table 2).
Stalk of the ganglion was identified in 6 % of the cases: two 1st MTPJ ganglia; one 4th TMTJ ganglion; one flexor hallucis longus (FHL) ganglion at the toe pulp and one ankle joint ganglion. The overall rate of presence of pathology was 26 % (Table 3). The prevalence of the presence of pathology was 100 % for recurrent ganglia after open resection.
The outcome related to the symptomatology was summarized in Table 4.
No wound complication was observed in this series. There were two kinds of complication identified: recurrence/residual lesion and cutaneous nerve injury with numbness or paraesthesia.
The overall rate of recurrence or residual lesion was 12 % (11 cases). The recurrence rate of different group of ganglion was summarized in Table 5. The recurred ganglia were resected openly except in 2 patients with EDL ganglia as they refused further operation.
Cutaneous nerve injury with numbness or paraesthesia was present in four patients (4 %) including 1 case of EDL ganglion at the ankle level (intermediate branch of superficial peroneal nerve), 1 case of EDL ganglion at the foot dorsum (intermediate branch of superficial peroneal nerve), 1 case of 1st tarsometatarsal joint ganglion (deep peroneal nerve) and 1 case of 1st metatarsophalangeal joint ganglion at the plantar medial side (plantar medial digital nerve).
Discussion
The most important finding of the present study was that arthroscopic ganglionectomy is a feasible approach for foot and ankle ganglion.
Ganglion of the foot and ankle can originate from various joints and tendon sheaths [2, 3, 7, 8, 10, 15, 16, 27, 35], and most common present as foot dorsum lump [1, 21], which was coherent to the finding of this series. It is because the dorsal capsuloligamentous structure is weaker and the ganglion is easier to erupt from the dorsum of the joint and the joints are superficial at the dorsum making any dorsal lump easily visible. Similarly, the first metatarsophalangeal joint ganglion will present at the proximal plantar medial aspect rather than at the distal plantar aspect of the joint because of the proximal insertion of the plantar plate is thinner than the distal insertion.
It is important to differentiate whether the foot dorsum ganglion arises from the joint or the extensor tendons. Foot dorsum ganglion arising from the joint will have the cutaneous nerves superficial to it and will not be damaged during the resection of the deep part of the ganglion cyst and the joint capsule. Ganglion arising from the extensor tendon will have the nerves superficial or deep to it, and there will be risk for nerve damage during the arthroscopic ganglionectomy. Unlike ganglion from the joint or fibrous tendon sheath that is usually present as a discrete roundish lump, ganglion from the extensor tendons is a diffuse distension of the synovial lining and present as a soft sausage like lesion with the long axis of the lump in line with the extensor tendons and move with the extensor tendons (Supplementary material 1). Extensor tendon ganglion at the ankle will present as a dumbbell lesion as the ganglion cyst is constricted at the waist by the superior extensor retinaculum with apparently positive emptying sign (Supplementary material 2). Similar dumbbell ganglion was observed at the medial ankle underneath the medial malleolus. If the ganglion cyst is emptyable, compression of the site of origin can cause reappearance of the cyst (Supplementary material 3).
Magnetic resonance imaging was indicated in cases of uncertain diagnosis [27], tarsal tunnel ganglion, planning of the optimal location of the ganglion portal, posterior ankle or plantar ganglion, foot dorsum ganglion that covered the area of the intermetatarsal space and toe pulp ganglion. It is useful for the identification of the site of origin and study of the relationship between the posterior ankle or plantar ganglion and the surrounding neurovascular structures. It is important to identify the site of origin of the tarsal tunnel ganglion and the relation between the nerve and the ganglion in order to choose the appropriate arthroscopic approach. MRI can detect any deep extension of the foot dorsum ganglion through the intermetatarsal space [29, 31]. The deep extension should be addressed during arthroscopic ganglionectomy, and tarsometatarsal joint is the best site of drainage for this kind of ganglion. MRI is also important for preoperative planning of the toe pulp ganglion because of the high chance of multilobulation and off-site from the flexor tendon sheath. Multilobulation of the ganglion cyst is not a contraindication for arthroscopic ganglionectomy but should be defined in details by clinical examination or MRI. The septa of all the lobulations should be broken down during the operation to allow adequate drainage of all the chambers. However, in contrast to the common nodular type of multilobulation (Supplementary material 4), the chain-type is contraindicated for arthroscopic procedure as adequate drainage of all chambers seems impossible.
Intra-operatively, the site of origin may be determined by shrinkage of the ganglion cyst by aspiration and then injection of normal saline to the expected site of origin (Supplementary material 5).
Resection of the intra-articular cyst opening during internal arthroscopic drainage was proposed to eliminate the valvular mechanism [22]. Although adequate ganglion stalk visualization and resection has been emphasized for surgical treatment of wrist ganglion in order to minimize the risk of recurrence, it can be identified in only 10 % of patients with arthroscopic or open resection of wrist ganglia [4, 36]. Unlike the quite constant intra-articular pathology of wrist ganglion, most ganglia of the foot and ankle do not communicate with the joint space [26], and stalk can only be identified in 6 % of cases in this series. Therefore, the aim of arthroscopic ganglionectomy of the foot and ankle is the establishment of an adequate passage to a drainage site of adequate draining potential, which may not be the site of origin of the ganglion rather than resection of the ganglion stalk or breakage of the valvular mechanism. It is particular true in case of huge foot dorsum ganglion that may span several joints and the site of origin cannot be identified. Postoperative compression dressing is an essential component of success for internal drainage. However, it is not effective for the ganglion in the retrocalcaneal space. Instead, the presence of a potential space allows complete resection of the cyst through the retrocalcaneal endoscopy.
Prevalence of pathology was much higher in revision cases than primary cases. It can be the result of previous operation rather than the source of recurrence. Moreover, the prevalence in primary cases may be underestimated because the site of drainage may not be identical to the site of origin especially for huge foot dorsum ganglion.
Although there was no significant relationship between location of the cyst and recurrence after the open resection [25], it is not the case in arthroscopic ganglionectomy. Ganglia arisen from the extensor tendons or the end of flexor hallucis longus tendon sheath (present as toe pulp ganglion) had a high recurrence rate. The apparent high recurrence rate of intercuneiform joint ganglion was due to its rarity and one case of misdiagnosis as EDL ganglion. The high recurrence rate of extensor tendon ganglion implied that the deep potential space is not a good drainage site. Drainage to the adjacent joints is not be feasible especially at the ankle level as the extensor tendons have the tendency of bowstring and away from the anterior ankle capsule. Moreover, the large excursion of the extensor tendons and the ganglion sac during ankle and toe motion made a stable drainage to the joint impossible. Complete resection of the ganglion sac is possible but is risky to the surrounding cutaneous nerve. The toe pulp ganglia of the hallux were usually multiloculated. The main body of the ganglion was usually at the side of the distal end of the flexor tendon sheath, probably because of pressure applied to the ganglion during walking. It was therefore difficult to establish an adequate drainage to the flexor tendon sheath and lead to a high recurrence rate. Finally, the recurrence rate may be underestimated because recurrence of small deep-seated ganglion at the posterior ankle or sole may be missed.
Revision surgery for recurrent foot and ankle ganglion tends to be more difficult than the initial treatment, resulting in increased postoperative pain, high rates of recurrence and lower patient satisfaction [23]. Management of recurrent ganglia has focused on complete ganglion resection and tract obliteration, with attention to treatment of underlying disorders of joints, bones and tendons [28], which can result in damage to or exposure of adjacent structures or the structures from which the ganglia arise [13, 25, 28]. Arthroscopic management of the revision cases has the advantage of internal drainage of the cyst and treatment of the underlying disorders of the joints and tendons without the risk of extensive soft tissue dissection. This can lead to good clinical result as shown in this series.
The limitation of this study is that it is a retrospective study without a control group for comparison. Moreover, the relatively small numbers of cases of individual site make it difficult to draw conclusion of its effectiveness of each site.
The clinical relevance of this study is that it provides the clinical guide for arthroscopic ganglionectomy of the foot and ankle.
Conclusion
Arthroscopic ganglionectomy of the foot and ankle ganglion by either internal drainage or complete resection is a feasible approach. Good results can be achieved in case of adequate internal drainage of the ganglion to the joints or fibrous tendon sheath.
References
Ahn JH, Choy WS, Kim HY (2010) Operative treatment for ganglion cysts of the foot and ankle. J Foot Ankle Surg 49:442–445
Antoniadis G, Scheglmann K (2008) Posterior tarsal tunnel syndrome: diagnosis and treatment. Dtsch Arztebl Int 105:776–781
Casal D, Bilhim T, Pais D, Almeida MA, O’Neill JG (2010) Paresthesia and hypesthesia in the dorsum of the foot as the presenting complaints of a ganglion cyst of the foot. Clin Anat 23:606–610
Edwards SG, Johansen JA (2009) Prospective outcomes and associations of wrist ganglion cysts resected arthroscopically. J Hand Surg 34A:395–400
Friedli A, Saurat JH, Harms M (2002) Serpiginous ganglion cyst of the foot mimicking cutaneous larva migrans. J Am Acad Dermatol 47:S266–S267
Gallego S, Mathoulin C (2010) Arthroscopic resection of dorsal wrist ganglia: 114 cases with minimum follow-up of 2 years. Arthroscopy 26:1675–1682
Green MR, Yanklowitz B (1992) Asymptomatic naviculocuneiform synostosis with a ganglion cyst. J Foot Surg 31:272–275
Haslam ET (1952) Posterior ganglion at the ankle: a case report. Am Surg 18:191–194
Ho PC, Lo WN, Hung LK (2003) Arthroscopic resection of volar ganglion of the wrist: a new technique. Arthroscopy 19:218–221
Huang JI, Gilmore A (2007) Ganglion cysts of the midfoot presenting as bilateral accessory tarsal navicular bones in a child: a case report. Foot Ankle Int 28(5):621–623
Kenjiro Nakama K, Gotoh M, Mitsui Y, Shirachi I, Higuchi F, Nagata K (2010) Use of autologous fibrin sealants to treat ganglion cysts: a report of two cases. J Orthop Surg 18:104–106
Kiehn MW, Gutowski KA (2004) A recurrent foot ganglion managed with extensor digitorum brevis muscle flap coverage. J Foot Ankle Surg 43:423–425
Kliman ME, Freiberg A (1982) Ganglia of the foot and ankle. Foot Ankle 3:45–46
Lui TH (2007) Arthroscopy and endoscopy of the foot and ankle: indications for new techniques. Arthroscopy 23:889–902
Lui TH (2011) Extensor tendoscopy of the ankle. Foot Ankle Surg 17:e1–e6
Lui TH (2009) Flexor hallucis longus tendoscopy: a technical note. Knee Surg Sports Traumatol Arthrosc 17:107–110
Lui TH (2006) New technique of arthroscopic triple arthrodesis. Arthroscopy 22:464.e1–464.e5
Lui TH (2007) Arthroscopic tarsometatarsal (Lisfranc) arthrodesis. Knee Surg Sports Traumatol Arthrosc 15:671–675
Lui TH, Chan KB, Ng S (2005) Arthroscopic lapidus arthrodesis. Arthroscopy 21:1516.e1–1516.e4
Lui TH (2008) Clinical tips: anterior subtalar (talocalcaneonavicular) arthroscopy. Foot Ankle Int 29:94–96
MacDonald DJM, Holt G, Vass K, Marsh A, Kumar CS (2007) The differential diagnosis of foot lumps: 101 cases treated surgically in North Glasgow over 4 years. Ann R Coll Surg Engl 89:272–275
Nishikawa S, Toh S (2004) Arthroscopic treatment of a ganglion of the first metatarsophalangeal joint. Arthroscopy 20:69–72
Ogose A, Hotta T, Kawashima H, Endo N (2007) A painful large ganglion cyst of the ankle treated by the injection of OK-432. Mod Rheumatol 17:341–343
Osterman AL, Raphael JS (1995) Arthroscopic resection of dorsal ganglion of the wrist. Hand Clin 11:7–12
Pontious J, Good J, Maxian SH (1999) Ganglions of the foot and ankle. A retrospective analysis of 63 procedures. J Am Podiatr Med Assoc 89:163–168
Rawool NM, Nazarian LN (2000) Ultrasound of the foot and ankle. Semin Ultrasound CT MRI 21:275–284
Rodriguez NN, Blitz NM (2008) Hemorrhagic ganglion of the tibialis anterior tendon: report of an unusual variant. J Foot Ankle Surg 47:571–575
Rozbruch SR, Chang V, Bohne WH, Deland JT (1998) Ganglion cysts of the lower extremity: an analysis of 54 cases and review of the literature. Orthopedics 21:141–148
Saeva JT, Kaye MR (1995) Presentation of an intermetatarsal ganglion. J Am Podiatr Med Assoc 85:274–276
Slavitt JA, Beheshti F, Lenet M, Sherman M (1980) Ganglions of the foot: a six-year retrospective study and a review of the literature. J Am Podiatr Assoc 70:459–465
Talawadekar GD, Damodaran P, Jain SA (2010): Hourglass ganglion cyst of the foot: a case report. J Foot Ankle Surg 49:489.e11–489.e12
Tanaka Y, Takakura Y, Kumai T, Sugimoto K, Taniguchi A, Hattori K (2009) Sclerotherapy for intractable ganglion cyst of the hallux. Foot Ankle Int 30:128–132
van Dijk C, Kort N (1998) Tendoscopy of the peroneal tendons. Arthroscopy 14:471–478
van Dijk CN, Scholten PE, Krips R (2000) A 2-portal endoscopic approach for diagnosis and treatment of posterior ankle pathology. Arthroscopy 16:871–876
Warren RF (1980) Ganglion of the sunus tarsi. A case report. Am J Sports Med 8:133–134
Yao J, Trindade MCD (2011) Color-aided visualization of dorsal wrist ganglion stalks aids in complete arthroscopic excision. Arthroscopy 27:425–429
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Video 1: The extensor tendon ganglion moved with the toe motion. Supplementary material 1 (AVI 23752 kb)
Video 2: A case of extensor tendon ganglion at the ankle level. Apparently positive emptying sign was observed as the fluid was squeezed to the other side of the dumbbell lump. Supplementary material 2 (AVI 28687 kb)
Video 3: A case of sinus tarsi ganglion which present as a lump at anterior ankle. The lump can be emptied and refilled with compression at the sinus tarsi. Supplementary material 3 (AVI 26889 kb)
Video 4: A case of nodular type mutliloculation of syndesmosis ganglion. Supplementary material 4 (AVI 20471 kb)
Video 5: A case of first metatarsophalangeal ganglion. The gelatinous fluid of the cyst was aspirated. Normal saline was injected into the joint and the cyst refilled. Supplementary material 5 (AVI 7682 kb)
Rights and permissions
About this article
Cite this article
Lui, T.H. Arthroscopic ganglionectomy of the foot and ankle. Knee Surg Sports Traumatol Arthrosc 22, 1693–1700 (2014). https://doi.org/10.1007/s00167-012-2065-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-012-2065-8