
Abstract
We describe an arthroscopic approach of tarsometatarsal arthrodesis for post-traumatic arthritis. Five tarsometatarsal portals (medial, P1–2, P2–3, P3–4, P4–5) are identified at the junctional points between the metatarsals by means of image intensifier. The first metatarsocuneiform joint is approached through the medial and P1–2 portal. Articular cartilage is denuded and micro-fracture of subchondral bone is performed with an arthroscopic awl. The second metatarsocuneiform joint is approached through the P1–2 and P2–3 portals and the third metatarsocuneiform joint is approached through the P2–3 and P3–4 portals. The articular surfaces are prepared for arthrodesis. The articulations are kept in desired position and transfixed with 4.0 mm cannulated screws. The fourth and fifth metatarsocuboid articulations are rarely included in the procedure. Arthroscopic arthrodesis or tendon arthroplasty of the lateral column can be performed through the P3–4 and P4–5 portals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fracture dislocation of the tarsometatarsal joint complex is usually associated with high energy although it may be seen in association with minimal trauma from minor twisting injuries, particular in athletes and the elderly [1]. Post-traumatic arthritis is the most common problem after injuries to the tarsometatarsal joint. Post-traumatic arthritis may be treated initially with non-operative measures of non-steroidal anti-inflammatory drugs, insoles and shoewear modification. If conservative management failed to relieve the symptoms, arthrodesis of the painful tarsometatarsal joints is the treatment of choice. We present an arthroscopic approach of tarsometatarsal arthrodesis.
Portal anatomy
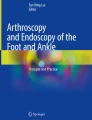
Five tarsometatarsal portals are designed to approach the five tarsometatarsal articulations (Fig. 1). The first metarsocuneiform joint is approached through medial portal which is located at the plantar medial aspect of the first metatarsocuneiform joint and the P1–2 portal which is located at the junction point between medial cuneiform, first and second metatarsal bones. The second metatarsocuneiform joint is approached through the P1–2 portal and the P2–3 portal which is located at the junction point between the second metatarsal, intermediate and lateral cuneiform bones. The third metatarsocuneiform joint is approached through the P2–3 portal and the P3–4 portal which is located at the junction point between lateral cuneiform and cuboid and third and fourth metatarsal bones. The fourth and fifth metatarsocuboid joints can be approached through the P3–4 portal and the P4–5 portal which is located between the proximal articular surfaces of the fourth and fifth metatarsal. Besides the medial portal, the other four portals are “junction portals” with the capability of approaching the adjacent articulation. Moreover, these portals can be used to approach the intercuneiform spaces and spaces between the proximal parts of metatarsal bones. This can allow debridement and release of these spaces in order to facilitate reduction of the Lisfranc joint in both sagittal and transverse planes. For example, the first and second metatarsocuneiform joints can be approached through the P1–2 portal. The spaces between medial and intermediate cuneiform and between first and second metatarsals can be approached through the same portal.

Five tarsometatarsal portals are designed to approach the five tarsometatarsal articulations. The first metatarsocuneiform joint is approached through medial portal (A) which is located at the plantar medial aspect of the first metatarsocuneiform joint and the P1–2 portal (B) which is located at the junction point between medial cuneiform, first and second metatarsal bones. The second metatarsocuneiform joint is approached through the P1–2 portal and the P2–3 portal (C) which is located at the junction point between the second metatarsal, intermediate and lateral cuneiform bones. The third metatarsocuneiform joint is approached through the P2–3 portal and the P3–4 portal (D) which is located at the junction point between lateral cuneiform and cuboid and third and fourth metatarsal bones. The fourth and fifth metatarsocuboid joints can be approached through the P3–4 portal and the P4–5 portal (E) which is located between the proximal articular surfaces of the fourth and fifth metatarsal. Through these portals, the whole tarsometatarsal articulation (narrow arrows) and the longitudinal intertarsal articulation and intermetatarsal spaces (broad arrows) can be approached. These allow realignment of the forefoot in both sagittal and transverse plane before arthrodesis
Description of technique
Patient is put in supine position with pneumatic tourniquet applied to the thigh. No traction device is required. The five tarsometatarsal portals are identified under image intensifier. Portals are established by cut open the skin followed by blunt dissection of subcutaneous tissue with haemostat. The first metatarsocuneiform joint is approached with the same technique as arthroscopic Lapidus arthrodesis [2]. The P1–2 portal is slightly lateral to that of dorsomedial portal in arthroscopic Lapidus arthrodesis. An 2.7 mm 30° arthroscope is introduced to visualize the joint and the joint is debrided with arthroscopic shaver. The remaining articular cartilage is denuded by means of arthroscopic osteotome and small periosteal elevator and the subchondral bone is left intact. Micro-fracture of the subchondral bone is then performed by means of arthroscopic awls.
Because of the elasticity of the dorsal skin of the foot, the P1–2 portal skin wound is retracted proximally to approach the second metatarsocuneiform joint. Sometimes it is difficult to identify the tarsometatarsal joints of the lesser rays. It is helpful to identify and locate the joint by means of a needle under image intensifier and then perform the arthroscopy again with the needle as the landmark. With the arthroscope at the P1–2 portal, the dorsal capsule is then released with arthroscopic shaver at the P2–3 portal. The cartilage is denuded with arthroscopic osteotome and small periosteal elevator and the subchondral bone is left intact. Micro-fracture of the subchondral bone is then performed by means of arthroscopic awls (Fig. 2). The third metatarsocuneiform joint can be approached with the P2–3 and P3–4 portal. The fusion surfaces can be prepared as described above. The three joints is reduced into desired position and transfixed with 4.0 mm cannulated screws. Cancellous bone graft can be packed into the fusion site through the portals with the aid of a small bone trephine.

A needle is inserted into the target lesser ray tarsometatarsal articulation under image intensifier and arthroscopy is performed with the needle as the landmark (a). This can facilitate the identification of the joint by arthroscopy. After dorsal capsulotomy, the articular cartilage is debuded with an arthroscopic osteotome under arthroscopic guide (b). After articular cartilage debridement (c), micro-fracture of the subchondral bone is performed with arthroscopic awl (d)
Occasionally, there is degeneration of the fourth and fifth metatarsocuboid joints which are recalcitrant to non-operative management. These joints can be approached with P3–4 portal and P4–5 portal which is medial to the peroneal tertius. Either arthrodesis [3] or tendon arthroplasty [4] of these joints can be performed. Arthrodesis is performed similar to that described above. In case of tendon arthroplasty of these joints, the peroneal tertius tendon is identified through the P4–5 portal and the tendon is released proximally through a proximal stab wound. The tendon is then retracted to the P4–5 portal. The joints are debrided with arthroscopic shaver and burr at the P4–5 portal under arthroscopic guide at P3–4 portal. A trough is created at the joints with preservation of ligamentous structures. The tendon graft is then rolled up and inserted into the trough through the P4–5 portal and stabilized with K wire.
Post-operative, a short leg cast is put on and patient is advised on non-weight bearing walking for 8–12 weeks.
Case illustration
A 46-year-old lady had history of left foot injury after fall from height in 1982. She was treated with traditional Chinese medicine. It took a year of sick leave before she resumed duty as a factory worker. She noticed on and off left foot pain afterwards. Her left foot pain deteriorated in recent years, so that she cannot bear weight on her left forefoot. Clinically, there is a big bony prominence at medial side of midfoot dorsum, which was non-tender and not inflamed. Passive pronation and abduction of her left foot [5] reproduced the pain, which was located at the first to third metatarsocuneiform joint. X-rays showed degeneration of first to third metatarsocuneiform joints of her left foot with huge dorsal osteophyte at first metatarsocuneiform joint (Fig. 3). Conservative management of insoles, shoewear modification and physiotherapy had been tried but failed to relieve the pain. Arthroscopic Lisfranc arthrodesis of first to third metatarsocuneiform joints was performed. Post-operatively, a short leg cast was put on. Cast was removed on 8 weeks after the operation and the patient was allowed to have weight bearing walking with a rocker boot for another 4 weeks. X-rays showed good union of the fusion sites (Fig. 4). At 20 months of follow-up, her left foot pain subsided.

Preoperative clinical photos (a, b) and X-rays (c, d) of the patient’s left foot

Clinical photos (a, b) and X-rays (c, d) of the patient’s left foot 20 months after operation
Discussion
The tarsometatarsal articulation can be considered as a combination of three columns [5]. The medial column consists of the first metatarsocuneiform joint. The middle column consists of the second and third metatarsocuneiform joints. The lateral column consists of the fourth and fifth metatarsocuboid joints. Traumatic arthritis of the tarsometatarsal articulation can be present with any combination of the three columns. There may be some difficulty in identifying the painful joints, but the middle column and to a less extent the medial column are the most commonly involved [6]. Tarsometatarsal arthrodesis is the treatment of choice for symptomatic tarsometatarsal arthritis resistant to conservative management. In view of the success of arthroscopic arthrodesis procedures in ankle, subtalar [7], metatarsophalangeal [8], first metatarsocuneiform [2] joint and even triple arthrodesis [9], we extend the technique to arthroscopic tarsometatarsal arthrodesis. With the help of small joint arthroscopy, we can debride the joint and articular cartilage with preservation of the subchondral bone. This may reduce the risk of malunion and non-union. The medial column arthrodesis is identical to the arthroscopic Lapidus arthrodesis [2]. The progression of the joint line from one articulation to another is not smooth. There are two abrupt transitions. The first is between the first and second metatarsocuneiform joints and the second offset lies between the second and third metatarsocuneiform joints [10]. Because of the elasticity of the dorsal skin of the foot, the P1–2 and P2–3 portal can be retracted proximally and distally to approach the second and third metatarsocuneiform joints. Moreover, the design of the P1–2, P2–3, P3–4, and P4–5 portals at the junction points between the metatarsals allows debridement, release and anatomical reduction of the individual rays in both transverse and sagittal plane. This allows arthrodesis with realignment of the forefoot rather than arthrodesis in situ.
The lateral column arthritis usually does not cause significant symptoms, probably because it is the most mobile in both the sagittal and horizontal planes [11]. Inclusion of these articulations is not recommended for routine tarsometatarsal arthrodesis. In case of uncorrectable lateral midfoot collapse, lateral column arthrodesis can be performed through the P3–4 and P4–5 portals. In those patients with painful arthritis of the lateral column, we preferred tendon arthroplasty rather than arthrodesis in order to maintain certain degree of mobility of the lateral column.
References
Curtis MJ, Myerson MS, Szura B (1993) Tarsometatarsal joint injuries in the athlete. Am J Sports Med 21:497–502
Lui TH, Chan KB, Ng S (2005) Technical note: arthroscopic Lapidus arthrodesis. Arthroscopy 21(12):1516e1–1516e4
Raikin SM, Schon LC (2003) Arthrodesis of the fourth and fifth tarsometatarsal joints of the midfoot. Foot Ankle Int 24(8):584–590
Berlet GC, Anderson RB (2002) Tendon arthroplasty for basal fourth and fifth metatarsal arthritis. Foot Ankle Int 23(5):440–446
Komenda GA, Myerson MS, Biddinger KR (1996) Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 78-A:1665–1676
Myerson MS (1999) The diagnosis and treatment of injury to the tarsometatarsal joint complex. J Bone Joint Surg Br 81-B(5):756–763
Scranton PE Jr (1999) Comparison of the open isolated subtalar arthrodesis with autogenous bone graft versus outpatient arthroscopic subtalar arthrodesis using injectable bone morphogenous protein-enhanced graft. Foot Ankle Int 20(3):162–165
Perez Carro L, Busta Vallina B (1999) Arthroscopic-assisted first metatarophalangeal joint arthrodesis. Arthroscopy 15(2):215–217
Lui TH (2006) New technique: arthroscopic triple arthrodesis. Arthroscopy 22(4):464e1–464e5
Early JS, Bucholz RW (1996) Lisfranc injuries and their management. Curr Orthop 10:169–173
Ouzounian TJ, Shereff MJ (1989) In vitro determination of midfoot motion. Foot Ankle 10:140–146
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lui, T.H. Arthroscopic tarsometatarsal (Lisfranc) arthrodesis. Knee Surg Sports Traumatol Arthrosc 15, 671–675 (2007). https://doi.org/10.1007/s00167-006-0142-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-006-0142-6