
Abstract
Purpose
Anteroposterior knee stability is a relevant factor for the decision-making process of various surgical procedures. In degenerative joints when the implantation of unicompartimental prostheses or corrective osteotomies of the limb are planned, the integrity of the anteroposterior stability with an intact ACL has been regarded as a necessary prerequisite. We hypothesise that joint degeneration, however, may influence the anteroposterior knee laxity. Therefore, we set out to test this hypothesis simulating a progressively ‘degenerated’ joint in an experimental cadaveric setting.
Methods
Twelve intact transfemorally resected Thiel-fixated cadaver knee joints were divided into 2 groups for manipulation in the medial or lateral compartment. In each knee, we performed (1) unilateral total meniscectomy; (2) simulation of advanced osteoarthritis, by unilateral total cartilage debridement; (3) simulation of a unilateral tibial impression fracture, by resection of 5 mm of the tibial plateau; (4) transection of the ACL. The KT-1000 arthrometer was used to measure the extent of anteroposterior translation at 30° of knee flexion.
Results
The mean value for tibial anteroposterior translation before intervention was 3.2 mm (SD: ±0.8). The mean translation after each intervention was 4.6 mm (SD: ±0.9; +44%; n.s.) after meniscectomy, 5.9 mm (SD: ±1.5; +84%; P < 0.05) after cartilage debridement, 8 mm (SD: ±1.5; +150%; P < 0.01) after bone debridement, and finally 9.7 mm (SD: ±2.2; +203%; P < 0.05) after resection of the ACL. There were no significant differences between the medial and lateral compartment.
Conclusion
In absence of massive osteophytes or capsular shrinkage, rapid loss of meniscus, cartilage and particularly loss of subchondral bone may result in a massive increase in anteroposterior translation, mimicking a tear of the ACL. In such a situation, a false positive impression of a ligamentous injury may arise, and decision making is falsely directed away from totally or partially knee joint-preserving procedures. Therefore, in degenerate joints, clinical evaluation of anteroposterior stability should rather rely on the presence of a firm stop than an overall increased joint translation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Clinical evaluation of anteroposterior knee stability can be challenging, even for the experienced examiner. It usually includes the assessment of the overall translation and the finding of a firm stop of the translation, corresponding to the resistance of intact ligamentous structures. The integrity of these ligaments is important in the decision making of various surgical procedures. Also in the treatment of degenerative joints, where meniscal transplantation, corrective osteotomies or unicompartimental knee prosthesis are considered, the sagittal stability has to be taken into account. Several anatomical structures contribute to the anteroposterior stability, such as the cruciate ligaments, the joint capsule with the incorporated ligaments [6], the menisci [16, 17] and the active tension of the surrounding musculature [18]. Further, geometrical factors as shape of the joint, particularly the posterior slope of the tibial plateau, influence relevant joint stability [10]. However, all ligamentous structures, which connect the femur with the tibia, have to cross the joint line at a certain angle. Therefore, their line of action is not exactly parallel with the direction of the anteroposterior translatory movement. The effect of the loss of the above-mentioned structures on varus/valgus laxity is well known [20, 21]. The effect of the sagittal stability in late stage of a long-standing osteoarthritis is also described [5, 9]. However, in case of rapid progression of cartilage loss (i.e. after trauma or infection), where compensating mechanisms like formation of osteophytes are missing, the sagittal stability may be otherwise influenced. Therefore, we hypothesised that loss of joint space beyond the known effect of meniscal resection will decrease the distance between insertion points of the stabilising ligaments with a consecutive slack of the corresponding ligaments and capsule.
Goal of the study was to test the above-described hypothesis regarding the anteroposterior laxity simulating a progressively ‘degenerated’ joint in an experimental cadaveric setting.
Material and method
Sixteen transfemorally resected, Thiel-fixated [24] lower limbs, including two-thirds of the femoral bone and soft tissue, were prepared for the purpose of this study. The specimens were obtained from thirteen donors, including three matched pairs. A fixation device was constructed to allow arthroscopic treatment of the knee joints. Two Steinman pins were transversely placed in the distal diaphysis of the femur and clamped in the brackets of the fixation device. Arthroscopy was performed using two standard (anteromedial and anterolateral) portals. First, in all available knees, a diagnostic arthroscopy was performed to evaluate integrity of the menisci, the cartilage and the anterior cruciate ligament. Cartilage degeneration more than grade 2 according to Outerbridge, relevant osteophytic appositions, or ACL deficient knees were excluded. Four specimens had to be excluded as follows: two with advanced cartilage degeneration, one due to ACL deficiency and one because of a supracondylar fracture after Steinman pin insertion.
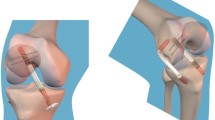
Finally, 12 intact cadaveric knee joints were available for further testing. The specimens were randomly divided into two groups of 6 knees. In the first group, the manipulation was performed only in the medial compartment, in the second group only in the lateral. The adding procedure for the selected compartment was standardised. All interventions were performed arthroscopically with meniscal resectors or motorised shavers, respectively, in order to minimise a destabilising effect caused by the surgical approach. First, a unilateral total meniscectomy was performed; second, simulation of advanced osteoarthritis by unilateral total cartilage debridement till subchondral bone was performed using a 5.5-mm serrated shaver blade; third, simulation of a unilateral tibial bone loss, by resection of 5 mm of the tibial plateau sloping posteriorly using a 5.5-mm oval burr; finally, transection of the ACL was performed. Figure 1 illustrates the medial compartment after each intervention. Under slight varus/valgus compression, anteroposterior radiographs were taken to confirm the corresponding cartilage or bone loss. Cartilage resection was considered completed, if the joint space was total narrowed.

Illustrations of the medial knee compartment before and after each intervention: First, a unilateral total meniscectomy was performed. Advanced osteoarthritis was simulated by unilateral total cartilage debridement. Finally, a unilateral tibial impression fracture was simulated by resection of 5 mm of the tibial plateau
The KT-1000 arthrometer (Medmetric Corporation, San Ciego, CA) was used to measure the extent of anteroposterior translation of the tibia to the femur. The same surgeon performed all measurements. The arthrometer was secured to the lower limb with the two dedicated Velcro straps, and the two sensing pads were positioned on the patella and on the tibial tubercle according to the manufacturer’s instructions. The anterior translation is the relative movement between the two pads, with a precision of 1 mm. The standardised measurement position was in 30° of flexion and neutral rotation of the tibia. A goniometer was used for correct angel positioning. Measurements were performed with a pressure of 30 pounds (133°N) [7, 14, 23].
In order to evaluate intraobserver agreement, two pre-intervention measurements were performed, one after diagnostic arthroscopy and the other one immediately prior to the primary intervention with at least 1 day in between. The mean of this two pre-intervention measurements functioned as the baseline value. Further tests were performed in exactly the same manner after each intervention. Care was taken to drain the knee before measurement, because effusions can have an effect on the measurement result [27].
Statistical analysis
Statistical analysis was performed with the software PRISM (PRISM 4 for Macintosh, Version 4.0c, Graphpad Inc) and R (R Development Core Team 2010) by a medical statistician. An analysis according to Bland and Altman was used to assess agreement between the two pre-intervention measurements. Normality was tested by the Kolmogrov–Smirnov test before applying the Mann–Whitney for statistical comparison between the lateral and the medial side at each of the time points. Due to lack of statistical differences between the lateral and medial side, the data were pooled for analysis of inter time point measures by means of one way ANOVA with either Bonferonni or Dunnett’s Posthoc test. All tests were performed at a significance level of alpha = 0.05, and confidence intervals were computed at a confidence level of 95%.
Results
The mean body donors age in the medial and lateral compartment group was 77 (SD: ±16) years and 79 (SD: ±11) years, respectively. There were 3 right and 3 left in the medial and 2 right and 4 left in the lateral compartment group. Gender distribution was 5:1 (f:m) in both groups.
Result of the Bland–Altman analysis provided differences between the two pre-intervention measurements within limits of agreement, so they can be used interchangeably.
The mean value for tibial translation before intervention was 3.2 mm (SD: ±0.8). The absolute mean translation after each intervention was 4.6 mm (SD: ±0.9; +44%; n.s.) after meniscectomy, 5.9 mm (SD: ±1.5; +84%; P < 0.05) after cartilage debridement, 8 mm (SD: ±1.5; +150%; P < 0.01) after fracture simulation (bone debridement), and finally 9.7 mm (SD: ±2.2; +203%; P < 0.05) after resection of the ACL. The mean increase of each intervention on the previous was +1.3 mm (28%; P < 0.01) after cartilage debridement following meniscectomy, +2.1 mm (36%; P < 0.01) after fracture simulation following cartilage debridement, and finally +1.7 mm (21%; P < 0.05) after transection of the ACL following fracture simulation (Table 1; Fig. 2).

Illustration of the anteroposterior tibial translation after each intervention. Statistically significant differences are marked. There was no significant difference between the medial and lateral compartment
There were no significant differences between the medial and lateral compartment when comparing the influence of the interventions on the anteroposterior translation (Table 2; Fig. 2).
Discussion
The most important finding of the present study was that loss of menisci, cartilage and subchondral bone influences gradually the anteroposterior stability in the knee joint. Therefore, the results did mostly confirm the hypothesis. The increase of instability in the stepwise procedure was, however, not a linear. Meniscectomy alone had a relatively small and non-significant effect, which is consistent with earlier reports [16, 17]. The increase between meniscectomy to cartilage debridement and further to bone resection was, however, significant. Interestingly, there was no significant difference between the procedures performed medially or laterally. However, this effect of increasing anteroposterior translation in degenerated joints has to our knowledge not been described before and may have an important clinical relevance.
Because the assessment of the anteroposterior stability is an integral part of every physical examination of the knee, an increased translation compared to an intact opposite side or absolute translations of more than 6–10 mm [8, 14, 19] is considered as a sign of anterior ligament insufficiency and knee instability. The integrity of the anterior cruciate ligament has been regarded as a necessary prerequisite [3, 11, 25] for the implantation of unicompartimental prostheses or corrective osteotomies of the limb. Knee instability may, therefore, be a contraindication for various procedures in the degenerative joint. However, our hypothesis that the rapid loss of joint space (meniscus and cartilage) and also loss of subchondral bone may have an indirect influence on anteroposterior laxity due to loss of tension on the knee stabilising ligaments and capsule was confirmed.
It is reasonable to assume that in the late stage osteoarthritic knee, this findings may not be found, as there are other, in part competing factors during joint degeneration, such as the stabilising effect of osteophyte formation [20] or contracture and tightness of the ligaments or capsular structures [5]. Cartilage loss occurs usually gradually but can be rapid in some cases, like trauma with osteochondral lesions or septic gonarthritis, which, however, may favour a destabilisation due to wearing out of ligaments around the knee [26]. It may further be speculated and investigated in future studies that not all patients react identically to loss of cartilage, as also not all patients form osteophytes in the same amount or at all. Also an altered tibial slope may be of importance and further increase the observed effect [10].
This study has some limitations. First, the cadaveric setting: even though accepted as a fixation method in mechanical tests, Thiel fixation may influence and most likely decrease general ligament flexibility [13]. Therefore, the tests may underestimate the actual knee laxity. Another factor is the measurement method. The KT-1000 is a widely accepted and valid tool for the instrumented measurement of the anteroposterior tibial translation not only in the clinical environment [2, 14, 19, 22, 28] but also in cadaveric testing [1, 4, 15, 27] but does rely on pressure on soft tissue (skin and subcutaneous fat) and is, therefore, prone to some variability. Still repeatability was in a very favourable range and appeared reasonable. In a preliminary test, radiological measurements of the translation and measurement in bigger flexion angles appeared both not feasible and too unreliable in this setting. The order in which the joint space was surgically narrowed may also be varied; the simulation of bilateral disorders may result in a more extensive alteration of knee stability, particularly on medio-lateral translation. However, in this series of tests, the intention was to simulate pathologies, which are treated with partially, or totally joint-preserving methods. We may further speculate that procedures which elevate the bone surface relative to the ligaments do not only result in a tighter varus/valgus, but also anteroposterior stability, which will be subject of future testing. Therefore, the use of computer-navigation tools that are most likely the best alternative in laboratory testing [12, 19] have to be considered, to allow investigation of transverse or rotational loading patterns.
Beyond the above-mentioned limitations, the presented study still reports to our knowledge a new observation and may help to improve the clinical evaluation of knee joints with a history of trauma, septic arthritis or other source of rapid unicompartimental degeneration. In such a situation, a false positive impression of a ligamentous injury may arise, and decision making is falsely directed away from totally or partially knee joint-preserving procedures.
Conclusion
Acute loss of the meniscus and cartilage and particularly impression of the joint surface may result in increased anteroposterior laxity, mimicking a relevant tear of the anterior cruciate ligament. Therefore, in degenerate joints, clinical evaluation of anteroposterior stability should rather rely on the presence of a firm stop than an overall increased joint translation.
References
Akgun I, Unlu MC, Edipoglu E, Uzun I (2009) Evaluation of the functional effects of anterior cruciate ligament bundles: a cadaveric experiment. J Knee Surg 22(4):317–324
Bach BR Jr, Warren RF, Flynn WM, Kroll M, Wickiewiecz TL (1990) Arthrometric evaluation of knees that have a torn anterior cruciate ligament. J Bone Joint Surg [Am] 72(9):1299–1306
Bonin N, Ait Si Selmi T, Donell ST, Dejour H, Neyret P (2004) Anterior cruciate reconstruction combined with valgus upper tibial osteotomy: 12 years follow-up. Knee 11(6):431–437
Boylan D, Greis PE, West JR, Bachus KN, Burks RT (2003) Effects of initial graft tension on knee stability after anterior cruciate ligament reconstruction using hamstring tendons: a cadaver study. Arthroscopy 19(7):700–705
Brage ME, Draganich LF, Pottenger LA, Curran JJ (1994) Knee laxity in symptomatic osteoarthritis. Clin Orthop Relat Res 304:184–189
Brantigan OC, Voshell AF (1941) The mechanics of the ligaments and menisci of the knee joint. J Bone Joint Surg [Am] 23:44–66
Daniel DM, Malcom LL, Losse G, Stone ML, Sachs R, Burks R (1985) Instrumented measurement of anterior laxity of the knee. J Bone Joint Surg [Am] 67(5):720–726
Daniel DM, Stone ML, Sachs R, Malcom L (1985) Instrumented measurement of anterior knee laxity in patients with acute anterior cruciate ligament disruption. Am J Sports Med 13(6):401–407
Dayal N, Chang A, Dunlop D, Hayes K, Chang R, Cahue S, Song J, Torres L, Sharma L (2005) The natural history of anteroposterior laxity and its role in knee osteoarthritis progression. Arthritis Rheum 52(8):2343–2349
Dejour H, Bonnin M (1994) Tibial translation after anterior cruciate ligament rupture. Two radiological tests compared. J Bone Joint Surg [Br] 76(5):745–749
Deschamps G, Lapeyre B (1987) Rupture of the anterior cruciate ligament: a frequently unrecognized cause of failure of unicompartmental knee prostheses. Apropos of a series of 79 lotus prostheses with a follow-up of more than 5 years. Rev Chir Orthop Reparatrice Appar Mot 73(7):544–551
Ferretti A, Monaco E, Labianca L, De Carli A, Maestri B, Conteduca F (2009) Double-bundle anterior cruciate ligament reconstruction: a comprehensive kinematic study using navigation. Am J Sports Med 37(8):1548–1553
Fessel G, Frey K, Schweizer A, Calcagni M, Ullrich O, Snedeker JG (2011) Suitability of thiel embalmed tendons for biomechanical investigation. Ann Anat 193(3):237–241
Highgenboten CL, Jackson AW, Jansson KA, Meske NB (1992) KT-1000 arthrometer: conscious and unconscious test results using 15, 20, and 30 pounds of force. Am J Sports Med 20(4):450–454
Hole RL, Lintner DM, Kamaric E, Moseley JB (1996) Increased tibial translation after partial sectioning of the anterior cruciate ligament. The posterolateral bundle. Am J Sports Med 24(4):556–560
Levy IM, Torzilli PA, Warren RF (1982) The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg [Am] 64(6):883–888
Levy IM, Torzilli PA, Gould JD, Warren RF (1989) The effect of lateral meniscectomy on motion of the knee. J Bone Joint Surg [Am] 71(3):401–406
Limbird TJ, Shiavi R, Frazer M, Borra H (1988) EMG profiles of knee joint musculature during walking: changes induced by anterior cruciate ligament deficiency. J Orthop Res 6(5):630–638
Monaco E, Labianca L, Maestri B, De Carli A, Conteduca F, Ferretti A (2009) Instrumented measurements of knee laxity: KT-1000 versus navigation. Knee Surg Sports Traumatol Arthrosc 17(6):617–621
Pottenger LA, Phillips FM, Draganich LF (1990) The effect of marginal osteophytes on reduction of varus-valgus instability in osteoarthritic knees. Arthritis Rheum 33(6):853–858
Sharma L, Lou C, Felson DT, Dunlop DD, Kirwan-Mellis G, Hayes KW et al (1999) Laxity in healthy and osteoarthritic knees. Arthritis Rheum 42(5):861–870
Sherman OH, Markolf KL, Ferkel RD (1987) Measurements of anterior laxity in normal and anterior cruciate absent knees with two instrumented test devices. Clin Orthop Relat Res 215:156–161
Steiner ME, Brown C, Zarins B, Brownstein B, Koval PS, Stone P (1990) Measurement of anterior-posterior displacement of the knee. A comparison of the results with instrumented devices and with clinical examination. J Bone Joint Surg [Am] 72(9):1307–1315
Thiel W (1992) The preservation of the whole corpse with natural color. Ann Anat 174(3):185–195
Tinius M, Hepp P, Becker R (2011) Combined unicompartmental knee arthroplasty and anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-011-1528-7
Wada M, Imura S, Baba H, Shimada S (1996) Knee laxity in patients with osteoarthritis and rheumatoid arthritis. Br J Rheumatol 35(6):560–563
Wright RW, Luhmann SJ (1998) The effect of knee effusions on KT-1000 arthrometry. A cadaver study. Am J Sports Med 26(4):571–574
Wroble RR, Van Ginkel LA, Grood ES, Noyes FR, Shaffer BL (1990) Repeatability of the KT-1000 arthrometer in a normal population. Am J Sports Med 18(4):396–399
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wieser, K., Betz, M., Farshad, M. et al. Experimental loss of menisci, cartilage and subchondral bone gradually increases anteroposterior knee laxity. Knee Surg Sports Traumatol Arthrosc 20, 2104–2108 (2012). https://doi.org/10.1007/s00167-011-1799-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-011-1799-z