
Abstract
The purpose of this study was to investigate the influence of tibial base plate angulation on knee kinematics and kinetics during knee arthroplasty. The amount of quadriceps force required to extend the knee and the anteroposterior displacement of a mobile bearing insert as well as tibiofemoral position were measured during an in vitro simulation of an isokinetic knee extension cycle. Human knee specimens (n = 7, mean age 62, range 52–75 years, all male) were tested in a kinematic knee simulating machine after total knee arthroplasty (TKA) with a mobile bearing insert prosthesis (Interax®, Stryker/Howmedica). During simulation, a hydraulic cylinder applied sufficient force to the quadriceps tendon to produce an extension moment of 31 N m about the knee. The quadriceps load was measured using a load cell attached to the quadriceps tendon, the anteroposterior displacement of the mobile bearing insert as well as the relative tibiofemoral position was measured using an ultrasound base motion analysis system (CMS 100®, Zebris). Quadriceps load, insert and tibial displacement were first investigated with the tibial base plate implanted with a neutral tibial base plate orientation, and subsequently after 10° posterior angulation. The quadriceps forces needed to produce a 31 N m knee extension moment after TKA with neutral slope reached levels as high as 1,391 N (SD 82 N). After applying a posterior slope of 10°, maximum quadriceps force was measured to be up to 1,303 N (SD 34 N, P = 0.04). The mobile bearing insert was observed to move up to 0.1 mm (SD 4.2 mm) anteriorly relative to the tibial base plate with neutral tibial slope, and up to 1.0 mm (SD 4.5 mm, P = 0.47) with tibial slope. Femoral position relative to the tibia moved from a posterior position of 13.1 mm (SD 4.0 mm) anteriorly up to 0.5 mm (SD 6.3 mm), and from 16.0 mm (SD 6.4 mm, P = 0.67) to 9.5 mm (SD 9.9 mm, P = 0.33) with a 10° tibial slope. Posterior slope of the tibial base plate resulted in a more physiologic insert movement with a more posterior position of the femur and reduced quadriceps force especially in knee flexion angles above 60° compared to TKA with a neutral slope of the tibial base plate. Thus, the data suggest that the quadriceps lever arm was improved, which might have positive effect in mobilization of patients after TKA.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
After implantation of a total knee arthroplasty (TKA), patients were observed to have altered walking patterns with less flexion and a shorter swing phase in the operated knee [1–3]. Furthermore, these patients showed abnormal functional adaptations and had more significant problems in stair climbing than in control subjects [6, 7, 23, 24]. The inability to extend the knee as strongly as needed for walking, lifting, and chair and stair rising was one of the most often occurring biomechanical reasons for the revision of TKA [19]. Furthermore, internal kinematic changes have been observed: Lewandowski et al. and Komistek et al. described a paradoxical movement of the tibiofemoral contact point from posterior to anterior during knee flexion after TKA, which was hypothesized to be caused by sacrifice of the cruciate ligaments [14–16, 16]. This paradoxical movement would decrease the distance between the tibial insertion of the patella tendon ligament and the tibiofemoral contact point especially in flexion, decreasing the lever arm of the extensor mechanism and resulting in higher quadriceps muscle force required to extend the knee at higher flexion angles [5]. An increase of tibial slope leads to a posterior displacement of the femur relative to the tibia and the tibiofemoral contact point, which increases the quadriceps lever arm and might have an effect on movement of a mobile bearing insert [10, 12]. This could lead to a higher quadriceps efficiency with a reduction of problems of the extensor mechanism [9, 11, 22].
The collected extension torque data from studies, which compared healthy subjects with patients who underwent TKA, were used as input data in the simulation of knee extension motions [4]. To determine the forces needed by the quadriceps muscle to produce a certain constant knee extension moment, we developed an in vitro experimental technique to simulate a constant extension moment knee motion. This simulation allows loadings that more closely approximate the magnitude of the physiologic forces and moments applied to the knee than has previously been reported in the literature [18].
We hypothesized that after TKA with a 10° posterior angulated tibial base plate (10° posterior slope) quadriceps force to exert the same extension moment would be reduced compared to implantation with a neutral (= 0°) tibial base plate, accompanied by a more physiologic movement of the insert and increased posterior position of the femur relative to the tibia.
Methods
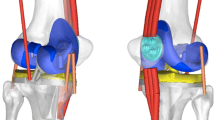
Seven fresh frozen knee specimens were tested in an isokinetic extension test in an in vitro simulation initially published by Stukenborg et al. and Ostermeier et al. [18, 20]. The Interax I.S.A.® (Stryker/Howmedica®, Ireland) was implanted into seven fresh frozen left knee cadaver (mean age 62, range 52–75 years). The knees were transected about 300 mm proximal and distal to the knee joint. The skin and subcutaneous tissues were removed, preserving the muscles, articular capsule, ligaments and tendons. The anterior cruciate ligament was removed and the posterior cruciate ligament was preserved. The Interax I.S.A.®-prosthesis-system provides a tibiofemoral articulation surface of the femoral prosthesis, which has a constant radius up to approximately 90° of knee flexion in the sagittal plane, reducing to higher degrees knee flexion degrees. The femoral component articulates on a high conforming surface with a mobile insert. The knee prosthesis permits anterior/posterior sliding and rotation of the mobile insert on the tibial base plate. Movement of the insert is guided by two metal pins on the tibial base plate which match the profile of a corresponding groove on the underside of the insert. The maximum possible movement of the insert center is 8.5 mm anterior/posterior and 18° of axial rotation relative to the tibial base plate. All specimens received the same size (400) of the femoral and tibial component. Each implantation was conducted by the same team of surgeons with the same implantation guidelines.
Insert movement and tibiofemoral position were measured by an ultrasonic tracking system (CMS 100®, Zebris GmbH, Isny, Germany), consisting of triplet markers (speakers) forming a plane for each object tracked, and a receiver unit with four microphones. The delay of the received ultrasonic signals between the microphones determined the marker position relative to the receiver unit. Each triplet marker was custom-mounted onto a PVC backing plate, forming an equilateral triangle with a base of 50 mm. One marker triangle was attached to the tibial base plate with its plane visually aligned perpendicular to the base plate horizontal plane. A second triangle was attached to the mobile bearing insert, perpendicular to the horizontal plane of the undersurface of the insert. The third triangle was fixed to the femur with unicortical screws parallel to the long axis of the femur. A distance of 1,000 mm between markers and receiver unit provided measurement of the triangle position at an accuracy of ± 0.1 mm and ±0.1° at a frequency of 10 Hz and a reproducibility of ± 0.005 mm (± 0.005°). Custom motion analysis software based on Excel® (Microsoft, USA) transformed the raw data into the anteroposterior positional coordinates of the insert center and the center of the femur relative to the center of the tibial base plate. The results were plotted as a function of flexion angle.
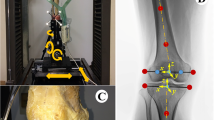
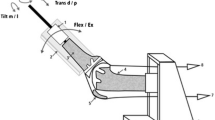
The specimens were mounted into a specially designed knee simulator in which isokinetic flexion–extension moments are simulated (Fig. 1). The knee specimens were oriented with the femur fixed horizontally and the patella facing downwards. The tibia was attached to the simulator at mid-length by means of a linear-rotational bearing which permits axial sliding and turning of the tibia. The bearing in turn was attached to a swing-arm, which allows varus–valgus rotation. The resulting arrangement gives complete freedom of motion of the joint, with the exception of flexion–extension, which is determined by the position of the swing arm. The swing arm was equipped with a strain gauge based load-measuring device which allows the torsional moment applied to the tibia to be monitored continuously. Movement of the tibia was generated by the coordinated activation of three hydraulic cylinders, one to simulate quadriceps muscle force, one to simulate a proprioreceptive co-contraction of the hamstring muscles and the third to apply an external flexion moment. A specially constructed tendon clamp, which allowed application of loads up to 2,000 N, was used to attach the quadriceps tendon and the hamstrings tendons to the hydraulic cylinder with a steel cable (Fig. 1).

Schematic side view of the test setup
Quadriceps load was measured with an accuracy of ± 0.1 N and a reproducibility of ± 0.005 N using a load cell (Hottinger Baldwin Messtechnik GmbH, Darmstadt, Germany) attached between the tendon clamp and the quadriceps cylinder. Knee flexion degree was measured using a voltage goniometer attached to the tibial swing arm with a frequency of 10 Hz and an accuracy of ± 0.05° and a reproducibility of ± 0.001°.
The test cycle simulated an isokinetic extension cycle from 120° of flexion to full extension, the quadriceps cylinder thereby applied sufficient force to the quadriceps tendon in a closed-loop control cycle to produce a constant extension moment of 31 N m about the knee. During simulation, the force applied by this cylinder changed depending of flexion angle of the knee. The hamstring cylinder simulated the co-contraction of the hamstrings muscles with a constant co-contractive flexion force of the hamstrings of 200 N.
First, quadriceps load, insert movement and tibiofemoral position were measured with the tibial base plate implanted with a neutral (zero) tibial slope. After explantation of the tibial base plate an additional bone wedge with 10° posterior slope and the center of the arc subtended by the wedge located at the anterior margin of the tibia was cut from the tibial head and the tibial base plate was reimplanted.
Each extension cycle was repeated three times and the measured data of each cycle was averaged at each decile of knee flexion angle. The difference between maximum quadriceps force, maximum relative insert displacement and relative femoral position to the tibial base plate with neutral (= 0°) and with 10° posterior tibiofemoral slope were analyzed using a parametric paired t test at a significance level of P = 0.05. In addition, significant differences between the values with and without tibial slope were investigated at 30°, 60° and 90° knee flexion.
Results
After TKA with neutral tibial slope, the shape of the quadriceps force curve was typically sinusoidal, reaching a maximum value of 1,390.6 N (SD 82.3 N) at 85.4°, and a minimum value of 741.6 N (SD 76.3 N) at 22.7° of knee flexion (Table 1, Fig. 2). After applying a posterior slope of 10°, maximum quadriceps force was measured to be up to 1,303.1 (SD 33.9 N, P = 0.04) at 96.2°, with a minimum force of 680.9 N (SD 38.8 N, P = 0.89) at 28.8° of knee flexion (Fig. 2). Anterior displacement of the mobile bearing insert relative to the tibial base plate with neutral tibial slope reached up to 0.1 mm (SD 4.2 mm) at 108.9°, with tibial slope the insert moved up to 1.0 mm (SD 4.5 mm, P = 0.47) at 77.9° of knee flexion (Fig. 3). After this, maximum anterior displacement of the insert was reduced, what represented a posterior movement relative to the tibial base plate in both conditions, up to −1.7 mm (SD 1.7 mm) with neutral and −1.0 mm (SD 1.8 mm, P = 0.71) with posterior tibial slope at maximum knee extension. During knee extension the femoral position with neutral tibial slope moved from a maximum posterior position relative to the tibia of −13.1 mm (SD 4.0 mm) at 100.1° of knee flexion anteriorly up to −0.5 mm (SD 6.3 mm) at 5.9°, with a 10° tibial slope from −16.0 mm (SD 6.4 mm, P = 0.67) at 84.1° to −9.5 mm (SD 9.9 mm, P = 0.33) at 5.5° (Fig. 4).

Post-TKA quadriceps load with neutral (=0°) tibial slope and with a posterior tibial slope of 10° to exert a constant knee extension moment of 31 N m (bars = standard deviation)

Post-TKA insert displacement relative to the tibial base plate after TKA with neutral (=0°) tibial slope and with a posterior tibial slope of 10° (bars = standard deviation)

Post-TKA position of femur relative to tibial base plate after TKA with neutral (=0°) tibial slope and with a posterior tibial slope of 10° (bars = standard deviation)
At 30° knee flexion, no significant difference in quadriceps load, insert displacement and femoral position were measured, whereas at 60° knee flexion quadriceps load was significantly reduced from 1,117.6 N (SD 91.1 N) to 943.9 N (SD 88.3 N, P = 0.04) and at 90° from 1,382.3 N (SD 51.2 N) to 1,298.9 N (SD 52.9 N, P = 0.04) after applying a posterior tibial slope of 10°, accompanied by a significantly increased anterior position of the insert position relative to the tibial base plate (Table 2).
Discussion
In this study, quadriceps muscle force needed to produce a constant extension moment was observed to change with angulation of the tibial base plate after TKA. The results showed that after applying a posterior tibial slope of 10°, a decreased quadriceps force was needed to exert the same extension moment, especially above 60° knee flexion. In addition, posterior slope of the tibial base plate resulted in a more physiologic insert movement at higher flexion angles with a more posterior position of the femur.
There are some limitations associated with this test setup which should be taken into consideration when interpreting the results of this study. The test only simulated one constant moment during the whole extension cycle, which is different to isokinetic extension cycles used in rehabilitation or evaluation of extension strength after implantation of TKA [4]. Those tests showed varying peak extension moments over the isokinetic extension cycle, with maximum moments showing a high interindividual variation. We thus chose to apply a constant moment which represents a mean extension moment reached by patients over the entire extension cycle. This does not always represent conditions during daily activity, e.g., the swing phase during walking, where lower external moments could occur [3]. During these movements, the differences in quadriceps load and kinematics of the components measured in this study should be lower after applying a posterior tibial slope of 10°. In addition, this test setup did not simulate the influence of weight bearing, which could have an additional stabilizing effect on the insert and tibial movement [8]. A systematic bias could exist, which should be taken into account, but as the results of the presented study were similar to previous studies, this error could be minimized [14, 18].
Generally, the lever arm changes during extension of the knee joint because of the translating tibiofemoral and patellofemoral contact point. Thus, the quadriceps muscle force also changes during extension in a sinusoidal shape, which was described by Nisell et al. and own previous studies [17, 18]. After TKA, this shape of force pattern is similar, which is also reflected in the presented study, but the amount of quadriceps extension force needed to exert the same extension moment especially in flexion is increased due to the different movement pattern of the tibiofemoral contact point [5, 14, 16, 18]. Applying a posterior slope at the tibial base plate should lead to a posterior displacement of the femur described by Giffin et al. [10], who found a significant posterior shift of 1.9 mm after a 5 mm anterior open wedge osteotomy. In this study, after implantation of the tibial base plate with a 10° posterior slope, the femoral position relative to the tibia shifted 2.9 mm posteriorly in flexion and 9.0 mm in extension showing the same shift. Interestingly, insert movement also showed an altered movement pattern: With a 10° tibial slope, the insert moved anteriorly during extension in higher degrees of knee flexion, which tends to be a more physiologic movement pattern [22]. In knee prosthesis with mobile bearing inserts, insert movement represents the movement of the tibiofemoral contact point due to the high conformity of the tibiofemoral insert surface [13, 14, 21]. Therefore, in this study, changing the tibial slope of the tibial base plate alters the movement of the tibiofemoral contact point to a more physiologic movement especially at knee flexion angles greater than 80°. With these altered movements of relative femoral position and insert position relative to the tibial base plate, quadriceps lever arm should increase and quadriceps extension force needed to exert the same extension moment was reduced, especially in high knee flexion angles [5, 6, 24]. This should improve quadriceps function in walking, raising and stair climbing and should be recognized for postoperative mobilization of patients who undergo TKA.
Conclusions
This in vitro test showed a potential improvement of quadriceps extension force after applying a posterior tibial slope on the tibia base plate during TKA.
References
Andriacchi TP (1988) Biomechanics and gait analysis in total knee arthroplasty. Orthop Rev 17:470–473
Andriacchi TP, Alexander EJ, Godman SB (1999) Understanding the role of functional adaptions in patients with total knee replacements. 1, 50–53. International Conference on Knee Replacement 1974–2024, IMechE Headquarters. Westminster, London, UK
Andriacchi TP, Galante JO, Fermier RW (1982) The influence of total knee-replacement design on walking and stair-climbing. J Bone Joint Surg [Am] 64:1328–1335
Berman AT, Bosacco SJ, Israelite C (1991) Evaluation of total knee arthroplasty using isokinetic testing. Clin Orthop 271:106–113
Dennis DA (1998) Proposed advantages of posterior cruciate ligament retention orthopaedics today 1[September/October], 10. New Jersey, Slack Incorporated
Dorr L, Scott R, Ranawat CS (1985) Controversies of total knee arthroplasty: importance of retention of the posterior cruciate ligament. In: Ranawat C (ed) Total knee arthroplasty: techniques, results and complications. Springer, Berlin, Heidelberg New York pp 197–202
Dorr LD (1988) Functional comparison of posterior of posterior cruciate retaining versus cruciate sacrificed total knee arthroplasty. Clin Orthop 236:36–41
Draganich LF (1984) The influence of the cruciate ligaments, knee musculature and anatomy on knee joint loading. University of Illinois at Chicago
Garg A, Walker PS (1990) Prediction of total knee motion using a three-dimensional computer-graphics model. J Biomech 23:45–58
Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD (2004) Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med 32:376–382
Godest AC, de Cloke CS, Taylor M, Gregson PJ, Keane AJ, Sathasivan S, Walker PS (2000) A computational model for the prediction of total knee replacement kinematics in the sagittal plane. J Biomech 33:435–442
Hernigou P, Deschamps G (2004) Posterior slope of the tibial implant and the outcome of unicompartmental knee arthroplasty. J Bone Joint Surg Am 86-A:506–511
Komistek RD, Dennis DA, Haas B (1999) Motion in LCS Rotating Platform. 1, 246–249. London, UK, Imech E. International conference on knee replacement 1974–2024. 22-4-0099
Komistek RD, Dennis DA, Walker SA, Anderson DT (1998) A multicenter analysis of A/P translation in TKA. 11th conference of the ESB, Toulouse
Komistek RD, Walker SA, Crossett LS, Running D, Dennis DA (1998) In vivo kinematics of PS implanted knees during gait. 11th Conference of the ESB, Toulouse
Lewandowski PJ, Askew MJ, Lin DF, Hurst FW, Melby A (1997) Kinematics of posterior cruciate ligament-retaining and -sacrificing mobile bearing total knee arthroplasties. J Arthroplasty 12:777–784
Nisell R, Ekholm J (1985) Mechanics of the knee. Acta Orthop Scand Suppl 216:1–42
Ostermeier S, Hurschler C, Stukenborg-Colsman C (2004) Quadriceps function after TKA—an in vitro study in a knee kinematic simulator. Clin Biomech (Bristol, Avon) 19:270–276
Rand JA (1994) Current concepts review: the patellofemoral joint in total knee arhtroplasty. JBJS 76-A:612–620
Stukenborg-Colsman C, Ostermeier S, Hurschler C, Wirth CJ (2002) Tibiofemoral contact stress after total knee arthroplasty comparison of fixed and mobile-bearing insert designs. Acta Orthop Scand 73:638–646
Stukenborg-Colsman C, Ostermeier S, Wenger K, Wirth CJ (2002) Relative motion of a mobile bearing insert after total knee arthroplasty—a dynamic in vitro study. Clin Biomech 17:49–55
Walker PS, Sathasivam S (1999) The design of guide surfaces for fixed-bearing and mobile-bearing knee replacements. J Biomech 32:27–34
Wimmer MA (1999) Wear of the polyethylene component created by rolling motion of the artificial knee joint. Shaker, Aachen
Wimmer MA, Andriacchi TP (1997) Tractive forces during rolling motion of the knee: implications for wear in total knee replacement. J Biomech 30:131–137
Acknowledgements
We thank the company Stryker/Howmedica®, Limerick, Ireland for their financial support of this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ostermeier, S., Hurschler, C., Windhagen, H. et al. In vitro investigation of the influence of tibial slope on quadriceps extension force after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 14, 934–939 (2006). https://doi.org/10.1007/s00167-006-0078-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-006-0078-x