
Abstract
Purpose
To describe trends in outcomes of cancer patients with unplanned admissions to intensive-care units (ICU) according to cancer type, organ support use, and performance status (PS) over an 8-year period.
Methods
We retrospectively analyzed prospectively collected data from all cancer patients admitted to 92 medical–surgical ICUs from July/2011 to June/2019. We assessed trends in mortality through a Bayesian hierarchical model adjusted for relevant clinical confounders and whether there was a reduction in ICU length-of-stay (LOS) over time using a competing risk model.
Results
32,096 patients (8.7% of all ICU admissions; solid tumors, 90%; hematological malignancies, 10%) were studied. Bed/days use by cancer patients increased up to more than 30% during the period. Overall adjusted mortality decreased by 9.2% [95% credible interval (CI), 13.1–5.6%]. The largest reductions in mortality occurred in patients without need for organ support (9.6%) and in those with need for mechanical ventilation (MV) only (11%). Smallest reductions occurred in patients requiring MV, vasopressors, and dialysis (3.9%) simultaneously. Survival gains over time decreased as PS worsened. Lung cancer patients had the lowest decrease in mortality. Each year was associated with a lower sub-hazard for ICU death [SHR 0.93 (0.91–0.94)] and a higher chance of being discharged alive from the ICU earlier [SHR 1.01 (1–1.01)].
Conclusion
Outcomes in critically ill cancer patients improved in the past 8 years, with reductions in both mortality and ICU LOS, suggesting improvements in overall care. However, outcomes remained poor in patients with lung cancer, requiring multiple organ support and compromised PS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Outcomes in critically ill cancer patients improved in the past eight years, with reductions in both mortality and ICU LOS, suggesting improvements in overall care. The fact that the largest improvement in survival was seen in the less severely ill patients suggests that ICU admission has a place in the management of complex patients regardless of traditional markers of organ failure. On the other hand, outcomes remained poor in patients with lung cancer, requiring multiple organ support and compromised performance status. |
Introduction
The number of cancer patients admitted to intensive care units (ICU) is rising [1,2,3]. Many patients are admitted for postoperative care after major surgical resections and generally present with good outcomes with low hospital mortality [3]. However, despite recent improvements in cancer care, the occurrence of life-threatening events, such as cancer-related complications, sepsis, acute respiratory failure, need for urgent surgeries, among other conditions, still poses challenge for oncologists and critical care physicians [1, 4,5,6,7]. Recent reports showed that cancer might be present in over 38% of all patients that died after receiving critical care in the last 90 days of their lives [8].
The prognosis of critically-ill patients with cancer appears to be improving in the last decades [1, 8,9,10], although mortality for specific groups, including some hematological malignancies, patients who underwent allogeneic bone marrow transplant, and those requiring multiple organ support remains relatively high [9, 11, 12]. Previous studies assessing outcome trends in these patients are relatively scarce and with intrinsic limitations to draw more robust conclusions. First, they were performed in specialized cancer centers or used information from large administrative databases with limited clinical characterization [9, 10, 13, 14]. Second, only trends in crude mortality rates over time were reported. Finally, understanding that cancer patients are a heterogeneous population and that their outcomes are dependent on previous clinical health status and acute illness, those studies are also limited by not evaluating subgroups of patients taking into consideration these clinical characteristics.
To help bridging these gaps, we evaluated a large contemporary cohort of patients with cancer with unplanned ICU admissions to assess changes in the admission clinical profiles and outcomes over 8 years. Our primary objective was determining the overall in-hospital mortality over time adjusted for several clinical confounders with focus on changes in the association between performance status (PS) and organ support use across the period in patients with different types of cancer. The ICU length-of-stay (LOS) was the secondary endpoint.
Patients and methods
Study design and participating centers
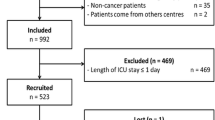
This was a retrospective cohort study starting in July 2011 until June 2019. Patients were included based on their ICU admission date. A total of 92 non-specialized medical–surgical ICUs in 34 hospitals of an integrated network of hospitals in several Brazilian States—Rede D’Or São Luiz de Hospitais—participated in the study. The number of participating units increased over time, as new hospitals joined the network (sFigure 1 in the Electronic Supplementary Material—ESM). Local Ethics Committee and the Brazilian National Ethics Committee (CAAE: 17079119.7.0000.5249) approved the study without the need for informed consent.
Participants and data collection
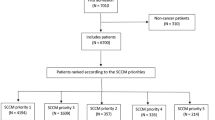
For the purposes of the present study, we elected for analysis only the first unplanned ICU admission for a given adult (≥ 16 yo) patient with a definite diagnosis of cancer before ICU admission due to acute medical complications or for postoperative care after urgent surgeries (defined as surgeries scheduled less than 24 h before the procedure and excluding codes for known elective surgical procedures, such as cancer resections). Readmissions and patients without comorbidity data were not considered. We retrieved all anonymized information from an electronic system used for quality improvement and benchmarking purposes for ICUs (Epimed Monitor®, Rio de Janeiro, Brazil) [15]. This database contains prospectively collected structured data of all admissions to the participating ICUs, with a comprehensive clinical characterization of patients including demographics, ICU admission diagnosis, comorbidities, PS in the week before hospital admission according to Eastern Cooperative Oncology Group (ECOG) stratified in 0–1, 2 or 3–4, as previously reported [16], Illness severity scores (Simplified Acute Physiology Score—SAPS—3 [17], use of organ support (mechanical ventilation—MV, renal replacement therapy—RRT, vasopressors), and ICU and hospital outcomes (mortality and LOS) [15]. A flowchart is shown in sFigure 2.
Outcomes
The primary outcome was in-hospital mortality for all analyses. The ICU LOS was the secondary outcome of interest.
Missing value policy
There were no missing data for age, PS, type of cancer, primary site of solid tumor, or outcomes. We imputed categorical variables with less than 1% missing values by the most common values. The remaining variables with missing values were mostly physiological (supplementary table—sTable—1 in the ESM), which were not considered for the main analysis.
Statistical analysis
We used descriptive methods to describe the cohort and graphical representations to show trends over time in patient features as well as outcomes from marginal posterior probabilities. The main analysis for hospital outcome was assessed through a Bayesian hierarchical binary model accounting for predefined relevant clinical variables: age, ECOG-PS, need for MV, vasopressors and RRT during ICU stay, cancer type (locoregional solid tumor, metastatic solid tumor, or hematological malignancy), and admission due to infection, cardiovascular, or respiratory (excluding sepsis) reasons. Bayesian models are set up differently from frequentist models, in the sense that priors for the effect sizes are incorporated to the regression and results are displayed as a distribution of possible values compatible if data, given the priors and the model. This allows querying the results (hence called posterior distributions) to obtain probabilistic inference. We have used non-informative priors, centered at the absence of effect, and that considered both “beneficial” and “harmful” effects as equally possible, but a wide distribution (that is, no hard information on the distribution of the effect size was made). This type of prior is frequently called regularizing prior, because it may reduce overfitting by simply making the model skeptic to very large or very small effect sizes. Details are provided in the ESM. We added a random intercept for admission year (as an eight-level factor) and added random slope within each year for PS, need for MV, vasopressors, and/or RRT. This allowed estimating posterior probabilities from the model, assuming that the effects of both PS and organ support would change over the study period. Results for fixed effects were reported as odds ratios (OR) with respective 95% credible intervals (CI). We also displayed the predicted marginal probabilities (that is, the distribution probability predicted by a model) for the main model by extracting samples from posterior predicted probabilities in several scenarios, considering both fixed and random effects, and reporting reduction in mortality over time with focus on difference between first year and last year of the study cohort. We performed a pre-specified subgroup analysis focused on the six most frequent primary sites of solid tumors that accounted for more than 60% of all solid tumor admissions. To confirm the main analysis findings under a different statistical approach, we also performed a sensitivity analysis considering the hospital where the patient was admitted as a random effect and year as fixed effect. A secondary sensitivity analysis was performed for the primary endpoint for the 37 ICUs that collected data during whole study period (2011–2019), including 20,084 patients.
For the secondary endpoint, case-specific sub-hazard ratios (SHR) accounting for competing events [18] (ICU death as a competitor for ICU discharge) were constructed from Cox regression models adjusted for SAPS 3 score, cancer type, PS and admission year. We provide all details on the adjustment for these models in the ESM. We followed the STROBE report for this manuscript (see ESM). We performed all analysis in R, version 3.6.1.
Results
The number of participating units over time and the study flowchart are shown in sFigures 1 and 2, respectively. During the study period, 365,295 patients were admitted to the participating ICUs and 43,025 (11.8%) had cancer. Out of them, 32,096 cancer patients (8.7% of all ICU admissions and 74.6% among cancer patients) were studied. There were 21,008 patients with locoregional solid tumors (65.4%), 7956 with metastatic solid tumors (24.7%), and 3132 with hematological malignancies (9.9%). sFigure 3 depicts the total number of cancer patients according to the primary tumor site, and the most frequent were breast (14.4%), prostate (14%), colon/rectum (11.2%), lung (10.9%), brain (6%), and kidney (5.5%). There were 30,770 patients (95.9%) admitted because of medical complications and 1326 (4.1%) following urgent surgeries. Infection or sepsis (31%), cardiovascular (19%), neurological (10.7%), digestive (9.5%), cancer-related (8.1%), and respiratory (6%) complications were the most frequent admission diagnosis. Patients’ characteristics and outcomes stratified by admission year are reported in Table 1.
There was an increase in the relative use of available bed/days by cancer patients, with over 30% of all bed/days being occupied by cancer patients in the two most recent years; unplanned admissions were responsible for most of this increase (Fig. 1a). ICU admissions for selected primary cancer sites are shown in Fig. 1b with varying trends over time. There was a decrease in the proportion of patients with metastatic disease and with ECOG-PS 0–1 from 2011 to 2019 (Table 1). Decreases in use of all organ support and in overall crude ICU (18.8% in 2011–2012 to 11% in 2018–2019) and hospital mortality (33% to 17.7%) were observed. Mean ICU LOS remained stable over time, but a substantial decrease in-hospital LOS was observed (21.61 days in 2011–2012 to 12.14 days in 2018–2019). The proportion of patients discharged home without the need for nursing assistance increased from 66.6% in 2011–2012 to 80.8% (2018–2019).

a Percentage of ICU bed-days occupied by cancer patients over time; b Percentage of admissions according to relevant primary tumor sites
The results of the fixed effects for the main mortality model are shown in sFigure 4. All predictors were associated with higher mortality with high degree of certainty, except cardiovascular admissions, that were associated with reduced odds for mortality. Among them, the need for MV was the strongest predictor of mortality with an adjusted OR of 7.82 (95% CI 7.04–8.76). Overall reduction in mortality from 2011–2012 until 2018–2019 was 9.2% (95% CI 13.1–5.6%). The reduction in adjusted mortality varied according to PS, organ support, and cancer type (Fig. 2). The largest reductions in mortality occurred in patients without need for organ support (9.6%) or with need for mechanical ventilation (MV) only (11%), and the smallest reduction was observed in those requiring MV, vasopressors, and renal replacement therapy (3.9%) simultaneously (Fig. 3). For patients with organ support, survival gains were less pronounced as the PS worsened (Figs. 2 and 3). sFigures 5, 6, and 7 depict the mortality reductions from the first and last cohort study year according to cancer type. Patients with metastatic solid tumors had lower reductions in mortality than in patients with locoregional solid tumors and hematological malignancies. Patients with metastatic solid tumor, poor PS and simultaneous need for MV, vasopressors, and RRT had the highest adjusted mortality, and had were negligible survival gains over the period (− 1.5% from 2011–2012 to 2018–2019, sFigure 6). The main findings of mortality reductions over time were consistent in the alternative method (sFigure 8, sTable 2) and in the analysis considering only patients admitted to ICUs that contributed during the whole study period (sFigure 9, sTable 3).

Predicted mortality for the cancer types (hematological, locoregional, and metastatic solid tumors) according to need for organ support. Y axis: year of admission; X axis: predicted mortality. Each subplot Y axis represents the probability density function. Panels represent the level of organ support: a none, b MV only, c MV plus VP, and d MV + VP + RRT. One sub-panel for each cancer type is shown inside each main panel. MV mechanical ventilation, VP vasopressors, RRT renal replacement therapy

Predicted reduction in-hospital mortality from 2011–2012 to 2018–2019 for a all patients, b ECOG-PS 0–1, c ECOG-PS 2, and d ECOG-PS 3–4. Y axis is the probability density function
We performed a subgroup analysis in patients with prostate, breast, lung, colon/rectum, brain, and kidney cancer according the PS and use of organ support (Fig. 4). In general, the results were comparable to the main analyses in the sense that adjusted mortality decreased over time, but reductions were less pronounced in patients with multiple organ failure and in those with higher ECOG. Figure 4d shows that mortality for patients with studied types of solid cancer and ECOG-PS 3–4 had a poor prognosis with small reductions in mortality over the years. As need for organ support increased (panels a–d), differences in baseline predicted mortality for different cancer types were reduced. Among these most frequent primary sties of solid tumors, lung cancer patients had the worst outcomes and the smallest survival gain over time.

Predicted mortality for the six most common solid cancer sites in the database according to need for organ support. Y axis: year of admission (for each subplot, Y axis represents the probability density function); X axis: predicted mortality. Panels represent the level of organ support: a none, b MV only, c MV plus VP, and d MV + VP + RRT. One sub-panel for each cancer site is shown inside each main panel. Note that trends in reduction in mortality are comparable to all cancer sites, but as need for support increases the predicted mortality rate of different cancer sites diminishes. MV mechanical ventilation, VP vasopressors, RRT renal replacement therapy. The number of included patients are: brain (1934); breast (4615); colon/rectum (3591); kidney (1752); lung (3490); and prostate (4502)
For secondary outcome analysis, each increase in admission year was associated with a lower SHR [0.93 (0.91–0.94)] of dying in the ICU and a higher SHR [1.01 (1–1.01)] of being discharged alive (sTable 4). Cumulative incidence plots for discharge and death according to tumor type and ECOG for 2011–2012 and 2018–2019 are shown in sFigure 10. Probability of ICU discharge over time for specific tumor types and different degrees of performance impairment are shown in sFigures 11–13. SAPS 3, metastatic disease, and worse PS were associated with worse outcomes (delayed discharge and higher mortality). There was an association between the increase in admission year with lower mortality and earlier ICU discharge.
Discussion
In this study, we demonstrated a consistent and continuous outcome improvement in a large contemporary cohort of cancer patients requiring ICU admission because of life-threatening complications over an 8-year period. Our study has three major findings. First, differently from the previous studies, here, we reported trends in mortality adjusted for several clinical confounders. Second, our results also suggest that outcomes are affected by a complex interplay among the different types of cancer, the level of organ support, a proxy for the severity of acute illness, and the PS, a key surrogate marker of chronic health status. Survival gain estimates decreased as both the severity of organ failures and PS worsened. Moreover, although there was an absolute risk reduction for all described scenarios, some specific subgroup of patients had negligible survival gains, particularly those with metastatic solid tumors, poor PS, and multiple organ failure needing invasive support. Third, we also demonstrated in a cause specific hazard approach that the decrease in mortality occurred along with a decrease in the adjusted ICU LOS. All these findings are important to assist clinicians and managers in decisions to provide high-quality and affordable critical care to an increasing number of patients with cancer needing ICU admission, as was also demonstrated in our study (more than 30% of all beds in general medical–surgical ICU were occupied by patients with cancer in the latter years).
Our results provide additional evidence to previous studies reporting comparable improvements in unadjusted mortality [9, 10, 13, 14]. Among the types of tumor, we found the largest survival gains in patients with locoregional solid tumors and hematological malignancies. As expected, survival gains were much less pronounced in patients with metastatic solid tumors. The importance of cancer site on determining outcome decreased as the illness severity increased, suggesting that for sickest patients, the primary cancer site is much less important than the acuity of their clinical condition. However, the outcomes of patients with lung cancer facing a critical illness remain, in general, worse when compared to other types of solid tumors [13, 19].
Our analysis confirms the role of several other known risk factors for poor outcomes in cancer patients, including PS impairment [16] and need for organ support [11]. The fact that mortality reductions were invariably less pronounced in patients with PS impairment reinforces the need for a more judicious use of organ support in these patients and highlights the importance of baseline health status on determining outcomes in critically ill patients [8]. Oncologists have used PS assessment for decades to define the most appropriate therapeutic plan for a given patient. Similarly, since PS impairments are also associated with worse outcomes in both general and cancer ICU patients, intensivists are increasingly measuring PS before the onset of critical illnesses to assist in decisions related to the appropriateness of care, including ICU admission policies and end-of-life (EOL) decisions [3, 7, 16, 19]. In the multivariate Bayesian analysis, MV had the highest odds for mortality, which is in line with the previous studies in cancer patients [11, 14, 20]. However, in one of the most striking findings in our study, we observed the largest mortality reductions in patients needing MV only.
There are several explanations for our findings. Improvements in overall ICU care and adoption of modern strategies in the management of organ dysfunction may result in lower hospital mortality. For instance, several changes in the management of cancer patients with respiratory failure, including a more judicious use of noninvasive ventilation and bronchoscopy, early intubation, and increase of the arsenal for a broader diagnostic workup, might have contributed for the improved outcomes [7, 21]. Along with improvements in critical care, the novel anticancer treatments and improvements in the management of several types of malignancies over the last 2 decades certainly contributed with these observations [1]. One interesting finding of this analysis is that an important reduction in mortality occurred in patients that did not require organ support. This may suggest that at least part of the improvement seen occurred in patients receiving non-ICU care inside the ICU. It may be possible that wards are no longer capable of carrying for such complex patients in some scenarios, for example.
Our study has, however, some important limitations. It was based solely in a large network of private hospitals in Brazil; therefore, some caution is needed when transposing our results to in other settings such as public hospitals or other countries; international validation of such findings is, therefore, needed. We did not have access to cost information for the study and we are, therefore, unable to provide information on relevant questions, such as whether costs per patient-day changed, how much was spent for specific scenarios (such as patients with multiple organ failure), etc. The model considered patients that received organ support, and it is conceivable that some sicker patients would die before use of organ support, especially renal replacement therapy. This is of special interest, because we did not consider treatment limitations (such as withhold and withdraw of organ support), since this information was not available in the database. Additionally, not all ICUs collected data during the whole study period. While hospitals were not accounted for in the main model, an alternative analysis considering hospital as random effect provided comparable results. We were also unable to explore reasons for the decline in patient mortality nor did we collect data on longer follow-up after the hospital. EOL decisions were not recorded in the cohort data, which may have influenced the results, especially in patients with severe PS impairment. Close to 10% of the patients had hematological malignancies, but this frequency is in accordance with the previous studies in patients admitted to general hospitals [3, 9]. In addition, some specific populations were underrepresented in this study, including bone marrow transplant recipients. Finally, urgent surgeries were defined according to the difference of time between scheduling and occurrence accounting for procedure coding, but it is still conceivable that some contamination of elective procedures occurred despite our best efforts.
Conclusion
Short-term outcomes of critically ill patients with cancer have improved in the past 8 years in several scenarios, including those requiring MV. This was accompanied by a reduction in ICU LOS. However, prognosis remained grim in some subgroups, especially in patients with metastatic disease, poor PS, and those requiring multiple organ support.
Change history
12 February 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00134-020-06252-7
References
Azoulay E, Schellongowski P, Darmon M et al (2017) The intensive care medicine research agenda on critically ill oncology and hematology patients. Intensive Care Med 43:1366–1382. https://doi.org/10.1007/s00134-017-4884-z
Puxty K, McLoone P, Quasim T et al (2015) Risk of critical illness among patients with solid cancers: a population-based observational study. JAMA Oncol 1:1078–1085. https://doi.org/10.1001/jamaoncol.2015.2855
Soares M, Bozza FA, Azevedo LCP et al (2016) Effects of organizational characteristics on outcomes and resource use in patients with cancer admitted to intensive care units. J Clin Oncol Off J Am Soc Clin Oncol 34:3315–3324. https://doi.org/10.1200/JCO.2016.66.9549
Shimabukuro-Vornhagen A, Böll B, Kochanek M et al (2016) Critical care of patients with cancer. CA Cancer J Clin 66:496–517. https://doi.org/10.3322/caac.21351
Gutierrez C, McEvoy C, Munshi L et al (2020) Critical care management of toxicities associated with targeted agents and immunotherapies for cancer. Crit Care Med 48:10–21. https://doi.org/10.1097/CCM.0000000000004087
Azoulay E, Shimabukuro-Vornhagen A, Darmon M, von Bergwelt-Baildon M (2019) Critical care management of chimeric antigen receptor T cell-related toxicity. Be aware and prepared. Am J Respir Crit Care Med 200:20–23. https://doi.org/10.1164/rccm.201810-1945ED
Azoulay E, Pickkers P, Soares M et al (2017) Acute hypoxemic respiratory failure in immunocompromised patients: the Efraim multinational prospective cohort study. Intensive Care Med 43:1808–1819. https://doi.org/10.1007/s00134-017-4947-1
Chaudhuri D, Tanuseputro P, Herritt B et al (2017) Critical care at the end of life: a population-level cohort study of cost and outcomes. Crit Care Lond Engl 21:124. https://doi.org/10.1186/s13054-017-1711-4
Ostermann M, Ferrando-Vivas P, Gore C et al (2017) Characteristics and outcome of cancer patients admitted to the ICU in England, Wales, and Northern Ireland and national trends between 1997 and 2013. Crit Care Med 45:1668–1676. https://doi.org/10.1097/CCM.0000000000002589
de Vries VA, Müller MCA, Sesmu Arbous M et al (2018) Time trend analysis of long term outcome of patients with haematological malignancies admitted at dutch intensive care units. Br J Haematol 181:68–76. https://doi.org/10.1111/bjh.15140
Darmon M, Bourmaud A, Georges Q et al (2019) Changes in critically ill cancer patients’ short-term outcome over the last decades: results of systematic review with meta-analysis on individual data. Intensive Care Med 45:977–987. https://doi.org/10.1007/s00134-019-05653-7
Azoulay E, Mokart D, Pène F et al (2013) Outcomes of critically ill patients with hematologic malignancies: prospective multicenter data from France and Belgium–a groupe de recherche respiratoire en réanimation onco-hématologique study. J Clin Oncol Off J Am Soc Clin Oncol 31:2810–2818. https://doi.org/10.1200/JCO.2012.47.2365
Slatore CG, Cecere LM, Letourneau JL et al (2012) Intensive care unit outcomes among patients with lung cancer in the surveillance, epidemiology, and end results-medicare registry. J Clin Oncol Off J Am Soc Clin Oncol 30:1686–1691. https://doi.org/10.1200/JCO.2011.40.0846
Wallace SK, Rathi NK, Waller DK et al (2016) Two decades of ICU utilization and hospital outcomes in a comprehensive cancer center. Crit Care Med 44:926–933. https://doi.org/10.1097/CCM.0000000000001568
Zampieri FG, Soares M, Borges LP et al (2017) The Epimed Monitor ICU Database®: a cloud-based national registry for adult intensive care unit patients in Brazil. Rev Bras Ter Intensiva 29:418–426. https://doi.org/10.5935/0103-507X.20170062
Zampieri FG, Bozza FA, Moralez GM et al (2017) The effects of performance status one week before hospital admission on the outcomes of critically ill patients. Intensive Care Med 43:39–47. https://doi.org/10.1007/s00134-016-4563-5
Moreno RP, Metnitz PGH, Almeida E et al (2005) SAPS 3–From evaluation of the patient to evaluation of the intensive care unit. Part 2: development of a prognostic model for hospital mortality at ICU admission. Intensive Care Med 31:1345–1355. https://doi.org/10.1007/s00134-005-2763-5
Gerds TA, Blanche P, Mortensen R et al (2020) Risk regression: risk regression models and prediction scores for survival analysis with competing risks. https://cran.r-project.org/web/packages/riskRegression/index.html. Accessed 08 May 2020
Soares M, Toffart A-C, Timsit J-F et al (2014) Intensive care in patients with lung cancer: a multinational study. Ann Oncol Off J Eur Soc Med Oncol ESMO 25:1829–1835. https://doi.org/10.1093/annonc/mdu234
Azevedo LCP, Caruso P, Silva UVA et al (2014) Outcomes for patients with cancer admitted to the ICU requiring ventilatory support: results from a prospective multicenter study. Chest 146:257–266. https://doi.org/10.1378/chest.13-1870
Azoulay E, Mokart D, Kouatchet A et al (2019) Acute respiratory failure in immunocompromised adults. Lancet Respir Med 7:173–186. https://doi.org/10.1016/S2213-2600(18)30345-X
Acknowledgements
This study was supported by the National Council for Scientific and Technological Development (CNPq) (Grant No. 302188/2018-5), Carlos Chagas Filho Foundation for Research Support of the State of Rio de Janeiro (FAPERJ), and by departmental funds from the D’Or Institute for Research and Education.
Author information
Authors and Affiliations
Contributions
FG.Z, TG.R, JI.F.S, FA.B, and MS contributed to the study conception and design, and data interpretation. FG.Z and MS performed the data processing and statistical analysis, and drafted the first version of the manuscript. LU.T, AP.NJr., and PM.H participated in data interpretation and revised the manuscript for important intellectual content. TG.R, PV.M, RC, WN.V, MO.M, MF.A.L, SB.C, AG.R.C, FV.C.DM, MS.S, EP, FG.M, GV.R, and AR.S performed data collection and revised the manuscript for important intellectual content. All authors commented on previous versions of the manuscript, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
Dr. Soares and Dr. Salluh are founders and equity shareholders of Epimed Solutions®, which commercializes the Epimed Monitor System®, a cloud-based software for ICU management and benchmarking. The other authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: There was an error in figure 4.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Zampieri, F.G., Romano, T.G., Salluh, J.I.F. et al. Trends in clinical profiles, organ support use and outcomes of patients with cancer requiring unplanned ICU admission: a multicenter cohort study. Intensive Care Med 47, 170–179 (2021). https://doi.org/10.1007/s00134-020-06184-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-020-06184-2