
Abstract
Objective
The objective was to examine the effect of repeated applications of coupled plasmafiltration-adsorption on the hemodynamic response in septic shock patients hospitalized in intensive care units (ICUs).
Design
Prospective, intention-to-treat.
Setting
General ICU of a tertiary care, non-teaching, 400-bed, city hospital.
Patients and participants
Twelve consecutive mechanically ventilated septic shock patients, with or without concomitant acute renal failure (ARF).
Intervention
A median of 10 consecutive sessions (prescribed treatment time: 10 h/session; delivered duration: 8.43±1.37 h/min) of coupled plasmafiltration-adsorption for each patient.
Measurements and results
Mean arterial pressure (77.2±12.5 [CI 95%; 74.5–79.8] vs. 83.3±14.1 [CI 95%; 80.3–86.3] mm Hg; [p<0.001]), cardiac index (4.03±0.89 [CI 95%; 3.83–4.22] vs. 3.46±0.82 [CI 95%; 3.28–3.64] L/m2/min; [p<0.001]), systemic vascular resistance index (1,388±496 [CI 95%; 1,278–1,497] vs. 1,753±516 [CI 95%; 1,639–1,867] dynes × s/cm5; [p<0.001]), PO2/FIO2 ratio (204±87 [CI 95%; 185–223] vs. 238±82 [CI 95%; 220–256]; [p<0.001]), significantly improved during 100 global treatments (pre- vs. post-treatment values). Intra-thoracic blood volume and extra-vascular lung water did not change across treatments. Vasopressor requirement was reduced: norepinephrine decrease from an infusion rate of 0.13±0.07 (CI 95%; 0.06–0.16) to 0 γ/kg/min after a mean of 5.3±2.7 sessions. C reactive protein (CRP) significantly decreased (from 29.3±7.3 vs. 7.9±4.8; p<0.0001) during treatment. Survival was 90% at day 28 and 70% at day 90.
Conclusion
Coupled plasmafiltration-adsorption was a feasible and safe extracorporeal treatment and exerted a remarkable improvement in the hemodynamics, the pulmonary function, and the outcome in septic shock patients with or without concomitant ARF.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sepsis is a major cause of morbidity and mortality in intensive care units (ICUs) worldwide [1] as it is a well-known primary cause of multiple organ dysfunction syndrome (MODS).
The mortality rates in sepsis are still very high, ranging from 20 to 70% depending on the severity of the disease, the times of treatment initiation, the number of affected organs, and the study design [2]. It has been recently described as the tenth most common cause of death in North America [3].
Sepsis, especially septic shock, is also a leading cause of acute renal failure (ARF) in ICUs [4]. Accordingly, the prevalence of ARF in sepsis ranges from 9 to 40% [5] and in a prospective study [6] the incidence rose from 19% in sepsis to 23% in severe sepsis to 51% in septic shock.
Extracorporeal therapies for ARF in ICU patients are widely used [7]: membranes with highly hydraulic permeability achieve increased ultrafiltration rates and solutes removal in the range of 5–50 kDa [8].
Continuous renal replacement therapy (CRRT) has become popular for treating critically ill patients characterized by high hemodynamic instability, fluid overload, and the need for high therapeutic and nutritional volumes.
More specific approaches have been proposed such as high-volume hemofiltration and continuous plasmafiltration [9, 10] in order to remove several pro- and anti-inflammatory mediators and to overcome the limitations of conventional CRRT (i.e., low volume exchange and low sieving coefficients for sepsis-associated mediators).
In order to improve the efficacy of a blood purification system in critically ill septic patients, unselective adsorption on a cartridge was added to plasmafiltration and conventional diffusion/convection in a newly designed extracorporeal device called coupled plasmafiltration-adsorption (CPFA).
Studies of this technique recently reported improved hemodynamics and survival in animal [11] and human [12] sepsis.
The aim of this study was to examine the safety and feasibility of repeated applications of CPFA and their effects on cardiac output, extravascular lung water, end-diastolic volume, and survival in septic shock patients with or without the presence of concomitant ARF.
Materials and methods
Patients
Twelve consecutive (June 2001–April 2002) mechanically ventilated patients admitted to one single center ICU with a clinical picture of septic shock according to the American College of Chest Physicians/Society of Critical Care Consensus conference criteria [13]. Acute Physiology and Chronic Health Evaluation II (Apache II) score [14] was used to assess the severity of patients' clinical conditions. This was calculated at the time of nephrology consultation before the CPFA started. All patients started CPFA within 6 h of diagnosis. Exclusion criteria were pregnancy, age less than 18 years, neoplasm, clinically overt AIDS disease, previous organ transplantation or previous chronic dialysis. Vascular access was with dual-lumen catheter (12 FG/4 mm, polyurethane, 20 or 16 cm length; Arrow, Reading, PA, USA) indwelled in a femoral or internal jugular vein. The design was a prospective, intention-to-treat study. The study was approved by the Regional Ethics Committee, to whom it was submitted in the unusual circumstances of including patients without renal failure. Informed consent was requested, obtained and signed by the legal proxy. Normal renal function was defined as serum creatinine concentration within a normal range according to surface area and laboratory reference values, with no variation during the ICU stay, and urinary output above 50 ml/h. Norepinephrine and dopamine vasopressors were used as base protocol. In some cases, epinephrine and dobutamine were added to the infusions, which were titrated according to the hemodynamic response to CPFA. In some of the patients (with relative adrenal insufficiency) hydrocortisone (50 mg intravenous bolus every 6 h) was added as well, in order to reduce the norepinephrine requirement.
Coupled plasmafiltration-adsorption
Coupled plasmafiltration-adsorption (Fig. 1) was performed using a three-pump, modular extracorporeal blood purification system (Multimat B.IC, Bellco, Mirandola, Italy) consisting of a plasmafilter (0.45 m2 polyethersulfone, with approximate cut-off of 800 kDa, MPS 05, Bellco SpA) and adsorption on a unselective hydrophobic resin cartridge (70 g, with a surface of about 700 m2/g), and a synthetic, high-permeability, 0.7 m2 polyethersulfone hemofilter (BLS 707, Bellco SpA).

Scheme of coupled plasmafiltration-adsorption
Continuous veno-venous hemodialysis (CVVHD) or hemofiltration (CVVH) were used in ARF and non-ARF patients, respectively. Cartridges were changed every 3 h, in accordance with previous in vitro data [15]. The plasmafiltration rate was maintained at around 30–40 ml/min and the blood flow rate ranged from 150 to 180 ml/min (filtration fraction maintained about 20 to 22). Dialysate flow and reinfusion flow rates were 40 ml/min and 25 ml/min in post-dilutional mode.
Sterile bicarbonate-based buffer solutions were used as dialysate or reinfusate fluid, with the following composition (mMol/l): Na+: 140, K+: 1.5, Ca++: 2, Mg++: 0.75, Cl+: 108, bicarbonate: 35, acetate: 4, glucose: 5.55 (CB 35, Fresenius Kabi, Isola della Scala, Italy). The fluids were administered at room temperature.
Blood was anticoagulated by means of unfractionated heparin titrated on patients' PTT (targeting 60 s) or clotting time. In one patient with subarachnoid hemorrhage no heparin was used, but pre-dilutional CPFA and intermittent rinsing of the extracorporeal circuit with saline were performed.
All sessions were isovolemic according to the residual diuresis of all the patients.
Hemodynamic/physiological variables
Hemodynamic variables were monitored with the Picco system (Pulsion Medical System, Munich, Germany) [16]: before starting, every 2 h during treatment and 2 and 4 h after the end of treatment, data were recorded about mean arterial pressure (MAP), heart rate, cardiac output, cardiac index (CI), systemic vascular resistance index (SVRI), intra-thoracic blood index (ITBI), extra-vascular lung water (ELWI), central venous pressure, oxygenation ratio (PO2/FIO2), diuresis, body core temperature.
Hematological/inflammatory variables
Blood counts and antithrombin III levels were measured every day at the beginning of the treatment.
Pre- and post-session C reactive protein (CRP) dosage was determined.
Statistics
Raw data are reported as mean ± SD and 95% confidence interval (CI) or mean and median. Differences of baseline values vs. changes of variable after treatment were evaluated using the Student's paired sample t-test or the Wilcoxon signed rank test, as appropriate. Normality was assessed by the Kolmogorov-Smirnov test, with the Shapiro-Wilk correction for samples <50. For hemodynamic variables concerning the first day of treatment, not normally distributed, the Wilcoxon signed rank test was applied and analysis of variance was used to assess differences in respect to the following days of treatment. A p value of <0.05 was considered statistically significant. The analysis was performed using the SPSS 9.0 statistical software package (SPSS, Chicago, IL, USA).
Results
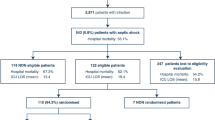
Only data gathered from patients who survived for more than 48 h after diagnosis were analyzed. We obtained valid data, according to the inclusion/exclusion criteria, from 10 patients, 7 males and 3 females (mean age 54±16), who underwent a median of 10 CPFA treatments (range 4–18, total 100 sessions).
The Apache II score before treatments was 24.8±5.6. All patients had multiorgan failure, with 2.8±1.1 organs involved (Table 1). Six out of ten patients had normal renal function.
Mean urinary output was 2,692±1,183 ml/day. Two patients were not included in the final analysis. One patient (male, 35 years old, with no ARF) died 37 h after diagnosis (two CPFA treatments run) during emergency surgery for post-traumatic mediastinitis. Another patient (male, 73 years old, with non-oliguric ARF) was transferred to another ICU after 24 h (1 CPFA treatment run).
Five patients showed pulmonary infections (due to isolated Pseudomonas aeruginosa, Klebsiella pneumoniae/oxytoca, Escherichia coli, Streptococcus agalatiae, Stenotrophomonas maltophilia, Staphylococcus aureus, Enterobacter cloacae), 3 patients had abdominal infections (due to Pseudomonas aeruginosa, Escherichia coli, Enterococcus faecalis), 1 had a urinary tract infection (Enterococcus faecalis) and in 1 patient no bacterial agent could be isolated.
Mean arterial pressure, cardiac index, systemic vascular resistance index and PO2/FIO2 ratio improved during treatments and worsened again during the overnight wash-out periods, with a global trend to a significant amelioration for every variable (Figs. 2, 3, 4).

Mean arterial pressure (MAP) trend throughout the first 10 sessions (each point is the mean of the measure at that time for all patients: n=10 from treatments 1 to 4; n=9 from treatments 5 to 7; n=8 treatment 8; n=7 treatment 9; n=6 treatment 10). Statistical significance is related to the difference between all 100 pre- vs. post-treatment measurements

Cardiac index (CI) trend throughout the first 10 sessions (each point is the mean of the measure at that time for all patients: n=10 from treatments 1 to 4; n=9 from treatments 5 to 7; n=8 treatment 8; n=7 treatment 9; n=6 treatment 10). Statistical significance is related to the difference between all 100 pre- vs. post-treatment measurements

PO2/FIO2 trend throughout the first 10 sessions (each point is the mean of the measure at that time for all patients: n=10 from treatments 1 to 4; n=9 from treatments 5 to 7; n=8 treatment 8; n=7 treatment 9; n=6 treatment 10). Statistical significance is related to the difference between all 100 pre- vs. post-treatment measurements
Statistically significant improvements were recorded about the differences before each treatment/after each treatment (n=100) concerning MAP 77.2±12.5 (CI 95%; 74.5–79.8) vs. 83.3±14.1 (CI 95%; 80.3–86.3) mm Hg (p<0.001), CI 4.03±0.89 (CI 95%; 3.83–4.22) vs. 3.46±0.82 (CI 95%; 3.28–3.64) l/m2/min (p<0.001), SVRI 1,388±496 (CI 95%; 1,278–1,497) vs. 1,753±516 (CI 95%; 1,639–1,867) dynes × s/cm5 (p<0.001), PO2/FIO2 ratio 204±87 (CI 95%; 185–223) vs. 238±82 (CI 95%; 220–256) (p<0.001) (Student's paired sample t-test applied). Concerning Picco calculated volumes, ITBI and ELWI were almost unchanged (819±154 vs. 780±144 ml/m2 and 10±3.8 vs. 10.1±3.9 ml/kg, respectively). A statistically significant difference was recorded between the values pre- and post-treatment on the first day concerning MAP (68.1±6.6 [CI 95%; 63.3–72.8] vs. 83.4±18.4 [CI 95%; 70.2–96.5] mm Hg [p=0.037]), CI (3.88±0.78 [CI 95%; 3.32–4.44] vs. 3.32±0.75 [CI 95%; 2.79–3.86] l/m2/min [p=0.022]), and SVRI (1,212±267 [CI 95%; 1,021–1,402] vs. 1,633±471 [CI 95%; 1,295–1,970] dynes × s/cm5 [p=0.007, Wilcoxon signed rank test applied]). The analysis of variance of the three variables as different treatments on different days showed non-statistically significant differences (MAP p=0.303, CI p=0.585, SVRI p=0.686). At the same time points (pre- and post-treatment on the first day), ITBI and ELWI were both almost unchanged (792±167 vs. 809±254 ml/m2 and 12.8±5.6 vs. 12.2.1±4.2 ml/kg, respectively).

C reactive protein (CRP) values before first treatment and after last treatment (mean of ten patients)
Table 2 outlines the effects of the first CPFA treatment on the main measured variables, showing a positive, acute influence on each one.
Norepinephrine need decreased from an infusion rate of 0.13±0.07 (CI 95%; 0.06–0.16) to 0 γ/kg/min after a mean of 5.3±2.7 consecutive treatments.
All patients but three were discharged from ICU after a mean of 38±24 days (range 10–93). The survival rate at day 28 was 90%. One patient (admitted for subarachnoid hemorrhage) died, after four CPFA treatments, of a massive infarction of the cerebral mass. The survival rate at 3 months was 70%; in fact, 1 patient died on day 40 of a relapse of post-traumatic septic shock in another hospital ICU, and 1 died on day 35 of a subsequent infection of an abdominal vascular prosthetic graft, which could not be removed by the surgeons.
Laboratory data showed a sharp decline of CRP throughout the treatment time (before the first treatment until after the last treatment) from 29.3±7.3 to 7.9±4.8 mg/l (−73%; p<0.0001) (Fig. 5).
Platelet counts and antithrombin III levels were unaffected by treatment: they both showed a non-significant increase during treatment.
All patients with ARF recovered with no further need of dialysis.
No relevant technical failure was recorded. In 26 cases the session had to be prematurely stopped (prescribed duration of the session: 10 h; delivered duration: 8.43±1.37 h/min): in 5 cases for clinical reasons (diagnostic evaluation, emergency surgery) and in 21 cases because of technical problems (mostly device software failure and plasmafilter malfunction/circuit coagulation, mainly in the first months of the study).
The mean dose of sodium heparin used was 1,011±428 U/h (range 844–1,750).
Discussion
The prognosis of septic shock patients with MODS remains poor [1, 2, 3]. Furthermore, its incidence is projected to increase 1.5% per annum due to the growth of predisposing segments of the population, particularly the elderly [17].
The issue of the contributory beneficial effect of blood purification techniques, namely CVVH or high-volume hemofiltration, in severe sepsis-septic shock remains controversial [18, 19, 20, 21] and recently published guidelines stated that "hemofiltration should not be used in patients with sepsis without renal indications unless ongoing studies provide positive results" [22].
Some technological advances in this field were described by Ronco et al. [12] in a pilot study using CPFA in septic shock patients in which they reported a significant improvement in MAP, norepinephrine requirement, and cardiac index. This study followed a preliminary observation in an animal experiment where 72 h cumulative survival was a significant improvement in CPFA-treated septic rabbits [11].
In March 2001 we obtained Regional Ethics Committee approval for the use of CPFA in ICU-hospitalized patients with septic shock independently of the presence of concomitant ARF. In this long-term study, we showed CPFA to be a safe and feasible treatment with significant improvement in hemodynamic stability, vasopressor requirement, pulmonary function, and 28- and 90-day survival. The 28 days survival rate was 90%, which was quite unexpected considering an Apache II-predicted mortality for these patients of about 40%.
It was very impressive to see the same modification of the single variable studied in every patient, with a repetitive sawteeth pattern of improvement during treatment and a worsening in the overnight wash-out periods, but with a global trend toward a significant amelioration over time. This was evident for all the hemodynamic variables (MAP, CI, SVRI, PO2/FIO2 ratio, and significantly reduced or even abrogated the vasopressor requirement).
Data concerning ITBI and ELWI, as expected, did not reveal any particular pattern over time: they were mainly used as extra information for cardiac filling, together with central venous pressure, the response to fluid challenge, the systolic pressure variation, the pulse pressure variation, and the urinary sodium excretion, but not as variables directly influenced by treatment. We may have expected a reduction of ELWI over time as an effect of the reduced inflammation: this was not the case in our observations, probably because the effect may take more time.
Taken together these results strengthen the hypothesis of CPFA-induced ameliorated hemodynamic performance without substantially affecting thoracic volumes.
No untoward clinical effects were recorded during the procedures, which confirms the safety of the technique. Some technical problems occurred in 21% of the sessions but were mostly related to device software failure and plasmafilter malfunction/circuit coagulation, mainly in the first months of the study. In fact the percentage of technical failure in the last 70 treatments amounted to only 8.5% (n=6).
As suggested in experimental and human studies, the described effects could be related to the unselective removal of cytokines involved in the pathophysiology of sepsis and in the immunomodulating effect. Avoiding the peak concentrations of different immunoactive mediators may represent a non-specific cytokine "magic shield" and could achieve a significant attenuation of the acute-phase response. The levels of PCR, IL-6, IL-10, and ICAM-1, occasionally measured in some patients in this study (data not reported), showed a decremental trend (from 13 to 73%) throughout a single CPFA session, also suggesting an effective body clearance beyond a reduced inflammatory state, according to previous studies [23, 24, 25].
However, this study has several limitations. Firstly, it was not a controlled/randomized study; for this reason we are now planning a phase II trial comparing this treatment with other two arms, one of patients receiving usual medical care and another using high-volume hemofiltration.
Secondly, this is a small sample size study and statistically significant reports should be confirmed with a large scale trial.
Thirdly, due to the small sample size, we could not divide the patients according to the presence or absence of ARF. We therefore cannot state what is the impact of this clinical condition, if any, on outcome [26]. Moreover, we think this study clearly underlines one of its premises, i.e., the use of this specific technique for septic shock irrespective of renal involvement.
Fourthly, a "high" dosage of heparin was used. The influence of this drug on the coagulation-inflammation process during sepsis has not been studied so far, and a possible improvement in mortality due to this pharmacological approach per se cannot be excluded [27].
Nevertheless, taking into consideration the high mortality rate of septic shock, this procedure might be beneficial in improving the outcome and suggests the benefit of early intervention in ICU-hospitalized patients with septic shock, before acute renal failure eventually develops. Indeed it seems the technique may be applied to prevent rather than to treat ARF.
The association of improved survival, ameliorated hemodynamics, and restoration of immune balance in CPFA-treated septic shock patients deserves further confirmation in a prospective trial tailored to these specific premises.
References
Friedman G, Silva E, Vincent JL (1998) Has mortality of septic shock changed with time? Crit Care Med 26:2078–2086
Wheeler AP, Bernard GR (1999) Treating patients with sepsis. N Engl J Med 340:207–214
USA National Vital Statistics Report (2001) 49:6
Liano G, Pascual J (1996) Acute renal failure. Madrid Acute Renal Failure Study Group. Lancet 17:347–349
Thijs A, Thijs LG (1998) Pathogenesis of renal failure in sepsis. Kidney Int 53 [Suppl 66]:S34–S37
Rangel-Frausto MS, Pittet D, Costigan M (1995) The natural history of the systemic inflammatory response syndrome (SIRS). A prospective study. JAMA 273:117–123
Bellomo R, Ronco C (1998) Indications and criteria for initiating renal replacement therapy in the intensive care unit. Kidney Int 53 [Suppl 66]:S106–S109
Kellum JA, Johnson JP, Kramer D, Pavelsky P, Brady JJ, Pinsky MR (1998) Diffusive vs. convective therapy: effects on mediators of inflammation in patient with severe systemic inflammatory response syndrome. Crit Care Med 26:1995–2000
Bellomo R, Baldwin I, Cole L, Ronco C (1988) Preliminary experience with high volume hemofiltration in human septic shock. Kidney Int 53:182–185
Reeves JH, Butt WW, Shann F, Layton JE, Stewart A, Waring PM, Presneill JJ (1999) Continuous plasmafiltration in sepsis syndrome. Crit Care Med 27:2096–2104
Tetta C, Gianotti L, Cavaillon JM, Wratten ML, Fini M, Braga M, Bisagni P, Giavaresi GL, Bolzani R, Giardino R (2000) Continuous plasmafiltration coupled with sorbent adsorption in a rabbit model of endotoxic shock. Crit Care Med 28:1526–1533
Ronco C, Brendolan A, Lonnemann G, Bellomo R, Piccinni P, Digito A, Dan M, Irone M, La Greca G, Inguaggiato P, Maggiore U, De Nitti C, Wratten ML, Ricci Z, Tetta C (2002) A pilot study on coupled plasma filtration with adsorption in septic shock. Crit Care Med 30:1250–1255
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RMH, Sibbald WJ (ACCP/SCCM Consensus conference committee (1992) Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest 101:1644–1655
Knaus WA, Draper EA, Wagner DP, Zimmerman JE (1985) APACHE II: a severity of disease classification system. Crit Care Med 13:818–829
Tetta C, Cavaillon JM, Schulze M, Ronco C, Ghezzi PM, Camussi G, Serra AM, Curti F, Lonnemann G (1998) Removal of cytokines and activated complement components in an experimental model of continuous plasma filtration coupled with sorbent adsorption. Nephrol Dial Transplant 13:1458–1464
Godje O, Hoke K, Fischlein T, Vetter H, Reichart B (1996) Less invasive, continuous cardiac output measurement through pulse contour analysis versus conventional thermal dilution. Intensive Care Med 22:S58
Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR (2001) Epidemiology of severe sepsis in the United States: analysis of incidence, outcome and associated costs of care. Crit Care Med 29:1303–1310
De Vriese AS, Vanholder RC, De Sutter JH, Colardyn FA, Lameire NH (1998) Continuous renal replacement therapies in sepsis: where are the data? Nephrol Dial Transplant 13:1362–1364
Ronco C, Bellomo R, Homel P, Brendolan A, Dan M, Piccinni P, La Greca G (2000) Effect of different doses in continuous veno-venous haemofiltration on outcomes of acute renal failure: a prospective randomized trial. Lancet 356:26–30
Cole L, Bellomo R, Journois D, Davenport P, Baldwin I, Tipping P (2001) High-volume hemofiltration in human septic shock. Intensive Care Med 27:978–986
Cole L, Bellomo R, Hart G, Journois D, Davenport P, Tipping P, Ronco C (2002) Crit Care Med 30:100–106
Carlet J (2001) Immunological therapy in sepsis: currently available. Guidelines for the management of severe sepsis and septic shock. Intensive Care Med 27:S93–S103
De Vriese AS, Colardyn FA, Philippe JJ, Vanholder RC, De Sutter JH, Lameire NH (1999) Cytokine removal during continuous hemofiltration in septic patients. J Am Soc Nephrol 10:846–853
Opal SM (2000) Hemofiltration-absorption systems for the treatment of experimental sepsis: is it possible to remove the "evil humors" responsible for septic shock? Crit Care Med 28:1681–1682
Yekebas EF, Eisenberger CF, Ohnesorge H, Saalmuller A, Elsner HA, Engelhardt M, Gillesen A, Meins J, The M, Strate T, Busch C, Knoefel WT, Bloechle C, Izbicki JR (2001) Attenuation of sepsis-related immunoparalysis by continuous veno-venous hemofiltration in experimental porcine pancreatitis. Crit Care Med 29:1423–1430
Schor N (2002) Acute renal failure and the sepsis syndrome. Kidney Int 61:764–776
Langer M, Riccardi F, Piovella F, Klersy C (2002) Use of anticoagulants in patients with sepsis. JAMA 287:448–489
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Formica, M., Olivieri, C., Livigni, S. et al. Hemodynamic response to coupled plasmafiltration-adsorption in human septic shock. Intensive Care Med 29, 703–708 (2003). https://doi.org/10.1007/s00134-003-1724-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-003-1724-0