
Abstract
Introduction
Mental illness stigma is prevalent among Asian Americans, and it is a key barrier that prevents them from seeking psychological services. Limited studies have experimentally examined how Asian Americans respond to biological and social explanations of mental illness. Understanding how to educate and communicate about mental illness effectively is crucial in increasing service utilization among Asian Americans.
Purpose
To assess how genetic, neurobiological, and social explanations for the onset of depression affects Asian American and European American’s mental illness stigma.
Methods
231 Asian Americans and 206 European Americans read about an individual with major depression and were randomly assigned to be informed that the cause was either genetic, neurobiological, social, or unknown. Various stigma outcomes, including social distance, fear, and depression duration were assessed.
Results
Consistent with prior research, Asian Americans had higher baseline levels of stigma compared to European Americans. Greater social essentialist beliefs predicted positive stigma outcomes for Asian Americans, such as a greater willingness to be near, help, and hire someone with depression, but genetic essentialist beliefs predicted negative stigma outcomes, such as fear. In addition, a social explanation for the etiology of depression led to lower stigma outcomes for Asian Americans; it decreased their fear of someone with depression and increased the perception that depression is treatable. For European Americans, both genetic and social essentialist beliefs predicted a greater perception of depression treatability.
Conclusion
Although genetics do play a role in the development of depression, emphasizing a social explanation for the origin of depression may help reduce stigma for Asian Americans.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Asian Americans underutilize almost all forms of mental health services compared to European Americans, despite experiencing mental illness [1]. Depression is the second leading cause of death for Asian Americans, and they show higher levels of depressive symptoms than European Americans [2]. One of the key barriers to seeking clinical services is stigma, which most researchers define as a negative stereotype that places the labeled person into a distinct group where there is potential status loss and discrimination [3]. Mental illness stigma is pervasive among ethnic minorities in general, but because of the cultural emphasis on saving “face” or upholding a social reputation, Asian Americans may be particularly stigmatized by mental health problems [4, 5]. Stigma is one of the primary reasons why many Asian Americans defer seeking treatment [1, 5, 6].
Stigma has adverse effects on people’s quality of life, job opportunities, and utilization of mental health services; therefore, lowering stigma is a crucial public priority [7–9]. In recent years, public education campaigns have focused primarily on genetic explanations of mental illness [10, 11], despite research showing that mental illnesses are caused by a variety of factors [12–14]. It is unclear how genetic explanations affect Asian Americans, or whether emphasizing an alternative explanation would be beneficial in lowering stigma among this population. One of the key ways to reduce stigma is through education [15], and thus finding the most culturally effective way to educate the public about mental illnesses is critical to lowering stigma.
Genetics and stigma
In an effort to shift the blame away from those diagnosed with a mental illness, there has been an increased tendency toward emphasizing the genetic origins of mental illnesses in psychoeducation and anti-stigma campaigns [10, 11]. Genetic explanations can have both positive and negative effects on different stigma components. According to attribution theory [16], genetic explanations can lead to a decrease in blame because of the perception that people are not responsible for their genes. Research shows that genetic explanations for depression are associated with greater acceptance [17]. Despite genetic explanations reducing blame, genetic essentialism theory predicts that people will perceive a mental illness caused by genes to be inherent and permanent. Studies have shown that a genetic portrayal of mental illness leads to increased fear and social distance [18–20], in addition to increased anger toward someone with depression [11]. Overall, studies with predominantly European American samples show that endorsement of a genetic origin of mental illness is related not only to benefits such as decreased blame and increased acceptance of certain mental illnesses, but also to costs such as increased fear and social distance.
Genetic essentialism may have culture-specific effects, in particular for Asian Americans. In contrast to European American cultures, there is a greater emphasis on social harmony and maintenance of a family’s reputation or “face” in Asian cultures [21–23]. Because genes are hereditary, genetic attribution can be associated with higher levels of stigma because it threatens social harmony and family lineage. To the author’s knowledge, only two studies have experimentally examined the impact of genetic explanations on Asian Americans’ level of stigma, and they have yielded mixed findings. One study with Chinese Americans found that genetic explanations increased willingness to date someone with a mental illness, suggesting a positive effect of genetic explanation [19]. However, another study found that Chinese Americans were more likely to endorse the importance of genetic screening and knowing one’s family history of mental illness [24]. Chinese Americans given a genetic explanation were also more likely to recall information about the genetic transmission of mental illness compared to those in the non-genetic condition, perhaps because they found this information to be threatening. Altogether, more research is needed to clarify how Asian Americans react to genetic explanations of mental illness.
Neurobiology and stigma
A neurobiological model of mental illness (e.g., depression is due to imbalances in the levels of neurotransmitters in the brain) has been hypothesized to function similarly to genetic essentialism, where it will be associated with negative stigma outcomes such as fear and increased social distance [25]. Studies with predominantly European American samples show that endorsement of a neurobiological cause for depression is related to increases in social distance, suggesting neuroessentialism [26]. Nonetheless, studies have also found neurobiological explanations to be associated with greater endorsement of treatment, less blame, and no greater desire for social distance [18, 26, 27]. A neurobiological explanation may differ from a genetic explanation in that it does not necessarily have the heritability, and thus the intergenerational transmission, that is tied with genetic essentialism. Prior studies tended to combine genetic and neurobiological causes together, and therefore it is important to experimentally examine whether they will lead to differential effects on stigma.
Asian Americans may prefer a neurobiological explanation because genes can be passed onto family members. Asian Americans with depression tend to emphasize somatic symptoms (e.g., lack of appetite) rather than psychological symptoms (e.g., feelings of depression) possibly because they associate less stigma with physical illness [27]. Reframing mental illness such as depression as being caused by an imbalance of brain chemicals is also more congruent with certain cultural conceptualization of illness [28]. For example, in Chinese medicine, there is an emphasis on balancing the energy levels within the body [28]. Explaining to Asian Americans that anti-depressants will restore and harmonize the imbalance of brain chemicals has been hypothesized as a culturally appropriate way to reframe Western conceptualization of depression [28]. Thus, a biological explanation such as the imbalance of brain chemicals may be a better alternative because it allows mental illness to be conceptualized as a temporary “brain disease.”
Social factors and stigma
Essentialism is not solely connected to genetics or neurobiology. Social essentialism, the belief that a person’s essential character is shaped by social factors, such as upbringing, social background, and socialization, is also a common belief [29]. The social explanation of depression is associated with lower acceptance of those with depression and increased perception of responsibility (i.e., blame) for their mental illness [20, 27]. Therefore for European Americans, social attribution may be related to an increase in blame, although it remains unclear how it is associated with other stigma outcomes. For Asian Americans, psychosocial stressors can be perceived to reflect family conflict [31], thus a social explanation may also increase blame. There has been a lack of research examining the impact of social attribution on Asian Americans’ mental illness stigma, and thus, more research is needed for clarification.
The present study
The objective of this research is to answer the following questions: (1) How will genetic and social essentialist beliefs predict stigma levels for Asian Americans and European Americans?; and (2) What is the explanation (i.e., genetic, neurobiological, and social) that will best lower stigma for Asian Americans and European Americans? It is hypothesized that (1) for Asian Americans, genetic essentialist beliefs will predict negative stigma outcomes; for European Americans, genetic essentialism will predict decreases in blame, but increases in social distance and fear. Social essentialist beliefs are hypothesized to predict increased blame for both groups; (2) For Asian Americans, a neurobiological explanation will lead to the lowest level of stigma, especially for the perception that depression is less enduring and more treatable than one caused by genes; for European Americans, a social explanation will lead to the lowest level of stigma compared to the biological explanations, although it may be associated with increased blame.
Methods
Participants
552 participants were recruited and compensated through Qualtrics Panel, a national online survey agency.Footnote 1 Those who reported having a mental illness (N = 75) and those who indicated minimal English language ability were excluded (N = 9). Those who completed the study in less than 5 min (N = 31; M = 25.5 min) were excluded because rushing through the experiment was considered problematic. A remaining sample of 437 participants included 231 Asian Americans (66 % female; mean age = 21.2, SD = 2.43) and 206 European Americans (63 % female; mean age = 23.9, SD = 8.65). There were roughly 50 participants in each condition. This sample size is consistent with prior studies of similar nature [19, 24], and has a power of 0.80 to detect differences at the alpha level of 0.05 for effect size of d = 0.25.
78 % of the Asian American and 96 % of the European American participants were born in the United States. The average time Asian Americans spent in the US was 18.01 years. Of the Asian Americans who were born outside of the US (N = 44), most were born in East Asia (i.e., 61 % reported being born in China/Hong Kong, Korea, Japan and Taiwan) or in Southeast Asia (i.e., 27 % reported being born in the Philippines, Vietnam, Thailand, Indonesia, etc.). Participants’ education level ranged from “some high school” to “graduate degree”. The modal response was “some college” for both ethnic groups, given that 37 % of the respondents were college students. The second highest educational attainment was “college degree” for Asian Americans, and “high school degree” for European Americans. Participants’ annual household income ranged from less than $25,000 to more than $120,001. For Asian Americans, the modal response was $40,001 through $70,000, while for European Americans, it was $25,000 or less. Due to the large discrepancy in income between the two samples, income was statistically controlled in all data analyses. In addition, age and education were also controlled to precisely parse out the effects of the depression explanation on stigma levels.
Design and materials
All of the study materials were completed online, and all study protocols were approved by the appropriate institutional review board.Footnote 2
Vignettes Participants first read a vignette describing a man named J.S. who was diagnosed with depression. J.S.’s symptoms were described in lay language using the criteria for depression from the Diagnostic and Statistical Manual of Mental Disorders IV [32] and modified after a previously used depression vignette [33] (see Supplementary Materials). The person in the vignette was male to control for gender effects [34]. Depression was chosen because it is a recognizable mental illness that the public believes to have various causes, and because of its negative impact on Asian Americans [2, 35, 36].
Participants were randomized to read an explanation given by a psychiatrist and experts regarding the cause of J.S.’s depression. In the genetic condition, participants were told that the experts found that J.S. had a genetic predisposition for depression and a family history of depression. In the neurobiological condition, the doctors found that J.S. had an imbalance of brain chemicals. In the social condition, the experts found that J.S. recently went through a divorce and lost his best friend at a young age. In the control condition, participants were told that the doctors could not uncover the cause.
Stigma outcomes After reading the vignette and explanation, participants answered a series of questions regarding their affective reactions and behavioral intentions using a scale that is commonly designed to assess the stigmatization of an individual [3]. They provided ratings on 5 social distance questions [33] to assess how willing they were to interact with the individual depicted in the vignette (1 = definitely not, 6 = definitely yes). These responses were averaged to create a composite (α = 0.89) and reverse coded with low numbers indicating less social distance from those with a mental illness. Participants answered questions regarding fear (4 items) and blame (3 items) using a 9-point Likert rating scale (1 = not at all, 9 = very much) from the Attribution Questionnaire [36]. Responses were averaged to create a composite for fear (α = 0.92) and blame (α = 0.77). In addition, three other items were created to assess how essential and enduring participants perceived depression to be. They rated how long they thought J.S. would have depression (range 1–3 months to more than 2 years), how treatable they thought his depression would be, and how easy it would be to treat his depression. The latter two questions were assessed using a 6-point scale (1 = definitely not, 6 = definitely yes), with low numbers indicating greater difficulties in treating depression. There were a priori hypotheses regarding these essentialism stigma variables, thus an alpha level of 0.05 was used for all statistical tests associated with these outcomes.Footnote 3
In addition, helping questions [34] assessed participants’ willingness to offer emotional support, to give the person advice, to perform a small favor, and to offer help in general (1 = definitely not, 6 = definitely yes). Responses were averaged to create a composite (α = 0.90). The Attribution Questionnaire also contains items associated with hiring/renting (4 items), pity (3 items), and anger (3 items). Composite measures of hiring/renting (α = 0.88), pity (α = 0.74) and anger (α = 0.90) were created by averaging the questions measuring those emotions. There were no a priori hypotheses concerning these variables, thus a Bonferroni correction with an alpha level of 0.0125 was used for these analyses.
Predictors and other measures The Beliefs in Genetic Essentialism Scale [37] consists of 18 items reflecting the perception that characteristics such as intelligence, personality, and sexual orientation are primarily determined by genetic factors (1 = not true at all, 7 = completely true). Responses were averaged to create a composite (α = 0.84) with higher scores indicating a greater agreement that one’s essence is genetically determined. The Beliefs in Social Essentialism Scale [30] consists of 12 items that assess the belief that human behavior and character are determined by social factors. Responses were again averaged to create a composite (α = 0.81) with higher scores indicating a greater agreement that one’s essence is determined by social factors. These scales were used to examine how general genetic and social essentialist attitudes predict stigma levels.
Contact is associated with lower stigma [15], therefore, participants were also given Corrigan’s modified level of contact survey [38]. As noted earlier, those who reported having a mental illness were excluded so that self-stigma would not confound the experimental results. Loss of Face Questionnaire [39] was included as a cultural variable, which consisted of 21 items to assess the extent that the participant would avoid situations and behaviors that could lead to decrease in reputation (1 = strongly agree, 7 = completely true). Responses were averaged to create a composite (α = 0.87). Loss of Face was found to not mediate or moderate the results using Preacher and Hayes’ method [41], and thus this scale will not be mentioned again. Questions regarding basic demographics and manipulation check questions were also included at the end of the experiment.Footnote 4
Analyses
An alpha level of 0.05 was used for all statistical tests associated with essentialism stigma outcomes (i.e., social distance, fear, blame, duration, treatability), and a Bonferroni corrected alpha level of 0.0125 was used for other outcomes.
Regression Hierarchical linear regression was first used to examine whether genetic and social essentialism predicted stigma outcomes differently according to race, and it was found that it did not. Because of a theoretical interest in genetic and social essentialism for both groups, regression analyses were used to examine how genetic and social essentialist beliefs predict stigma outcomes while controlling for the manipulation variable. Key demographic variables (i.e., age, education, income) along with the participant’s condition explanations were simultaneously entered into Model 1 equations to control for any potential confounding. Significant associations with genetic and social essentialism scores from Model 2 were reported only if the overall model was significant.
Vignette analyses A four (condition: genetic, neurobiological, social, and unknown explanation) by two (race: Asian American and European American) Factorial ANCOVA controlling for age, education, and income was first conducted. There was no significant interaction between condition and race for each of the stigma outcomes. Because of a theoretical interest in examining what explanation will best lower stigma for both groups, separate analyses using ANCOVA were conducted for each sample.
Results
Ethnic differences in stigma levels
Descriptive statistics are reported in Table 1. A univariate analysis of variance controlling for age, income, and education showed that Asian Americans reported significantly greater social distance (p = 0.004), blame (p = 0.02), anger (p = 0.002), and less willingness to hire and rent (p = 0.008) to a person with depression than European Americans did. Asian Americans were also trending to endorse greater fear of someone with depression (p = 0.54) than European Americans. Asian Americans and European Americans did not significantly differ on other outcomes. Overall, Asian Americans had significantly higher scores on many stigma measures than European Americans did.
Genetic and social essentialism predictors and stigma levels
Asian Americans For Asian Americans, genetic essentialist beliefs significantly predicted greater fear (p < 0.001) and blame (p = 0.03). Social essentialist beliefs predicted increases in willingness to be near (p < 0.001), help (p < 0.001) and hire/rent (p = 0.001) to someone with depression. Essentialist beliefs did not significantly predict other variables. Overall, genetic essentialist beliefs predicted negative stigma outcomes as hypothesized; however, social essentialist beliefs did not predict positive stigma outcomes for Asian Americans (see Table 2).
European Americans For European Americans, essentialist beliefs only predicted treatability of depression, where both genetic (p < 0.05) and social essentialism (p = 0.002) predicted a greater perception that depression is treatable.
Mental illness explanations and stigma levels
Asian Americans For stigma measurements associated with essentialism, there was a significant main effect of explanation on social distance for Asian Americans, F (3, 188) = 3.99, p = 0.009, ηρ2 = 0.06. Post hoc Tukey tests showed that those who received a social explanation were significantly more willing to be near someone with depression than those who received a genetic (p = 0.001) or neurobiological explanation (p = 0.02). Those who received a social explanation were trending to indicate more willingness to be near someone with depression than those who received no explanation (p = 0.08). There was a significant conditional effect of fear, F (3, 189) = 4.60, p = 0.004, ηρ2 = 0.07 (see Fig. 1). Post hoc Tukey tests showed that those given a social explanation were significantly less fearful of someone with depression than those given a genetic (p = 0.008), neurobiological (p < 0.001), or no explanation (p < 0.008). There was a significant main effect of condition for the duration of depression, F (3, 184) = 3.17, p = 0.03, ηρ2 = 0.05 (see Fig. 2). Post hoc Tukey tests showed that Asian Americans who received a social explanation were significantly more likely to predict a longer duration than those given no explanation (p = 0.003). There was a trend of Asian Americans who received a genetic explanation to believe in a longer duration of depression than those who were given no explanation (p = 0.06). There was also a significant main effect of explanation for the perception of depression treatability, F (3, 186) = 3.70, p = 0.01, ηρ2 = 0.06. Post hoc Tukey tests showed that those given a social explanation were significantly more likely to indicate that J.S.’s depression was more treatable than those given no explanation (p = 0.001). Those in the neurobiological condition were trending to perceive depression as being more treatable than those in the genetic condition (p = 0.06). There was no significant effect of explanation on personal responsibility beliefs/blame. Overall, a social explanation elicited lower levels of essentialism stigma outcomes, especially when compared to a genetic explanation, although the social explanation increased the perception that depression would last longer.

A social explanation for depression tended to decrease stigma for Asian Americans. For example, it lowered fear toward someone with depression. Higher scores indicate greater fear. Error bars indicate ±2 standard error

Although a social explanation for depression tended to decrease stigma for Asian Americans, it also increased the perception that depression would last longer. Higher numbers indicate longer duration. Error bars indicate ±2 standard error
For other stigma outcomes, there was a significant main effect of explanation for helping, F (3, 189) = 3.96, p = 0.005, ηρ2 = 0.07. Asian Americans who received a genetic explanation were significantly less willing to help an individual with depression than those who received a social (p = 0.001) or no explanation (p = 0.004). Participants in the genetic condition were trending to offer less help than those in the neurobiological condition (p = 0.07). A marginal significance for the effect of explanation on hiring/renting was found, F (3, 189) = 2.90, p = 0.04, ηρ2 = 0.04. Post hoc Tukey tests showed that those given a social explanation were significantly more likely to hire someone with depression than those given a genetic explanation (p = 0.004), and were trending to be more willing to hire someone with depression than those given no explanation (p = 0.09). There was no significant main effect of explanation for pity or for anger. Overall, there is consistency between the regression and experimental results for Asian Americans, with both demonstrating that the social explanation predicted lower stigma. The essentialism scales did not moderate or mediate these results. Descriptive statistics for these results are reported in Table 3.
European Americans There was no significant main effect of explanation for any of the stigma outcomes, except for a marginal significance for the effect of explanation on fear, F (3, 140) = 2.24, p = 0.09, ηρ2 = 0.05. Post hoc Tukey tests showed that those in the genetic condition were significantly more afraid of someone with depression than those in the neurological (p = 0.02) and social conditions (p = 0.03). Again, the essentialism scales did not moderate or mediate the results.
Discussion
Asian Americans At baseline, Asian Americans reported significantly greater stigma (e.g., social distance, blame, and anger) toward those with depression than European Americans did. This finding is consistent with prior research demonstrating that stigma is a barrier that prevents many Asian Americans from utilizing clinical services [1, 4, 5]. Both the regression and experimental data consistently indicated that for Asian Americans, genetic attributions predicted negative stigma outcomes while social attributions predicted positive outcomes. More specifically, social essentialist beliefs predicted positive outcomes such as a greater willingness to be near, help, and hire someone with depression, whereas genetic essentialist beliefs predicted higher levels of stigma, such as greater fear and blame. In addition, compared to a social explanation, those given a genetic explanation were more likely to stigmatize a person with depression. Overall, Asian Americans responded best to a social explanation of depression, which led to less fear and the perception that depression is more treatable.
These results are consistent with prior studies showing Chinese Americans are more likely than European Americans to endorse genetic screening, social distance, and reproductive restriction [18, 23]. These results also correspond with WonPat-Borja and colleagues’ finding that eugenic attitudes are significantly associated with negative stigma outcomes, such as increases in social distance and reproductive restriction for Chinese Americans [19]. These findings also support Yang and colleagues’ finding that Chinese Americans given a genetic explanation were more likely to recall and recognize information about the genetic transmission of mental illness compared to those in the non-genetic condition [24]. The genetic component of mental illness threatens social harmony and family reputation when people believe mental illness can be passed onto future generations, thus threatening what matters most in Asian American cultures [23].
These results suggest that for Asian Americans social explanations for depression are de-stigmatizing, despite previous beliefs that social attributions are stigmatizing [11]. There are several plausible cultural differences that may give rise to the beneficial effects of a social explanation for Asian Americans. First, positive results may be due to cultural differences in cognition. Research with culture and cognition has found that Asian Americans tend to focus on situational and contextual influences on behaviors [43]. Thus, Asian Americans’ cognitive and perceptual styles may allow them to attribute an external and malleable cause for depression.
Second, Asian Americans tend to be concerned with family “face” or reputation [22, 23]. Prior research has shown that Chinese American families tend to endorse non-genetic explanations for the cause of mental illness [41, 42]. A social explanation for depression such as a loss of a loved one may permit Asian Americans to save face because it allows for an external cause of depression, but without the fear of genetic components contaminating their family lineage. Although Asian Americans who are divorced may experience loss of face [44], limited studies have examined whether divorce as the cause of depression would lead to loss of face among Asian Americans. This is an area that needs further investigation and could possibly explain why Asian Americans given a social explanation predicted a longer duration of depression. The longer duration suggests that Asian Americans may perceive depression caused by social factors to be treatable, but more complex, thus enduring longer. Overall, a social explanation for depression is de-stigmatizing because it is consistent with Asian Americans’ cognitive and perceptual preferences, and it also protects the reputation of one’s family although more research is needed to clarify the exact reasons as to why it is associated with longer duration.
European Americans Genetic and social essentialism predicted greater perception of the treatability of depression for European Americans. It is possible that once European Americans identify the cause of depression, people perceive it to be more treatable regardless of the explanation. The hypothesis that etiological explanations would lead to changes in stigma levels for European Americans was in general not supported. One reason European Americans’ stigma levels did not differ is because they had low baseline levels of stigma on several of the stigma variables. These low baseline levels proved difficult to significantly reduce.
One of the limitations of this study is that the explanations of genetic and social essentialism accounted for a small amount of variance in stigma levels. It is possible that the manipulation was weak in changing people’s stigma levels because it was brief, thus did not produce a strong effect. In addition, many of the explanations did not lead to differences in Asian Americans’ stigma levels in comparison to the control condition. Given that the participants in the control condition were told that the cause was unknown, there may not have been identifiable differences because participants in the control condition may have endorsed one of the other explanations to explain the onset of depression. It is also unclear what the underlying mechanism of ethnic group differences is, thus future studies should include other cultural variables. Future research can also test whether the patterns in this study would generalize to different kinds of mental illnesses, such as schizophrenia and anxiety disorders, because the target vignette described only a male with depression. Finally, because the sample had a high portion of females and college students and may not have sampled from all Asian American subgroups, there are limits to the generalization of these results.
This study, however, has important implications for anti-stigma education and mental health care. Mental illnesses, including depression, are caused by a variety of factors, encompassing those that are biological, epigenetic, and psychosocial [12–14]. Instead of educating the public regarding the various factors that contribute to mental illness, there has been a shift toward geneticizing the origin of mental illnesses in psychoeducation and anti-stigma efforts [11]. This overemphasis on genetics leads to an exclusion of other important factors. Incorporating a social explanation for the origin of depression, alongside other causes can be useful in the effort to reduce mental health stigma for Asian Americans because both proper education about mental illness and increased contact with those with a mental illness are key ways to reduce stigma [15]. In addition, therapists should discuss environmental factors that have contributed to their Asian American clients’ depression to lower stigma. This inclusion may be especially important because Asian Americans not only have one of the lowest clinical service utilizations rates, but also have one of the highest dropout rates in therapy [5]. Overall, emphasizing the contribution of environmental factors to the development of mental illnesses may provide a helpful and educational framework to adopt in future anti-stigma efforts, especially for Asian Americans.
Notes
Qualtrics Panel partners with 20 online panel providers to supply a network of diverse and quality respondents. It utilizes hundreds of profiling attributes to target potential respondents (e.g., Asian Americans). Qualtrics Panel partners randomly select respondents for surveys where respondents are highly likely to meet the requested criteria. Each sample from the panel base is proportioned to the general population and then randomized before the survey is deployed. The response rate for this study was 15 %, and included a higher percentage of college students and females.
This study was part of a larger project that included other measures (e.g., Mind and Body Dualism Scale for Asian Americans) for validation and exploratory purposes. The additional measures were administered after this study, therefore, they should not affect these reported results.
Three questions that assessed for perceived danger were also created. The composite (α = 0.36) had low reliability, thus it was excluded from data analysis.
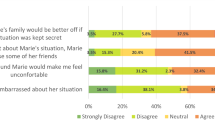
Manipulation check questions included one regarding participants’ agreement with the given explanation. Very few participants (18 Asian Americans and 9 European Americans) strongly disagreed or disagreed with the given explanation. Despite very few participants disagreeing with the given explanation, when asked what they believed to be the actual cause of J.S’s depression, the majority of the Asian Americans (62.1 %) reported that it was due to environmental factors such as life stress. The majority of European Americans believed it was either due to environmental factors (43.2 %) or neurobiological reasons (41.2 %). Because these questions were assessed after the experimental manipulation and the majority of participants still agreed with the manipulation, participants were not excluded nor replaced into a different condition.
References
Yang LH, Wonpat-Borja AJ (2007) Psychopathology among Asian Americans. In: Leong FTL, Inman, Ebreo A, Yang L, Kinoshita L, Fu M (eds) Handbook of asian american psychology, 2nd edn. Sage, Thousand Oaks, pp 379–406
NAMI (2011) Asian American and Pacific Islander (AA/PI) Community and Mental Health Fact Sheet
Link BG, Yang LH, Phelan JC, Collins PY (2004) Measuring mental illness stigma. Schizophr Bull 30(3):511–541
Gary FA (2005) Stigma: barrier to mental health care among ethnic minorities. Issues Ment Health Nurs 26(10):979–999. doi:10.1080/01612840500280638
Leong FTL, Lau ASL (2001) Barriers to providing effective mental health services to Asian Americans. Ment Health Serv Res 3(4):201–214. doi:10.1023/A:1013177014788
Ihara ES, Chae DH, Cummings JR, Lee S (2013) Correlates of mental health service use and type among Asian Americans. Adm Policy Ment Health 1–9
Corrigan PW (2004) How stigma interferes with mental health care. Am Psychol 59(7):614–625. doi:10.1037/0003-066X.59.7.614
Kondrat D, Early T (2011) Battling in the trenches: case managers’ ability to combat the effects of mental illness stigma on consumers’ perceived quality of life. Commun Ment Health J 47:390–398. doi:10.1007/s10597-010-9330-4
Thornicroft G (2007) Shunned: discrimination against people with mental illness. Oxford University Press, New York
Lee AA, Laurent SM, Wykes TL, Kitchen Andren KA, Bourassa KA, McKibbin CL (2014) Genetic attributions and mental illness diagnosis: effects on perceptions of danger, social distance, and real helping decisions. Soc Psychiatry Psychiatr Epidemiol 49(5):781–789. doi:10.1007/s00127-013-0764-1
Phelan JC (2005) Geneticization of deviant behavior and consequences for stigma: the case of mental illness. J Health Social Behav 46(4):307–322. doi:10.1177/002214650504600401
Akdeniz C, Tost H, Meyer-Lindenberg A (2014) The neurobiology of social environmental risk for schizophrenia: an evolving research field. Soc Psychiatry Psychiatr Epidemiol 49(4):507–517. doi:10.1007/s00127-014-0858-4
Kendler KS (1997) The genetic epidemiology of psychiatric disorders: a current perspective. Soc Psychiatry Psychiatr Epidemiol 32(1):5–11. doi:10.1007/BF00800661
van der Vegt EJM, Tieman W, van der Ende J, Ferdinand RF, Verhulst FC, Tiemeier H (2009) Impact of early childhood adversities on adult psychiatric disorders: a study of international adoptees. Soc Psychiatry Psychiatr Epidemiol 44(9):724–731. doi:10.1007/s00127-009-0494-6
Corrigan PW, Morris SB, Michaels PJ, Rafacz JD, Rüsch N (2012) Challenging the public stigma of mental illness: a meta-analysis of outcome studies. Psychiatr Serv 63(10):963–973. doi:10.1176/appi.ps.201100529
Weiner B (1995) Judgments of responsibility: a foundation for a theory of social conduct. Guilford Press, New York
Schnittker J (2008) An uncertain revolution: why the rise of a genetic model of mental illness has not increased tolerance. Soc Sci Med 67(9):1370–1381. doi:10.1016/j.socscimed.2008.07.007
Rüsch N, Todd AR, Bodenhausen GV, Corrigan PW (2010) Biogenetic models of psychopathology, implicit guilt, and mental illness stigma. Psychiatry Res 179(3):328–332. doi:10.1016/j.psychres.2009.09.010
WonPat-Borja AJ, Yang LH, Link BG, Phelan JC (2012) Eugenics, genetics, and mental illness stigma in Chinese Americans. Soc Psychiatry Psychiatr Epidemiol 47(1):145–156. doi:10.1007/s00127-010-0319-7
Schomerus G, Matschinger H, Angermeyer MC (2013) Causal beliefs of the public and social acceptance of persons with mental illness: a comparative analysis of schizophrenia, depression and alcohol dependence. Psychol Med 1–12
Fukuyama MA, Greenfield TK (1983) Dimensions of assertiveness in an Asian American student population. J Couns Psychol 30(3):429–432. doi:10.1037/0022-0167.30.3.429
Wynaden D, Chapman R, Orb A, McGowan S, Zeeman Z, Yeak S (2005) Factors that influence Asian communities’ access to mental health care. Int J Ment Health Nurs 14(2):88–95. doi:10.1111/j.1440-0979.2005.00364.x
Yang LH, Kleinman A, Link BG, Phelan JC, Lee S, Good B (2007) Culture and stigma: adding moral experience to stigma theory. Soc Sci Med 64(7):1524–1535. doi:10.1016/j.socscimed.2006.11.013
Yang LH, Purdie-Vaughns V, Kotabe H, Link BG, Saw A, Wong G et al (2013) Culture, threat, and mental illness stigma: identifying culture-specific threat among Chinese American groups. Soc Sci Med 88:56–67. doi:10.1016/j.socscimed.2013.03.036
Haslam N (2011) Genetic essentialism, neuroessentialism, and stigma: commentary on Dar-Nimrod and Heine (2011). Psychol Bull 137(5):819–824. doi:10.1037/a0022386
Pescosolido BA, Martin JK, Long JS, Medina TR, Phelan JC, Link BG (2010) “A disease like any other”? A decade of change in public reactions to schizophrenia, depression, and alcohol dependence. Am J Psychiatry 167(11):1321–1330
Miresco MJ, Kirmayer LJ (2006) The persistence of mind-brain dualism in psychiatric reasoning about clinical scenarios. Am J Psychiatry 163(5):913–918. doi:10.1176/appi.ajp.163.5.913
Yeung A, Trinh NHT, Chang TE, Fava M (2011) The Engagement Interview Protocol (EIP): improving the acceptance of mental health treatment among Chinese immigrants. Int J Cult Men Health 4(2):91–105. doi:10.1080/17542863.2010.507933
Ryder AG, Yang J, Zhu XZ, Yao SQ, Yi JY, Heine SJ, Bagby RM (2008) The cultural shaping of depression: Somatic symptoms in China, psychological symptoms in North America? J Abn Psychol 117:300–313
Rangel U, Keller J (2012) Essentialism goes social: belief in social determinism as a component of psychological essentialism. J Pers Soc Psychol 100(6):1056–1078. doi:10.1037/a0022401
Yang LH, Phelan JC, Link BG (2008) Stigma towards traditional Chinese medicine and psychiatric treatment among Chinese Americans. Cult Divers Ethnic Minor Psychol 14(1):10–18. doi:10.1037/1099-9809.14.1.10
American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders, 4th edn. doi:10.1176/appi.books.9780890423349
Link BG, Phelan JC, Bresnahan M, Stueve A, Pescosolido BA (1999) Public conceptions of mental illness: labels, causes, dangerousness, and social distance. Am J Public Health 89(9):1328–1333. doi:10.2105/AJPH.89.9.1328
Wirth JH, Bodenhausen GV (2009) The role of gender in mental-illness stigma: a national experiment. Psychol Sci 20(2):169–173. doi:10.1111/j.1467-9280.2009.02282.x
Angermeyer MC, Matschinger H (2003) Public beliefs about schizophrenia and depression: similarities and differences. Soc Psychiatry Psychiatr Epidemiol 38(9):526–534. doi:10.1007/s00127-003-0676-6
Corrigan P, Markowitz FE, Watson A, Rowan D, Kubiak MA (2003) An attribution model of public discrimination towards persons with mental illness. J Health Soc Behav 44(2):162–179. doi:10.2307/1519806
Keller J (2005) In genes we trust: the biological component of psychological essentialism and its relationship to mechanisms of motivated social cognition. J Pers Soc Psychol 88(4):686–702. doi:10.1037/0022-3514.88.4.686
Corrigan PW, Lurie BD, Goldman HH, Slopen N, Medasani K, Phelan S (2005) How adolescents perceive the stigma of mental illness and alcohol abuse. Psychiatr Serv 56(5):544–550. doi:10.1176/appi.ps.56.5.544
Zane N, Yeh M (2002) Use of culturally-based variables in assessment: studies on loss of face. In: Kurasaki K, Okazaki S, Sue S (eds) Asian American mental health: assessment, theories and methods. Kluwer Academic, Dordrecht, pp 123–138. doi:10.1007/978-1-4615-0735-2_9
Preacher KJ, Hayes AF (2008) Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods 40(3):879–891. doi:10.3758/BRM.40.3.879
Phillips MR, Li Y, Stroup TS, Xin L (2000) Causes of schizophrenia reported by patients’ family members in China. Br J Psychiatry 177(1):20–25. doi:10.1192/bjp.177.1.20
Furnham A, Chan E (2004) Lay theories of schizophrenia. A cross-cultural comparison of British and Hong Kong Chinese attitudes, attributions and beliefs. Soc Psychiatry Psychiatr Epidemiol 39(7):543–552. doi:10.1007/s00127-004-0787-8
Markus HR, Kitayama S (1991) Culture and the self: implications for cognition, emotion, and motivation. Psychol Rev 98(2):224–253. doi:10.1037/0033-295X.98.2.224
Zhou Q, Chen SH, Cookston JT, Wolchik S (2014) Evaluating the cultural fit of the New Beginnings Parent Program for divorced Asian American mothers: a pilot study. Asian Am J Psychol 5:126. doi:10.1037/a0035519
Acknowledgments
This research was supported by the University of Oregon’s Graduate Education Committee Research Award. Special thanks to Drs. Azim Shariff and Bobby Cheon for their helpful suggestions, and to Dr. Elliot Berkman for helping with data analysis.
Conflict of interest
There is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Cheng, Z.H. Asian Americans and European Americans’ stigma levels in response to biological and social explanations of depression. Soc Psychiatry Psychiatr Epidemiol 50, 767–776 (2015). https://doi.org/10.1007/s00127-014-0999-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-014-0999-5