
Abstract
Purpose
In the USA, white children receive psychoactive drugs more often than black or Hispanic children. This study investigates whether cultural attitudes statistically mediate differences between American parents’ self-identified racial–ethnic group membership and their willingness to medicate children for behavioral problems.
Methods
Using data from telephone interviews with 1,145 parents in two Florida counties, structural models tested associations between each group compared with the other, in willingness to medicate children exhibiting different problematic behaviors and hypothesized cultural (familism, fatalism, attitude toward corporal punishment, religiosity, concern about treatment stigma, birth abroad, language of interview) and other mediators (views about medications and causes of children’s problems). Respondent gender, age, socioeconomic status, parent-type household, taking psychoactive medication, and having a child with behavioral problems were used as covariates.
Results
Race–ethnicity was strongly associated with specific cultural attitudes and views about medications and problems, but only Hispanics distinguished themselves significantly from whites in willingness to medicate children. Across groups, parents who viewed medication favorably and endorsed biomedical causes for problems were more willing to medicate. In Hispanic–white and Hispanic–black comparisons, being interviewed in Spanish was the sole but modest cultural mediator of willingness, and in black–white comparisons, only concern about treatment stigma weakly mediated differences in willingness.
Conclusions
These findings provide faint support for a parent-centered cultural explanation of reported prescription differences among youths of different racial–ethnic groups in the USA. However, structural and professional components of a broader cultural hypothesis for such differences, within the USA and between different countries, still require evaluation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Since the first report that American black youths enrolled in a state Medicaid program were half as likely as their white counterparts to be prescribed psychoactive drugs [1], several studies controlling potentially confounding factors have reported a similar or higher ratio, usually exceeding 3:1 when white children were compared to Hispanic children [2–8]. The findings hold for stimulant, antidepressant, and antipsychotic drug classes, suggesting that observed differences between racial–ethnic groups may be driven partly by “cultural” factors—attitudes and behavior patterns that characterize how racial–ethnic groups see themselves and are seen by others. However, no model has specified these factors and their relationships, and the suggestion has remained untested though frequently evoked. The present study outlines such a model and describes the results of a quantitative test of the hypothesis that among parents from the three main racial–ethnic groups in the USA, cultural variables such as familism, fatalism, religiosity, and language of interview mediate willingness to medicate children for behavioral problems such as hyperactivity and inattention, hostility, depression, and voicing suicidal thoughts. If parental willingness or unwillingness to medicate one’s child is indirectly caused by cultural attitudes, then it might be resistant to change in the short term regardless of other incentives or constraints acting upon parents, and, like some other culturally influenced behaviors, might change with acculturation.
Racial and ethnic differences in parents’ attitudes toward psychoactive drugs
Research suggests that most American adults harbor negative sentiments about prescribed psychoactive medications’ effects on children, and 86 % believe that physicians overmedicate children for common behavioral problems [9]. Still, adults’ and parents’ willingness to resort to medications for children’s problems, and views about the nature of these problems, vary by race–ethnicity, with blacks and Hispanics expressing greater skepticism than whites. African-American parents of children taking stimulants for attention-deficit hyperactivity disorder (ADHD) are (a) less likely to recommend medication or to prefer it over counseling, (b) less likely to describe ADHD in medical terms or worry about ADHD-related school problems, and (c) more worried that medication leads to harm than white parents [10, 11]. African-Americans have been found less willing than whites to medicate children, mostly due to beliefs about drug efficacy and side effects [12]. McLeod et al. [13], however, found that more respondents would use medications on children for suicidal than for oppositional or ADHD-like behavior, but observed no link between race and such preferences. No study has yet included a sizeable sample of Hispanic parents, but 62 American Hispanic mothers of children with behavior problems (from Cuba, the Dominican Republic, and Puerto Rico) “overwhelmingly preferred” non-medication treatment “primarily because they understood medication to be addictive, dulling of cognitive processes, and inappropriate for behavior problems” [14, p. 311].
Culturally related factors in psychoactive drug prescriptions to children
What salient cultural factors might drive the relationship between racial–ethnic group membership and willingness to medicate children for behavior problems? Culture refers to learned, deeply held, and widely shared ideas, standards, values, attitudes, and beliefs that serve to interpret experience and guide action [15]. Ethnicity (e.g., Anglo-American, Hispanic, or Latino) refers to nationality and national identification but, like culture, comprises group-shared patterns of social interaction (prominently language-based) and values, behaviors, and perceptions. The concept of race (e.g., white, black or African-American) has profound political and historical dimensions, although racial differentiation mainly rests on skin color. Seen by most scholars as a socio-cultural construction that offers no adequate way to conceptualize either phenotypic or genotypic biological differences between humans, race nonetheless has colossal significance as “lived experience” [16].
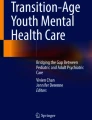
Singly or in interaction, three broad categories of social factors within American society could lead to differential rates of psychoactive drug prescription to children, as shown in the upper part of Fig. 1: structural barriers or incentives to care (e.g., availability, cost, underinsurance, direct-to-consumer advertising), attitudes and behaviors of providers (e.g., models of psychiatric illness, cultural competence), and attitudes and behaviors of parents, as discussed ahead. This study focuses on the latter category since without parental approval a child is unlikely to receive a prescription from a physician. The conceptual model of the culturally mediated relationship between race–ethnicity and willingness to prescribe psychoactive drugs to children for various behavioral problems used in this study is depicted in the lower part of Fig. 1.

Upper elements of a cultural hypothesis of differences in prescription rates to American children of different racial–ethnic groups, and lower conceptual model of the relationship between parental race–ethnicity and willingness to medicate children for behavior problems
Our review of the literature highlighted factors conceived as cultural and ethnic, given our above definitions, that could shape attitudes of parents toward the prescription of psychoactive drugs to children. Familism refers to families being closely knit and organized along an authoritarian hierarchy [17]. Parenting rests on strict demands and direct behavioral controls and fosters acquiescence to close relatives. Bird [15, p. 52] contrasts familism to “mainline American culture [with] highly individualistic orientation, greater latitude in child-rearing norms, more flexible disciplinary practices, and an emphasis on the development of autonomy.” In this study, familism is hypothesized to foster unwillingness to use extra-familial measures to change children’s behavior. Using corporal punishment to discipline children implies a view of children as morally responsible for their misbehavior or responsive to punishment, which runs counter to the therapeutic ethos that assigns impersonal causes to misbehavior or emphasizes the harm of punishment [18]. Greater acceptance of corporal punishment is hypothesized to be associated with lesser acceptance of drug treatment as a response to children’s oppositional behavior. Fatalism, the belief that one’s destiny is beyond one’s control, is hypothesized to foster an unwillingness to use medications to alter a functional or other behavioral deficit if it is perceived as part of one’s lot in life. Religiosity comprises cognitive, cultic, devotional, and social components [19], and might discourage or encourage medical explanations and management of distress. On the one hand, it fosters a view of personal problems as moral failings, with improvement resulting from personal resolve and discipline rather than technical remedies. On the other hand, religiosity fosters optimism and the use of multiple available resources to cope actively with a problem [20]. Finally, concerns about treatment-related stigma—defined as the social harm brought about by the label or the treatment of mental illness [21]—might be expected to lessen a parent’s willingness to medicate children.
Importantly, differences within racial or ethnic groups in the USA regularly surpass inter-group differences and are revealed by disaggregation [22]. About half of Hispanics in the USA are foreign-born [23]. Given lower prescription rates of psychoactive drugs to children outside the USA [24], we hypothesized that the sociodemographic variable of birth abroad could function as a cultural mediator in our model. Finally, a preference for the use of one’s Spanish native language in the USA when context and circumstances freely allow for the use of that language or English could indicate a stronger Hispanic ethnic identification. We therefore hypothesized that using Spanish during an interview would be related to specific attitudes concerning psychoactive medications and would mediate parents’ willingness to medicate children.
Most of the cultural constructs mentioned above may contribute to the observed racial–ethnic differences in prescriptions to children. For example, in a nationally representative sample of children under age 13 from two-parent families, black and Hispanic fathers showed more responsibility for child rearing and direct monitoring of children than white fathers, suggesting more familism [25]. Corporal punishment, though a normative practice in the USA [18], is regularly found to be more acceptable among racial–ethnic minority groups [26, 27]. In the USA, blacks have viewed themselves and have been viewed by others as especially religious and giving [28]. Samaan [29] argued that the perceived social support that stems partly from deeper religiosity among racial–ethnic minorities explains their tendency to report fewer mental health problems. Stigma is regularly cited as contributing to racial–ethnic minorities’ avoidance of mental health services [30] because it probably reveals a particular sensitivity of minorities to its exclusionary effects. However, Pescosolido et al.’s [9] observation that one-third to nearly 60 % of adults believe stigma is specifically attached to the drug treatment of children’s behavioral problems suggests a widespread sensitivity in the majority population as well, but it remains unclear how such stigma reflects on medical help-seeking.
To test the hypothesis that any racial–ethnic differences in parental willingness to use psychoactive drugs with children are mediated by particular attitudes toward psychoactive medications, particular views about what causes the behavior problems of children, and especially by the cultural constructs discussed in the preceding paragraphs, we collected data from three sufficiently large samples of parents of children aged 5–17 years, who were identified as non-Hispanic white, non-Hispanic black, or Hispanic of any race, drawn from two adjacent, urban, ethnically diverse counties in South Florida. According to the US Census Bureau [23], Miami-Dade County’s population of 2.5 million includes 74 % who categorize themselves as whites, 19 % as blacks, and 65 % as Hispanics of any race. Broward County has a population of 1.75 million, including 63 % whites, 27 % blacks, and 25 % Hispanics of any race. The full study protocol was approved by Florida International University’s Office of Research Integrity.
We conducted statistical analyses of the data to accomplish three goals: (1) To determine the direct relationship between membership in a racial–ethnic group (predictor) and the cultural constructs (mediators); here we hypothesized that black and Hispanic parents would express higher levels of familism, fatalism, religiosity, acceptance of corporal punishment, and perceived stigma of youth drug treatment than white parents, and white parents would endorse more biomedical causes for children’s problems and view psychoactive drugs as more beneficial than black and Hispanic parents. (2) To determine the direct relationship between the proposed mediators and willingness to have medications prescribed to one’s child (outcome); here we hypothesized that regardless of racial–ethnic membership, lower levels of familism, fatalism, religiosity, acceptance of corporal punishment, perceived stigma of youth drug treatment, and higher endorsement of biomedical causes and views of psychoactive drugs as beneficial, would be associated with higher willingness of parents to use medications. (3) To determine the mediational or indirect effect of each of these constructs in accounting for any differences between racial–ethnic groups on willingness to use medications; here we hypothesized that each cultural construct would emerge as a statistically significant mediator of the relations between racial–ethnic group membership and willingness to use medications.
Methods
Sampling and data collection
Data were collected by trained bilingual (English/Spanish) interviewers under the supervision of Florida International University Institute for Public Opinion Research from May 11 until October 8, 2009. Potential telephone numbers (landline only) in Miami-Dade and Broward counties were computer-dialed during the late afternoon and early evening hours on weekdays and during daytime on Saturdays. In 2009, 3.8 % of households in these two targeted counties of Florida were estimated not to have a landline [31].
In all, 35,311 different telephone numbers were called, yielding 1,145 complete interviews (see Table 1). Selecting quotas of respondents who met the inclusion criteria was accomplished in three phases: (1) filtering out-of-scope cases, (2) screening the remaining (eligible) cases to identify qualifying households, and (3) completing a full interview once a qualifying household was identified. First, we excluded all businesses, fax numbers, modems or other automatic disconnects, as well as respondents not residing in the household. Second, all numbers associated with residential households were considered eligible for screening. An eligible number could be called back up to 10 times until its final disposition was assigned. Third, all numbers of qualifying households were pursued to obtain consent to conduct an interview.
Non-cooperation at either the second (screening) or third (interview) phase produces sample bias when it results in different population groups having different probabilities of selection. However, non-cooperation at the interview phase can result in bias related to the content of the study as it involves a decision by potential respondents who have been introduced to the survey topic. Since we did not seek to estimate population parameters, we considered interview non-cooperation as the more serious problem. We obtained a screener cooperation rate (proportion of eligible households of all numbers called) of 34.4 %, or 41.4 % if out-of-scope numbers are excluded. Our interview cooperation rate (proportion of completed interviews of all qualifying households identified) was 87.9 %. “Response rate” in a telephone survey with no fixed population frame refers to the proportion of total numbers called that result in complete or incomplete interviews (3.2 % in this study, or 3.9 % if out-of-scope numbers are excluded) [32].
Questionnaire
Our structured questionnaire contained 60 variables, including some from previous English-language US population-based studies, especially the 1998 and 2002 General Social Survey (GSS, www.norc.uchicago.edu/GSS+Website). The choice of variables was guided by the literature review, published reliability and validity statistics, and ease of use during a telephone interview. A Spanish-language version was produced via independent translation and back-translation, and then review of each item’s wording by two native Spanish-speaking researchers to ensure fit with various idioms in common use in the South Florida Spanish-speaking population. Copies of these instruments are available from the authors.
Measures
Measures of all variables are described below. Table 2 provides descriptive statistics and internal consistency estimates (where appropriate) for each measure for each of the three racial–ethnic groups of parents in the study.
Predictor: race–ethnicity
Of the 1,145 respondents, 1,080 (94.3 %) were classified as either non-Hispanic black (n = 345), non-Hispanic white (n = 344), or Hispanic of any race (n = 391, including 84.0 % white, 5.4 % black, and 10.6 % mixed race, Asian, American-Indian, and other). All subsequent analyses are restricted to these 1,080 respondents, and the three groups are hereafter referred to as black, white, and Hispanic for brevity.
Outcome: willingness to give children doctor-prescribed medication for behavioral problems
This observed variable was composed of four items adapted from the 1998 GSS, asking respondents to indicate how likely they “would be willing to give doctor-prescribed medication to your child or a child you were responsible for in each of the following situations”: a child who “is hostile, often loses his/her temper, often argues with adults, actively defies authority and seems spiteful and vindictive,” a child who “is not paying attention in school, does not finish school work or chores, has difficulty organizing activities, is easily distracted, and seems to run around and fidget constantly,” a child who “is depressed or irritable, withdraws from family, friends, and activities, and is not sleeping or eating properly,” and a child who “was talking about killing him- or herself.” The first three situations mapped roughly onto the oppositional defiant disorder, ADHD, and depression constructs of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision [33]. Responses to each item were rated on a 4-point scale (from 1 = very unlikely to 4 = very likely) summed, and averaged.
Proposed mediators
Perceived biomedical causes for children’s problems This variable was adapted from the 2002 GSS and variants have been used in several cited studies. Respondents were read each of the four problem situations from the outcome variable above and asked to choose one most likely cause from eight choices representing moral, biomedical, stress-related, family-rearing, diet, and supernatural explanations. The score consisted of a count of the number of times (from 0 to 4) a respondent endorsed either “a chemical imbalance in the brain” or “a genetic or inherited problem” for the problems taken together.
Perceived benefits of medications This variable was measured as a latent construct with four items from the 2002 GSS, asking respondents to rate the benefits of psychoactive medications (from 1 = strongly disagree to 4 = strongly agree). The items were “Psychiatric medications help people deal with day-to-day stresses,” “get along with family and friends,” “control their symptoms,” and “feel better about themselves.” Results of tests of this and other latent constructs are described ahead.
Perceived sigma of mental health treatment of youth This variable was measured as a latent construct with the only scale known to assess it, from the 2002 National Stigma Study (NSS) [9]. Respondents were asked to rate their agreement (from 1 = strongly disagree to 4 = strongly agree) with whether a child receiving mental health treatment “would become an outsider at school,” “would suffer as an adult if others learned of the past treatment,” whether the “community would manage to identify such a child,” and whether the “parent would feel like a failure.” We obtained internal reliability coefficients of 0.61 (for whites and for Hispanics) and 0.62 (for blacks) for this latent construct but opted to retain it as it yielded a Cronbach’s α of 0.68 when used in the NSS with a large sample that included only 3 % Hispanics.
Religiosity We developed this latent construct made up of five items from the 2002 GSS [19] tapping five different dimensions: “Do you have a religious affiliation? (1 = No, 2 = Yes); How often do you attend religious services? (1 = never to 7 = every day); How often do you pray privately in places other than at church or synagogue? (1 = never to 7 = every day); If you had a problem or were faced with a difficult situation, how much comfort would the people in your congregation be willing to give you? (1 = no congregation, 2 = no comfort at all to 5 = all the comfort I need); To what extent do you consider yourself a religious person? (1 = non-religious to 4 = very religious).
Familism This 2-item observed variable was adapted from Portes and Rumbaut [34]. Respondents were asked how much they agreed (from 1 = strongly disagree to 4 = strongly agree) with the statements: “When someone has a serious problem, only relatives can help,” and “One should find a job near his/her parents even if it means losing a better job somewhere else.” Answers were summed and averaged to yield a total familism score.
Fatalism This two-item observed variable was adapted from Saucier [35]. Respondents were asked how much they agreed (from 1 = strongly disagree to 4 = strongly agree) with two statements: “Most events are predetermined by fate, and therefore unchangeable,” and “Most people decide what happens to them in their lives.” After reverse-coding the second item, answers were summed and averaged to yield a total fatalism score.
Acceptability of corporal punishment This single-item variable was adapted from the 2002 GSS: “How much do you agree that it is sometimes necessary to discipline a child with a good, hard spanking?” Responses were rated from 1 = strongly disagree to 4 = strongly agree.
Country of birth Respondents were categorized as born in or outside the USA.
Language of interview Respondents were categorized as interviewed in English or in Spanish.
Sociodemographic variables
Using tests described ahead, the following sociodemographic variables were examined for their potentially confounding role in the analyses: respondent gender; respondent age; socioeconomic status (SES, a composite measure with a score ranging from 1 to 12 by summing the annual household income variable ranging from 1 = <$10,000) to 6 = >$80,000) and the education variable ranging from 1 = grade school completed to 6 = graduate degree completed); single- or two-parent-type household; whether respondent had a child with a behavioral, emotional, or psychological problem; and whether respondent himself or herself took doctor-prescribed medication for such a problem. Based on the literature, we expected that women, those with lower socioeconomic status and those in single-parent households would be more willing to prescribe. We did not locate studies of parental attitudes (or studies of prescription rates in children) that controlled for having a child with a problem and for taking a psychoactive medication. Assuming that these circumstances indicated that parents had actually faced the decision to medicate their child or themselves, we expected that controlling for them would increase the validity of the present test of a parent-centered cultural mediation hypothesis.
Statistical analyses
All analyses were conducted using SPSS version 17 (SPSS, 2008) [36] and Mplus (Muthén and Muthén, 2007) [37] statistical software.
Preliminary analyses
We first calculated frequency distributions for all continuous variables to determine if they violated the assumption of normality (i.e., absolute skewness and kurtosis values >2.3 [38]). Within each ethnic/racial group, we calculated descriptive statistics for, and bivariate correlations among, mediators and covariates. Pearson product-moment and Spearman’s rank correlation coefficients were examined between all continuous and non-continuous mediators and covariates, respectively, included in the final mediation analyses for evidence of discriminant validity and multicollinearity (i.e., correlation coefficient values <0.70 [39]). Nominal variables (language of interview and country of birth) were dummy coded a value of 1 or 2 to facilitate analyses (see Table 2 notes).
Analyses of potential confounds across racial and ethnic groups
We conducted a multivariate analysis of variance (MANOVA) and Chi-square difference tests to identify potentially confounding sociodemographic variables across racial and ethnic groups. For variables where the omnibus analysis of variance (ANOVA) was significant in the MANOVA, least significant difference (LSD) pair-wise comparisons among the three racial–ethnic groups were conducted to identify significant differences between any two groups. Any variables yielding such differences were accounted for as covariates, using multiple indicators, multiple causes (MIMIC) modeling in Mplus [40], in the final mediation analyses.
Measurement model for assessing latent constructs
We conducted a confirmatory factor analysis to examine the fit of a measurement model consisting of the three proposed latent construct (perceived benefits of medications, perceived treatment stigma, and religiosity). Of note, three separate structural mediation models were used in this study to test direct associations between (1) Hispanics vs. whites, (2) Hispanics vs. blacks, and (3) blacks vs. whites in their willingness to medicate and the hypothesized mediators. Hence, the measurement model including all latent constructs was examined separately using data from each of the three comparison groups in the study. In each comparison, the model was estimated using the maximum-likelihood mean-adjusted method in Mplus, and it was evaluated using the comparative fit index (CFI), for which values above 0.90 reflect adequate fit [41] and values above 0.95 represent excellent fit [42]; and the root mean square error of approximation (RMSEA), for which values below 0.08 represent adequate fit [41] and those below 0.05 represent excellent fit [43]. These same guidelines were used to evaluate model fit for each of the three structural mediation models used to test mediated effects.
Structural mediation models
Our next step was to assess (a) differences between racial–ethnic groups in willingness to medicate (direct effects), and (b) the roles of the hypothesized mediators in the relationship between membership in a racial–ethnic group and willingness to medicate (indirect effects) via the three structural mediation models (Hispanics vs. whites, Hispanics vs. blacks, and blacks vs. whites). Statisticians have questioned the traditional requirement in mediation testing [44] that the independent variable must be directly associated with the outcome [45, 46]. Thus, we planned to proceed with tests of mediations even in the absence of statistically significant direct effects (p < 0.05), since mediation might still be assumed if the relationship operates through a third unobserved variable [47]. Traditional methods of assessing the statistical significance of mediation effects on the basis of normal theory [44] might be inappropriate because the product of the two path coefficients that make up an indirect effect is not distributed normally [48]. Therefore, we used a procedure based on bootstrap methods to test statistical significance of the hypothesized mediation effects in all three structural mediation models [46]. Unlike the traditional test [44], the procedure based on bootstrap methods can test more than one mediating sequence at a time. Five hundred bootstrap samples from the original data in each of the three models were run to generate point estimates of the magnitude of the indirect effects and the associated 95 % confidence intervals. If the confidence intervals exclude zero, then the indirect effects are statistically significant at the 0.05 level [46].
Results
Preliminary analyses
None of the variables were deemed problematic on the basis of skewness and kurtosis in any of the three racial–ethnic groups, and bivariate correlations suggested acceptable discriminant validity and an absence of multicollinearity in all models (see Table 2).
Potential confounds across racial–ethnic groups
A MANOVA conducted with race–ethnicity as the predictor variable and SES and age as criterion variables was significant, Wilks’ Λ = 858, F (4, 1716) = 32.21, p < 0.001, η 2 = 0.07. Subsequent ANOVAs revealed significant F values for SES and age (see Table 3), and LSD pair-wise comparisons revealed that on average, whites had significantly higher SES than either blacks or Hispanics and Hispanics a higher SES than blacks; whites were also older than blacks and Hispanics.
Chi-square tests were conducted to detect proportional differences between racial and ethnic groups based on participant gender; parent-type household; having a child or children with behavioral, emotional or psychological problems; and whether respondent took any doctor-prescribed medication for a psychological, emotional or behavioral problem (Table 3). The following significant results were observed. More white men than black and Hispanic men responded. Blacks indicated more single parent households than Hispanics and whites, and Hispanics more than whites. Whites reported having a child with behavioral, emotional or psychological problems more often than blacks and Hispanics, and also indicated taking prescribed medication for a psychological, emotional or behavioral problem more often. Therefore, when comparing Hispanics or blacks vs. Whites in their respective structural direct effect and mediation models, we controlled for age, gender, SES, household, having a child with behavioral, emotional or psychological problems, and taking prescribed psychoactive medication oneself. When comparing Hispanics vs. blacks in the corresponding structural direct effect and mediation models, we controlled only for SES and household.
Measurement model for testing mediated effects
Results indicated an excellent fit of the measurement model to the data in each of the three comparison group: whites vs. Hispanics (n = 735; CFI = 0.97; RMSEA = 0.04); Hispanics vs. blacks (n = 736; CFI = 0.99; RMSEA = 0.02); and whites vs. blacks (n = 689; CFI = 0.98; RMSEA = 0.03). Factor loadings of all 13 measured items on their three corresponding latent variables were statistically significant (β 0.37–0.82, p < 0.001) in each of the three comparison groups, suggesting that the latent variables were adequately measured by their indicators.
Structural mediation models
Hispanic vs. white model
Results indicated an adequate fit to the data (CFI = 0.90, RMSEA = 0.05). Examining covariate effects, having a child with a problem was the only covariate to significantly associate (positively) with willingness to medicate (β = −0.25, p < 0.001). As for associations between the covariates and mediators, parents with such a child (β = 0.58, p < 0.001) and women (β = −0.22, p = 0.01) endorsed more biomedical causes, and women were more often born outside the USA (β = 0.15, p = 0.03). Lower SES was associated with more fatalism (β = −0.26, p < 0.001), more familism (β = −0.19, p < 0.001) with birth outside the USA (β = −0.11, p = 0.002), and with being interviewed in Spanish (β = –0.28, p < 0.001).
Looking at direct effects of race–ethnicity on willingness, Hispanics reported a significant lesser willingness to medicate in comparison to white participants, after accounting for covariates. Hispanics reported more acceptance of corporal punishment, less perceived benefit of psychiatric medications, and higher familism. Hispanics were also more often born outside of the USA and interviewed in Spanish, but were less fatalistic. Parents from either group perceiving more benefits of medications, endorsing more biomedical causes of children’s problems, and being less concerned about treatment stigma were more willing to medicate, whereas those interviewed in Spanish were less willing (see Table 4).
Perceived benefits of medications and language of interview mediated the relationship between Hispanic or white group membership and willingness to medicate children after controlling for covariates (see Table 5).
Hispanic vs. black model
Results indicated an adequate fit to the data (CFI = 0.90; RMSEA = 0.04). Examining covariate effects, SES was the only covariate to significantly associate with willingness to medicate (β = −0.11, p = 0.012). Parents reporting higher SES were less willing to medicate. As for associations between the covariates and mediators, SES was inversely related to familism (β = −0.22, p < 0.001), fatalism (β = −0.19, p < 0.001), being interviewed in Spanish (β = −0.22, p < 0.001) and being born outside of the USA (β = −0.08, p < 0.001). Parents from two-parent households reported more religiosity (β = 0.26, p = 0.011).
Looking at direct effects of race–ethnicity on willingness, no significant difference in willingness to medicate was determined between Hispanic and black participants, after accounting for covariates. Hispanics reported less religiosity, less acceptance of corporal punishment, less treatment stigma concerns, and less fatalism than blacks. They were also more likely to be born outside of the USA and to be interviewed in Spanish. Parents from either group perceiving more benefits of medications and endorsing more biomedical causes for children’s problems were more willing to medicate, as were those interviewed in English (see Table 4). Finally, language of interview mediated the relationship between Hispanic or black group membership and willingness to medicate after controlling for covariates (see Table 5).
Black vs. white model
Results indicated an adequate fit to the data (CFI = 0.91; RMSEA = 0.04). No covariates significantly associated with willingness to medicate. As for associations between the covariates and mediators, men (β = 0.42, p = 0.001) and parents with lower SES (β = −0.18, p = 0.02) showed more treatment stigma concerns. Women (β = −0.35, p = 0.001), parents from two-parent households (β = 0.36, p < 0.001), as well as older parents (β = 0.10, p = 0.009) reported more religiosity. Parents having a child with a problem endorsed more biomedical causes of problems (β = 0.71, p < 0.001) and perceived more benefits of medications (β = 0.43, p < 0.001). Women also endorsed more biomedical causes (β = −0.20, p = 0.017). Parents with lower SES (β = −0.25, p < 0.001) and men (β = 0.18, p = 0.036) reported more familism. Parents in two-parent households (β = 0.44, p < 0.001), those who are not having a child with a problem (β = 0.21, p = 0.008), and women (β = 0.17, p = 0.03) were born outside of the USA more often than their counterparts.
Looking at direct effects of race–ethnicity on willingness, no significant difference in willingness to medicate was indicated between black and white participants, after controlling for covariates. Black parents reported more religiosity, more acceptance of corporal punishment, and more treatment stigma concerns. They also reported more fatalism and more familism, and were born outside of the USA more often. Parents of either group perceiving more benefits of medications, endorsing more biomedical causes of problems, and reporting more familism were more willing to medicate (see Table 4). Finally, perception of treatment stigma mediated the relationship between black or white racial group membership and willingness to medicate after controlling for covariates (see Table 5).
Post hoc comparison of within-Hispanic group differences
Since being interviewed in Spanish mediated the relationships between Hispanic and either white or black group membership and willingness to medicate children, we explored the relationship between language of interview and willingness to medicate within the Hispanic sample only. Hispanic participants who requested to be interviewed in Spanish were less willing to medicate than Hispanics who were interviewed in English (β = −0.25, p = 0.007).
Discussion
This study is the first to test directly, among the three major racial–ethnic groups in the USA, the hypothesis that cultural factors might account for differences in parents’ willingness to medicate children—itself conceptualized as one component of a broader cultural explanation for observed differences in psychoactive drug prescription rates among American children. However, only one of the six hypothesized cultural mediators passed the statistical mediation test: opting for speaking Spanish in the study interview had a significant negative mean indirect effect on parents’ willingness to medicate, in Hispanic vs. white and in Hispanic vs. black comparisons, as well as in a post hoc comparison with English-interviewed Hispanics. This indicates that the significant direct relationship observed between racial and ethnic group comparisons involving Hispanics was driven by differences in language spoken during the interview—a variable that some consider a unidimensional marker of acculturation [49, 50]. However, its effect was modest (<−0.20). Two non-cultural hypothesized mediators also passed the mediation tests, but showed weak or very weak magnitude (Table 5). In the Hispanic vs. white comparison, holding less favorable view of the benefits of psychoactive medications had a significant mean indirect effect on a parent’s willingness to medicate; and in the relationship between black vs. white group membership and willingness to medicate, a higher concern for treatment stigma also exerted a very small mean indirect effect on willingness. By simultaneously controlling for theoretically derived and empirically important covariates, the MIMIC analyses in this study provided a higher degree of accuracy in the estimates generated for the relations among racial–ethnic group membership and willingness to medicate and the mediated effects. We conclude that although self-reported cultural attitudes vary substantially by race and ethnicity, once potentially confounding variables are accounted for, these attitudes do not seem to exert substantial influence on parents’ hypothetical willingness to medicate their children for behavioral problems.
The mediation of language of interview in comparisons involving Hispanics raises the question of the meaning of a respondent using Spanish during a telephone interview. It is unsatisfactory to consider this variable as a proxy for acculturation, a complex and multidimensional construct [51] that was not assessed in this study. Yet, even if reflecting only a preference to speak Spanish with a Spanish-speaking interviewer in a county with a majority of Hispanics, the variable speaks about the respondent’s identification with the locally dominant ethnicity. In sum, opting for a Spanish interview has an unclear meaning in accounting for differences between Hispanic and white or black parents’ willingness to medicate their children, and it might support a hypothesis of cultural mediation of such parental willingness, especially since Hispanics interviewed in English were more willing to medicate. Future studies on this topic should explore the specific role of acculturation with measures doing justice to the complexity of this construct.
In this study, differences between the three groups in the outcome variable were in the expected directions but not pronounced, with only Hispanics distinguishing themselves significantly from whites. Thus, the consistently reported sharp differences in prescription rates of psychoactive drugs to children of different races and ethnicities in the USA were not isometric with the present observed relationships between parents’ racial and ethnic group membership and their willingness to have drugs prescribed. The findings are more aligned with previous findings that US adults overall report being wary of medicating children [9]. However, in the absence of empirical usage data (about numerous medication classes) to strengthen the presumed relationship between expressed willingness and rates of dispensation, the findings must remain provisional.
We observed that the three main American racial–ethnic groups vary especially in their religiosity and attitude toward corporal punishment of children. We also observed that most constructs, in one or more group comparisons, are associated with variations between the groups concerning their perceptions of psychoactive medication’s benefits. In turn, in all group comparisons, viewing medication more positively was associated with more willingness to resort to it to handle a child’s problems. In comparisons between whites and Hispanics and whites and blacks, viewing medication positively was also associated with endorsing more biomedical causes for distress and misbehavior in children. Endorsing more biomedical causes, in turn, was associated with more willingness to medicate children when blacks and Hispanics were compared. In sum, these findings suggest that views of psychiatric medications as beneficial, biomedical understandings of children’s behavioral problems, and views of children’s drug treatment as socially benign would be expected to increase any parent’s willingness to resort to psychoactive prescriptions to manage their child’s problem. The extent that such views are shared more often by whites in America than by blacks or Hispanics might explain why actual prescriptions to children differ so sharply along racial and ethnic lines. The first two variables—key elements of the medical model that dominates the management of problem behavior in the USA in general—appear in this study as leveling influences on all parents concerning their willingness to medicate children, while an opposite concern with stigma of the mental health treatment of youth appears much less relevant. Although treatment stigma emerged as a very weak mediator in this study, we used its only available measure [9]; one yielding higher coefficients of internal consistency might have increased the strength of its observed effect. Our hypothesis did not account for recent work suggesting that some stigmatizing attitudes are related to an increased willingness to seek professional help [52].
Sociodemographic covariates—in particular, SES and having a child with a behavioral problem—exerted significant influences on the hypothesized mediators. In both Hispanic vs. white and Hispanic vs. blacks comparisons, lower SES was associated with more familism, more fatalism, and being interviewed in Spanish. In blacks vs. whites, lower SES was associated with more familism as well as more concerns about treatment stigma. Having a child with a problem also, as expected, was associated with endorsing more biomedical causes and greater willingness to medicate in Hispanics vs. whites comparisons and in black vs. white comparisons. Respondents reporting having a child with a problem more closely resemble parents in the USA who seek or obtain mental health interventions for their children, for whom the decision to medicate is probably not hypothetical. A parent-centered cultural mediation hypothesis for reported prescription rate differences assumes that cultural constructs operate among all parents. Using this variable as a covariate in the present analyses yields results confirming that cultural attitudes that might influence parents’ actual decisions to medicate are only some of the factors at work in producing actual prescription decisions (e.g., they interact with other factors such as a parent’s encounter with and conceptualization of his or her child’s distress, the treatment system, and yet other factors, as conceptualized in Fig. 1).
The absence of observed relationships between the covariate of a respondent taking a psychoactive medication and any of the hypothesized predictors or the outcome suggests that personal considerations involved in the decision to medicate oneself, and those involved in decisions to medicate one’s child, are separate. This suggestion, however, must be reconciled with persistently observed differences in rates of prescription of psychoactive drugs to adults in the USA along the same lines as are observed in children, e.g., 14 % of non-Hispanic white persons aged 12 and over take antidepressant medications, compared with 4 % of non-Hispanic black and 3 % of Mexican-American persons [53]. Religiosity also showed no relationships with either the hypothesized predictor or the outcome when controlling for covariates. Although our measure for this construct was probably conceptually adequate and sufficiently reliable, we remained without a convincing hypothesis for how the multiple intentions and behaviors constituting religiosity would, on balance, reduce parents’ willingness to medicate their children for behavior problems.
Some limitations or cautions in interpreting the findings include the following. First, among potentially eligible participants, an unknown proportion of the nearly 2,200 individuals with whom contact was established but who hung up or refused before being informed of the purpose of the interview could have represented qualifying households. Thus, self-selection remains a potential threat to the validity of the study. Second, the validity of the Spanish version of this study instrument remains somewhat undetermined. While the outcome variable showed good internal consistency in all groups, reliability coefficients for the three latent construct variables were lower in the Hispanic and black groups. The inclusion of a sizeable number of Hispanic respondents, a definite strength of this study, highlights the importance for future studies to use instruments validated with the populations of study. Finally, the findings may be not be generalizable to the larger US Hispanic population, as the national origins of South Florida Hispanic respondents differ substantially from those of the larger population [54].
Conclusion
In the USA, a longstanding controversy over prescribing psychoactive drugs to children shows no signs of abating as approximately 7 % of boys and 5 % of girls under the age of 19 in the USA are taking a psychotropic medication [55], often in multi-drug combinations [56]. Based on our review of literature published over the past two decades, we discern three main justifications for prescriptions to youth: (1) medications are a familiar social and medical response to any acute distress, deviance and misbehavior, (2) the use of psychoactive drugs flows logically from heavily researched neurobiological causal hypotheses of same problems, and (3) validated observations exist for stimulants’ short-term alterations of hyperactive and inattentive behavior. On the other hand, we discern four main concerns: (1) prescription patterns outpace evidence of pediatric safety and efficacy, (2) normal family conflicts, childhood misbehaviors, and variations in temperament are medicalized, (3) conflicts of interests in the research enterprise mislead providers and consumers about drug effects, and (4) the study of potential harm to the child’s developing brain and emotions is neglected by responsible authorities. Considering both positions, therefore, it remains undetermined whether, at a population level, observed racial–ethnic differences in prescriptions rates to American children constitute a traditional health disparity favoring white children (because of their proportionally greater exposure to medications’ benefits), or conversely, an advantage for black and Hispanic children (because of their lesser exposure to medications’ risks). This study therefore took a logical first step of investigating possible reasons for the majority’s apparently greater approval of psychoactive medications and for racial–ethnic minorities’ apparently greater skepticism.
In international comparisons, the cultural causation hypothesis appears more compelling. Like the USA, most European countries have strong biomedical orientations in health research and practice and strong interests in the wellbeing of their children. Moreover, their often-universal health insurance programs cover an equally or larger range of medicines than the best private or public insurance programs in the USA. The use of psychotropic medications among children in these countries, though growing, remains substantially lower than in the USA, suggesting that cultural factors—learned, deeply held, and widely shared ideas that serve to interpret experience and guide action—are at work. Although a cultural causation hypothesis centered on parental decisions as mechanisms through which cultural influence may operate in the USA mostly failed in the quantitative test we devised for it, the findings do not speak about other structural and professional factors that may explain why white children in the USA are more likely to receive psychoactive drugs, and why children in the USA generally are more likely to receive psychoactive drugs than children in many other countries with similar or higher socioeconomic indicators.
References
Zito JM, Safer DJ, dosReis S, Riddle MA (1998) Racial disparity in psychotropic medications prescribed for youth with Medicaid insurance in Maryland. J Am Acad Child Adolesc Psychiatry 37:179–184
Hoagwood K, Jensen PS, Feil M, Vitiello B, Bhatara VS (2000) Medication management of stimulants in pediatric practice settings: a national perspective. J Dev Beh Pediatr 21:322–331
Olfson M, Blanco C, Liu L, Moreno C, Laje G (2006) National trends in the outpatient treatment of children and adolescents with antipsychotic drugs. Arch Gen Psychiatry 63:679–685
Olfson M, Gameroff MJ, Marcus SC, Waslick BD (2003) Outpatient treatment of child and adolescent depression in the United States. Arch Gen Psychiatry 60:1236–1242. doi:10.1001/archpsyc.60.12
Olfson M, Marcus SC, Weissman MM, Jensen PS (2002) National trends in the use of psychotropic medications by children. J Am Acad Child Adolesc Psychiatry 41:514–521
Rhagavan R, Zima BT, Andersen RM, Leibowitz AA, Schuster MA, Landsverk JA (2005) Psychotropic medication use in a national probability sample of children in the child welfare system. J Child Adolesc Psychopharmacol 15:97–106
Rowland AS, Umbach DM, Stallone L, Naftel AJ, Bohlig EM, Sandler DP (2002) Prevalence of medication treatment for attention-deficit hyperactivity disorder among elementary school children in Johnston County, North Carolina. Am J Public Health 92:231–234
Zuvekas SH, Vitiello B, Norquist GS (2006) Recent trends in stimulant medication use among US children. Am J Psychiatry 163:579–585
Pescosolido BA, Perry BL, Martin JK, McLeod JD, Jensen PS (2007) Stigmatizing attitudes and beliefs about treatment and psychiatric medications for children with mental illness. Psychiatr Serv 58:613–618
Bussing R, Gary FA, Mills TL, Garvan C (2003) Parental explanatory models of ADHD: gender and cultural variations. Soc Psychiatry Psychiatr Epidemiol 38:563–575
DosReis S, Zito JM, Safer DJ, Soeken KL, Mitchell JW Jr, Ellwood LC (2003) Parental perceptions and satisfaction with stimulant medication for attention-deficit hyperactivity disorder. J Dev Behav Pediatr 24:155–162
Schnittker J (2003) Misgivings of medicine? African Americans’ skepticism of psychiatric medication. J Health Soc Behav 44:506–524
McLeod JD, Pescosolido BA, Takeuchi DT, White TF (2004) Public attitudes toward the use of psychiatric medications for children. J Health Soc Behav 45:53–67
Arcia E, Fernández MC, Jáquez M (2004) Latina mothers’ stances on stimulant medication: complexity, conflict, and compromise. J Dev Behav Pediatr 25:311–317
Bird HR (2004) The role of culture, race, and ethnicity in child and adolescent psychiatry. In: Wiener JM, Dulcan MK (eds) American psychiatric publishing textbook of child and adolescent psychiatry, 3rd edn. American Psychiatric Publishing, Washington, pp 45–55
Goodman AH (2000) Why genes do not count (for racial differences in health). Am J Public Health 90:1699–1702
Unger JB, Ritt-Olson A, Teran L, Huang T, Hoffman BR, Palmer P (2002) Cultural values and substance use in a multiethnic sample of California adolescents. Addict Res Theor 10:257–279
Straus MA (2010) Prevalence, societal causes, and trends in corporal punishment by parents in world perspective. Law Contemp Probl 73:1–30
Idler EL, Musik MA, Ellison CG, George LK, Krause N, Ory MG, Pargament KI, Powell LH, Underwood LG, Williams DR (2003) Measuring multiple dimensions of religion and spirituality for health research: conceptual background and findings from the 1998 General Social Survey. Res Aging 25:307–347
Cummings JP, Pargament KI (2010) Medicine for the spirit: religious coping in individuals with medical conditions. Religions 1:28–53
Corrigan P (2004) How stigma interferes with mental health care. Am Psychol 59:614–625
Flores G, Bauchner H, Feinstein AR, Nguyen UDT (1999) The impact of ethnicity, family income, and parental education on children’s health and use of health services. Am J Public Health 89:1066–1067
US Census Bureau (2011) http://quickfacts.census.gov. Accessed 19 Dec 2011
Scheffler RM, Hinshaw SP, Modrek S, Levine P (2007) The global market for ADHD medications. Health Aff 26:450–457
Hofferth SL (2003) Race/ethnic differences in father involvement in two-parent families: culture, context, or economy? J Fam Issues 24:185–216
Giles-Sims J, Lockhart C (2005) Culturally shaped patterns of disciplining children. J Fam Issues 26:196–218
Straus MA, Stewart JH (1999) Corporal punishment by American parents: national data on prevalence, chronicity, severity, and duration, in relation to child and family characteristics. Clin Child Fam Psychol Rev 2:55–70
Utsey SO, Adams EP, Bolden M (2000) Development and initial validation of the africultural coping systems inventory. J Black Psychol 26:194–215
Samaan RA (2000) The influences of race, ethnicity, and poverty on the mental health of children. J Health Care Poor Underserved 11:100–110
Gary FA (2005) Stigma: barrier to mental health care among ethnic minorities. Issues Ment Health Nurs 26:979–999
US Census Bureau (2010) 2007–2009 American Community Survey 3-year estimates: tenure by telephone service in occupied housing units (Broward County, Miami-Dade County). http://factfinder.census.gov. Accessed 19 Dec 2011
American Association for Public Opinion Research (2009) Standard definitions: final dispositions of case codes and outcome rates for surveys. http://www.AAPOR.org. Accessed 02 June 2010
American Psychiatric Association (2000) Diagnostic and Statistical Manual of Mental Disorders, 4th ed text rev. American Psychiatric Press, Washington
Portes A, Rumbaut RG (2001) Legacies: the story of the immigrant second generation. University of California Press, Berkeley
Saucier G (2000) Isms and the structure of social attitudes. J Pers Soc Psychol 78:366–385
SPSS (2008) SPSS 17. SPSS Inc, Chicago
Muthén LK, Muthén BO (1997–2008) Mplus user’s guide (5th ed). Muthén & Muthén, Los Angeles
Lei M, Lomax RG (2005) The effect of varying degrees of nonnormality in structural equation modeling. Struct Equ Modeling 12:1–27
Tabachnick BG, Fidell RG (2007) Using multivariate statistics (5th ed). Allyn and Bacon, Boston
Bollen KA (1989) Structural equations with latent variables. Wiley-Interscience, Hoboken
Hu L, Bentler PM (1999) Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model 6:1–55
Tomarken AJ, Waller NG (2005) Structural equation modeling: strengths, limitations, and misconceptions. Annu Rev Clin Psychol 1:31–65
Hancock GR, Freeman MJ (2001) Power and sample size for the root mean square error of approximation test of not close fit in structural equation modeling. Educ Psychol Meas 61:741–758
Baron RM, Kenny DA (1986) The moderator-mediator variable distinction in social psychological research: conceptual, strategic and statistical considerations. J Pers Soc Psychol 51:1173–1182
Kenny DA, Kashy DA, Bolger N (1998) Data analysis in social psychology. In: Gilbert DT, Fiske ST, Lindzey G (eds) The handbook of social psychology, 4th edn. Oxford University Press, New York, pp 233–265
Shrout PE, Bolger N (2002) Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods 7:422–445
MacKinnon DP, Krull JM, Lockwood CM (2000) Equivalence of the mediation, confounding and suppression effect. Prev Sci 1:173–181
MacKinnon DP, Warsi G, Dwyer JH (1995) A simulation study of mediated effect measures. Multivariate Behav Res 30:41–62
Allen ML, Elliott MN, Fugligni AJ, Morales LS, Hambarsoomian K, Schuster MA (2008) The relationship between Spanish language use and substance use behaviors among Latino youth: a social network approach. J Adolesc Health 43:372–379. doi:10.1016/j.jadohealth.2008.02.016
Caetano R, Ramisetty-Mikler S, Wallisch LS, McGrath C, Spence RT (2008) Acculturation, drinking, and alcohol abuse and dependence among Hispanics in the Texas-Mexico border. Alcohol Clin Exp Res 32:314–321. doi:10.1111/j.1530-0277.2007.00576.x
Lopez-Class M, Castro FG, Ramirez AG (2011) Studying acculturation: a review and statement of critical issues. Soc Sci Med 72:1555–1562. doi:10.1016/j.socscimed.2011.03.011
Mojtabai R (2010) Mental illness stigma and willingness to seek mental health care in the European Union. Soc Psychiatry Psychiatr Epidemiol 45:705–712. doi:10.1007/s00127-009-0109-2
Pratt LA, Brody DJ, Gu Q (2011) Antidepressant use in persons aged 12 and over: United States, 2005–2008 NCHS data brief no. 76, National Center for Health Statistics, Hyattsville, MD
US Census Bureau (2010) The Hispanic population: 2010. www.census.gov/prod/cen2010/briefs/c2010br-04.pdf. Accessed 6 May 2012
Medco (2012) America’s state of mind. http://apps.who.int/medicinedocs/en/m/abstract/Js19032en/Accessed 6 Mar 2012
Comer JS, Olfson M, Mojtabai R (2010) National trends in child and adolescent psychotropic polypharmacy in office-based practice, 1996–2007. J Am Acad Child Adolesc Psychiatry 49:1001–1010. doi:10.1016/j.jaac.2010.07.007
Acknowledgments
This work was supported by grant no. 1R21MH084832 from the US National Institute of Mental Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cohen, D., Dillon, F.R., Gladwin, H. et al. American parents’ willingness to prescribe psychoactive drugs to children: a test of cultural mediators. Soc Psychiatry Psychiatr Epidemiol 48, 1873–1887 (2013). https://doi.org/10.1007/s00127-013-0710-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-013-0710-2